Sociodemographic Differences in the Dietary Quality of Food-at-Home Acquisitions and Purchases among Participants in the U.S. Nationally Representative Food Acquisition and Purchase Survey (FoodAPS)


Abstract
:1. Introduction
2. Methods
2.1. Data Source
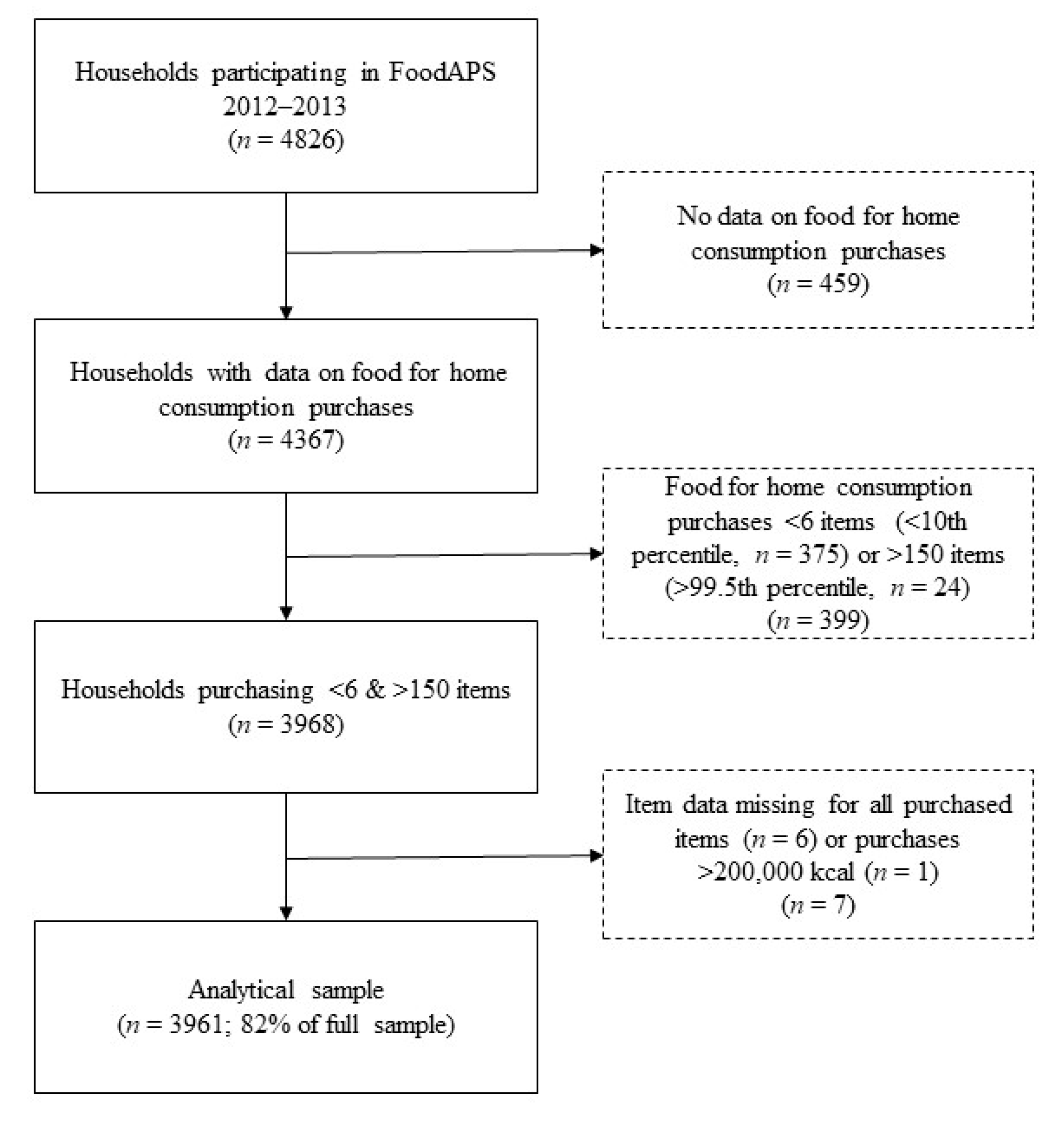
2.2. Analytical Sample
2.3. Healthy Eating Index 2015
2.4. Exposures
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Descriptive Characteristics
3.2. Unadjusted HEI-2015 Scores across Sociodemographic Groups
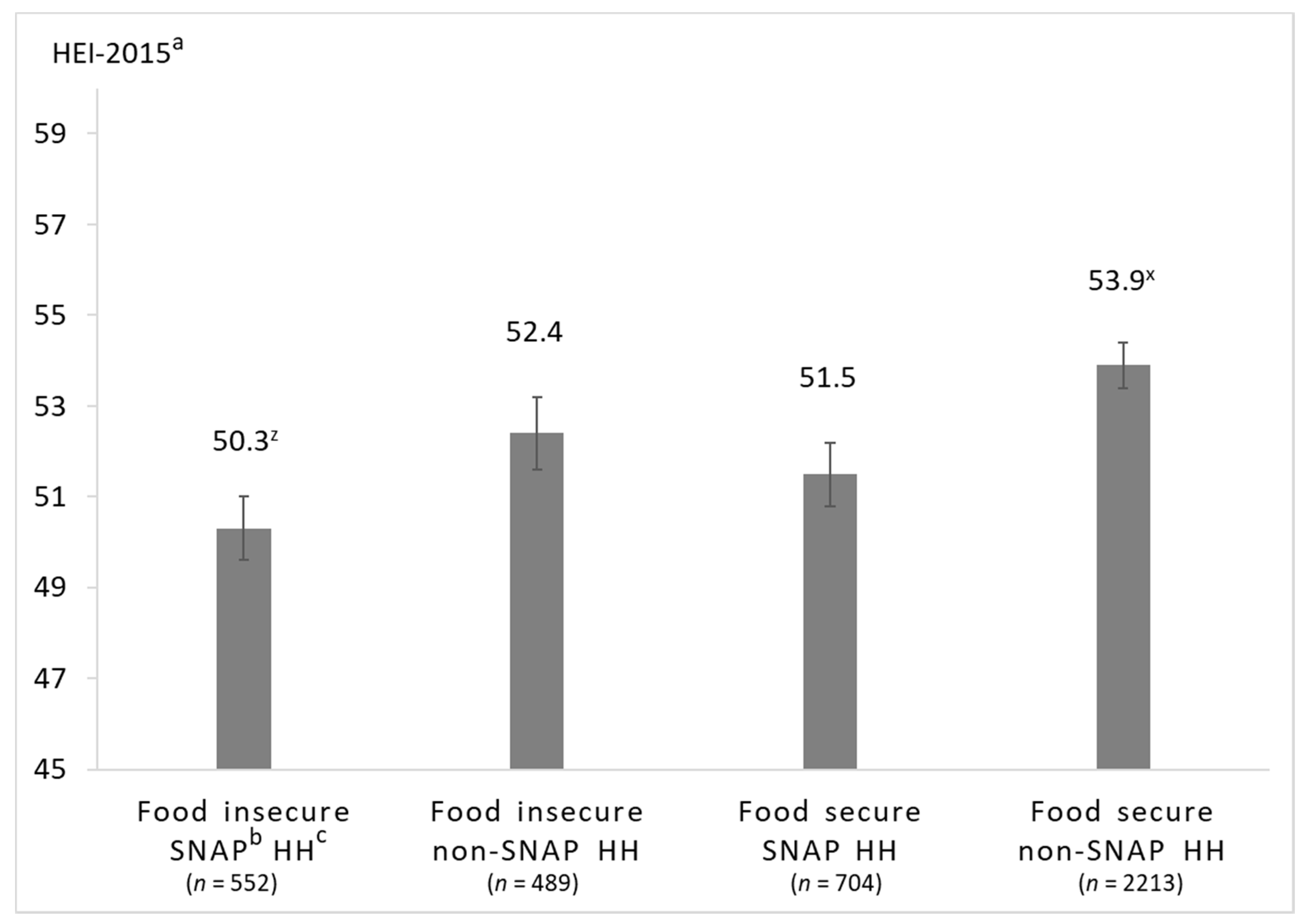
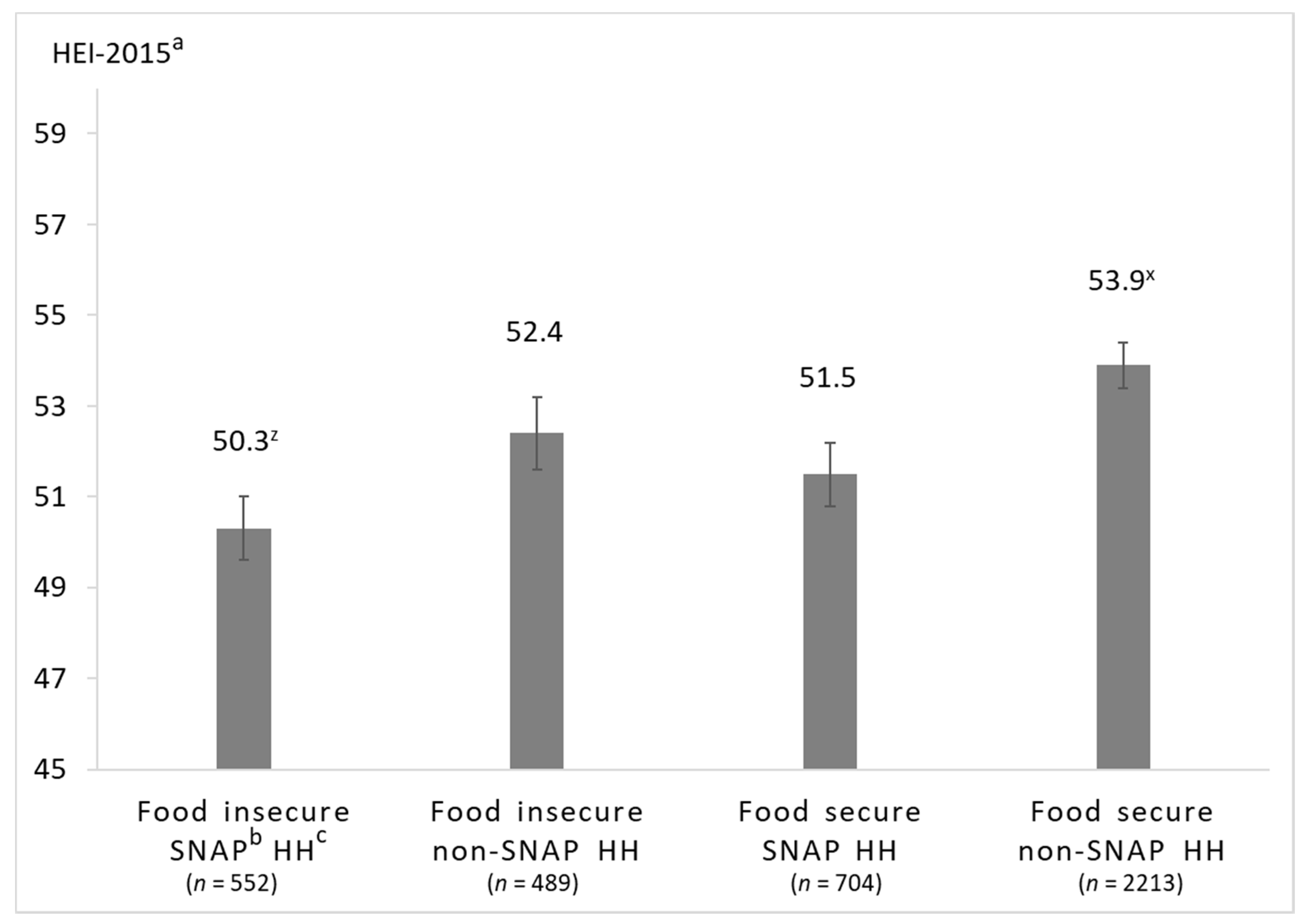
3.3. Associations between Food Security and SNAP-Participation on HEI-2015 Scores
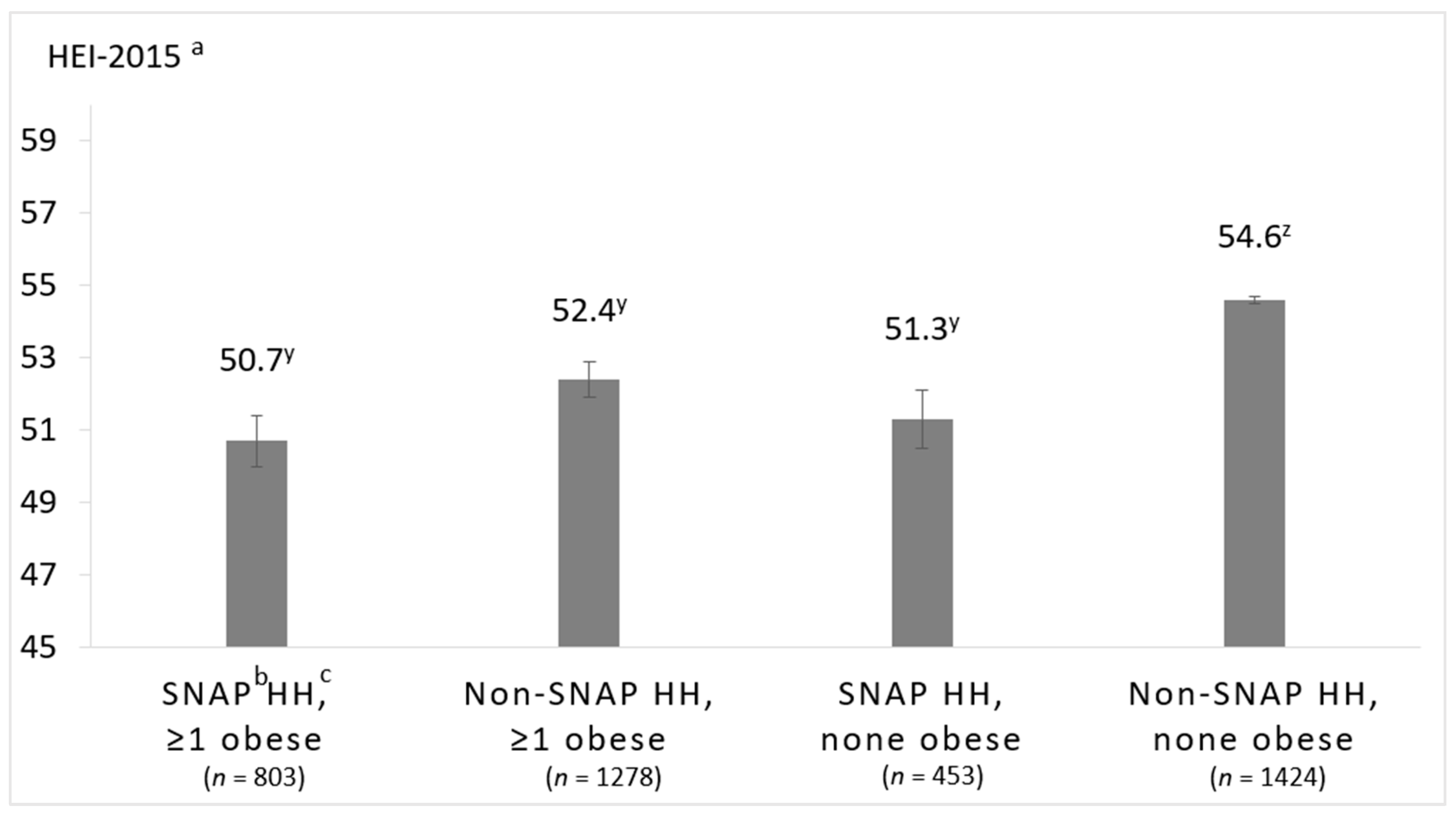
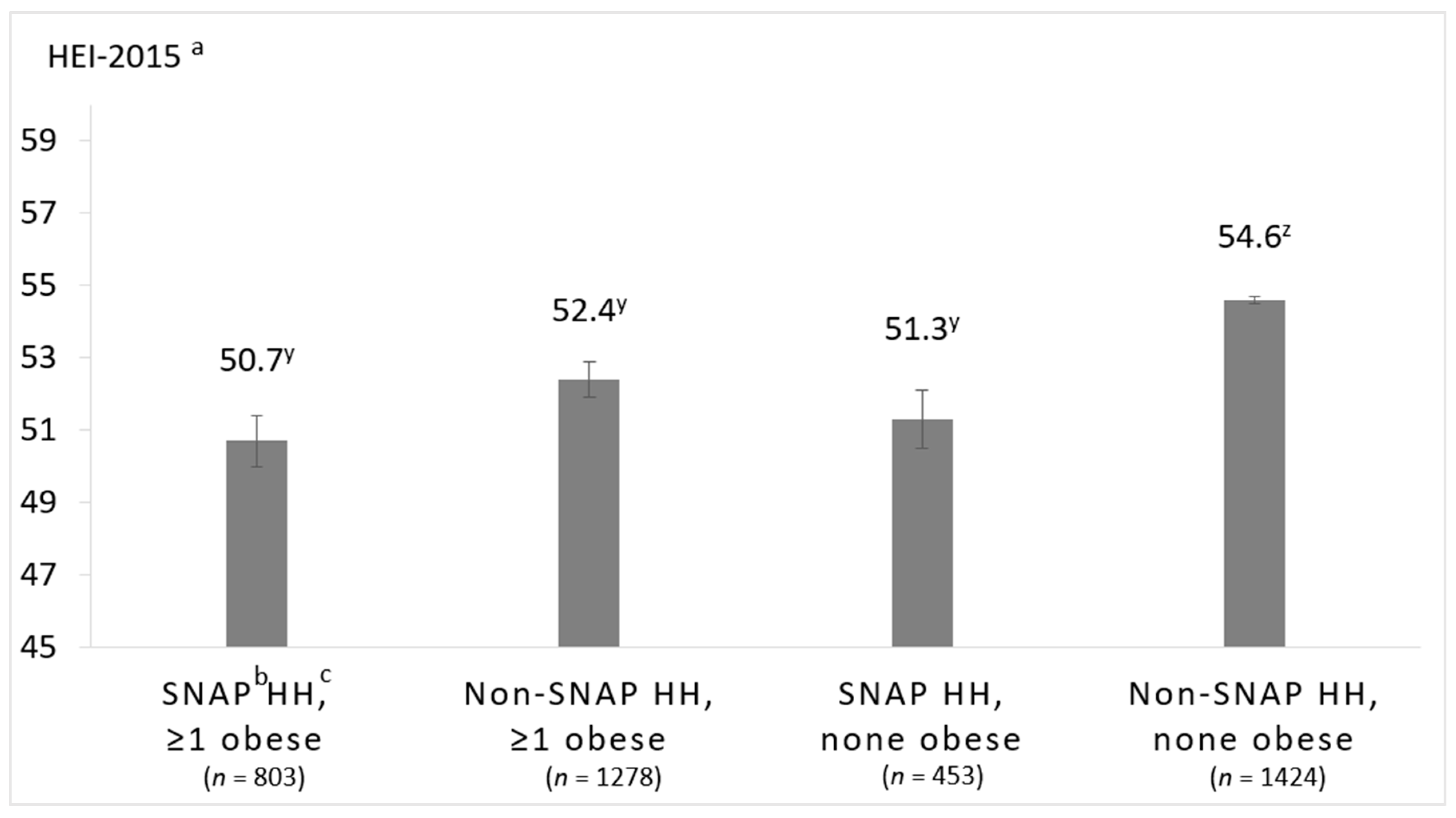
3.4. Associations between SNAP-Participation and Household-Level Obesity on HEI-2015 Scores
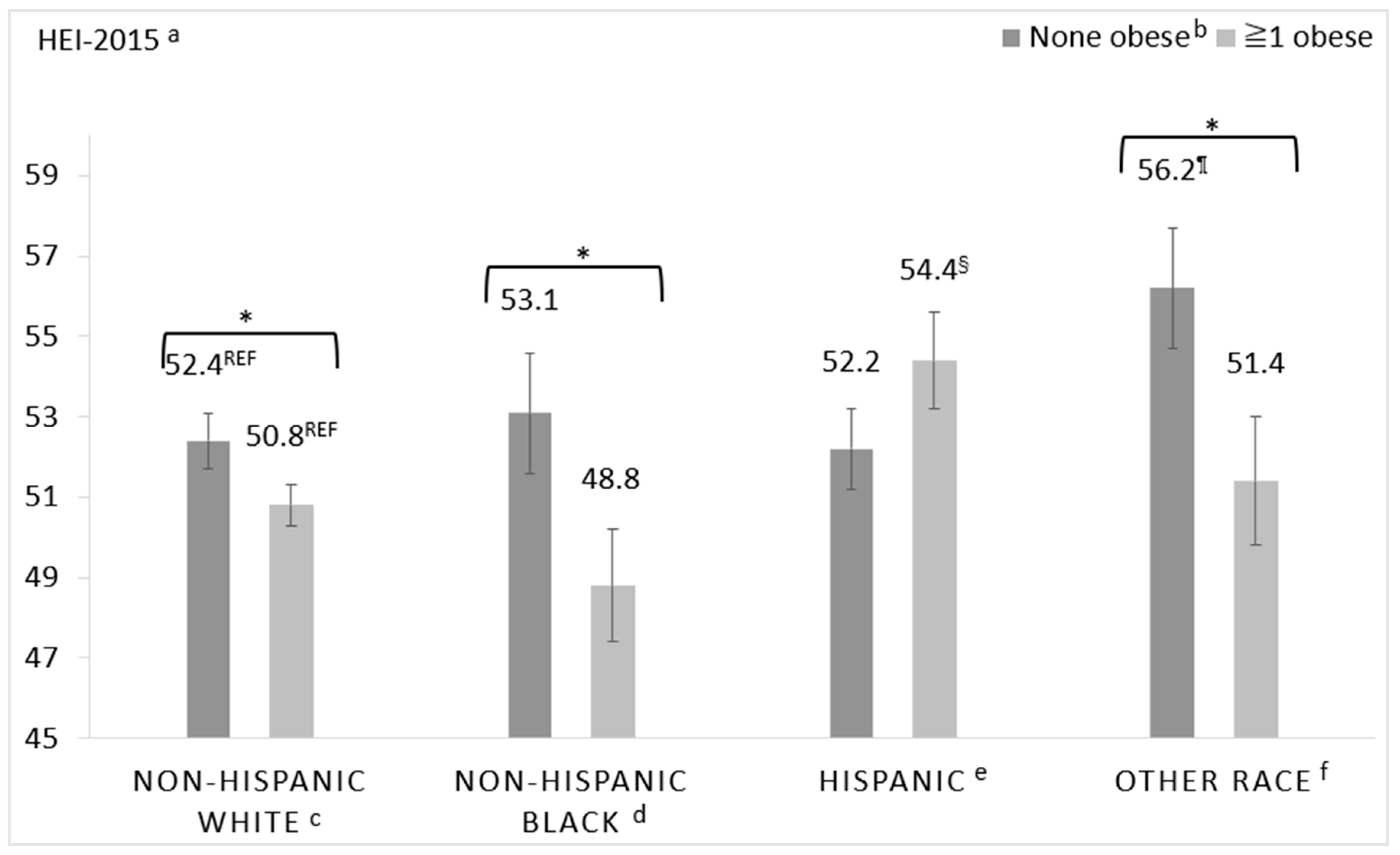
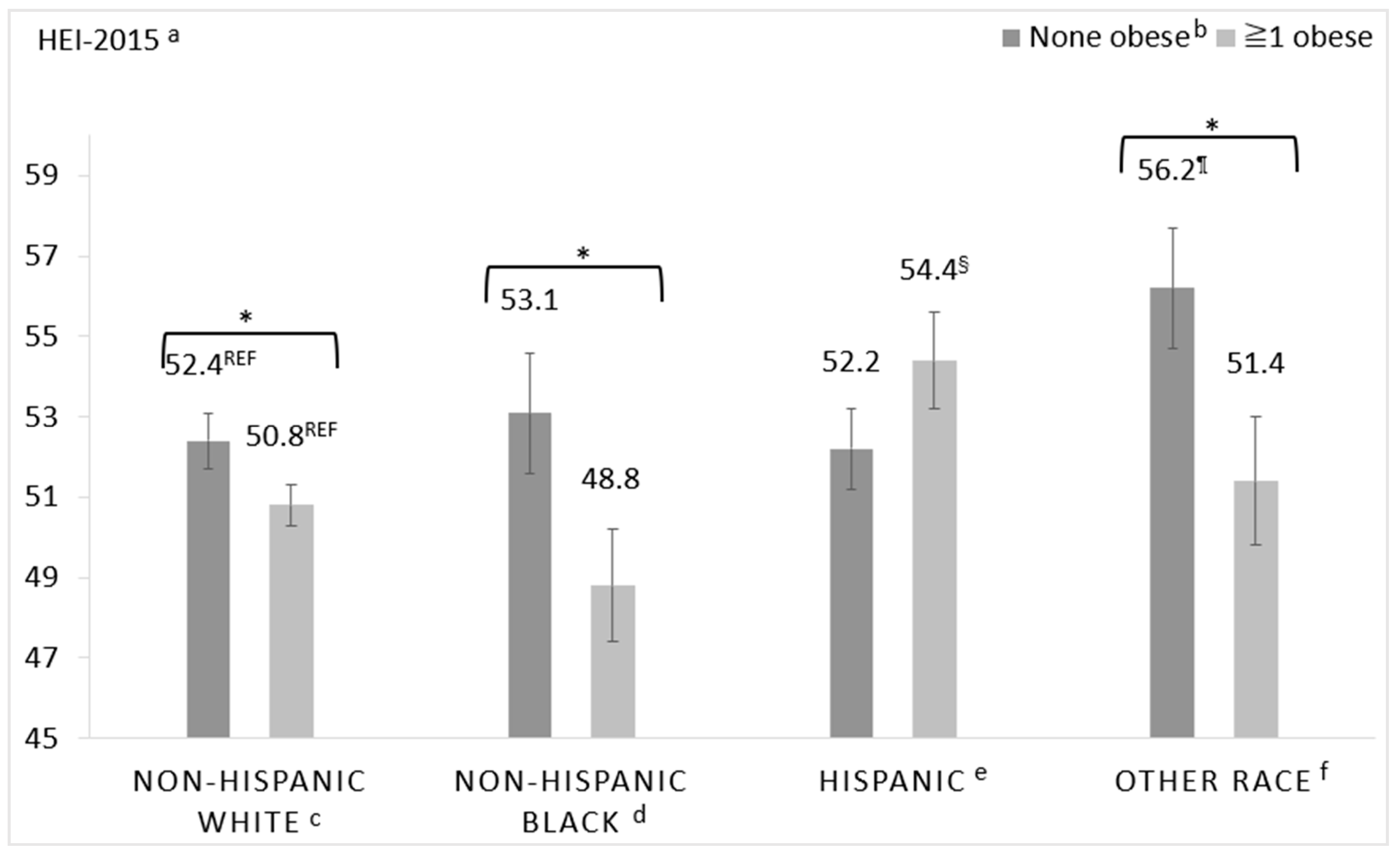
3.5. Associations between Race/Ethnicity and Household-Level Obesity on HEI-2015 Scores
4. Discussion
4.1. Sociodemographic Differences in FAH Acquisition Quality
4.2. Using FAH Acquisition Data as a Proxy Measure of Dietary Intake Quality
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| FoodAPS | Food Acquisition and Purchase Survey |
| FAH | food at home |
| HEI | Healthy Eating Index |
| HH | household |
| NHB | non-Hispanic Black |
| NHW | non-Hispanic White |
| PIR | poverty income ratio |
| PR | primary respondent |
| SNAP | Supplemental Nutrition Assistance Program |
| WIC | Women, Infants, and Children |
References
- Wang, D.D.; Leung, C.W.; Li, Y.; Ding, E.L.; Chiuve, S.E.; Hu, F.B.; Willett, W.C. Trends in dietary quality among adults in the United States, 1999 through 2010. JAMA Intern. Med. 2014, 174, 1587–1595. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Liu, J.; Rehm, C.D.; Wilde, P.; Mande, J.R.; Mozaffarian, D. Trends and disparities in diet quality among us adults by supplemental nutrition assistance program participation status. JAMA Netw. Open 2018, 1, e180237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L.; Thompson, F.E.; Potischman, N.; Guenther, P.M.; Tarasuk, V.; et al. Addressing Current Criticism Regarding the Value of Self-Report Dietary Data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subar, A.F.; Kushi, L.H.; Lerman, J.L.; Freedman, L.S. Invited Commentary: The Contribution to the Field of Nutritional Epidemiology of the Landmark 1985 Publication by Willett et al. Am. J. Epidemiol 2017, 185, 1124–1129. [Google Scholar] [CrossRef] [Green Version]
- National Institutes of Health, Nutrition Research Task Force. 2020–2030 Strategic Plan for NIH Nutrition Research. Available online: https://www.niddk.nih.gov/about-niddk/strategic-plans-reports/strategic-plan-nih-nutrition-research (accessed on 24 July 2020).
- Rumpler, W.V.; Kramer, M.; Rhodes, D.G.; Moshfegh, A.J.; Paul, D.R. Identifying sources of reporting error using measured food intake. Eur. J. Clin. Nutr. 2008, 62, 544–552. [Google Scholar] [CrossRef]
- Brewster, P.J.; Durward, C.M.; Hurdle, J.F.; Stoddard, G.J.; Guenther, P.M. The Grocery Purchase Quality Index-2016 Performs Similarly to the Healthy Eating Index-2015 in a National Survey of Household Food Purchases. J. Acad. Nutr. Diet. 2019, 119, 45–56. [Google Scholar] [CrossRef]
- Eyles, H.; Jiang, Y.; Ni Mhurchu, C. Use of household supermarket sales data to estimate nutrient intakes: A comparison with repeat 24-hour dietary recalls. J. Am. Diet. Assoc. 2010, 110, 106–110. [Google Scholar] [CrossRef]
- Ransley, J.K.; Donnelly, J.K.; Khara, T.N.; Botham, H.; Arnot, H.; Greenwood, D.C.; Cade, J.E. The use of supermarket till receipts to determine the fat and energy intake in a UK population. Public Health Nutr. 2001, 4, 1279–1286. [Google Scholar] [CrossRef]
- Appelhans, B.M.; French, S.A.; Tangney, C.C.; Powell, L.M.; Wang, Y. To what extent do food purchases reflect shoppers’ diet quality and nutrient intake? Int. J. Behav. Nutr. Phys. Act. 2017, 14, 46. [Google Scholar] [CrossRef]
