
Characterization of Homicides in Mexico: Analysis of 2015–2022

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Description
2.2. Statistical Analysis
2.3. Ethical Considerations
3. Results
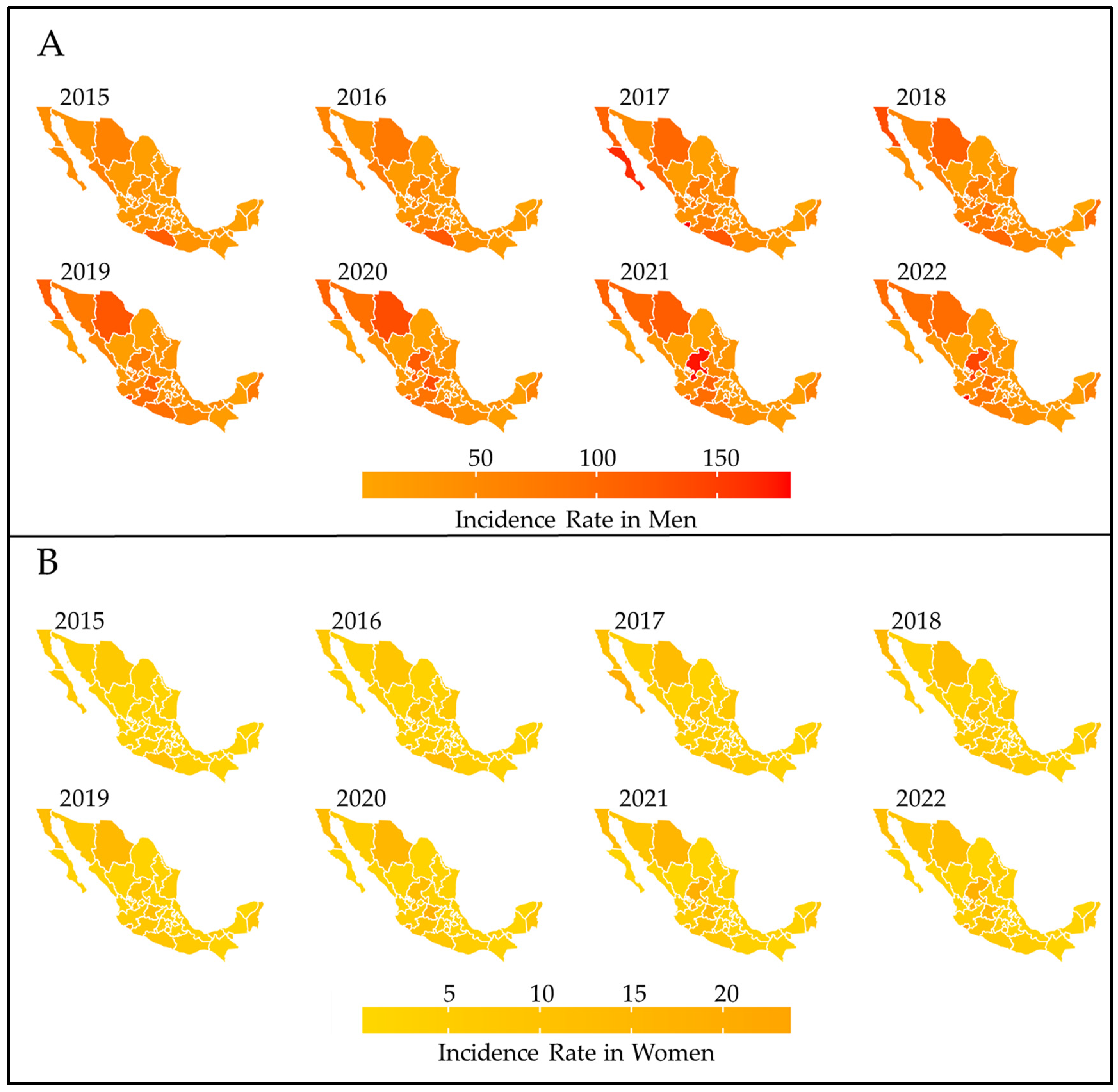
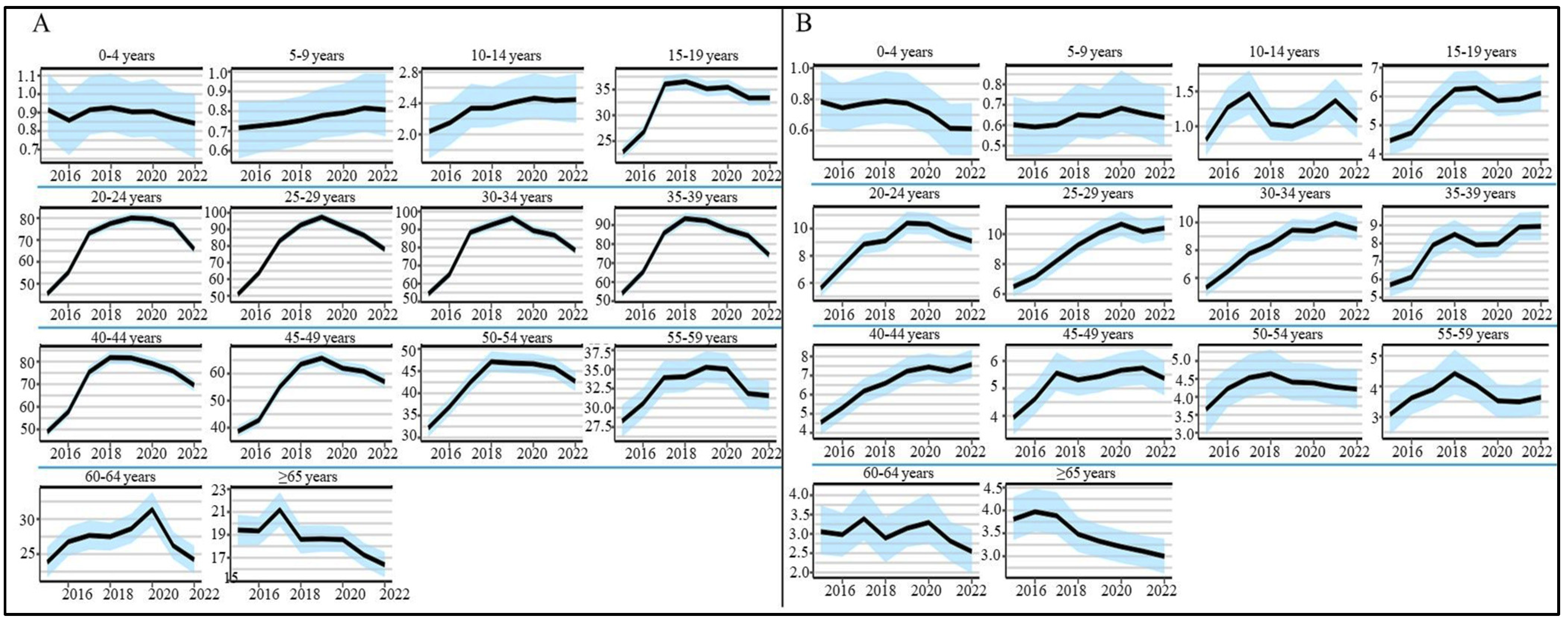
3.1. Mortality by Sex According to Age Groups
3.2. Sociodemographic Factors Associated with Homicides
3.2.1. Age
3.2.2. Occupation
3.2.3. Education
3.2.4. Marital Status
3.2.5. Place of Occurrence
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations Peace, Justice and Strong Institutions. Available online: https://www.un.org/sustainabledevelopment/peace-justice/ (accessed on 26 March 2024).
- Centers for Disease Control and Prevention. The Public Health Approach to Violence Prevention|Violence Prevention|Injury Center|CDC. Available online: https://www.cdc.gov/violenceprevention/about/publichealthapproach.html (accessed on 26 March 2024).
- American Public Health Association. Violence Is a Public Health Issue: Public Health Is Essential to Understanding and Treating Violence in the U.S. Available online: https://www.apha.org/policies-and-advocacy/public-health-policy-statements/policy-database/2019/01/28/violence-is-a-public-health-issue (accessed on 26 March 2024).
