
Digital Mounting Jigs: A Novel Technique


1
Division of Prosthodontics, Department of Restorative Sciences, University of Minnesota, Minneapolis, MN 55455, USA
2
Division of Endodontics, Department of Restorative Sciences, University of Minnesota, Minneapolis, MN 55455, USA
*
Author to whom correspondence should be addressed.
Digital 2022, 2(2), 164-170; https://doi.org/10.3390/digital2020010
Submission received: 9 March 2022
/
Revised: 8 April 2022
/
Accepted: 12 April 2022
/
Published: 14 April 2022
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:The accuracy with which virtual articulators are able to simulate centric and eccentric movements when fabricating definitive restorations has not yet been proven to be on par with mechanical articulators which have been reliably used in restorative dentistry for decades. This may be an issue when working on complex restorative cases utilizing a digital workflow and could result in considerable chairside adjustment time and subsequent loss of occlusal anatomy and morphology. Interchanging between digital and analog workflows is a challenge as accurate cross-mounting is difficult due to the changes that occur as the digital and analog workflows progress. This technique article provides a method for the fabrication of simple digital mounting jigs that enable clinicians and laboratory technicians to mount printed digital wax-ups and working casts back onto a programmed mechanical articulator, opposing diagnostic casts that have originally been mounted by means of a facebow transfer. This allows for the positioning of printed digital wax-ups and working casts to be in the correct 3-dimensional spatial relationship on the mechanical articulator for any necessary occlusal adjustments of the digitally designed wax-ups and/or definitive restorations before they are moved chairside.
1. Introduction
The use of digital technology in dentistry has increased significantly in the past decade. Digital workflows bring many advantages, namely predictability and improved esthetic outcomes [1,2,3,4]. Utilizing digital workflows for procedures such as wax-ups provides improved symmetry due to reduced human error and allows restorations to be designed while referencing facial features which is challenging with analog wax-up techniques [2,4,5]. One of the limitations of digital wax-ups and subsequent restorations is the usage of a virtual articulator. Although there has been significant improvement with virtual articulators over the past few years since their introduction in the late 1990s [6], a standardized technique for their use has not been established [7]. Furthermore, no studies compare or validate the accuracy of currently available virtual mounting techniques [7].
Contrary to analog mounting techniques using a facebow transfer, a method widely accepted for mounting casts in the correct frontal, horizontal and sagittal planes [8], digitally relating the maxilla to the condyles using contemporary techniques is a long process that usually requires a CBCT scan to identify landmarks before overlaying data [7,9,10]. Digital facebows have been suggested in lieu of CBCT scans for virtual mounting, but their accuracy is questionable and has not been validated. Further, they require advanced knowledge of digital concepts and tools such as facial scanners [11,12,13].
Accurate mounting is required for clinicians to develop and design specific occlusal schemes for complex cases. Regardless of the preferred concept or philosophy, an appropriate occlusal scheme that is reflected in anatomy such as cusp heights and ridge and groove directions is vital for the long-term success of prosthetic rehabilitations [14]. Multiple studies have been conducted on virtual articulators to compare occlusal contacts with natural dentition or mechanical articulators [15,16,17]. Although most studies found that virtual articulators provided similar occlusal contacts, their focus was on maximum intercuspation, and no eccentric movements were considered. Limited studies that considered dynamic movements provided contradicting findings. Hsu et al. showed that dynamic movements on virtual and mechanical articulators were equally accurate [18]. but a more recent study by Buduru et al. concluded that mechanical semi-adjustable articulators were superior in both static and dynamic occlusion [19].