- Kirkpatrick, S.I. Examining the Quality of Foods and Beverages Across the Food Stream. J. Acad. Nutr. Diet. 2019, 119, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Lucan, S.C.; Mitra, N. Perceptions of the food environment are associated with fast-food (not fruit-and-vegetable) consumption: Findings from multi-level models. Int. J. Public Health 2012, 57, 599–608. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Wimer, C.; Seligman, H. Moderation of the Relation of County-Level Cost of Living to Nutrition by the Supplemental Nutrition Assistance Program. Am. J. Public Health 2016, 106, 2064–2070. [Google Scholar] [CrossRef] [PubMed]
- Todd, J.E.; Scharadin, B. Where Households Get Food in a Typical Week: Findings from USDA’s FoodAPS; EIB-156; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2016. [Google Scholar]
- Ver Ploeg, M.; Larimore, E.; Wilde, P. The Influence of Food Store Access on Grocery Shopping and Food Spending; EIB-180; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2017. [Google Scholar]
- Camargo, D.F.M.; Belon, A.P.; Marín-León, L.; Do Nascimento Jacinto de Souza, B.F.; Pérez-Escamilla, R.; Segall-Corrêa, A.M. Comparing food environment and food purchase in areas with low and high prevalence of obesity: Data from a mapping, in-store audit, and population-based survey. Cad. Saude Publica 2019, 35, e00247218. [Google Scholar] [CrossRef]
- Pitt, E.; Gallegos, D.; Comans, T.; Cameron, C.; Thornton, L. Exploring the influence of local food environments on food behaviours: A systematic review of qualitative literature. Public Health Nutr. 2017, 20, 2393–2405. [Google Scholar] [CrossRef] [Green Version]
- Satia, J.A. Diet-related disparities: Understanding the problem and accelerating solutions. J. Am. Diet. Assoc. 2009, 109, 610–615. [Google Scholar] [CrossRef] [Green Version]
- Whitaker, K.M.; Jacobs, D.R.; Kershaw, K.N.; Demmer, R.T.; Booth, J.N.; Carson, A.P.; Lewis, C.E.; Goff, D.C.; Lloyd-Jones, D.M.; Gordon-Larsen, P.; et al. Racial Disparities in Cardiovascular Health Behaviors: The Coronary Artery Risk Development in Young Adults Study. Am. J. Prev. Med. 2018, 55, 63–71. [Google Scholar] [CrossRef]