- Gebo, E. Intersectoral Violence Prevention: The Potential of Public Health–Criminal Justice Partnerships. Health Promot. Int. 2022, 37, daac062. [Google Scholar] [CrossRef] [PubMed]
- Cervantes, A.; Jhunjhunwala, R.; Castañeda Alcántara, I.D.; Elizundia Cisneros, M.E.; Ringel, R.; Cortes Rodriguez, A.; Del Valle, D.; Hill, S.; Meara, J.G.; Uribe-Leitz, T. Estimating the Economic Impact of Interpersonal Violence in Mexico in 2021: Projecting Three Hypothetical Scenarios for 2030. Rev. Panam. Salud Pública 2023, 47, e39. [Google Scholar] [CrossRef] [PubMed]
- Poveda, A.C.; Martínez, C.I.P. Violence and Economic Development in Mexico: A Panel Data Cointegration Approach. Dev. Stud. Res. 2023, 10, 2169733. [Google Scholar] [CrossRef]
- World Health Organization. Violence Prevention through Multisectoral Collaboration: An International Version of the Collaboration Multiplier Tool to Prevent Interpersonal Violence. Available online: https://www.who.int/publications/m/item/violence-prevention-through-multisectoral-collaboration (accessed on 26 March 2024).
- Sheats, K.J.; Irving, S.M.; Mercy, J.A.; Simon, T.R.; Crosby, A.E.; Ford, D.C.; Merrick, M.T.; Annor, F.B.; Morgan, R.E. Violence-Related Disparities Experienced by Black Youth and Young Adults: Opportunities for Prevention. Am. J. Prev. Med. 2018, 55, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Fenimore, D.M.; Perez, N.; Jennings, W.G. Early Risk Factors for Violence among Hispanic Youth: Evidence from a Systematic Review. Aggress. Violent Behav. 2019, 49, 101305. [Google Scholar] [CrossRef]
- UNODC. Global Study on Homicide 2023. Available online: https://www.unodc.org/documents/data-and-analysis/gsh/2023/Global_study_on_homicide_2023_web.pdf (accessed on 23 April 2024).
- Aburto, J.M.; Beltrán-Sánchez, H. Upsurge of Homicides and Its Impact on Life Expectancy and Life Span Inequality in Mexico, 2005–2015. Am. J. Public Health 2019, 109, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Blair, K.J.; De Virgilio, M.; Dissak-Delon, F.N.; Dang, L.E.; Christie, S.A.; Carvalho, M.; Oke, R.; Mbianyor, M.A.; Hubbard, A.E.; Etoundi, A.M.; et al. Associations between Social Determinants of Health and Interpersonal Violence-Related Injury in Cameroon: A Cross-Sectional Study. BMJ Glob. Health 2022, 7, e007220. [Google Scholar] [CrossRef]
- Wanzinack, C.; Signorelli, M.C.; Reis, C. Violence and Social Determinants of Health in Brazil: Association between Homicides, Urbanization, Population, Inequality, and Development. Cad. Saúde Pública 2022, 38, e00282621. [Google Scholar] [CrossRef]
- Soares Filho, A.M.; Duarte, E.C.; Merchan-Hamann, E. Tendência e Distribuição Da Taxa de Mortalidade Por Homicídios Segundo Porte Populacional Dos Municípios Do Brasil, 2000 e 2015. Ciênc. Saúde Coletiva 2020, 25, 1147–1156. [Google Scholar] [CrossRef]
- INEGI. Estadísticas de Defunciones Registradas. Comunicado de Prensa 2023. Available online: https://www.inegi.org.mx/contenidos/saladeprensa/boletines/2023/EDR/EDR2022.pdf (accessed on 23 April 2024).
- Jasso Vargas, R. Decrease in Mexico’s life expectancy due to multiple homicides: The murder of women adjacent to the homicide of one or more men. Salud Colect. 2023, 19, e4247. [Google Scholar] [CrossRef]
- Flores-Martínez, I.; Phillips, M. The Perfect Storm. An Analysis of the Processes That Increase Lethal Violence in Mexico after 2006. Trends Organ. Crime 2022, 25, 58–83. [Google Scholar] [CrossRef]
- Gamlin, J. Violence and Homicide in Mexico: A Global Health Issue. Lancet 2015, 385, 605–606. [Google Scholar] [CrossRef] [PubMed]
- Velasco-Calderón, O.; Castañeda, A.; Gutiérrez, J.P. Trend of inequalities in homicides in Mexico for the period from 2000 to 2021: Longitudinal ecological analysis. Rev. Panam. Salud Pública 2023, 47, 1. [Google Scholar] [CrossRef] [PubMed]
- Bureau of Justice Assistance Community. Based Violence Intervention and Prevention Initiative (CVIPI)|Overview|Bureau of Justice Assistance. Available online: https://bja.ojp.gov/program/community-violence-intervention/overview (accessed on 26 March 2024).
