
Role of 18F-FDG PET/CT in the Management of Patients Affected by HHV-8-Associated Multicentric Castleman’s Disease

Abstract
:1. Introduction
2. Materials and Methods
2.1. 18F-FDG PET/CT Protocol and Interpretation
2.2. Conventional Imaging
2.3. Statistical Analysis
3. Results
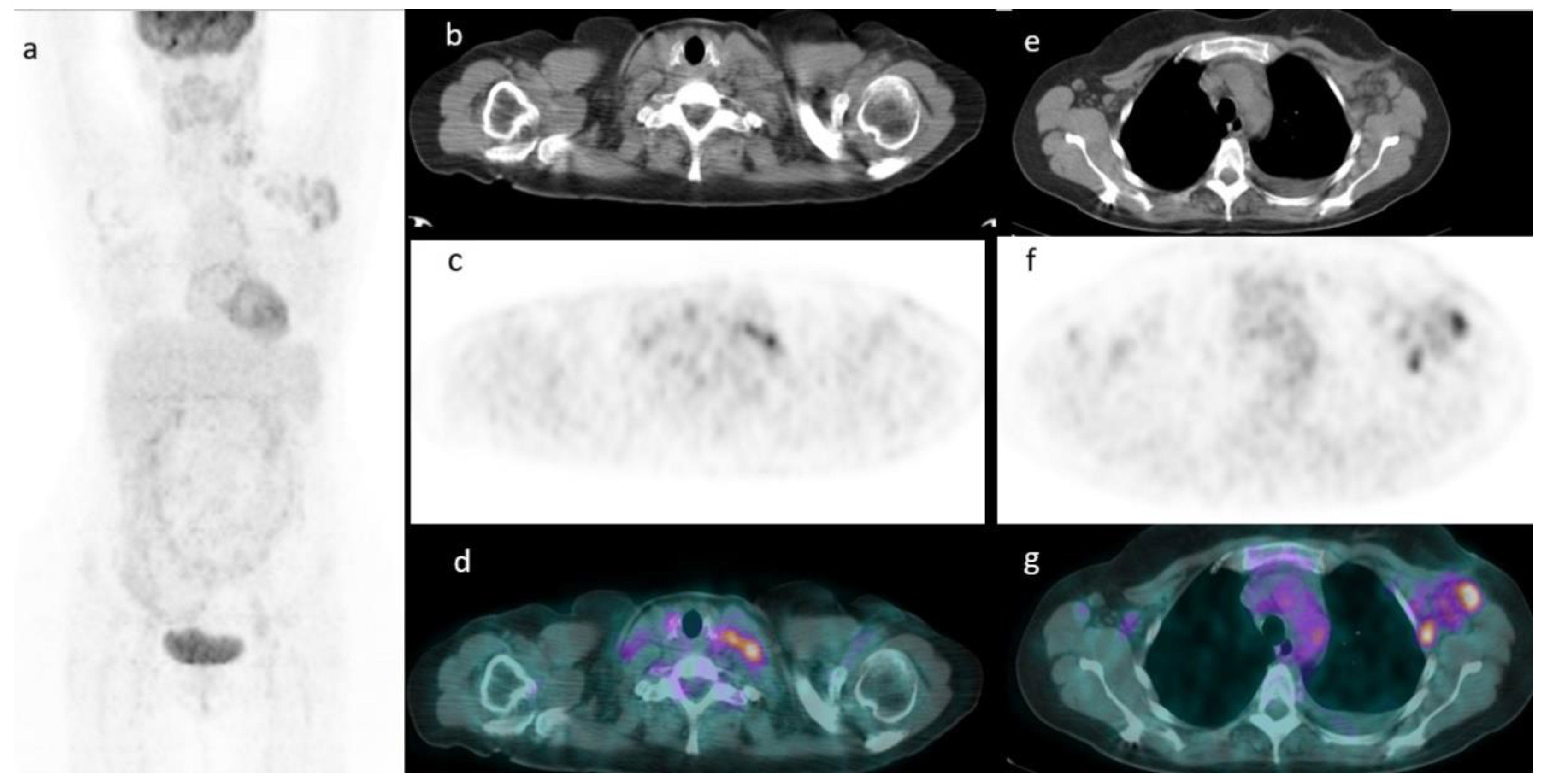
3.1. 18F-FDG PET/CT Baseline Findings
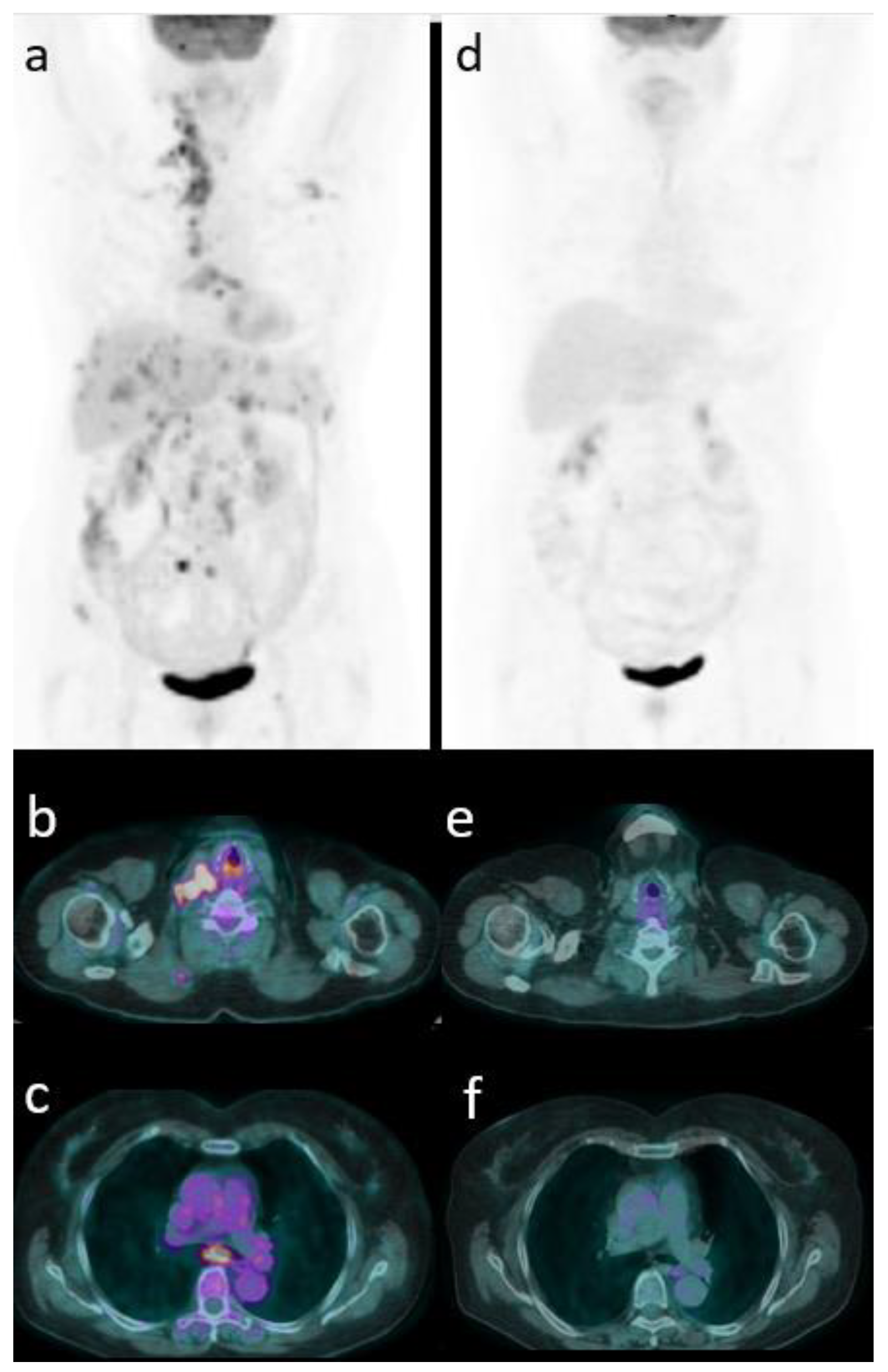
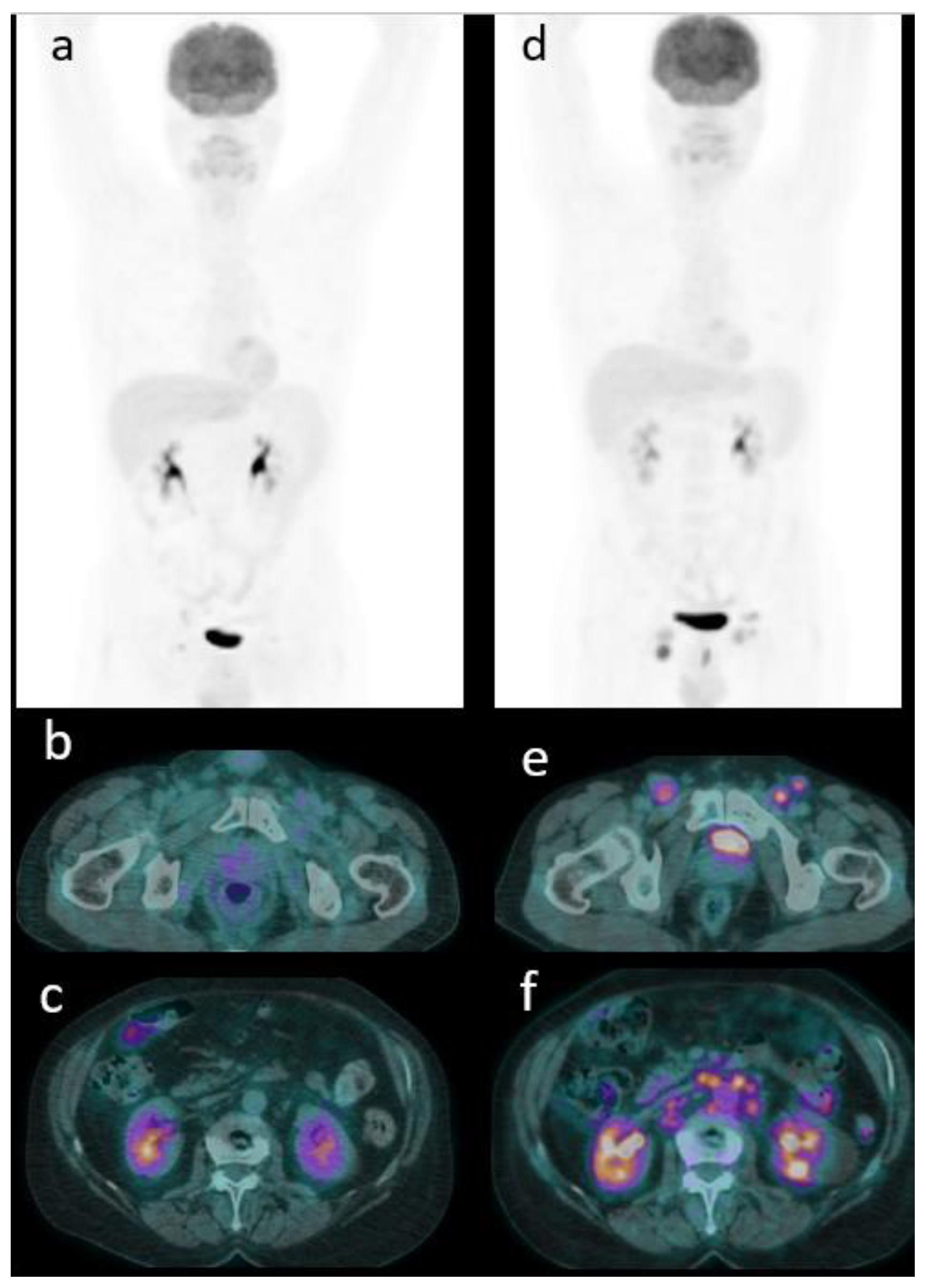
3.2. Restaging/Follow Up 18F-FDG PET/CT and Comparison with Other Imaging Modalities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fajgenbaum, D.; Uldrick, T.S.; Bagg, A.; Frank, D.; Wu, D.; Srkalovic, G.; Simpson, D.; Liu, A.Y.; Menke, D.; Chandrakasan, S.; et al. International, evidence-based consensus diagnostic criteria for HHV-8-negative/idiopathic multicentric Castleman disease. Blood 2017, 129, 1646–1657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, J.P.; Shen, X.F.; Du, J.-F.; Guan, W.-X. A retrospective study of 34 patients with unicentric and multicentric Castleman’s disease: Experience from a single institution. Oncol. Lett. 2018, 15, 2407–2412. [Google Scholar] [PubMed] [Green Version]
- Oksenhendler, E.; Boutboul, D.; Fajgenbaum, D.; Mirouse, A.; Fieschi, C.; Malphettes, M.; Vercellino, L.; Meignin, V.; Gérard, L.; Galicier, L. The full spectrum of Castleman disease: 273 patients studied over 20 years. Br. J. Haematol. 2017, 180, 206–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fajgenbaum, D.C.; van Rhee, F.; Nabel, C.S. HHV-8-negative, idiopathic multicentric Castleman disease: Novel insights into biology, pathogenesis, and therapy. Blood 2014, 123, 2924–2933. [Google Scholar] [CrossRef] [PubMed]