- Kromhout, D.; Sijtsma, F.P.; Shikany, J.M.; Meyer, K.A.; Van Horn, L.; Harnack, L.; Steffen, L.M.; Jacobs, D.R., Jr. Longitudinal trends in diet and effects of sex, race, and education on dietary quality score change: The Coronary Artery Risk Development in Young Adults study. Am. J. Clin. Nutr. 2012, 95, 580–586. [Google Scholar] [CrossRef] [Green Version]
- Nowlin, S.Y.; Cleland, C.M.; Vadiveloo, M.; D’Eramo Melkus, G.; Parekh, N.; Hagan, H. Explaining Racial/Ethnic Dietary Patterns in Relation to Type 2 Diabetes: An Analysis of NHANES 2007–2012. Ethn. Dis. 2016, 26, 529–536. [Google Scholar] [CrossRef] [Green Version]
- Asghari, G.; Mirmiran, P.; Yuzbashian, E.; Azizi, F. A systematic review of diet quality indices in relation to obesity. Br. J. Nutr. 2017, 117, 1055–1065. [Google Scholar] [CrossRef] [Green Version]
- Wilcox, S.; Sharpe, P.A.; Liese, A.D.; Dunn, C.G.; Hutto, B. Socioeconomic factors associated with diet quality and meeting dietary guidelines in disadvantaged neighborhoods in the Southeast United States. Ethn. Health 2018, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Darmon, N.; Drewnowski, A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: A systematic review and analysis. Nutr. Rev. 2015, 73, 643–660. [Google Scholar] [CrossRef] [PubMed]
- Volaco, A.; Cavalcanti, A.M.; Filho, R.P.; Precoma, D.B. Socioeconomic Status: The Missing Link Between Obesity and Diabetes Mellitus? Curr. Diabetes Rev. 2018, 14, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Finch, B.K.; Bird, C.E.; Escarce, J.J.; Hale, L.; Heron, M.; Lurie, N.; Basurto-Dávila, R.; Dubowitz, T. Neighborhood socioeconomic status and fruit and vegetable intake among whites, blacks, and Mexican Americans in the United States. Am. J. Clin. Nutr. 2008, 87, 1883–1891. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Agriculture Economic Research Service. FoodAPS National Household Food Acquisition and Purchase Survey. Available online: https://www.ers.usda.gov/data-products/foodaps-national-household-food-acquisition-and-purchase-survey/ (accessed on 27 July 2020).