As a result of the current limitations of virtual mounting and articulation, clinicians and laboratory technicians may decide to mount printed digital wax-ups and working casts of complex cases back onto a mechanical articular to verify and adjust occlusion. Cross-mounting casts in the correct 3-dimensional spatial relationship on the mechanical articulator is challenging due to the changes that occur within the digital workflow. To overcome these challenges, this article presents a simple technique that utilizes free software (Autodesk MeshMixer; Autodesk Inc., San Rafael, CA, USA) to create mounting jigs that allow for cross-mounting of printed and analog casts while moving through different workflows, provided that the original diagnostic casts were mounted on a mechanical articulator in centric relation (CR) at the desired vertical dimension of occlusion (VDO) by means of a facebow transfer.
2. Technique
- Mount the diagnostic casts in CR at the desired VDO on a mechanical articulator using a facebow transfer and program the articulator to simulate the patient’s eccentric movements.
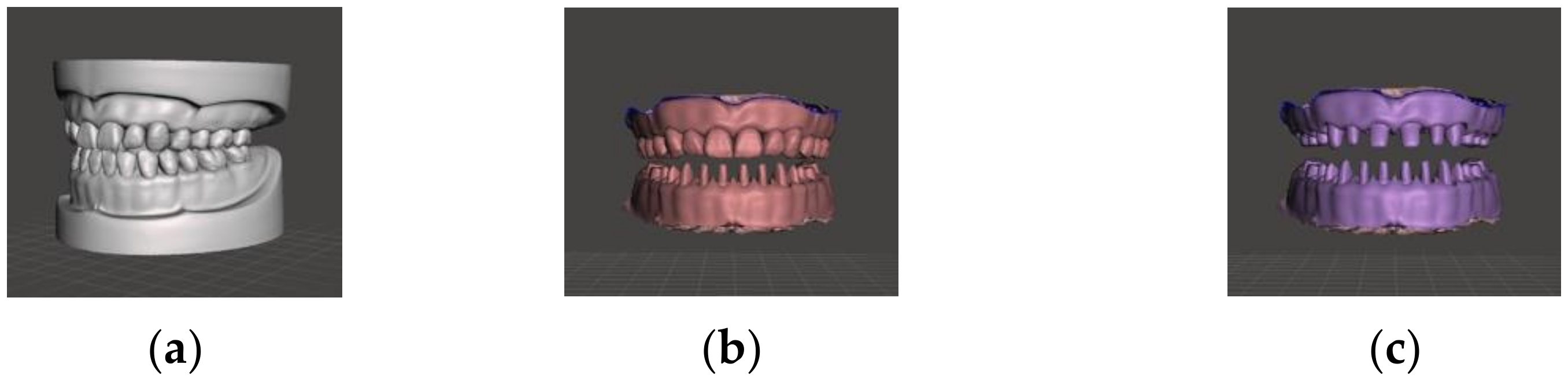
- Scan the maxillary and mandibular casts individually via desktop scanner (E4 Scanner; 3Shape, Copenhagen, Denmark) to obtain Standard Tessellation Language (STL) files, and then scan the articulator mounting (jaw relation record) to virtually relate the STL files (Figure 1a).
- Prepare patient’s mandibular teeth while ensuring that the maxilla remains unchanged. Using an intraoral scanner (TRIOS3; 3Shape, Copenhagen, Denmark), make a final impression of the unprepared maxillary and prepared mandibular arches followed by jaw relations records in CR at the pre-determined VDO (Figure 1b).
- Prepare the maxillary teeth and make a final impression scan of the prepared maxilla and mandible and jaw relation records in CR while maintaining the same VDO (Figure 1c). Import the STL files of all three sets of scans into MeshMixer (Autodesk MeshMixer; Autodesk Inc., San Rafael, CA, USA) and begin the virtual alignment procedure.
Figure 1.
(a) Digitally articulated diagnostic casts (grey) in CR at the desired VDO. (b) Final impression scan (pink) of mandibular preparations and intact maxillary arch. (c) Final impression scan (purple) of maxillary and mandibular preparation arches.
Figure 1.
(a) Digitally articulated diagnostic casts (grey) in CR at the desired VDO. (b) Final impression scan (pink) of mandibular preparations and intact maxillary arch. (c) Final impression scan (purple) of maxillary and mandibular preparation arches.

