The Association of Serum Uric Acid with Risk of Obstructive Sleep Apnea: The Korean National Health and Nutrition Examination Survey 2019–2021


Abstract
1. Introduction
2. Materials and Methods
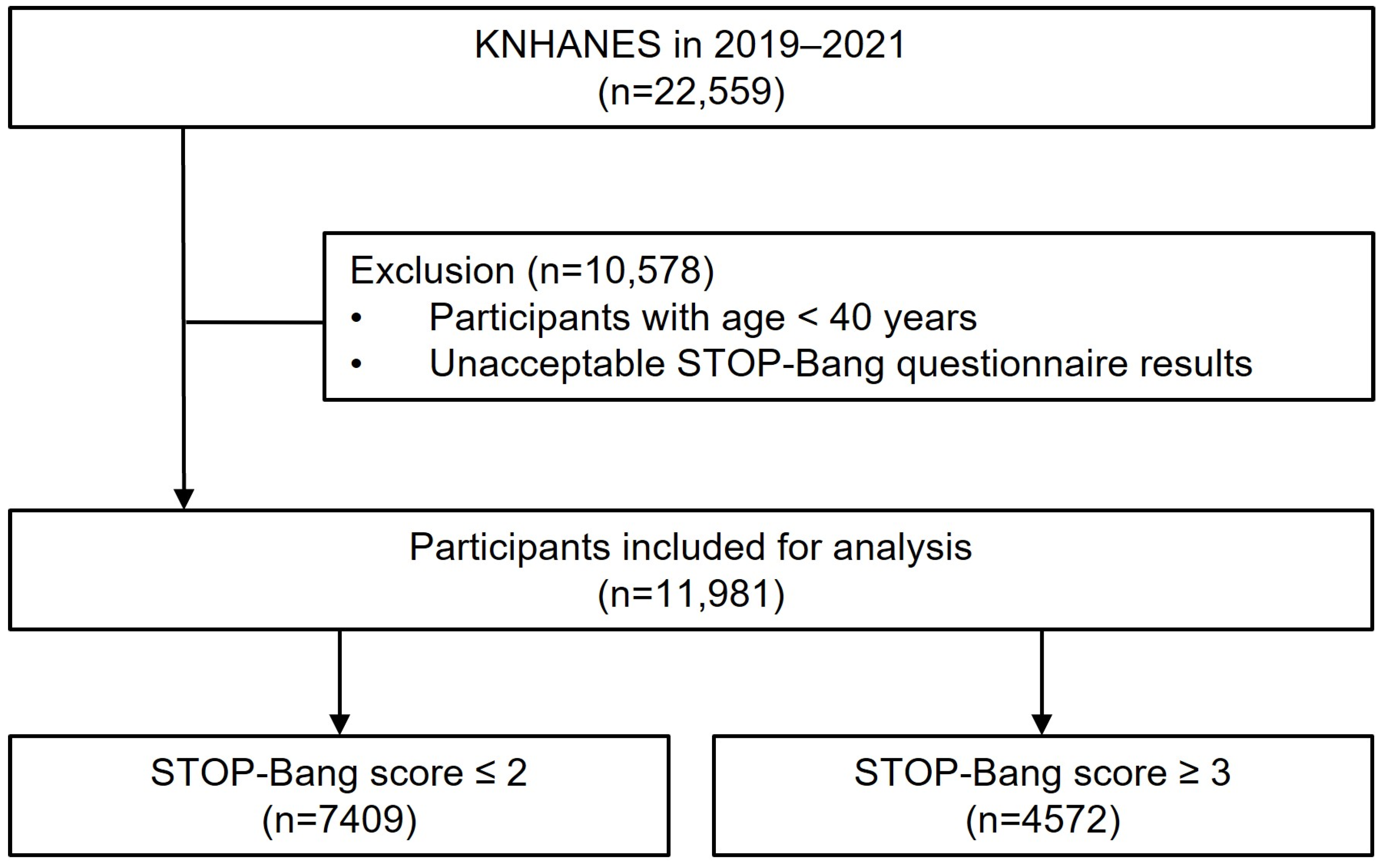
2.1. Study Population
2.2. Data Collection
2.3. Study Parameters
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mediano, O.; González Mangado, N.; Montserrat, J.M.; Alonso-Álvarez, M.L.; Almendros, I.; Alonso-Fernández, A.; Barbé, F.; Borsini, E.; Caballero-Eraso, C.; Cano-Pumarega, I.; et al. International Consensus Document on Obstructive Sleep Apnea. Arch. Bronconeumol. 2022, 58, 52–68. [Google Scholar] [CrossRef] [PubMed]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Ip, M.S.; Lam, B.; Tang, L.C.; Lauder, I.J.; Ip, T.Y.; Lam, W.K. A community study of sleep-disordered breathing in middle-aged Chinese women in Hong Kong: Prevalence and gender differences. Chest 2004, 125, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Lyons, M.M.; Bhatt, N.Y.; Pack, A.I.; Magalang, U.J. Global burden of sleep-disordered breathing and its implications. Respirology 2020, 25, 690–702. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, A.; Orr, J.E.; Owens, R.L. On the cutting edge of obstructive sleep apnoea: Where next? Lancet Respir. Med. 2015, 3, 397–403. [Google Scholar] [CrossRef]
- Gleeson, M.; McNicholas, W.T. Bidirectional relationships of comorbidity with obstructive sleep apnoea. Eur. Respir. Rev. 2022, 31, 164. [Google Scholar] [CrossRef] [PubMed]
- Yaggi, H.K.; Concato, J.; Kernan, W.N.; Lichtman, J.H.; Brass, L.M.; Mohsenin, V. Obstructive sleep apnea as a risk factor for stroke and death. N. Engl. J. Med. 2005, 353, 2034–2041. [Google Scholar] [CrossRef] [PubMed]
- Terán-Santos, J.; Jiménez-Gómez, A.; Cordero-Guevara, J. The association between sleep apnea and the risk of traffic accidents. Cooperative Group Burgos-Santander. N. Engl. J. Med. 1999, 340, 847–851. [Google Scholar] [CrossRef]
- Young, T.; Evans, L.; Finn, L.; Palta, M. Estimation of the clinically diagnosed proportion of sleep apnea syndrome in middle-aged men and women. Sleep 1997, 20, 705–706. [Google Scholar] [CrossRef]
