1. Introduction
Musculoskeletal injuries to athletes are common and represent a threat to continued participation in sports and physical activity [
1]. Runners are particularly susceptible to lower-body injuries, with one recent systematic review producing estimates of ~20 such injuries per 100 runners [
2]. Some injuries include pain in the iliotibial band, Achilles tendonitis, and plantar fasciitis [
3]. One of the more common injuries for runners is patellofemoral pain, characterized by pain in the knee at the site of the patella during flexion and weight-bearing activity [
4]. Recent evidence estimates that patellofemoral pain is prevalent in 16.7% of runners [
3]. This relatively high injury rate may limit or even prevent running activity, making sufficient physical activity difficult to attain and limiting long-term fitness and health [
5,
6]. Taping techniques with rigid athletic tape are commonly used in rehabilitative settings to limit the range of motion (ROM) at a variety of joints and prevent further aggravation of athletes’ injured muscles, tendons, or other joint structures [
7]. Increasing joint stability without complete immobilization enables movement with a lower risk of re-injury [
8].
Kinesio tape is a variety of tape which can be applied in a way that supports muscles and joints without restricting range of motion [
9]. Unlike traditional athletic tape, Kinesio tape is made of material with elastic properties and can be stretched up to 160% of its initial length [
10]. The tension in the Kinesio tape that results from its application on the skin is purported to reduce pain by limiting the input of nociceptors in the skin [
9] and also to improve blood flow in the tissue to encourage the healing of damaged muscle [
11].
The recoil of stretched Kinesio tape also provides supplemental force production for the muscle it is aligned with. This allows practitioners to apply the tape on the skin so that the desired amount of tension is produced over the joint to aid in muscle contraction for functional and stability purposes. An increase in proprioception via the activation of the cutaneous receptors is also believed to contribute to enhanced muscle function [
12]. Typical Kinesio tape placement at the knee incorporates taping across the anterior aspect of the knee [
13]. This orientation of Kinesio tape supplements the force produced by the quadriceps muscle group during knee extension and opposes the force produced by the hamstring muscle group during knee flexion.
The allocation of force in this way may be unfavorable during continuous aerobic exercise such as running, which relies on both knee flexion and extension throughout the exercise. The quadriceps group has a greater force-generating capability than its antagonist hamstring group, a characterization termed the H:Q ratio [
14,
15]. The imbalance in strength between these two muscle groups may be amplified with traditional Kinesio tape application along the anterior aspect of the knee. However, it may be possible to offset this strength imbalance between the quadriceps and hamstrings by instead applying Kinesio tape to the posterior aspect of the knee. In this novel technique, the Kinesio tape would act as a spring to enhance the function of the hamstring group.
Taping techniques, including the application of Kinesio tape, may have some beneficial effect on muscle function in athletes (for review, see Lau and Cheng, 2019) [
16]. Yet, the impact of taping techniques on performance metrics associated with aerobic endurance exercise remains unexplored. Low-cost strategies to improve performance while also offering previously cited benefits (decreased patellofemoral pain, improved blood and lymphatic flow, etc.) are relevant to this population of athletes, who report high rates of overuse injury [
3,
17]. The muscle activation required to run at a given pace and the oxygen consumption required to sustain this running are of particular interest, since this mechanism of action for Kinesio tape has not been reported upon.
Runners may opt to use taping techniques such as athletic taping for added joint stability, or to use Kinesio tape to reduce pain or improve muscle perfusion. There is also the potential for taping techniques (i.e., the spring method) to be used for ergogenic benefit by offsetting the H:Q ratio found in the muscles which control the knee. Taping at the knee joint may be the most commonly considered due to the prominence of injuries and chronic pain there [
3]. Whatever the motivation to implement these different taping techniques, the impact of these strategies on running efficiency, and, hence, running performance, should also be considered [
18]. No published research to date has examined the effects of different taping techniques on running efficiency. Therefore, the purpose of this study was to determine if different commonly used taping techniques (the use of athletic tape and Kinesio tape) and one novel taping technique (spring) for the knee during treadmill running would impact the exercise efficiency of the running activity.