- Pria, A.D.; Pinato, D.; Roe, J.; Naresh, K.; Nelson, M.; Bower, M. Relapse of HHV8-positive multicentric Castleman disease following rituxi-mab-based therapy in HIV-positive patients. Blood 2017, 129, 2143–2147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madan, R.; Chen, J.H.; Trotman-Dickenson, B.; Jacobson, F.; Hunsaker, A. The spectrum of Castleman’s disease: Mimics, radiologic path-ologic correlation and role of imaging in patient management. Eur. J. Radiol. 2012, 81, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Koa, B.; Borja, A.J.; Aly, M.; Padmanabhan, S.; Tran, J.; Zhang, V.; Rojulpote, C.; Pierson, S.K.; Tamakloe, M.-A.; Khor, J.S.; et al. Emerging role of 18F-FDG PET/CT in Castleman disease: A review. Insights Imaging 2021, 12, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Barker, R.; Kazmi, F.; Stebbing, J.; Ngan, S.; Chinn, R.; Nelson, M.; O’Doherty, M.; Bower, M. FDG-PET/CT imaging in the management of HIV-associated multicentric Castleman’s disease. Eur. J. Nucl. Med. Mol. Imaging 2008, 36, 648–652. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.S.; Paeng, J.C.; Park, C.M.; Chang, W.; Lee, W.W.; Kang, K.W.; Chung, J.