- Jordan, A.S.; McSharry, D.G.; Malhotra, A. Adult obstructive sleep apnoea. Lancet 2014, 383, 736–747. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, H.; Maeda, N.; Shimomura, I. Impact of hyperuricemia on chronic kidney disease and atherosclerotic cardiovascular disease. Hypertens. Res. 2022, 45, 635–640. [Google Scholar] [CrossRef]
- Zhu, C.; Sun, B.; Zhang, B.; Zhou, Z. An update of genetics, co-morbidities and management of hyperuricaemia. Clin. Exp. Pharmacol. Physiol. 2021, 48, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhang, Y.; Zeng, C. Update on the epidemiology, genetics, and therapeutic options of hyperuricemia. Am. J. Transl. Res. 2020, 12, 3167–3181. [Google Scholar] [PubMed]
- Liu, R.; Han, C.; Wu, D.; Xia, X.; Gu, J.; Guan, H.; Shan, Z.; Teng, W. Prevalence of Hyperuricemia and Gout in Mainland China from 2000 to 2014: A Systematic Review and Meta-Analysis. Biomed. Res. Int. 2015, 2015, 762820. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kang, J.; Kim, G.T. Prevalence of hyperuricemia and its associated factors in the general Korean population: An analysis of a population-based nationally representative sample. Clin. Rheumatol. 2018, 37, 2529–2538. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Pandya, B.J.; Choi, H.K. Comorbidities of gout and hyperuricemia in the US general population: NHANES 2007–2008. Am. J. Med. 2012, 125, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Eun, Y.; Han, K.D.; Kim, D.H.; Kim, I.Y.; Park, E.J.; Lee, S.; Cha, H.S.; Koh, E.M.; Lee, J.; Kim, H. Association between anemia and hyperuricemia: Results from the Korean National Health and Nutrition Examination Survey. Sci. Rep. 2019, 9, 19067. [Google Scholar] [CrossRef] [PubMed]
- Chung, F.; Yegneswaran, B.; Liao, P.; Chung, S.A.; Vairavanathan, S.; Islam, S.; Khajehdehi, A.; Shapiro, C.M. STOP questionnaire: A tool to screen patients for obstructive sleep apnea. Anesthesiology 2008, 108, 812–821. [Google Scholar] [CrossRef]