- 5.
- Align the unprepared maxillary/prepared mandibular casts to the diagnostic casts by using the maxilla as a reference (Figure 2a). Then, align the working casts of both prepared arches to the unprepared maxillary/prepared mandibular casts using the mandibular preparations as a reference (Figure 2b). The three sets of scans should now be virtually aligned. After alignment, hide the scan of the unprepared maxillary/prepared mandibular arches as it is no longer required.
- 6.
- Append a rectangular block with a thickness of 2–5 mm, depending on the available inter-arch space, and place it between both arches. Akin to analog interocclusal records, the rectangular block extends to register the cusp/prep tips. Hide the mandibular working cast and reveal the original mandibular diagnostic cast to have it oppose the maxillary working cast.
- 7.
- Combine the maxillary working cast and the mandibular diagnostic cast by selecting both layers simultaneously and selecting ‘combine’ on the upper left side bar (Figure 3).
- 8.
- From the object viewer, select the combined casts and the rectangular block layers. The Boolean difference option will appear on the upper left side bar. This feature works by subtracting objects in areas where they intersect; thus, a digital bite registration is made between the maxillary working cast on the upper surface and the mandibular diagnostic cast on the lower surface. This forms ‘digital mounting jig #1’ that can now be exported and printed (Figure 4a).
- 9.
- Export digital mounting jig #1 by going to file > export and proceed with the 3D printing process on your printer of choice, using any of the model resins. Follow post-processing and curing instructions recommended by the manufacturer for the resin and curing unit used (Figure 4b).
Figure 4.
(a) A digital bite registration is obtained on the rectangular block after a Boolean difference. This forms ‘digital mounting jig #1’ that can be exported and printed. (b) The 3D printed jig after printing, post-processing and curing.
Figure 4.
(a) A digital bite registration is obtained on the rectangular block after a Boolean difference. This forms ‘digital mounting jig #1’ that can be exported and printed. (b) The 3D printed jig after printing, post-processing and curing.

- 10.
- Seat the jig onto the previously mounted mandibular diagnostic cast, which is preserving the 3-dimensional spatial relationship, and place the printed maxillary working cast on the opposing surface. Mount the maxillary working cast to the mechanical articulator (Figure 5).
- 11.
- Fabricate ‘digital mounting jig #2’ to mount the mandibular working cast. Append a new rectangular block between the two working casts and follow the same steps. Once the casts are combined, perform a Boolean difference to create jig #2 and proceed to printing.
- 12.
- 13.
- Adjust centric and eccentric contacts on the wax-up, provisional, or definitive restorations fabricated digitally onto the mechanical articulator until they are deemed satisfactory.
3. Discussion
This novel technique presents the steps for the fabrication of mounting jigs that can be used to mount printed working casts onto the mechanical articulator to perform final occlusal adjustments on definitive restorations before they are moved chairside. The same technique may be used to mount printed wax-up casts in order to perform similar adjustments. For the jigs to provide accurate results, it is critical to ensure that CR and VDO are maintained by using a modified Lucia jig or similar jigs and that all reference casts are accurately aligned. This may be done automatically by the software or manually through a single- or three-point alignment technique [20,21,22]. Alignment using this technique not only improves accuracy by relying on stable hard tissue references but also verifies the CR record as multiple scans are obtained.
Positional changes of the digital working cast relative to the reference axes on the mechanical articulator will result in changes to the orientation of the occlusal plane. As a result, the anatomy, tooth morphology, and orientation of the ridge and groove direction will be affected. These features are important in the development of a harmonious occlusal scheme, particularly with posterior group function [23]. The use of a facebow to record the horizontal orientation as well as the frontal and sagittal inclinations of the occlusal plane results in improved outcomes as a result of developing appropriate morphology and occlusal contacts [24,25,26,27].