- Hohl, B.C.; Kondo, M.C.; Kajeepeta, S.; MacDonald, J.M.; Theall, K.P.; Zimmerman, M.A.; Branas, C.C. Creating Safe And Healthy Neighborhoods With Place-Based Violence Interventions. Health Aff. 2019, 38, 1687–1694. [Google Scholar] [CrossRef]
- Butts, J.A.; Roman, C.G.; Bostwick, L.; Porter, J.R. Cure Violence: A Public Health Model to Reduce Gun Violence. Annu. Rev. Public Health 2015, 36, 39–53. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.C.; Andreyeva, E.; South, E.C.; MacDonald, J.M.; Branas, C.C. Neighborhood Interventions to Reduce Violence. Annu. Rev. Public Health 2018, 39, 253–271. [Google Scholar] [CrossRef] [PubMed]
- Secretaría de Salud. Manual de Llenado del Certificado de Defunción y Certificado Fetal Modelo 2022. Available online: https://intranet.saludtlax.gob.mx/documentos/ManualesSistemas/seed/Manual.Llenado.CD_CMF_2022.pdf (accessed on 23 April 2024).
- Proyecciones de la Población de México y de las Entidades Federativas, 2020–2070. Available online: https://datos.gob.mx/busca/dataset/proyecciones-de-la-poblacion-de-mexico-y-de-las-entidades-federativas-2020-2070 (accessed on 27 March 2024).
- INEGI Esperanza de Vida al Nacimiento por Entidad Federativa según Sexo, Serie Anual de 2010 a 2024. Available online: https://www.inegi.org.mx/app/tabulados/interactivos/?pxq=Mortalidad_Mortalidad_09_b87a4bf1-9b47-442a-a5fc-ee5c65e37648 (accessed on 27 March 2024).
- Delajara, M.; Dositeo, G. Intergenerational Social Mobility in Mexico and Its Regions. Available online: https://ceey.org.mx/wp-content/uploads/2018/06/06-Delajara-Gra%C3%B1a-2017.pdf (accessed on 27 March 2024).
- Índices de Marginación 2020. Available online: http://www.gob.mx/conapo/documentos/indices-de-marginacion-2020-284372 (accessed on 27 March 2024).
- Donegan, C. Surveil: Time Series Models for Disease Surveillance 2023. Available online: https://cran.r-project.org/web/packages/surveil/surveil.pdf (accessed on 27 March 2024).
- Chudasama, Y.V.; Khunti, K.; Gillies, C.L.; Dhalwani, N.N.; Davies, M.J.; Yates, T.; Zaccardi, F. Estimates of Years of Life Lost Depended on the Method Used: Tutorial and Comparative Investigation. J. Clin. Epidemiol. 2022, 150, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Gary, S. Violence Is a Contagious Disease. Available online: https://www.ncbi.nlm.nih.gov/books/NBK207245/ (accessed on 27 March 2024).
- Gary, S.; Ransford, C.; Zvetina, D. How the Health Sector Can Reduce Violence by Treating It as a Contagion. AMA J. Ethics 2018, 20, 47–55. [Google Scholar]
- Institute for Health Metrics and Evaluation GBD Results. Available online: https://vizhub.healthdata.org/gbd-results (accessed on 14 March 2024).
- Aburto, J.M.; Di Lego, V.; Riffe, T.; Kashyap, R.; Van Raalte, A.; Torrisi, O. A Global Assessment of the Impact of Violence on Lifetime Uncertainty. Sci. Adv. 2023, 9, eadd9038. [Google Scholar] [CrossRef]
- World Health Organization. Preventing Injuries and Violence: An Overview. Available online: https://www.who.int/publications-detail-redirect/9789240047136 (accessed on 14 March 2024).
- Instituto Nacional de Estadística y Geografía. Densidad de Población por Entidad Federativa, Serie de años Censales de 1990 a 2020. Available online: https://en.www.inegi.org.mx/app/tabulados/interactivos/?pxq=Poblacion_Poblacion_07_fb7d5132-39f0-4a6c-b6f6-4cbe440e048d (accessed on 20 March 2024).