- Jeon, H.J.; Bang, Y.R.; Yoon, I.Y. A validation study on three screening questionnaires for obstructive sleep apnea in a Korean community sample. Sleep Breath. 2019, 23, 969–977. [Google Scholar] [CrossRef]
- Seo, H.Y.; Mun, C.Y.; Park, C.Y.; Bin Choi, S.; Hwang, J.H.; Lee, J.H.; Yoon, H. The relationship between hyperuricemia and anemia and metabolic syndrome in Korean adults: The Korea National Health and Nutrition Examination Survey 2019. Prim Care Diabetes 2023, 17, 91–97. [Google Scholar] [CrossRef]
- Prabhakar, N.R.; Peng, Y.J.; Nanduri, J. Hypoxia-inducible factors and obstructive sleep apnea. J. Clin. Investig. 2020, 130, 5042–5051. [Google Scholar] [CrossRef]
- Suzuki, Y.J.; Jain, V.; Park, A.M.; Day, R.M. Oxidative stress and oxidant signaling in obstructive sleep apnea and associated cardiovascular diseases. Free Radic. Biol. Med. 2006, 40, 1683–1692. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Nishimura, M.; Shibuya, E.; Makita, H.; Tsujino, I.; Miyamoto, K.; Kawakami, Y. Tissue hypoxia in sleep apnea syndrome assessed by uric acid and adenosine. Chest 2002, 122, 1686–1694. [Google Scholar] [CrossRef]
- Jeong, K.Y.; Sim, J.J.; Park, M.; Kim, H.M. Accumulation of poly (adenosine diphosphate-ribose) by sustained supply of calcium inducing mitochondrial stress in pancreatic cancer cells. World J. Gastroenterol. 2022, 28, 3422–3434. [Google Scholar] [CrossRef]
- Hirotsu, C.; Tufik, S.; Guindalini, C.; Mazzotti, D.R.; Bittencourt, L.R.; Andersen, M.L. Association between uric acid levels and obstructive sleep apnea syndrome in a large epidemiological sample. PLoS ONE 2013, 8, e66891. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Min, M.; Sun, C.; Cheng, C.; Zhang, Y.; Liang, M.; Rizeq, F.K.; Sun, Y. A meta-analysis of the association between gout, serum uric acid level, and obstructive sleep apnea. Sleep Breath 2019, 23, 1047–1057. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Lv, T.; Lv, X.; Wan, F.; Zhou, H.; Wang, X.; Zhang, L. Association of serum uric acid with all-cause and cardiovascular mortality in obstructive sleep apnea. Sci. Rep. 2023, 13, 19606. [Google Scholar] [CrossRef]