3. Discussion
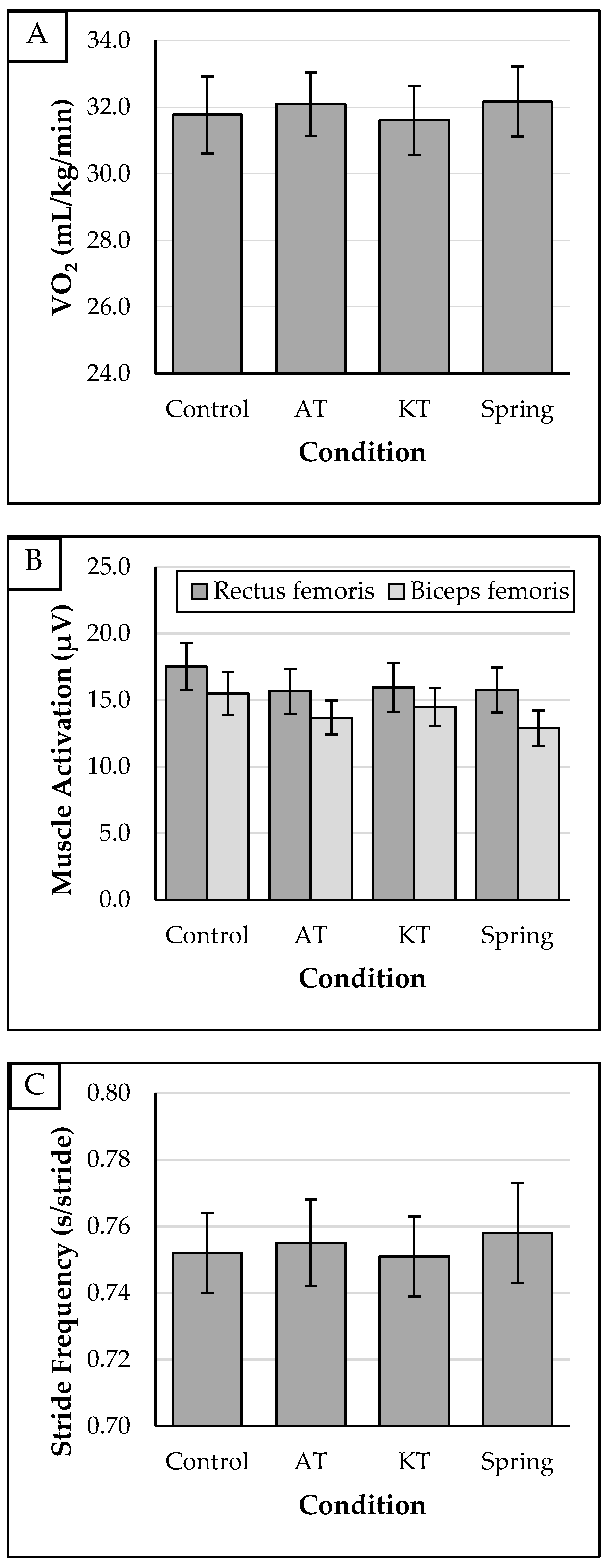
The purpose of this study was to determine if a variety of different taping techniques for the knee during treadmill running would impact the exercise efficiency of the running activity. We hypothesized that the novel spring method of Kinesio tape application would yield muscle activation, oxygen consumption, and stride frequency benefits to running activity. The results observed do not support our hypotheses. Furthermore, there were no differences in these variables between any of the other taping conditions compared to the control condition. These findings and their implications will be discussed.
There was no effect of any taping condition on muscle activation of the primary knee flexor or extensor muscles. The conditions using Kinesio tape (the KT and spring conditions) were expected to see a reduced muscle activation of the muscle that the tape was applied to, given the elastic properties and supplementary force production upon recoil. Specifically, the spring taping technique was designed to modify the H:Q ratio, or the notable difference in the force production capability between the hamstring and quadriceps muscle groups [
15]. Applying Kinesio tape to the posterior aspect of the knee was theorized to assist the weaker hamstring group and necessitate a lower activation of the biceps femoris muscle. Although EMG
biceps was the lowest in the spring group, this difference was not significant, and, therefore, not attributable to the taping condition per se. The large effect size observed (
η2 = 0.184 > 0.14), however, suggests that this non-significant reduction in biceps femoris activation may have been more pronounced if the running bouts were of a longer duration, if the hamstring group was substantially fatigued prior to the running bout, or if more participants had been included to increase statistical power.