- Armstead, T.L.; Wilkins, N.; Nation, M. Structural and Social Determinants of Inequities in Violence Risk: A Review of Indicators. J. Community Psychol. 2021, 49, 878–906. [Google Scholar] [CrossRef]
- Weitzman, A. Does Increasing Women’s Education Reduce Their Risk of Intimate Partner Violence? Evidence from an Education Policy Reform. Criminology 2018, 56, 574–607. [Google Scholar] [CrossRef]
- Chappell, D.; Di Martino, V. Violence at Work, 3rd ed.; International Labour Office: Geneva, Switzerland, 2006; p. 360. [Google Scholar]
- Orraca-Romano, P. Crime exposure and educational outcomes in Mexico. Ens. Rev. Econ. 2018, 37, 177–212. [Google Scholar]
- Wilkins, N.J.; Zhang, X.; Mack, K.A.; Clapperton, A.J.; Macpherson, A.; Sleet, D.; Kresnow-Sedacca, M.J.; Ballesteros, M.F.; Newton, D.; Murdoch, J.; et al. Societal Determinants of Violent Death: The Extent to Which Social, Economic, and Structural Characteristics Explain Differences in Violence across Australia, Canada, and the United States. SSM Popul. Health 2019, 8, 100431. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, A.; Bergquist, R.; Fathi, G.; Pishgar, E.; De Melo, S.N.; Sharifi, A.; Kiani, B. Homicide Rates Are Spatially Associated with Built Environment and Socio-Economic Factors: A Study in the Neighbourhoods of Toronto, Canada. BMC Public Health 2022, 22, 1482. [Google Scholar] [CrossRef] [PubMed]
- Freire-Vargas, L. Violence as a Public Health Crisis. AMA J. Ethics 2018, 20, 25–28. [Google Scholar]
- Dahlberg, L.L.; Mercy, J.A. History of violence as a public health problem. Virtual Mentor 2009, 11, 167–172. [Google Scholar] [PubMed]
- Souama, C.; Milaneschi, Y.; Lamers, F.; Vinkers, C.H.; Giltay, E.J.; Liemburg, E.J.; Penninx, B.W.J.H. Metabolic Syndrome after Childhood Trauma: A 9-Year Longitudinal Analysis. Psychol. Med. 2023, 54, 1373–1381. [Google Scholar] [CrossRef] [PubMed]
- Ponte-González, A.D.; Guerrero-Morales, A.L.; López-Ortiz, G. Violencia hacia la mujer y su impacto en la salud. Rev. Mex. Med. Fam. 2023, 10, 117–125. [Google Scholar] [CrossRef]
- Zhong, S.; Yu, R.; Fazel, S. Drug Use Disorders and Violence: Associations with Individual Drug Categories. Epidemiol. Rev. 2020, 42, 103–116. [Google Scholar] [CrossRef]
- Smith, M.E.; Sharpe, T.L.; Richardson, J.; Pahwa, R.; Smith, D.; DeVylder, J. The Impact of Exposure to Gun Violence Fatality on Mental Health Outcomes in Four Urban U.S. Settings. Soc. Sci. Med. 2020, 246, 112587. [Google Scholar] [CrossRef]
- Jones, V.; Becote-Jackson, M.; Parnham, T.; Lewis, Q.; Ryan, L.M. Violence Prevention Through Mentoring for Youth with Emergency Department Treated Peer Assault Injuries. J. Pediatr. 2021, 6, 100064. [Google Scholar] [CrossRef] [PubMed]
- Ragavan, M.I.; Culyba, A.J.; Muhammad, F.L.; Miller, E. Supporting Adolescents and Young Adults Exposed to or Experiencing Violence During the COVID-19 Pandemic. J. Adolesc. Health 2020, 67, 18–20. [Google Scholar] [CrossRef] [PubMed]
- Hyatt, J.M.; Densley, J.A.; Roman, C.G. Social Media and the Variable Impact of Violence Reduction Interventions: Re-Examining Focused Deterrence in Philadelphia. Soc. Sci. 2021, 10, 147. [Google Scholar] [CrossRef]
- Ostermann, M.; Hashimi, S. Recidivism among People Convicted of Gun Offenses: A Call to Better Leverage Reentry Resources to Decrease Gun Violence. Justice Q. 2023, 40, 791–812. [Google Scholar] [CrossRef]
- Gobaud, A.N.; Jacobowitz, A.L.; Mehranbod, C.A.; Sprague, N.L.; Branas, C.C.; Morrison, C.N. Place-Based Interventions and the Epidemiology of Violence Prevention. Curr. Epidemiol. Rep. 2022, 9, 316–325. [Google Scholar] [CrossRef] [PubMed]
- Herrera Kelly, D.S. Local Non-Violent Strategies amid Guatemala’s Post-Accord Violence: Understanding the Potential and Limitations in Poor Urban Neighbourhoods. Peacebuilding 2023, 3, 1–18. [Google Scholar] [CrossRef]
- Prieto-Curiel, R.; Campedelli, G.M.; Hope, A. Reducing cartel recruitment is the only way to lower violence in Mexico. Science 2023, 381, 1312–1316. [Google Scholar] [CrossRef]
- Organizacion de las Naciones Unidas México: El Oscuro Hito de 100,000 Desapariciones|ONU-DH. Available online: https://hchr.org.mx/comunicados/mexico-el-oscuro-hito-de-100000-desapariciones-refleja-un-patron-de-impunidad-advierten-expertos-de-la-onu/ (accessed on 25 March 2024).