- Zeng, Z.; Jin, T.; Ni, J.; Huang, L.; Xie, Y.; He, W.; Zhang, L.; Ding, C.; Cen, H. Assessing the causal associations of obstructive sleep apnea with serum uric acid levels and gout: A bidirectional two-sample Mendelian randomization study. Semin. Arthritis Rheum. 2022, 57, 152095. [Google Scholar] [CrossRef]
- Bartziokas, K.; Papaioannou, A.I.; Haniotou, A.; Nena, E.; Kostikas, K.; Steiropoulos, P. Serum uric acid and arterial lactate levels in patients with obstructive sleep apnea syndrome: The effect of CPAP treatment. Postgrad. Med. 2021, 133, 518–524. [Google Scholar] [CrossRef]
- Sahebjani, H. Changes in urinary uric acid excretion in obstructive sleep apnea before and after therapy with nasal continuous positive airway pressure. Chest 1998, 113, 1604–1608. [Google Scholar] [CrossRef] [PubMed]
- Etindele Sosso, F.A.; Matos, E. Socioeconomic disparities in obstructive sleep apnea: A systematic review of empirical research. Sleep Breath. 2021, 25, 1729–1739. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.J.; Piantadosi, C.; Appleton, S.L.; Hill, C.L.; Visvanathan, R.; Wilson, D.H.; McEvoy, R.D. Investigating obstructive sleep apnoea: Will the health system have the capacity to cope? A population study. Aust. Health Rev. 2012, 36, 424–429. [Google Scholar] [CrossRef]
- Petrovic, D.; Haba-Rubio, J.; Carmeli, C.; Vollenweider, P.; Heinzer, R.; Stringhini, S. Social inequalities in sleep-disordered breathing: Evidence from the CoLaus|HypnoLaus study. J. Sleep Res. 2019, 28, e12799. [Google Scholar] [CrossRef] [PubMed]
- Tarasiuk, A.; Greenberg-Dotan, S.; Simon, T.; Tal, A.; Oksenberg, A.; Reuveni, H. Low socioeconomic status is a risk factor for cardiovascular disease among adult obstructive sleep apnea syndrome patients requiring treatment. Chest 2006, 130, 766–773. [Google Scholar] [CrossRef] [PubMed]