This technique is advantageous for multiple reasons. The open software, ease of fabrication, and minimal cost of 3D printing make it an ideal method of combining workflows. The rectangular block used to fabricate the jig is one of the preset shapes on the software, which makes it convenient to append and use. Adjusting occlusion on a mechanical articulator after digital fabrication of restorations may result in reduced chairside occlusal adjustments and the preservation of occlusal anatomy, particularly when multiple restorations are being simultaneously delivered. Additionally, interproximal contacts may also be adjusted on the solid printed cast to further reduce chairside adjustment time. Clinicians wishing to challenge certifying examinations, such as Board Certification by The American Board of Prosthodontics (ABP), would benefit greatly from this technique as it would allow them to accurately re-approximate casts on mechanical articulators should they decide to utilize a digital workflow. The ABP allows the use of digital workflows but requires candidates to present physical casts mounted on an articulator during the examination, regardless of the workflow of choice [28]. Although this technique was described for restorative dentistry procedures, it is applicable to other specialties such as orthodontics as they may find it useful to cross mount digitally acquired casts on to a physical articulator for a closer assessment of occlusion.
As with other digital workflows, this technique is limited by the accuracy of the intraoral and desktop scanners, 3D printer, resin material, printing parameters, and post-printing processing which includes polymerization shrinkage, amongst others. Depending on the 3D printer and resins used, polymerization shrinkage that occurs after curing may make complete seating of casts into the jigs challenging. Clinicians can overcome this limitation by offsetting casts prior to making the respective jigs. Offsetting creates an iota of uniform spacing between the cast and the corresponding jig, thereby accounting for potential shrinkage. Although they fall within a close range, recommended offset parameters differ depending on the manufacturer and should be followed to ensure ideal outcomes. In addition, shortcomings of the different software that may be necessary for scanning and trimming casts, alignment, jig design, as well as operator experience all could directly influence the final outcome [19].
Although this technique addresses current limitations in the digital workflow, the rapid progression of digital dentistry may result in virtual articulators and/or virtual patients that are on par or superior to mechanical articulators. Until such virtual articulators are developed and accompanying workflows become relatively simple to follow, mechanical articulators remain an important tool for successful prosthetic outcome in complex rehabilitations.
4. Conclusions
This article presents clinicians and laboratory technicians with a simple method for the fabrication of digital mounting jigs to allow for cross mounting between the digital and analog workflows for complex restorative cases, while preserving the 3-dimensional spatial relationship of the casts. This may allow for better occlusal harmony, reduced chairside time, preservation of tooth anatomy and maintaining the bulk strength of the digitally fabricated restorations. Shortcomings pertaining to scanning and printing errors should be taken into account to minimize the potential for cross mounting errors.
Author Contributions
