
A Case of a Patient Who Successfully Achieved Early Wound Closure by Local Negative Pressure Wound Therapy (NPWT) against Compromised Wound Healing after Arterio-Venous Graft Infection


Abstract
:1. Background
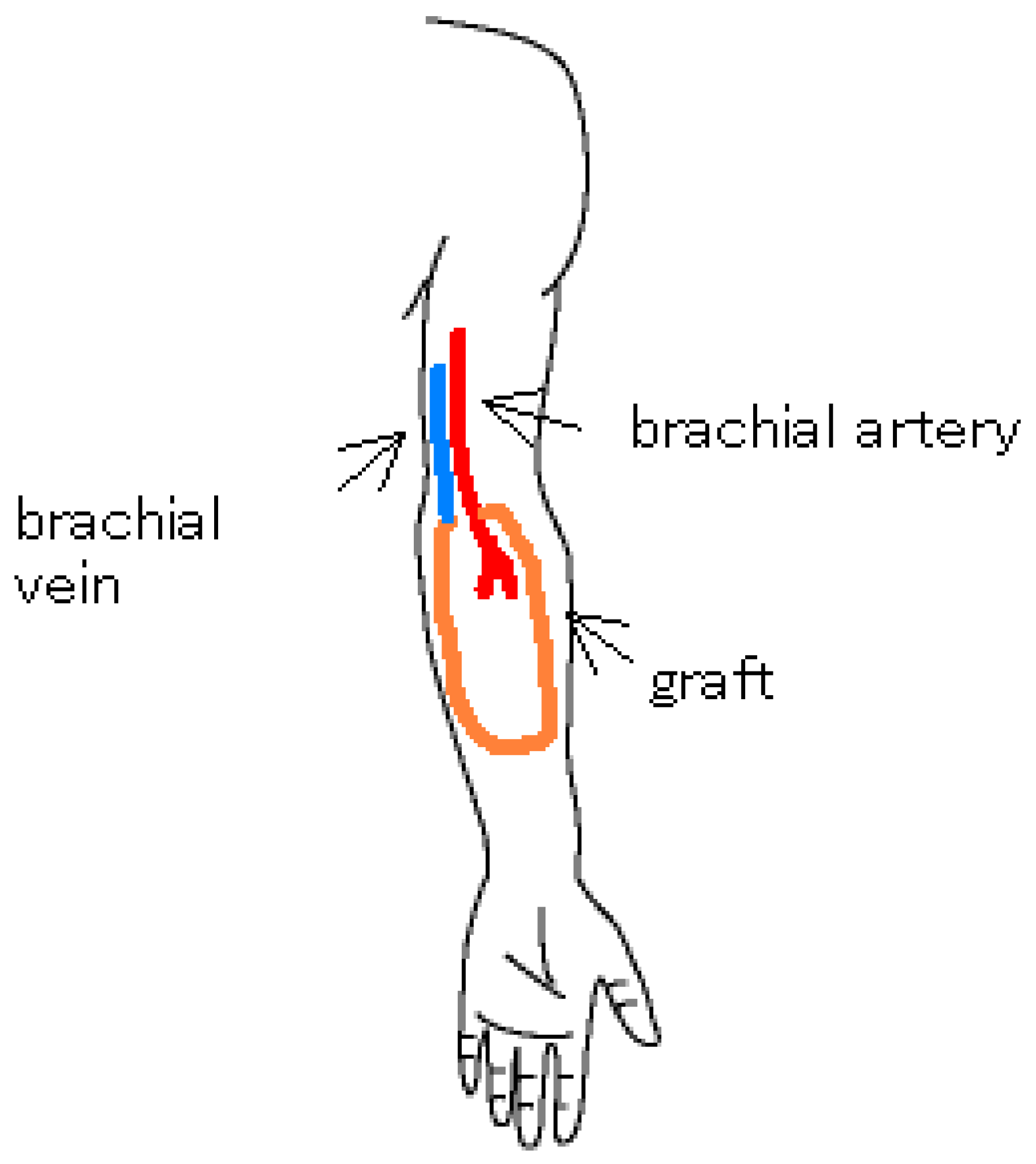
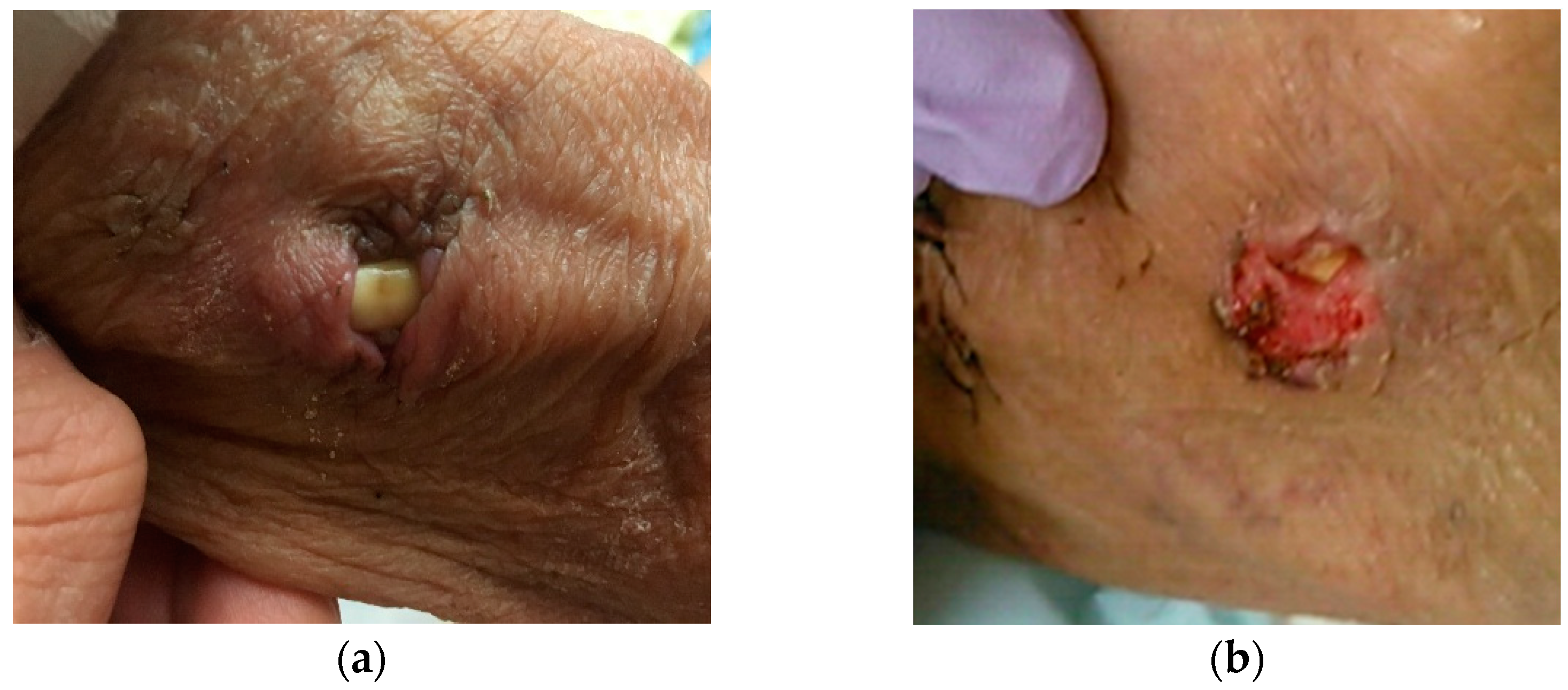
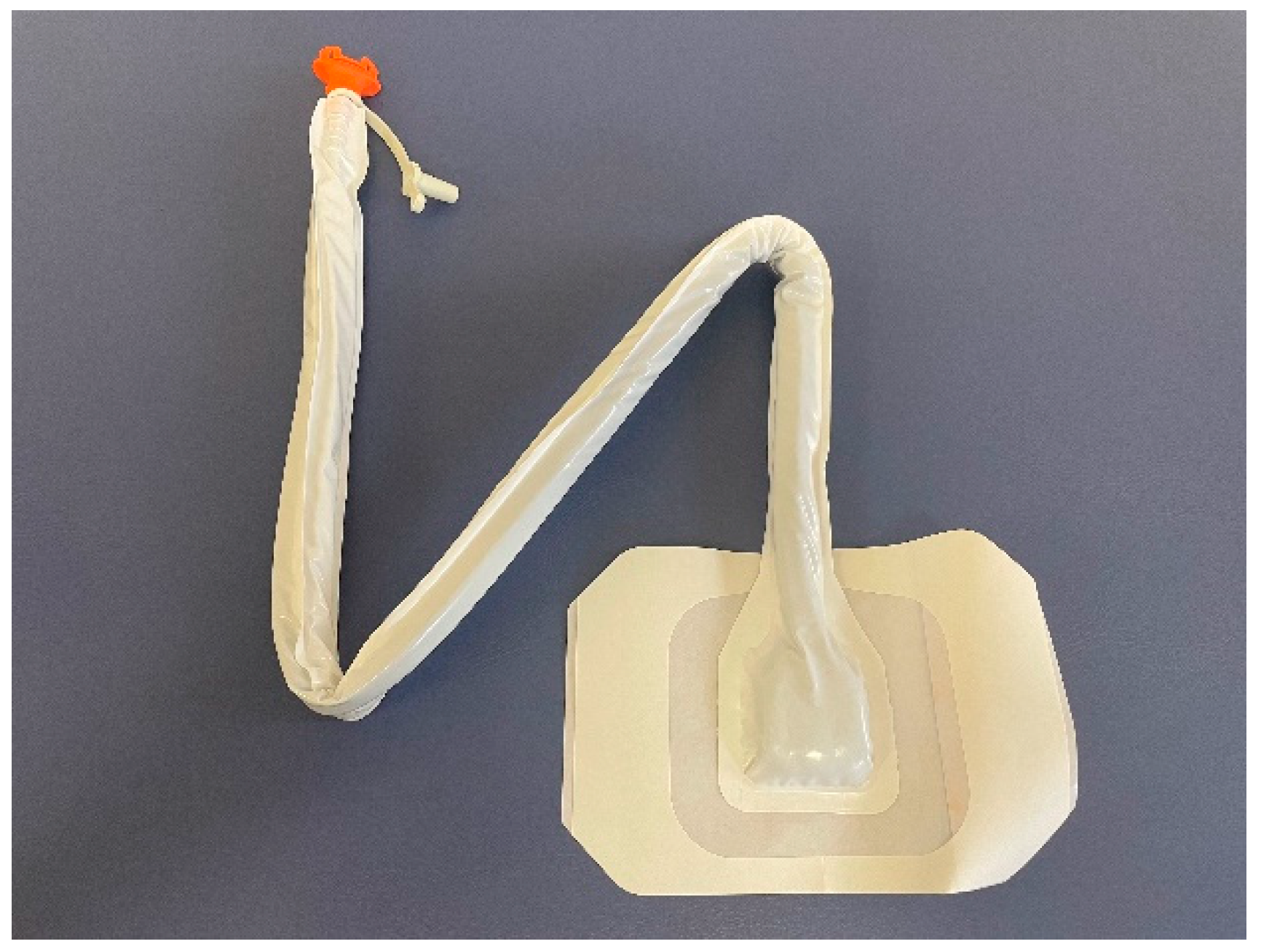
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Ryan, S.V.; Calligaro, K.D.; Scharff, J.; Dougherty, M.J. Management of infected prosthetic dialysis arteriovenous grafts. J. Vasc. Surg. 2004, 39, 73–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Argenta, L.C.; Morykwas, M.J. Vacuum-assisted closure: A new method for wound control and treatment: Clinical experience. Ann. Plast. Surg. 1997, 38, 563–576. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, P.; Kukrele, R.; Sharma, D. Vacuum assisted closure (VAC)/negative pressure wound therapy (NPWT) for difficult wounds: A review. J. Clin. Orthop. Trauma 2019, 10, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; A Lavery, L.; Abu-Rumman, P.; Espensen, E.H.; Vazquez, J.R.; Nixon, B.P.; Boulton, A.J.M. Outcomes of subatmospheric pressure dressing therapy on wounds of the diabetic foot. Ostomy Wound Manag. 