- Reedy, J.; Lerman, J.L.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the Healthy Eating Index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef]
- Kuhn, M.A. Who feels the calorie crunch and when? The impact of school meals on cyclical food insecurity. J. Public Econ. 2018, 166, 27–38. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture Economic Research Service. National Household Food Acquisition and Purchase Survey (FoodAPS). Available online: https://www.ers.usda.gov/foodaps (accessed on 2 April 2020).
- Mancino, L.; Todd, J.E.; Scharadin, B. USDA’s National Household Food Acquisition and Purchase Survey: Methodology for Imputing Missing Quantities to Calculate Healthy Eating Index-2010 Scores and Sort Foods into ERS Food Groups; TB-1947; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2018. [Google Scholar]
- U.S. Department of Agriculture Economic Research Service. National Household Food Acquisition and Purchase Survey (FoodAPS): User’s Guide to Survey Design, Data Collection, and Overview of Datasets; Department of Agriculture, Economic Research Service: Washington, DC, USA, 2016. [Google Scholar]
- Juul, F.; Simoes, B.D.S.; Litvak, J.; Martinez-Steele, E.; Deierlein, A.; Vadiveloo, M.; Parekh, N. Processing level and diet quality of the US grocery cart: Is there an association? Public Health Nutr. 2019, 22, 1–10. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. 2015–2020 Dietary Guidelines for Americans, 8th ed.; U.S. Government Printing Office: Washington, DC, USA, 2015. [Google Scholar]
- Jahns, L.; Scheett, A.J.; Johnson, L.K.; Krebs-Smith, S.M.; Payne, C.R.; Whigham, L.D.; Hoverson, B.S.; Kranz, S. Diet Quality of Items Advertised in Supermarket Sales Circulars Compared to Diets of the US Population, as Assessed by the Healthy Eating Index-2010. J. Acad. Nutr. Diet. 2016, 116, 115–122.e111. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Institute. Research Uses of the HEI. Available online: https://epi.grants.cancer.gov/hei/uses.html (accessed on 24 July 2020).