Conceptualization, M.A.A.; Methodology, M.A.A., D.E.M., W.S., F.Z.; Writing—original draft preparation, M.A.A., D.E.M.; Writing—review and editing, W.S., F.Z.; Visualization, M.A.A., D.E.M.; Supervision, W.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Marsango, V.; Bollero, R.; D’Ovidio, N.; Miranda, M.; Bollero, P.; Barlattani, A., Jr. Digital work-flow. Oral Implantol. (Rome) 2014, 7, 20–24. [Google Scholar] [CrossRef]
- Garcia, P.P.; da Costa, R.G.; Calgaro, M.; Ritter, A.V.; Correr, G.; Da Cunha, L.F.; Gonzaga, C.C. Digital smile design and mock-up technique for esthetic treatment planning with porcelain laminate veneers. J. Conserv. Dent. 2018, 21, 455–458. [Google Scholar] [PubMed]
- Coachman, C.; De Arbeloa, L.; Mahn, G.; Sulaiman, T.; Mahn, E. An improved direct injection technique with flowable composites: A digital workflow case report. J. Oper. Dent. 2020, 45, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Akl, M.A.; Wee, A.G. From virtual smile design to guided wax-up using Adobe Photoshop. Int. J. Prosthodont. Restor. Dent. 2020, 10, 176–179. [Google Scholar] [CrossRef]
- Abduo, J. Morphological symmetry of maxillary anterior teeth before and after prosthodontic planning: Comparison between conventional and digital diagnostic wax-ups. Med. Princ. Pract. 2016, 25, 276–281. [Google Scholar] [CrossRef]
- Szentpétery, A. Dinamikus rágófelszín-kialakítás CAD/CAM-módszerekkel. I. rész. Fogaszati CAD/CAM-rendszerek altalanos ismertetese [Dynamic correction of occlusal surfaces with CAD/CAM methods. Part I. General description of dental CAD/CAM-systems]. Fogorv. Szle. 1999, 92, 231–242. (In Hungarian) [Google Scholar]
- Lepidi, L.; Galli, M.; Mastrangelo, F.; Venezia, P.; Joda, T.; Wang, H.L.; Li, J. Virtual articulators and virtual mounting procedures: Where do we stand? J. Prosthodont. 2021, 30, 24–35. [Google Scholar] [CrossRef]
- Samet, N.; Smidt, A.; Samet, N.; Weiss, E.I. A clinical and cost-benefit evaluation of five facebows. Quintessence Int. 2002, 33, 511–515. [Google Scholar]
- Lepidi, L.; Chen, Z.; Ravida, A.; Lan, T.; Wang, H.-L.; Li, J. A full-digital technique to mount a maxillary arch scan on a virtual articulator. J. Prosthodont. 2019, 28, 335–338. [Google Scholar] [CrossRef]
- Lepidi, L.; Suriano, C.; Wang, H.L.; Granata, S.; Joda, T.; Li, J. Digital fixed complete-arch rehabilitation: From virtual articulator mounting to clinical delivery. J. Prosthet. Dent. 2020, in press. [Google Scholar] [CrossRef]
- Solaberrieta, E.; Mínguez, R.; Barrenetxea, L.; Etxaniz, O. Direct transfer of the position of digitized casts to a virtual articulator. J. Prosthet. Dent. 2013, 109, 411–414. [Google Scholar] [CrossRef]
- Solaberrieta, E.; Otegi, J.R.; Mínguez, R.; Etxaniz, O. Improved digital transfer of the maxillary cast to a virtual articulator. J. Prosthet. Dent. 2014, 112, 921–924. [Google Scholar] [CrossRef] [PubMed]
- Solaberrieta, E.; Mínguez, R.; Barrenetxea, L.; Otegi-Olaso, J.R.; Szentpétery, A. Comparison of the accuracy of a 3-dimensional virtual method and the conventional method for transferring the maxillary cast to a virtual articulator. J. Prosthet. Dent. 2015, 113, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, B.; Ladha, K.; Lalit, A.; Naik, B.D. Occlusal concepts in full mouth rehabilitation: An overview. J. Indian Prosthodont. Soc. 2014, 14, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Delong, R.; Ko, C.C.; Anderson, G.C.; Hodges, J.S.; Douglas, W. Comparing maximum intercuspal contacts of virtual dental patients and mounted dental casts. J. Prosthet. Dent. 2002, 88, 622–630. [Google Scholar] [CrossRef] [PubMed]
- Krahenbuhl, J.T.; Cho, S.H.; Irelan, J.; Bansal, N.K. Accuracy and precision of occlusal contacts of stereolithographic casts mounted by digital interocclusal registrations. J. Prosthet. Dent. 2016, 116, 231–236. [Google Scholar] [CrossRef] [Green Version]