- Gobierno de Mexico Estadística del Registro Nacional de Personas Desaparecidas y No Localizadas. Available online: https://versionpublicarnpdno.segob.gob.mx/Dashboard/Sociodemografico (accessed on 25 March 2024).
- El Cambiante Panorama de la Delincuencia Organizada. Available online: https://www.indicedepazmexico.org/el-cambiante-panorama-de-la-delincuencia-organizada (accessed on 28 March 2024).
- Impunidad en Homicidio Doloso y Feminicidio 2022. Available online: http://www.impunidadcero.org/articulo.php?id=175&t=impunidad-en-homicidio-doloso-y-feminicidio-2022 (accessed on 28 March 2024).


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Men n (%) | Women n (%) | * p |
|---|---|---|---|
| Place of death | |||
| Ministry of Health hospitals | 21,694 (10.63%) | 2231 (8.82%) | <0.001 |
| Social Security hospitals | 7883 (3.86%) | 961 (3.80%) | 0.522 |
| National Defense hospitals | 135 (0.06%) | 18 (0.07%) | 0.872 |
| Private hospitals | 2843 (1.39%) | 354 (1.40%) | 0.964 |
| Home | 17,220 (8.44%) | 5621 (22.22%) | <0.001 |
| Streets and highways | 101,246 (49.65%) | 9475 (37.47%) | <0.001 |
| Not specified | 52,877 (25.93%) | 6624 (26.18%) | 0.370 |
| Marital status | |||
| Single | 85,731 (42.04%) | 11,151 (44.10%) | 0.045 |
| Married or cohabitation | 92,772 (45.49%) | 9356 (37.00%) | <0.001 |
| Separated or divorced | 8351 (4.09%) | 2330 (9.21%) | <0.001 |
| Not specified | 17,044 (8.35%) | 2447 (9.67%) | 0.014 |
| Education | |||
| None or elementary | 69,142 (33.91%) | 8207 (32.45%) | <0.001 |
| Secondary or high school | 103,587 (50.80%) | 12,464 (49.29%) | 0.045 |
| Bachelor’s degree or postgraduate | 16,891 (8.28%) | 2629 (10.39%) | <0.001 |
| Not specified | 14,278 (7.00%) | 1984 (7.84%) | 0.045 |
| Occupation | |||
| Administrative | 15,233 (7.47%) | 1300 (5.15%) | <0.001 |
| Agriculture | 21,229 (10.41%) | 315 (1.13%) | <0.001 |
| Commerce | 24,625 (12.07%) | 3040 (12.02%) | 0.811 |
| Security | 7650 (3.75%) | 742 (2.93%) | <0.001 |
| Technician | 63,177 (30.90%) | 1346 (5.32%) | <0.001 |
| Unemployed | 24,679 (12.10%) | 12,574 (49.72%) | <0.001 |
| Not specified | 47,305 (23.20%) | 5967 (23.50%) | 0.159 |
| Age Group (Men) | North Central | Center | North | Northwest | South | National |
|---|---|---|---|---|---|---|
| 0–4 | 0.82 | 1.10 | 1.04 | 0.86 | 0.53 | 0.89 |
| 5–9 | 0.86 | 0.93 | 0.69 | 0.66 | 0.56 | 0.76 |
| 10–14 | 2.24 | 2.52 | 2.58 | 2.50 | 1.85 | 2.32 |
| 15–19 | 36.09 | 29.21 | 41.15 | 44.02 | 25.27 | 32.45 |
| 20–24 | 80.50 | 59.33 | 88.94 | 87.56 | 56.77 | 69.14 |
| 25–29 | 97.26 | 68.40 | 104.46 | 99.36 | 64.98 | 80.50 |
| 30–34 | 97.13 | 70 | 107.81 | 96.04 | 64.86 | 81.43 |
| 35–39 | 96.45 | 64.93 | 106.77 | 93.51 | 67.19 | 79.64 |
| 40–44 | 84.04 | 57.26 | 95.14 | 81.13 | 63.31 | 71.20 |