- Dashzeveg, S.; Oka, Y.; Purevtogtokh, M.; Tumurbaatar, E.; Lkhagvasuren, B.; Luvsannorov, O.; Boldbaatar, D. Obstructive Sleep Apnea in a Clinical Population: Prevalence, Predictive Factors, and Clinical Characteristics of Patients Referred to a Sleep Center in Mongolia. Int. J. Environ. Res. Public Health 2021, 18, 12032. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.Y.; Chen, P.Y.; Chuang, L.P.; Chen, N.H.; Tu, Y.K.; Hsieh, Y.J.; Wang, Y.C.; Guilleminault, C. Diagnostic accuracy of the Berlin questionnaire, STOP-BANG, STOP, and Epworth sleepiness scale in detecting obstructive sleep apnea: A bivariate meta-analysis. Sleep Med. Rev. 2017, 36, 57–70. [Google Scholar] [CrossRef]
- Nagappa, M.; Liao, P.; Wong, J.; Auckley, D.; Ramachandran, S.K.; Memtsoudis, S.; Mokhlesi, B.; Chung, F. Validation of the STOP-Bang Questionnaire as a Screening Tool for Obstructive Sleep Apnea among Different Populations: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0143697. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Total (n = 11,981) | STOP-Bang (≤2) (n = 7409) | STOP-Bang (≥3) (n = 4572) | p Value |
|---|---|---|---|---|
| Age (Mean ± SD) | 59.9 ± 11.7 | 57.7 ± 11.8 | 63.4 ± 10.6 | <0.001 |
| 40–49 | 2853 (23.8) | 2336 (31.5) | 517 (11.3) | <0.001 |
| 50–59 | 3074 (25.7) | 1909 (25.8) | 1165 (25.5) | |
| 60–69 | 3139 (26.2) | 1709 (23.1) | 1430 (31.3) | |
| ≥70 | 2915 (24.3) | 1455 (19.6) | 1460 (31.9) | |
| Men (n, %) | 5206 (43.5) | 1961 (26.5) | 3245 (71.0) | <0.001 |
| Smoking history (%) | ||||
| Never | 7143 (59.7) | 5357 (72.4) | 1786 (39.1) | <0.001 |
| Former | 3017 (25.2) | 1196 (16.2) | 1821 (39.9) | |
| Current | 1807 (15.1) | 849 (11.5) | 958 (21.0) | |
| BMI (%) | ||||
| <18.5 | 314 (2.6) | 256 (3.5) | 58 (1.3) | <0.001 |
| 18.5–24.9 | 7170 (59.8) | 5037 (68.0) | 2133 (46.7) | |
| 25.0–29.9 | 3843 (32.1) | 1992 (26.9) | 1851 (40.5) | |
| ≥30 | 654 (5.5) | 124 (1.7) | 530 (11.6) | |
| Medical history | ||||
| Hypertension | 4081 (34.1) | 1186 (16.0) | 2895 (63.3) | <0.001 |
| Hyperlipidemia | 3469 (29.0) | 1648 (22.2) | 1821 (39.8) | <0.001 |
| Stroke | 369 (3.1) | 144 (1.9) | 225 (4.9) | <0.001 |
| Myocardial infarct or angina | 524 (4.4) | 193 (2.6) | 331 (7.2) | <0.001 |
| Diabetes | 1700 (14.2) | 708 (9.6) | 992 (21.7) | <0.001 |
| Chronic kidney disease | 179 (1.5) | 78 (1.1) | 101 (2.2) | <0.001 |