Other studies have reported similar findings that Kinesio tape application does not alter the level of muscle activity. Yeung et al. [
13] found that Kinesio tape application to the knee shortened the time required to generate peak torque during knee extension, but saw no difference in knee extensor activation. Similarly, at the shoulder joint, the application of Kinesio tape produced a reduction in muscle contraction onset time without differences in peak muscle activation during abduction and flexion [
19]. Similar conclusions were made when assessing the muscle activation onset time of the lateral gastrocnemius muscle during walking, with and without Kinesio tape application. The onset time was shorter, yet the level of EMG activity was unchanged with Kinesio tape [
20]. These findings are supported by a study demonstrating that Kinesio tape application facilitated an increase in the motor unit pool activation of the muscle application site [
12]. The stimulation of cutaneous receptors is thought to be the mechanism of action explaining an increase in muscle response time, a structure which would not be thought to impact muscle activation levels.
The effect of the application of taping techniques on athletic performance may be due, in part, to this improvement in muscle contraction onset time. Functional athletic skills, such as maximal power output, jumping, sprinting, etc., require high rates of force development [
21], a benefit that appears to be imbued by Kinesio tape application. Cochrane, Nkuna, and Dawood [
22] noted that the application of Kinesio tape to various muscles of the lower body resulted in improvements in speed, agility, and lower-body power in college-age soccer players. Similarly, Kinesio tape application for 72 h resulted in improvements in vertical jump height and ground reaction force [
23]. The performance of some skills and balance were also reported to be improved in athletes with the application of taping by Lau and Cheng [
16] in their large-scale review article.
On the other hand, a study on the effects of Kinesio tape application in volleyball players found no effect on vertical jump height or peak jump power [
24]. Other studies support the idea that the benefits from Kinesio tape application may be due to a placebo effect [
25,
26,
27]. More investigations into the circumstances under which taping practices improve performance are needed to fully elucidate the effectiveness of this strategy.
Few studies to date have examined the effect of how potential muscular and biomechanical changes brought on by taping application might translate into metabolic changes during continuous running exercise. The current study was designed to address this gap in the literature. We attempted to control for the effects of perceived exertion, fatigue, and cardiovascular strain between the different conditions by using a fixed individualized running intensity and ensuring a sufficient recovery time between each running bout. The consistent levels of HR and RPE for each condition confirmed that these potential confounders to VO2 levels were not present to a substantial degree.
The lack of difference in VO
2 between conditions makes sense, given that no changes in muscle activation were observed, and, hence, no difference in O
2 utilization would be necessitated. The intensity of the muscle contraction for running activity or the low levels of fatigue in the muscles may have limited the effects of the taping conditions on muscle activation, and hence, metabolic activity. For example, Yeung et al. [
13] noted that effects of KT were present in a fatigued state for knee flexor activity. Additionally, Kinesio tape application has been found to be beneficial to anaerobic, but not aerobic, performance of a lesser intensity [
28], supporting the possible explanation that the intensity of muscle contraction determines the effectiveness of taping techniques.
Practical applications of this study merit discussion. Despite no beneficial effects of any taping application on running efficiency, there were no negative effects observed either. Runners who are advised to use taping at the knee joint during physical activity can do so without a measurably diminished running efficiency, muscle activity, or stride frequency. Athletic tape and Kinesio tape application is common in rehabilitative settings, so their continued use in more applicable exercise scenarios (running at a preferred speed) does not appear to have drawbacks in terms of muscular or metabolic function. Furthermore, the cost of trying Kinesio tape and assessing its actual (or perceived) effectiveness on an individual basis is not prohibitively expensive.
Strengths and Limitations
The current study was characterized by several strengths, one of which was that a repeated-measures design was used to make comparisons between conditions, limiting the effect of interindividual variability. The use of wireless EMG sensors to assess muscle activation preserved some of the generalizability of the running activity, since no effort was needed by participants to avoid stepping on or tripping over wires. The use of a reputable metabolic cart to measure oxygen consumption ensured that valid data were used to address the novel research aims of this study.