- National Cancer Institute. Comparing the HEI-2015, HEI-2010 & HEI-2005. Available online: https://epi.grants.cancer.gov/hei/comparing.html (accessed on 24 July 2020).
- Guenther, P.M.; Kirkpatrick, S.I.; Reedy, J.; Krebs-Smith, S.M.; Buckman, D.W.; Dodd, K.W.; Casavale, K.O.; Carroll, R.J. The Healthy Eating Index-2010 is a valid and reliable measure of diet quality according to the 2010 Dietary Guidelines for Americans. J. Nutr. 2014, 144, 399–407. [Google Scholar] [CrossRef] [Green Version]
- Gunderson, C.; Ziliak, J.P. Food Security and Geographic Factors in Food Purchase and Acquisition Decisions: A Compilation of Research Conducted under USDA Cooperative Agreements 58-500-1-0050 and 58-5000-3-0066; University of Kentucky Center for Poverty Research Discussion Paper Series; University of Kentucky Center for Poverty Research: Lexington, KY, USA, 2016. [Google Scholar]
- National Cancer Institute. SAS Code. Available online: https://epi.grants.cancer.gov/hei/sas-code.html (accessed on 24 July 2020).
- Rahkovsky, I.; Young, J.; Carlson, A. Consumers Balance Time and Money in Purchasing Convenience Foods; ERR-251; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2018. [Google Scholar]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [Green Version]
- Bickel, G.; Nord, N.; Price, C.; Hamilton, W.; Cook, J. Guide to Measuring Household Food Security, Revised 2000; U.S. Department of Agriculture, Food and Nutrition Service: Alexandria, VA, USA, 2000. [Google Scholar]
- National Household Food Acquisition and Purchase Survey (FoodAPS): Codebook: FoodAPS Individual Public Use File, Faps_Individual_Puf. U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2016.
- US Census Bureau. How the Census Bureau Measures Poverty. Available online: https://www.census.gov/topics/income-poverty/poverty/guidance/poverty-measures.html (accessed on 16 December 2019).