- Úry, E.; Fornai, C.; Weber, G.W. Accuracy of transferring analog dental casts to a virtual articulator. J. Prosthet. Dent. 2020, 123, 305–313. [Google Scholar] [CrossRef]
- Hsu, M.R.; Driscoll, C.F.; Romberg, E.; Masri, R. Accuracy of dynamic virtual articulation: Trueness and precision. J. Prosthodont. 2019, 28, 436–443. [Google Scholar] [CrossRef]
- Buduru, S.; Finta, E.; Almasan, O.; Fluerasu, M.; Manziuc, M.; Iacob, S.; Culcitchi, C.; Negucioiu, M. Clinical occlusion analysis versus semi-adjustable articulator and virtual articulator occlusion analysis. Med. Pharm. Rep. 2020, 93, 292–296. [Google Scholar] [CrossRef]
- Cattoni, F.; Teté, G.; Calloni, A.M.; Manazza, F.; Gastaldi, G.; Capparè, P. Milled versus moulded mock-ups based on the superimposition of 3D meshes from digital oral impressions: A comparative in vitro study in the aesthetic area. BMC Oral Health 2019, 19, 230. [Google Scholar] [CrossRef]
- Moldovani, D.; Diamantopoulou, S.; Edelhoff, D.; Papazoglou, E. Accuracy of indirect veneer mock-up in comparison to diagnostic wax-up. Int. J. Prosthodont. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.; Shull, F.; Schiner, B. Maxillary full-arch reconstruction using a sequenced digital workflow. J. Esthet. Restor. Dent. 2020, 32, 336–356. [Google Scholar] [CrossRef] [PubMed]
- Seong, W.J.; Polack, M.A.; Delima, L.F.; Lee, J. Technique to maintain the correct spatial orientation of the maxillary diagnostic cast to that of the master cast in a full-mouth rehabilitation case. J. Prosthodont. 2021, 30, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Palaskar, J.N.; Joshi, N.; Gullapalli, P.; Shah, P. Comparative evaluation of sagittal inclination of the occlusal plane with Frankfort horizontal plane in facebow transfers to semi adjustable and fully adjustable articulators. J. Prosthet. Dent. 2020, 123, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Stade, E.H.; Hanson, J.G.; Baker, C.L. Esthetic considerations in the use of face-bows. J. Prosthet. Dent. 1982, 48, 253–256. [Google Scholar] [CrossRef]
- Okane, H.; Yamashina, T.; Nagasawa, T.; Tsuru, H. The effect of anteroposterior inclination of the occlusal plane on biting force. J. Prosthet. Dent. 1979, 42, 497–501. [Google Scholar] [CrossRef]
- Ogawa, T.; Koyano, K.; Umemoto, G. Inclination of the occlusal plane and occlusal guidance as contributing factors in mastication. J. Dent. 1998, 26, 641–647. [Google Scholar] [CrossRef]
- Examination Guidelines for the Certification Process [ebook]: The American Board of Prosthodontics. pp. 20–21. Available online: https://www.abpros.org/application/files/6716/2342/2018/ABP-Guidelines-2021-06-11.pdf (accessed on 2 December 2021).
Figure 2.
(a) Alignment of unprepared maxillary/prepared mandibular casts (pink) to diagnostic casts (grey) using the maxillary arch as a reference. (b) Alignment of the working casts of both prepared arches (purple) to the unprepared maxillary/prepared mandibular casts (pink) using the mandibular preparations as a reference. The pink and purple “speckles” showing through the aligned side confirms accurate alignment as it indicates overlapping of the meshes.
Figure 2.
(a) Alignment of unprepared maxillary/prepared mandibular casts (pink) to diagnostic casts (grey) using the maxillary arch as a reference. (b) Alignment of the working casts of both prepared arches (purple) to the unprepared maxillary/prepared mandibular casts (pink) using the mandibular preparations as a reference. The pink and purple “speckles” showing through the aligned side confirms accurate alignment as it indicates overlapping of the meshes.