| 45–49 | 66.32 | 43.90 | 73.70 | 63.10 | 51.33 | 55.66 |
| 50–54 | 45.51 | 34.27 | 53.57 | 48.38 | 43.78 | 42.56 |
| 55–59 | 34.97 | 26.54 | 40.17 | 34.92 | 34.29 | 32.56 |
| 60–64 | 26.99 | 22.75 | 33.55 | 25.48 | 29.38 | 27.02 |
| 65 or above | 18.78 | 17.34 | 18.41 | 20.90 | 20.22 | 18.67 |
| Age group (Women) | North Central | Center | North | Northwest | South | National |
| 0–4 | 0.61 | 0.78 | 1.04 | 0.83 | 0.46 | 0.72 |
| 5–9 | 0.67 | 0.63 | 0.61 | 0.78 | 0.58 | 0.63 |
| 10–14 | 1.18 | 1.14 | 1.25 | 1.30 | 0.99 | 1.14 |
| 15–19 | 7.00 | 5.28 | 6.66 | 6.44 | 4.42 | 5.65 |
| 20–24 | 9.26 | 8.42 | 12.41 | 9.08 | 6.22 | 8.78 |
| 25–29 | 10.32 | 8.73 | 12.11 | 8.55 | 6.64 | 9.05 |
| 30–34 | 8.20 | 7.98 | 11.89 | 7.80 | 6.22 | 8.27 |
| 35–39 | 8.34 | 7.24 | 10.35 | 7.13 | 6.42 | 7.74 |
| 40–44 | 6.66 | 6.07 | 8.26 | 6.03 | 5.97 | 6.51 |
| 45–49 | 5.28 | 4.72 | 6.96 | 4.93 | 4.66 | 5.20 |
| 50–54 | 4.30 | 3.80 | 5.10 | 4.15 | 4.56 | 4.29 |
| 55–59 | 3.42 | 3.69 | 3.72 | 3.34 | 4.08 | 3.71 |
| 60–64 | 3.16 | 2.86 | 3.34 | 2.45 | 3.09 | 3.01 |
| 65 or above | 3.52 | 3.61 | 3.33 | 2.29 | 3.64 | 3.47 |
| Sociodemographic Characteristics | Men OR CI (95%) | p | Women OR (CI 95%) | p |
|---|---|---|---|---|
| Sex | 6.48 (6.39–6.56) | <0.001 | Reference | |
| Age group in years | ||||
| 0–4 | Reference | Reference | ||
| 5–9 | 1.66 (1.43–1.92) | <0.001 | 1.75 (1.48–2.05) | <0.001 |
| 10–14 | 3.72 (3.31–4.18) | <0.001 | 2.51 (2.18–2.90) | <0.001 |
| 15–19 | 19.03 (17.23–21.08) | <0.001 | 7.35 (6.54–8.29) | <0.001 |
| 20–24 | 25.38 (23–28.09) | <0.001 | 8.78 (7.83–9.88) | <0.001 |
| 25–29 | 23.05 (20.89–25.51) | <0.001 | 7.23 (6.45–8.13) | <0.001 |
| 30–34 | 18.57 (16.84–20.56) | <0.001 | 5.1 (4.54–5.74) | <0.001 |
| 35–39 | 13 (11.78–14.38) | <0.001 | 3.26 (2.90–3.67) | <0.001 |
| 40–44 | 8.29 (7.51–9.18) | <0.001 | 1.763(1.56–1.98) | <0.001 |
| 45–49 | 4.53 (4.10–5.02) | <0.001 | 0.88 (0.78–0.99) | 0.038 |
| 50–54 | 2.45 (2.22–2.71) | <0.001 | 0.461 (0.40–0.52) | <0.001 |
| 55–59 | 1.27 (1.14–1.40) | <0.001 | 0.249 (0.21–0.28) | <0.001 |
| 60–64 | 0.71 (0.64–0.79) | <0.001 | 0.129 (0.11–0.14) | <0.001 |
| 65 or above | 0.16 (0.14–0.18) | <0.001 | 0.041 (0.036–0.04) | <0.001 |
| Occupation | ||||
| Agriculture | Reference | Reference | ||
| Technician | 2.89 (2.85–2.94) | <0.001 | 0.89 (0.794–1.017) | 0.085 |
| Security | 3.13 (3.05–3.22) | <0.001 | 1.86 (1.632–2.13) | <0.001 |
| Commerce | 2.66 (2.614–2.71) | <0.001 | 1.09 (0.979–1.23) | 0.114 |
| Administrative | 1.68 (1.64–1.71) | <0.001 | 0.37 (0.334–0.42) | <0.001 |
| Unemployed | 0.70 (0.69–0.71) | <0.001 | 0.13 (0.122–0.15) | <0.001 |
| Not specified | 3.48 (3.43–3.54) | <0.001 | 0.93 (0.83–1.04) | 0.222 |
| Scholarity | ||||
| Bachelor’s degree or postgraduate | Reference | Reference | ||