2002, 48, 64–68. [Google Scholar]
- Apelqvist, J.; Armstrong, D.G.; Lavery, L.A.; Boulton, A.J. Resource utilization and economic costs of care based on a randomized trial of vacuum-assisted closure therapy in the treatment of diabetic foot wounds. Am. J. Surg. 2008, 195, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Borgquist, O.; Ingemansson, R.; Malmsjö, M. The Influence of Low and High Pressure Levels during Negative-Pressure Wound Therapy on Wound Contraction and Fluid Evacuation. Plast. Reconstr. Surg. 2011, 127, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Kairinos, N.; Solomons, M.; Hudson, D.A. Negative-Pressure Wound Therapy I: The Paradox of Negative-Pressure Wound Therapy. Plast. Reconstr. Surg. 2009, 123, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Minga, T.E.; Flanagan, K.H.; Allon, M. Clinical consequences of infected arteriovenous grafts in hemodialysis patients. Am. J. Kidney Dis. 2001, 38, 975–978. [Google Scholar] [CrossRef] [PubMed]
- Hisashi, S. Vacuum Assisted Closure on Infected Prosthetic Vascular Grafts in the Groin. Jpn. J. Vasc. Surg. 2020, 29, 271–274. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Blood Counts | Value | Unit |
|---|---|---|
| White blood cell | 7500 | /μL |
| Neutrophil | 73.2% | |
| Eosinophil | 3.6% | |
| Basophil | 0.5% | |
| Monocyte | 5.9% | |
| Lymphocyte | 16.8% | |
| Red blood cell | 290 | ×104/μL |
| Hemoglobin | 8.9 | g/dL |
| Platelet | 19.7 | ×104/μL |
| Blood chemistry | ||
| Sodium | 136 | mEq/L |
| Potassium | 5.4 | mEq/L |
| Chloride | 99 | mEq/L |
| Calcium | 7.8 | mg/dL |
| Phosphorus | 5.5 | mg/dL |
| Urea nitrogen | 56.6 | mg/dL |
| Creatinine | 5.19 | mg/dL |
| Total protein | 6.6 | mg/dL |
| Albumin | 4.2 | mg/dL |
| AST | 28 | U/L |
| ALT | 8 | U/L |
| ALP | 253 | U/L |
| γGTP | 44 | U/L |
| CK | 354 | U/L |
| Total bilirubin | 0.2 | mg/dL |
| Glucose | mg/dL | |
| C-reactive protein | 0.02 | mg/dL |