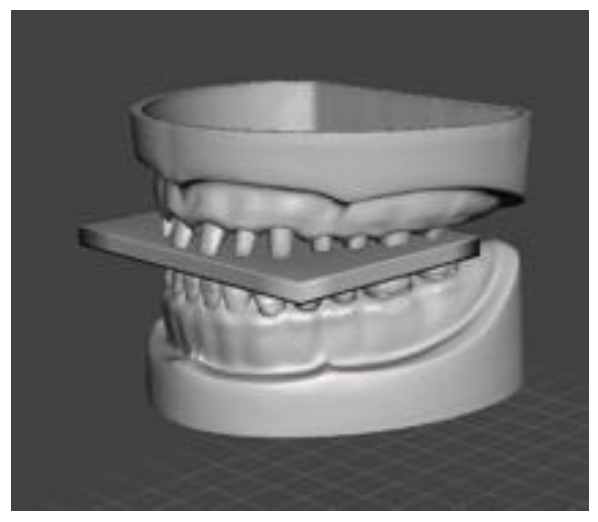
Figure 3.
The rectangular block is placed between the maxillary working cast and mandibular diagnostic cast.
Figure 3.
The rectangular block is placed between the maxillary working cast and mandibular diagnostic cast.

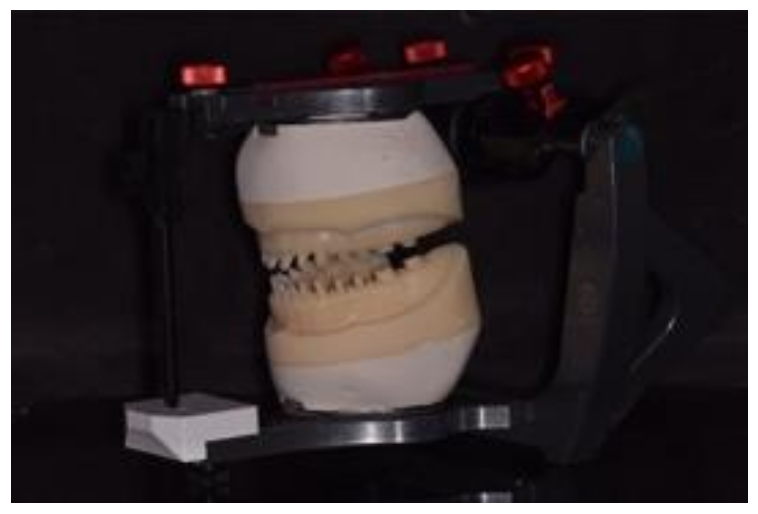
Figure 5.
The maxillary working cast is positioned onto the mechanical articulator using digital mounting jig #1 against the previously mounted mandibular diagnostic cast.
Figure 5.
The maxillary working cast is positioned onto the mechanical articulator using digital mounting jig #1 against the previously mounted mandibular diagnostic cast.

Figure 6.
The mandibular working cast is mounted against the maxillary working cast using digital mounting jig #2.
Figure 6.
The mandibular working cast is mounted against the maxillary working cast using digital mounting jig #2.

Figure 7.
The maxillary and mandibular printed working casts are mounted in CR at the desired VDO on a mechanical articulator.
Figure 7.
The maxillary and mandibular printed working casts are mounted in CR at the desired VDO on a mechanical articulator.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Akl, M.A.; Mansour, D.E.; Zheng, F.; Seong, W. Digital Mounting Jigs: A Novel Technique. Digital 2022, 2, 164-170. https://doi.org/10.3390/digital2020010
AMA Style
Akl MA, Mansour DE, Zheng F, Seong W. Digital Mounting Jigs: A Novel Technique. Digital. 2022; 2(2):164-170. https://doi.org/10.3390/digital2020010
Chicago/Turabian StyleAkl, Mohammed A., Dina E. Mansour, Fengyuan Zheng, and WookJin Seong. 2022. "Digital Mounting Jigs: A Novel Technique" Digital 2, no. 2: 164-170. https://doi.org/10.3390/digital2020010