| Gout | 286 (2.4) | 81 (1.1) | 205 (4.5) | <0.001 |
| Household income | ||||
| Q1 | 2633 (22.1) | 1430 (19.4) | 1203 (26.4) | <0.001 |
| Q2 | 3016 (25.3) | 1813 (24.6) | 1203 (26.4) | |
| Q3 | 3033 (25.4) | 1965 (26.6) | 1068 (23.4) | |
| Q4 | 3254 (27.3) | 2171 (29.4) | 1083 (23.8) |
| Variables | Univariate Analysis OR (95% CI) | p Value | Multivariate Analysis OR (95% CI) | p Value |
|---|---|---|---|---|
| Age | ||||
| 40–49 | Ref. | Ref. | ||
| 50–59 | 2.80 (2.44–3.20) | <0.001 | 4.71 (3.98–5.59) | <0.001 |
| 60–69 | 3.53 (3.10–4.02) | <0.001 | 5.47 (4.58–6.54) | <0.001 |
| ≥70 | 3.70 (3.23–4.23) | <0.001 | 6.61 (5.48–7.96) | <0.001 |
| Men (n, %) | 6.62 (6.02–7.27) | <0.001 | 10.25 (8.68–12.10) | <0.001 |
| Smoking history (%) | ||||
| Never | Ref. | Ref. | ||
| Former | 4.50 (4.05–5.01) | <0.001 | 1.23 (1.04–1.46) | 0.016 |
| Current | 3.34 (2.94–3.79) | <0.001 | 1.20 (0.98–1.46) | 0.073 |
| BMI (%) | ||||
| <18.5 | Ref. | Ref. | ||
| 18.5–24.9 | 1.83 (1.27–2.62) | 0.001 | 1.73 (1.17–2.56) | 0.006 |
| 25.0–29.9 | 4.34 (3.01–6.25) | <0.001 | 3.98 (2.67–5.94) | <0.001 |
| ≥30 | 20.93 (13.88–31.57) | <0.001 | 53.80 (34.06–84.99) | <0.001 |
| Medical history | ||||
| Hyperlipidemia | 2.55 (2.31–2.81) | <0.001 | 2.50 (2.19–2.86) | <0.001 |
| Stroke | 2.71 (2.13–3.43) | <0.001 | 1.59 (1.19–2.12) | 0.002 |
| Myocardial infarct or angina | 3.01 (2.40–3.79) | <0.001 | 1.44 (1.08–1.91) | 0.012 |
| Diabetes | 2.64 (2.34–2.99) | <0.001 | 1.33 (1.14–1.55) | 0.000 |
| Chronic kidney disease | 1.99 (1.34–2.96) | 0.001 | 2.25 (1.40–3.61) | 0.001 |
| Gout | 3.98 (2.98–5.31) | <0.001 | 1.56 (1.14–2.15) | 0.006 |
| Household income | ||||
| Q1 | Ref. | Ref. | ||
| Q2 | 0.80 (0.70–0.91) | 0.001 | 0.87 (0.73–1.03) | 0.111 |
| Q3 | 0.66 (0.59–0.74) | <0.001 | 0.76 (0.65–0.89) | 0.001 |
| Q4 | 0.66 (0.59–0.74) | <0.001 | 0.76 (0.64–0.90) | 0.002 |
| Hyperuricemia | 2.01 (1.78–2.27) | <0.001 | 1.30 (1.11–1.53) | 0.001 |
| Before Propensity Score Matching | After Propensity Score Matching | |||||
|---|---|---|---|---|---|---|