- Johnson, C.L.; Paulose-Ram, R.; Ogden, C.L.; Carroll, M.D.; Kruszon-Moran, D.; Dohrmann, S.M.; Curtin, L.R. National Health and Nutrition Examination Survey: Analytic guidelines, 1999–2010. Vital Health Stat. 2013, 1–24. [Google Scholar]
- Hiza, H.A.; Casavale, K.O.; Guenther, P.M.; Davis, C.A. Diet quality of Americans differs by age, sex, race/ethnicity, income, and education level. J. Acad. Nutr. Diet. 2013, 113, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Andreyeva, T.; Tripp, A.S.; Schwartz, M.B. Dietary Quality of Americans by Supplemental Nutrition Assistance Program Participation Status: A Systematic Review. Am. J. Prev. Med. 2015, 49, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, B.T.; Shuval, K.; Bertmann, F.; Yaroch, A.L. The Supplemental Nutrition Assistance Program, Food Insecurity, Dietary Quality, and Obesity Among U.S. Adults. Am. J. Public Health 2015, 105, 1453–1459. [Google Scholar] [CrossRef]
- SAS. SAS, 9.4; SAS Institute, Inc.: Cary, NC, USA, 2013. [Google Scholar]
- Lee, S.; Lee, D.K. What is the proper way to apply the multiple comparison test? Korean J. Anesth. 2018, 71, 353–360. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, B.T.; Powell, L.M. The impact of restaurant consumption among US adults: Effects on energy and nutrient intakes. Public Health Nutr. 2014, 17, 2445–2452. [Google Scholar] [CrossRef] [Green Version]
- An, R. Fast-food and full-service restaurant consumption and daily energy and nutrient intakes in US adults. Eur. J. Clin. Nutr. 2016, 70, 97–103. [Google Scholar] [CrossRef]
- Mancino, L.; Guthrie, J.; Ver Ploeg, M.; Lin, B.H. Nutritional Quality of Foods Purchased and Acquired by Americans: Findings from USDA’s National Household Food Acquisition and Purchase Survey; EIB-188; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2018. [Google Scholar]
- Hebert, J.R.; Clemow, L.; Pbert, L.; Ockene, I.S.; Ockene, J.K. Social desirability bias in dietary self-report may compromise the validity of dietary intake measures. Int. J. Epidemiol. 1995, 24, 389–398. [Google Scholar] [CrossRef]
- Grummon, A.H.; Taillie, L.S. Nutritional profile of Supplemental Nutrition Assistance Program household food and beverage purchases. Am. J. Clin. Nutr. 2017, 105, 1433–1442. [Google Scholar] [CrossRef] [Green Version]
- Gregory, C.A.; Mancino, L.; Coleman-Jensen, A. Food Security and Food Purchase Quality among Low-Income Households: Findings from the National Household Food Acquisition and Purchase Survey (FoodAPS); ERR-269; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2019. [Google Scholar]
- Keith-Jennings, B.; Llobrera, J.; Dean, S. Links of the Supplemental Nutrition Assistance Program With Food Insecurity, Poverty, and Health: Evidence and Potential. Am. J. Public Health 2019, 109, 1636–1640. [Google Scholar] [CrossRef]
- Brown, A.F.; Liang, L.J.; Vassar, S.D.; Escarce, J.J.; Merkin, S.S.; Cheng, E.; Richards, A.; Seeman, T.; Longstreth, W.T., Jr. Trends in Racial/Ethnic and Nativity Disparities in Cardiovascular Health Among Adults Without Prevalent Cardiovascular Disease in the United States, 1988 to 2014. Ann. Int. Med. 2018, 168, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Rehm, C.D.; Penalvo, J.L.; Afshin, A.; Mozaffarian, D. Dietary Intake Among US Adults, 1999–2012. JAMA 2016, 315, 2542–2553. [Google Scholar] [CrossRef] [PubMed]
- Ejima, K.; Thomas, D.M.; Allison, D.B. A Mathematical Model for Predicting Obesity Transmission with Both Genetic and Nongenetic Heredity. Obesity (Silver Spring Md.) 2018, 26, 927–933. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y. The Differences in Characteristics among Households with and without an Obese Child.: Findings from USDA’s FoodAPS; EIB-179; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2017. [Google Scholar]
- Patetta, M.A.; Pedraza, L.S.; Popkin, B.M. Improvements in the nutritional quality of US young adults based on food sources and socioeconomic status between 1989–1991 and 2011–2014. Nutr. J. 2019, 18, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medina-Inojosa, J.; Jean, N.; Cortes-Bergoderi, M.; Lopez-Jimenez, F. The Hispanic Paradox in Cardiovascular Disease and Total Mortality. Prog. Cardiovasc. Dis. 2014, 57, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.; Kirlin, J.A.; West, B.T.; He, W.; Ong, A.R.; Zhang, S.; Zhang, X. Estimation of Underreporting in Diary Surveys: An Application using the National Household Food Acquisition and Purchase Survey. J. Surv. Stat. Methodol. 2019. [Google Scholar] [CrossRef]
- Hu, M.; Gremel, G.W.; Kirlin, J.A.; West, B.T. Nonresponse and Underreporting Errors Increase over the Data Collection Week Based on Paradata from the National Household Food Acquisition and Purchase Survey. J. Nutr. 2017, 147, 964–975. [Google Scholar] [CrossRef]
- Carlson, A.C.; Tselepidakis-Page, E.; Palmer-Zimmerman, T.; Tornow, C.E.; Hermansen, S. Linking USDA Nutrition Databases to IRI Household-Based and Store-Based Scanner Data; TB-1952; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2019. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Households | HEI-2015 a <40 | HEI-2015 40–59 | HEI-2015 ≥60 | p |
|---|---|---|---|---|---|