| Procalcitonin | <0.5 | ng/mL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kusuta, R.; Shimazu, K.; Mizoguchi, K.; Komura, K.; Tanaka, A. A Case of a Patient Who Successfully Achieved Early Wound Closure by Local Negative Pressure Wound Therapy (NPWT) against Compromised Wound Healing after Arterio-Venous Graft Infection. Kidney Dial. 2021, 1, 14-19. https://doi.org/10.3390/kidneydial1010003
Kusuta R, Shimazu K, Mizoguchi K, Komura K, Tanaka A. A Case of a Patient Who Successfully Achieved Early Wound Closure by Local Negative Pressure Wound Therapy (NPWT) against Compromised Wound Healing after Arterio-Venous Graft Infection. Kidney and Dialysis. 2021; 1(1):14-19. https://doi.org/10.3390/kidneydial1010003
Chicago/Turabian StyleKusuta, Risa, Keiji Shimazu, Kazuhiro Mizoguchi, Kazumasa Komura, and Atsuo Tanaka. 2021. "A Case of a Patient Who Successfully Achieved Early Wound Closure by Local Negative Pressure Wound Therapy (NPWT) against Compromised Wound Healing after Arterio-Venous Graft Infection" Kidney and Dialysis 1, no. 1: 14-19. https://doi.org/10.3390/kidneydial1010003