Still, several limitations exist as well. First, the conclusions of this study are limited to young, healthy participants, as this was the target population that was tested. The results we present cannot necessarily be generalized to other groups beyond this population, such as older people or those with injuries and chronic pain. Specifically, people with patellofemoral pain syndrome or other knee conditions present during running may experience the effects of taping application differently than the sample selected for this study. This is particularly true for the KT condition, because this technique is designed specifically to alleviate joint pain when appropriately implemented. Future studies in this area should consider investigating the effects of taping techniques in people with mild–moderate joint pain. The relatively small sample size of this study also contributes to the lack of generalizability of the presented findings.
Second, we did not assess some potential structural issues within the participants’ limbs and joints. Specifically, the position of the knee structures (i.e., the patella) before and after taping were not formally assessed, as the technology available made this unfeasible, and no tape was placed directly on the patella in any conditions tested. Changes in the locations of knee structures may be useful in future studies to explain the potential ergogenic effects of taping techniques. Similarly, we did not measure the precise lengths of both legs of each participant to ensure that they were the same length. Leg length discrepancies may impact the neuromuscular or biomechanical function, so the results reported can only be said to be true for the dominant legs of the participants.
A third research design limitation was the potential effects of fatigue, due to the need to conduct all four running bouts on the same day. This schedule was used to ensure consistent placement of the EMG leads for all running bouts and control for the effects of day-to-day variation in metabolic rate/muscle soreness that could result from participants’ daily schedules or workout regimens. We attempted to control for the effects of resulting fatigue by maintaining a sufficient recovery period between running bouts and using a running task which was of an appropriate duration and intensity to complete four times in succession. If a future study was undertaken with only the spring technique and a control condition, running bouts of a longer duration could be completed, allowing for a more robust understanding of the effects of this taping strategy over the course of a more typical running task. Using fewer conditions would also allow for the order of the conditions to be fully counterbalanced, which was not achieved in this study and could limit the results presented.
Finally, a fourth limitation was that the tension of the Kinesio tape in the spring condition may have been less than needed to generate the force to balance the H:Q ratio, which was the intended effect of the spring condition. This is a novel technique and there were no previous studies upon which to base the tape application. The findings presented here suggest that modifications to the spring technique, such as increasing the number of pieces of Kinesio tape applied or the tension applied by the tape (i.e., the amount of stretch when applied), are necessary to observe the effects we are interested in.
4. Materials and Methods
4.1. Research Design
To address the research questions of interest, a repeated-measures crossover design was used, in which healthy recreational runners completed four 6-min bouts of treadmill running at a previously determined preferred running speed. Each condition used a different taping technique, as follows: no tape (control), athletic tape (AT), Kinesio tape (KT), and a spring taping technique using both athletic and Kinesio tapes (spring). The order of the conditions was randomized and counterbalanced as equally as possible. Given the number of participants and the large number of possible orders of the conditions, it was not possible to fully counterbalance the order of the conditions. The order in which each participant completed the conditions was unique to them, however, which helped to control for potential effects of fatigue or previous taping conditions. During each bout, oxygen consumption (VO2), muscle activation of the rectus femoris (EMGrectus), muscle activation of the biceps femoris (EMGbiceps), stride frequency (SF), Borg rating of perceived exertion (RPE), and heart rate (HR) data were collected for analysis with repeated measures. Institutional Review Board approval (#2069992) was obtained prior to any data collection for this study.
4.2. Outcome Measures
The specific aims of the study were to determine if the taping technique had an effect on the following measures of exercise efficiency during running bouts at a preferred running speed: (1) oxygen consumption, (2) muscle activation of the knee agonists during running exercise, and (3) stride frequency. We hypothesized that the spring technique would result in (H1) a lower oxygen consumption, (H2) a lower muscle activation of the agonist muscles, and (H3) a lower stride frequency than the other taping techniques and a control condition.
4.3. Participants
Adults (age ≥ 18 years) who self-identified as recreational runners were recruited for this study via the posting and dissemination of flyers and word-of-mouth. All participants were full-time students and did not participate in heavy labor occupations, which have the potential to alter gait mechanics. The exclusion criteria included the inability to run for a full 60 min without rest and the presence of any type of injury which would interfere with a treadmill running activity. In addition to current injuries, any major injury in the previous year or lower-limb surgery at any time previously would result in exclusion from participating in the study. People with conditions which could influence HR (congenital heart disease, cardiac arrhythmias, etc.) were also excluded from the study.