-K.; Lee, D.S. Metabolic Characteristics of Castleman Disease on 18F-FDG PET in Relation to Clinical Implication. Clin. Nucl. Med. 2013, 38, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Hou, G.; Zhu, Z.; Huo, L.; Li, F.; Cheng, W. The value of multiparameter 18F FDG PET/CT imaging in differentiating retro-peritoneal paragangliomas from unicentric Castleman disease. Sci. Rep. 2020, 10, 12887. [Google Scholar] [CrossRef] [PubMed]
- Han, E.J.; Jung, S.E.; Park, G.; Choi, B.O.; Jeon, Y.W.; Min, G.J.; Cho, S.G. FDG PET/CT Findings of Castleman Disease Assessed by Histologic Subtypes and Compared with Laboratory Findings. Diagnostics 2020, 10, 998. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, staging, and response as-sessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef] [PubMed]
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; Müeller, S.P.; Schwartz, L.H.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014, 32, 3048–3058. [Google Scholar] [CrossRef] [PubMed]
- El-Osta, H.E.; Kurzrock, R. Castleman’s Disease: From Basic Mechanisms to Molecular Therapeutics. Oncologist 2011, 16, 497–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaidyanathan, S.; Patel, C.; Scarsbrook, A.; Chowdhury, F. FDG PET/CT in infection and inflammation—Current and emerging clinical applications. Clin. Radiol. 2015, 70, 787–800. [Google Scholar] [CrossRef] [PubMed]
- Polizzotto, M.N.; Millo, C.; Uldrick, T.S.; Aleman, K.; Whatley, M.; Wyvill, K.M.; O’Mahony, D.; Marshall, V.; Whitby, D.; Maass-Moreno, R.; et al. 8F-fluorodeoxyglucose Positron Emission Tomography in Kaposi Sarcoma Herpesvirus–Associated Multicentric Castleman Disease: Correlation With Activity, Severity, Inflammatory and Virologic Parameters. J. Infect. Dis. 2015, 212, 1250–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| N° (%) | |