| None or elementary | 0.77 (0.76–0.78) | <0.001 | 0.29 (0.28–0.31) | <0.001 |
| Secondary or high school | 2.70 (2.65–2.74) | <0.001 | 1.74 (1.67–1.81) | <0.001 |
| Not specified | 2.09 (2.05–2.14) | <0.001 | 1.29 (1.22–1.37) | <0.001 |
| Marital status | ||||
| Married or cohabitation | Reference | Reference | ||
| Single | 2.7 (2.67–2.72) | <0.001 | 2.27 (2.21–2.34) | <0.001 |
| Separated or divorced | 0.282 (0.27–0.28) | <0.001 | 0.22 (0.21–0.24) | <0.001 |
| Not specified | 1.69 (1.67–1.72) | <0.001 | 1.65 (1.58–1.72) | <0.001 |
| Death location | ||||
| Private hospital | Reference | Reference | ||
| Home | 0.539 (0.51–0.56) | <0.001 | 1.508 (1.35–1.68) | <0.001 |
| Streets and highways | 41.77 (40.24–43.38) | <0.001 | 135.29 (121.89–150.67) | <0.001 |
| Ministry of health hospitals | 2.10 (2.02–2.18) | <0.001 | 2.276 (2.03–2.54) | <0.001 |
| Social security hospital | 0.50 (0.48–0.52) | <0.001 | 0.544 (0.48–0.61) | <0.001 |
| Military hospital | 0.35 (0.29–0.41) | <0.001 | 0.39 (0.23–0.60) | <0.001 |
| Not specified | 12.75 (12.28–13.24) | <0.001 | 20.12 (18.13–22.41) | <0.001 |
| Structural | ||||
| Percentage of population with education lagging | 1.018 (1.01–1.01) | <0.001 | 1.013 (1.011–1.014) | <0.001 |
| Marginalization degree | ||||
| Very Low | Reference | Reference | ||
| Low | 1.37 (1.35–1.38) | <0.001 | 1.29 (1.25–1.34) | <0.001 |
| Medium | 0.88 (0.86–0.89) | <0.001 | 0.78 (0.73–0.82) | <0.001 |
| High | 0.85 (0.84–0.87) | <0.001 | 0.772 (0.72–0.82) | <0.001 |
| Very high | 1.49 (1.45–1.53) | <0.001 | 1.374 (1.26–1.48) | <0.001 |
| Percentage of population living in poverty | 1.02 (1.001–1.003) | 0.028 | 1.002 (1.001–1.002) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Ortiz, E.; Altamirano, J.M.; Romero-Henríquez, L.F.; López-Ortiz, G. Characterization of Homicides in Mexico: Analysis of 2015–2022. Int. J. Environ. Res. Public Health 2024, 21, 617. https://doi.org/10.3390/ijerph21050617
López-Ortiz E, Altamirano JM, Romero-Henríquez LF, López-Ortiz G. Characterization of Homicides in Mexico: Analysis of 2015–2022. International Journal of Environmental Research and Public Health. 2024; 21(5):617. https://doi.org/10.3390/ijerph21050617
Chicago/Turabian StyleLópez-Ortiz, Eduardo, Juan Manuel Altamirano, Luisa Fernanda Romero-Henríquez, and Geovani López-Ortiz. 2024. "Characterization of Homicides in Mexico: Analysis of 2015–2022" International Journal of Environmental Research and Public Health 21, no. 5: 617. https://doi.org/10.3390/ijerph21050617
APA StyleLópez-Ortiz, E., Altamirano, J. M., Romero-Henríquez, L. F., & López-Ortiz, G. (2024). Characterization of Homicides in Mexico: Analysis of 2015–2022. International Journal of Environmental Research and Public Health, 21(5), 617. https://doi.org/10.3390/ijerph21050617