| (n = 3961) Mean (SE b) | (n = 702) Mean (SE) | (n = 2195) Mean (SE) | (n = 1064) Mean (SE) | ||
| Percent, % | 17.7 | 55.4 | 26.9 | ||
| Household size | 2.49 (0.05) | 2.54 (0.11) | 2.59 (0.06) | 2.32 (0.05) | 0.005 |
| Children (0–18 years) in HH c | 0.64 (0.03) | 0.70 (0.07) | 0.73 (0.05) | 0.49 (0.03) | <0.001 |
| Race/ethnicity of primary respondent, % | |||||
| Non-Hispanic White | 70.3 | 69.5 | 69.7 | 71.6 | <0.001 |
| Non-Hispanic Black | 9.9 | 11.7 | 12.0 | 5.93 | |
| Hispanic | 13.0 | 14.5 | 12.5 | 13.2 | |
| Other race (non-Hispanic) | 6.8 | 4.36 | 5.85 | 9.32 | |
| Sex of primary respondent, % | 0.59 | ||||
| Male | 29.8 | 30.4 | 30.9 | 28.0 | |
| Female | 70.2 | 69.6 | 69.1 | 72.0 | |
| Age primary respondent, years | 50.6 (0.53) | 48.4 (1.39) | 50.4 (0.68) | 51.8 (0.65) | 0.02 |
| Education level primary respondent, % | <0.001 | ||||
| Less than high school | 9.1 | 12.0 | 9.93 | 6.54 | |
| High school degree/some college | 57.8 | 71.1 | 61.1 | 47.1 | |
| Bachelor’s degree or higher | 33.1 | 17.0 | 29.0 | 46.3 | |
| Family income to poverty ratio, % | <0.001 | ||||
| <130% | 16.9 | 27.2 | 18.1 | 10.9 | |
| 130–349% | 41.1 | 46.8 | 42.6 | 36.4 | |
| ≥350% | 42.0 | 25.9 | 39.4 | 52.7 | |
| SNAP d participation, % | 12.7 | 21.0 | 14.7 | 6.27 | <0.001 |
| WIC e participation f, % | 27.0 | 33.3 | 29.8 | 19.4 | 0.038 |
| Food security status, % | <0.001 | ||||
| Food secure household | 86.0 | 78.2 | 84.5 | 91.5 | |
| Food insecure household | 14.0 | 21.8 | 15.5 | 8.50 | |
| Smoker in HH, % | 29.3 | 46.8 | 32.9 | 16.4 | <0.001 |
| ≥1 obese g person in HH, % | 45.4 | 53.7 | 48.6 | 36.9 | <0.001 |
| Self-perceived health status of primary respondent, % | <0.001 | ||||
| Excellent | 13.1 | 9.64 | 13.1 | 14.5 | |
| Very good | 34.5 | 24.2 | 30.8 | 44.6 | |
| Good | 36.0 | 40.7 | 38.7 | 29.7 | |
| Fair | 13.4 | 20.1 | 14.1 | 9.65 | |
| Poor | 3.02 | 5.41 | 3.35 | 1.52 | |
| Region, % | 0.001 | ||||
| Northeast | 15.8 | 15.0 | 14.6 | 18.0 | |
| Midwest | 31.4 | 27.3 | 33.6 | 29.4 | |
| South | 34.7 | 44.1 | 35.6 | 29.4 | |
| West | 18.2 | 13.6 | 16.3 | 23.3 | |
| HH located in rural census tract, % | 34.6 | 40.8 | 37.0 | 28.3 | 0.004 |
| Total FAH h purchases in 7 days, kcal | 35615.9 (730.5) | 32271.0 (1698.3) | 37370.4 (1068.5) | 34209.6 (1203.3) | 0.99 |
| Total FAH items purchased in 7 days | 33.1 (0.58) | 26.6 (1.34) | 32.93 (0.79) | 35.9 (0.88) | <0.001 |
| Perceived healthfulness of diet i, % | <0.001 | ||||
| Excellent | 8.20 | 5.6 | 6.3 | 12.3 | |
| Very good | 29.6 | 23.9 | 26.7 | 36.8 | |
| Good | 42.0 | 39.9 | 45.4 | 37.4 | |
| Fair | 17.0 | 24.5 | 18.5 | 11.7 | |
| Poor | 3.11 | 6.03 | 3.15 | 1.83 |
| HEI-2015 a Total and Component Scores (Maximum Score) | Mean (SE b) | p |
|---|---|---|
| All households | ||
| Total score (100) | 54.7 (0.4) | |
| Total fruits (5) | 2.8 (0.1) | |
| Whole fruits (5) | 2.9 (0.0) | |
| Total vegetables (5) | 1.9 (0.1) | |
| Greens and beans (5) | 2.5 (0.1) | |
| Whole grains (10) | 2.8 (0.1) | |
| Dairy (10) | 5.3 (0.1) | |
| Total protein foods (5) | 3.6 (0.0) | |
| Seafood and plant proteins (5) | 2.4 (0.1) | |
| Fatty acids ratio (10) | 5.0 (0.1) | |
| Refined grains (10) | 6.7 (0.1) | |
| Sodium (10) | 6.8 (0.1) | |
| Added sugars (10) | 5.7 (0.1) | |
| Saturated fats (10) | 6.2 (0.1) | |
| Total HEI-2015 score by race/ethnicity | <0.001 | |
| Non-Hispanic White, ref. c | 54.9 (0.5) | |
| Non-Hispanic Black | 51.5 (1.3) | 0.008 |
| Hispanic | 54.1 (0.7) | 0.366 |
| Other race (non-Hispanic) | 58.1 (1.1) | 0.020 |
| Total HEI-2015 score by food security status | <0.001 | |
| Food secure household, ref. | 55.4 (0.4) | |
| Food insecure household | 50.1 (0.6) | <0.001 |
| Total HEI-2015 score by SNAP d-participation | <0.001 | |
| Household not participating in SNAP, ref. | 55.5 (0.4) | |
| SNAP-household | 49.1 (0.5) | <0.001 |
| Total HEI-2015 score by weight-status | <0.001 | |
| None obese in household, ref. | 56.2 (0.5) | |
| ≥1 obese e person in household | 52.8 (0.6) | <0.001 |
| Total HEI-2015 score by family income to poverty ratio | <0.001 | |
| ≥350%, ref. | 57.1 (0.6) | |
| 130–349% | 53.8 (0.6) | <0.001 |
| <130% | 50.7 (0.7) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vadiveloo, M.K.; Parker, H.W.; Juul, F.; Parekh, N. Sociodemographic Differences in the Dietary Quality of Food-at-Home Acquisitions and Purchases among Participants in the U.S. Nationally Representative Food Acquisition and Purchase Survey (FoodAPS). Nutrients 2020, 12, 2354. https://doi.org/10.3390/nu12082354
Vadiveloo MK, Parker HW, Juul F, Parekh N. Sociodemographic Differences in the Dietary Quality of Food-at-Home Acquisitions and Purchases among Participants in the U.S. Nationally Representative Food Acquisition and Purchase Survey (FoodAPS). Nutrients. 2020; 12(8):2354. https://doi.org/10.3390/nu12082354
Chicago/Turabian StyleVadiveloo, Maya K., Haley W. Parker, Filippa Juul, and Niyati Parekh. 2020. "Sociodemographic Differences in the Dietary Quality of Food-at-Home Acquisitions and Purchases among Participants in the U.S. Nationally Representative Food Acquisition and Purchase Survey (FoodAPS)" Nutrients 12, no. 8: 2354. https://doi.org/10.3390/nu12082354