An a priori power analysis for a repeated-measures design using one group and four measurements was completed using G*Power version 3.1 [
29]. With an alpha level of 0.05, power level of 0.80, and estimated moderate-large effect size of
f = 0.33 (based on the pilot data collected in our laboratory), it was determined that an estimated 14 participants would be needed to complete the study with sufficient power.
4.4. Instruments
An SECA 769 stadiometer and scale (Seca GmbH & Co. KG; Hamburg, Germany) was used to collect the participants’ height and weight. A Polar H10 telemetric HR belt-worn sensor and watch (Polar Electro Inc.; Bethpage, NY, USA) were used to collect the HR data. Muscle activation was assessed using a Delsys Trigno wireless EMG system (Delsys Inc.; Natick, MA, USA), which recorded signals from sensors taped in place on the muscles of interest (rectus femoris and biceps femoris). Wireless sensors were secured in place using double-sided adhesive medical tape (3M Company; Greenville, SC, USA).
A TrueOne 2400 metabolic cart (Parvo Medics; Salt Lake City, UT, USA) calibrated to manufacturer specifications within 1 h of data collection was used to assess VO2. The participants’ expired breath was collected using a Hans Rudolph 7450 Series V2 mask (Hans Rudolph Inc.; Lenexa, KS, USA), connected to the metabolic cart using a 2 m hose.
The running activity was completed on a Trackmaster TMX425C model treadmill (Full Vision Inc.; Newton, KS, USA). Athletic tape (Hampton Adams Inc.; Orange County, CA, USA) and Kinesio tape (OK TAPE Inc.; El Monte, CA, USA) were used in the respective taping technique conditions. The Borg 6–20 rating of perceived exertion scale was used to measure the rating of perceived exertion (RPE), a subjective rating of work intensity, on a scale from 6 (no exertion) to 20 (maximal exertion) [
30]. The participants were asked “How hard do you feel that you are working from 6, no exertion, to 20, maximal exertion?”, and were then requested to point at a printed version of the scale to indicate their response.
4.5. Procedures
All data collection for this study was completed in one visit to the Exercise Physiology Laboratory at Augusta University. Upon arrival, the participants completed the informed consent form and were provided with explanations for any questions that arose. The collection of participants’ height (cm) and body mass (kg) was completed. Investigators also collected age, sex, and average running distance per week at this time. The participants were fitted with an HR belt to which the HR sensor was attached. A 5 min warm-up of light-intensity walking/jogging ensued, during which time, the instructions for the RPE scale were reviewed and the proper functioning of the HR monitor was verified.
Following the warm-up, a blind measurement of preferred running speed was conducted. The treadmill display face was covered from view while the speed of the treadmill belt was slowly increased, starting at a speed of 2 miles per hour. Once the treadmill belt was moving, the participant increased the speed until they achieved a running speed that they felt comfortable adopting for a 30-min training run. In this way, the participants gauged their preferred running speed based on interoception and personal judgement, with less influence from bias resulting from investigator presence. This preferred running speed was recorded by the investigator, who was able to view the treadmill display without revealing to the participant the speed that they had selected. This process was completed a total of three times, and the average of all three trials was used to calculate the preferred speed for individual participants. If one trial’s result was more than 20% faster or slower than either of the speeds selected in the other two trials, then a fourth trial was conducted to replace the outlying value.
After the measurement of preferred speed, EMG sensors were applied by the investigators to the two muscle sites on the dominant leg according to the SENIAM guidelines [
31]. The site of sensor placement was shaved by the participants prior to their arrival at the lab. Adhesive tape was applied directly to the EMG sensors, and an additional ace bandage secured by athletic trainer tape was applied to the associated area to secure the sensors throughout all experimental running conditions. The application of this ace bandage and athletic tape was implemented in a way to ensure that the sensor remained in place throughout the entire study, but was not so tight that it caused discomfort or impeded the range of motion of the participant.
The participants completed all four running bouts in succession. Each bout was 6 min in length, was completed at the predetermined preferred running speed, and was followed by a brief period of rest. The duration of 6 min was used to ensure that there was enough time to collect the artifact-free data needed for analysis, while also limiting the effects of fatigue on successive running activity. The rest period was of a sufficient length for the next taping condition to be applied and for the participants’ HR to return to within 10 beats per minute of the HR value measured following 5 min of recovery from the preferred running speed determination. For example, if a participant had a HR of 90 bpm 5 min after the preferred running speed test, they would rest after each running condition until their HR decreased to at least 100 bpm, and the next taping condition was applied. For this reason, the rest duration varied for each participant in between each condition. The taping technique for each condition (control, AT, KT, and spring in a randomized order) was applied by the same investigator for all participants following the preferred running speed measurement (for the first bout) and during the rest period between bouts (bouts 2–4).