|---|---|
| Age average (range) | 51 (14–79) |
| Gender male | 10 (67%) |
| female | 5 (33%) |
| Size lymph node cm average (range) | 2.8 (1.1–5.5) |
| HIV positive | 4 (27%) |
| Fever | 7 (47%) |
| Histologic subtype: Hyaline vascular | 7 (47%) |
| Plasma cell | 5 (33%) |
| Mixed | 3 (20%) |
| Hemoglobin low * (NR 130–180 man; 115–160 woman) (g/L) | 4 (27%) |
| Hemoglobin g/L average (range) | 119 (95–140) |
| Platelet low * 109/L (NR 150–450) | 4 (27%) |
| Platelet 109/L average (range) | 140 (100–320) |
| Albumin low * (g/L) (NR 4–5.4) | 5 (33%) |
| Albumin g/L average (range) | 4.5 (3.5–5.4) |
| Leucocyte count low * (NR 4–11) 109/L | 5 (33%) |
| Leucocyte 109/L average (range) | 4 (2.9–8) |
| CRP > 0.4 mg/L | 11 (73%) |
| Average (range) | 5.7 (0.2–99) |
| LDH > 115 IU/L | 6 (40%) |
| LDH IU/L average (range) | 113 (102–250) |
| N° PET/CT | 52 |
| PET/CT positive | 15 (100%) |
| SUVmax average (range) | 8.75 (4–14) |
| Lesion-to-liver SUVmax ratio average (range) | 3.9 (1.8–6.7) |
| Lesion-to-blood pool SUVmax ratio average (range) | 4.7 (3.6–7.7) |
| aSUVmax | p Value | aL-L S Ratio | p Value | aL-B S Ratio | p Value | |
|---|---|---|---|---|---|---|
| Age | 0.222 | 0.356 | 0.310 | |||
| Gender | 0.884 | 0.501 | 0.941 | |||
| Male | 8.25 | 3.49 | 4.68 | |||
| Female | 8.90 | 4.27 | 4.78 | |||
| Size | 0.250 | 0.299 | 0.350 | |||
| Fever | 0.011 (0.024) * | 0.028 (0.045) * | 0.041 (0.049) * | |||