| Variables | Low OSA Risk (n = 7409) | High OSA Risk (n = 4572) | SMD | Low OSA Risk (n = 3408) | High OSA Risk (n = 3408) | SMD |
| Body mass index | 23.4 ± 3.0 | 25.5 ± 3.6 | 2.061 | 24.6 ± 3.0 | 24.8 ± 3.5 | 0.178 |
| Age | 58.6 ± 12.2 | 63.6 ± 10.7 | 4.979 | 62.4 ± 12.5 | 62.6 ± 10.5 | 0.191 |
| Neck circumference | 33.8 ± 2.8 | 37.2 ± 3.2 | 3.374 | 35.8 ± 2.6 | 36.2 ± 2.9 | 0.397 |
| Male gender (n, %) | 1961 (26.5) | 3245 (71.0) | −0.448 | 1903 (55.8) | 2115 (62.1) | −0.062 |
| Variables | Univariate Analysis OR (95% CI) | p Value | Multivariate Analysis OR (95% CI) | p Value |
|---|---|---|---|---|
| Snoring | 18.78 (15.58–22.63) | <0.001 | 86.99 (62.73–120.65) | <0.001 |
| Tiredness | 10.92 (9.56–12.47) | <0.001 | 63.97 (47.93–85.38) | <0.001 |
| Observed apnea | 29.79 (20.60–43.08) | <0.001 | 132.30 (80.13–218.45) | <0.001 |
| Hypertension | 6.79 (6.09–7.58) | <0.001 | 68.08 (51.50–89.98) | <0.001 |
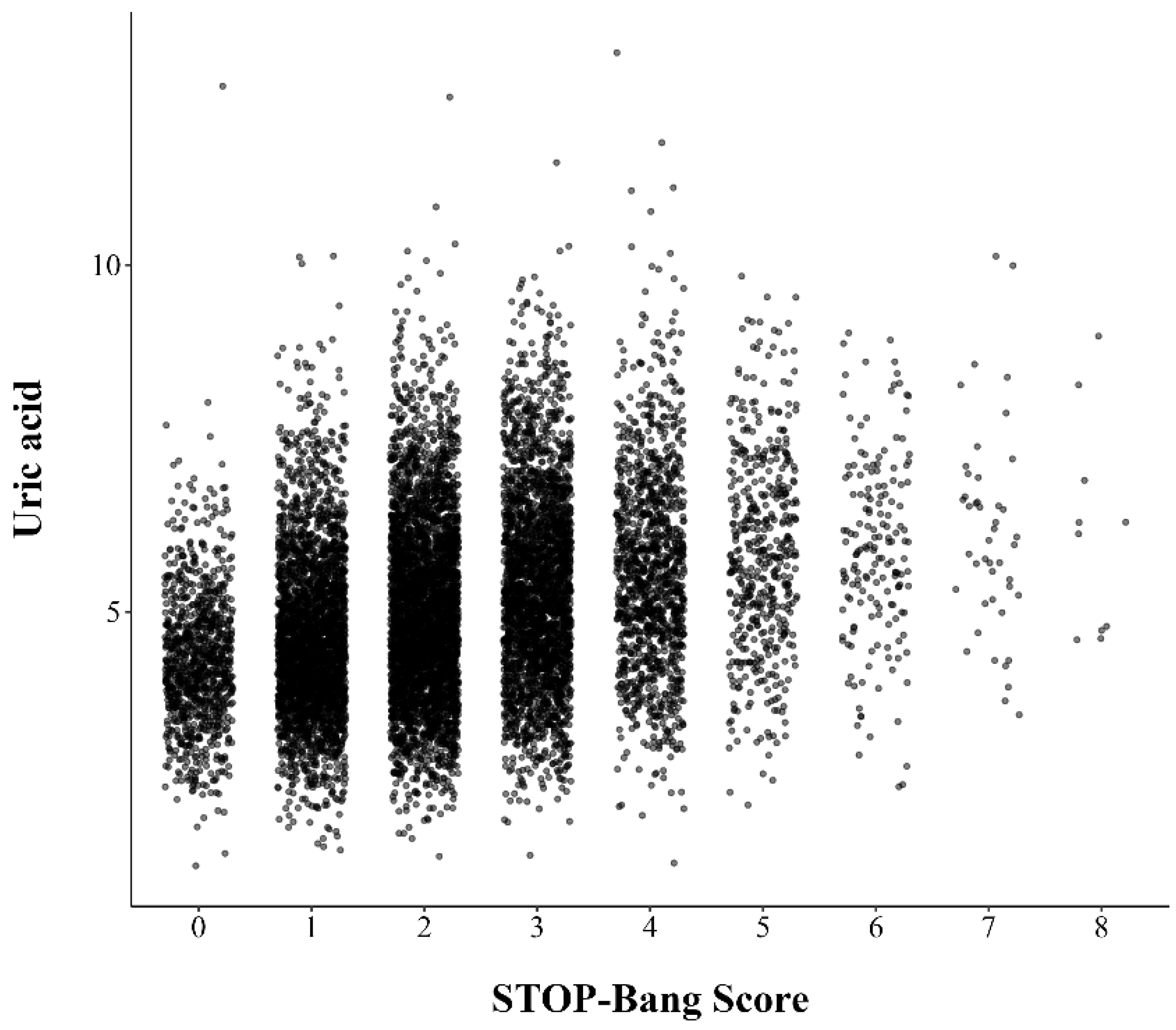
| Uric acid level | 1.06 (1.02–1.09) | 0.003 | 1.36 (1.28–1.44) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.-L.; Lim, J.; Lee, J.-H. The Association of Serum Uric Acid with Risk of Obstructive Sleep Apnea: The Korean National Health and Nutrition Examination Survey 2019–2021. J. Pers. Med. 2024, 14, 532. https://doi.org/10.3390/jpm14050532
Park S-L, Lim J, Lee J-H. The Association of Serum Uric Acid with Risk of Obstructive Sleep Apnea: The Korean National Health and Nutrition Examination Survey 2019–2021. Journal of Personalized Medicine. 2024; 14(5):532. https://doi.org/10.3390/jpm14050532
Chicago/Turabian StylePark, Su-Lim, Jihye Lim, and Ji-Ho Lee. 2024. "The Association of Serum Uric Acid with Risk of Obstructive Sleep Apnea: The Korean National Health and Nutrition Examination Survey 2019–2021" Journal of Personalized Medicine 14, no. 5: 532. https://doi.org/10.3390/jpm14050532
APA StylePark, S.-L., Lim, J., & Lee, J.-H. (2024). The Association of Serum Uric Acid with Risk of Obstructive Sleep Apnea: The Korean National Health and Nutrition Examination Survey 2019–2021. Journal of Personalized Medicine, 14(5), 532. https://doi.org/10.3390/jpm14050532