The control condition consisted of no tape applied to the participant. The AT condition consisted of athletic tape applied to the lateral aspects of the knee joint according to common practices [
32]. For the KT condition, a technique used for the prevention of patellofemoral pain was applied, as follows: one 6–8-inch strip of Kinesio tape was cut down the middle for 2/3 the length of the strip; the then two separate ends were applied above the kneecap, attaching to the quadriceps group. The tape was then stretched to 150% of its resting length and applied around the kneecap. The uncut 1/3 of the tape was applied below the kneecap and secured for the proper adhesion of the Kinesio tape. For the spring condition, both athletic tape and Kinesio tape were used. Three, 4-inch-long strips of Kinesio tape were applied in tandem (side-by-side-by-side), with 150% of the resting length stretching to the back of the knee, starting at the distal end of the hamstring group and inserting at the proximal end of the gastrocnemius on the lower leg. Athletic tape was then wrapped around the thigh and lower leg over each end of the Kinesio tape strips to secure it in place and maintain the desired tension throughout the running trial. The result was a taping condition designed to increase the flexion torque of the hamstrings muscle group. Images of the three taping conditions are presented in
Figure 2.
During each 6-min running bout, VO2 was measured continuously and averaged across the entire bout. SF was measured at the start of minute 4 of each bout, beginning with a forward propulsion of the participants’ dominant leg and ending with the twentieth repetition from zero of the same leg. Subsequently, RPE assessment was solicited from the participant. In the fifth minute of the six-minute trial, EMG sensors recording the biceps femoris and rectus femoris were activated by the researcher, measuring the muscle activity for a thirty-second recording. HR was recorded as the average HR over the final 30 s of each bout.
4.6. Data Reduction and Processing
A fourth-order five-point moving window average was used for VO2 to obtain comparable data for each of the four conditions. VO2 (mL/kg/min) was represented by a five-breath average for the six-minute trial per condition and averaged across the entirety of the steady state during the 6 min of each condition.
A bandpass filter was applied to the EMG data, including only data points that exerted 5–500 Hz. Electromyography was averaged across 5 strides for each condition. The 5 strides were identified using vertical accelerometer data from the sensor placed on the biceps femoris within the 30 s collected. The first 5 strides available were used for analysis, unless the EMG signal was interrupted, at which point, the first uninterrupted 5 strides of data were used. The EMG activity (in μV) was then averaged across these five values and used for statistical analysis. DC bias was removed from the data and a full wave rectification was applied.
The SF for each condition was determined using accelerometer data obtained from the EMG sensor on the biceps femoris. The time (in seconds) for 5 complete strides was determined and the average time per stride was calculated and used for analysis.
4.7. Statistical Analysis
The results were analyzed using SPSS, version 29 (IBM, Armonk, NY, USA) using an alpha level of 0.05. The data were screened for outliers, defined as scores with standardized values of >3.0 from the group mean, and none were detected. The Shapiro–Wilk test was used to determine if the distribution of scores in each group was approximately normal.
A series of one-way repeated-measures ANOVAs was used to determine differences between the four conditions (control, AT, KT, and spring) for the following variables: VO2, EMGrectus, EMGbiceps, and SF. Additional repeated-measures ANOVAs were used to determine if there were differences between conditions for RPE and HR, variables which served as a verification that approximately equivalent levels of cardiovascular and psychological strain between conditions were encountered.
Violations of the assumption of sphericity (
p < 0.05) were determined using Mauchley’s Test. In such instances, Greenhouse–Geisser-adjusted results are reported. In the case of a significant ANOVA (
p < 0.05), Bonferroni-adjusted post hoc tests would be used to ensure a test-wise alpha level of 0.05. The effect sizes for the ANOVA results are reported as partial eta squared (
η2) and interpreted according to the following benchmark values: small (0.01), medium (0.06), and large (0.14) [
33].






{kind=link}
{kind=link}