| Histologic subtype: | 0.758 | 0.898 | 0.789 | |||
| Hyaline Vascular | 8.45 | 3.8 | 4.6 | |||
| Plasma cell | 9.1 | 4 | 4.9 | |||
| Mixed | 7.9 | 3.6 | 3.8 | |||
| Hemoglobin low (NR 130–180 man; 115–160 woman) (g/L) | 0.333 | 0.252 | 0.352 | |||
| Platelet low 109/l (NR 150–450) | 0.210 | 0.222 | 0.422 | |||
| Albumin low (g/L) (NR 4–5.4) | 0.158 | 0.365 | 0.369 | |||
| Leucocyte count low (NR 4–11) 109/L | 0.625 | 0.700 | 0.600 | |||
| CRP > 0.4 mg/L | 0.001 (0.003) * | 0.007 (0.012) | 0.015 (0.041) * | |||
| LDH > 115 IU/L | 0.258 | 0.301 | 0.500 | |||
| HIV | 0.308 | 0.464 | 0.441 | |||
| positive | 6.25 | 3.12 | 3.67 | |||
| negative | 9.37 | 4.17 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albano, D.; Bertagna, F.; Cerudelli, E.; Dondi, F.; Giubbini, R. Role of 18F-FDG PET/CT in the Management of Patients Affected by HHV-8-Associated Multicentric Castleman’s Disease. Hemato 2021, 2, 383-391. https://doi.org/10.3390/hemato2020024
Albano D, Bertagna F, Cerudelli E, Dondi F, Giubbini R. Role of 18F-FDG PET/CT in the Management of Patients Affected by HHV-8-Associated Multicentric Castleman’s Disease. Hemato. 2021; 2(2):383-391. https://doi.org/10.3390/hemato2020024
Chicago/Turabian StyleAlbano, Domenico, Francesco Bertagna, Elisabetta Cerudelli, Francesco Dondi, and Raffaele Giubbini. 2021. "Role of 18F-FDG PET/CT in the Management of Patients Affected by HHV-8-Associated Multicentric Castleman’s Disease" Hemato 2, no. 2: 383-391. https://doi.org/10.3390/hemato2020024