
A Dual Mind Approach to Understanding the Conscious Self and Its Treatment


Developmental Biopsychiatry Research Program, Department of Psychiatry, McLean Hospital, Harvard Medical School, Belmont, MA 02478, USA
NeuroSci 2021, 2(2), 224-234; https://doi.org/10.3390/neurosci2020016
Submission received: 24 May 2021
/
Revised: 6 June 2021
/
Accepted: 8 June 2021
/
Published: 9 June 2021
(This article belongs to the Collection Neuroanatomy of Consciousness and the Will)
{kind=link}
Abstract
:In this paper I will address questions about will, agency, choice, consciousness, relevant brain regions, impacts of disorders, and their therapeutics, and I will do this by referring to my theory, Dual-brain Psychology, which posits that within most of us there exist two mental agencies with different experiences, wills, choices, and behaviors. Each of these agencies is associated as a trait with one brain hemisphere (either left or right) and its composite regions. One of these agencies is more adversely affected by past traumas, and is more immature and more symptomatic, while the other is more mature and healthier. The theory has extensive experimental support through 17 peer-reviewed publications with clinical and non-clinical research. I will discuss how this theory relates to the questions about the nature of agency and I will also discuss my published theory on the physical nature of subjective experience and its relation to the brain, and how that theory interacts with Dual-Brain Psychology, leading to further insights into our human nature and its betterment.
1. Introduction
Dual-brain Psychology comes out of my early clinical experiences in which I observed that my patients seemed to have two, and only two, personalities [1]. One was quite symptomatic, and affected by past traumas [2]. As the person progressed, there often was a shift to a more mature, healthier personality. A regression led to the immature personality. Later I reread the split-brain studies and had the hypothesis that these two personalities I was observing related to the two cerebral hemispheres [3,4]. The studies by Sperry and his associates showed that, after callosotomy, patients had two minds [5,6]. For example, by showing a photograph to the left lateral visual field the image would be seen only by the right hemisphere due to the neural connections between the medial retina, which received the image, and the contralateral hemisphere. All but one of these patients had speech in the left brain and each reported that they could not see the image and were not able to pick the item from a group of items with their right hand, controlled by the left brain. The right hemisphere is mute, but with the left hand can easily pick out the item shown as instructed. This demonstrates that the mute right hemisphere understands the English language and is able to perform the task. Due to the corpus callosum in ordinary people, the image is transferred to the opposite hemisphere and either hemisphere can perform the task.
Werner Wittling and his associates reported that by tracking eye movements and masking a computer screen, they were able to show an upsetting movie to one hemisphere or the other in intact people [7,8]. The participants’ responses were different depending on which side the movie was shown, and in patients from a clinic, the side which was more troubled by the film was not the right hemisphere, as expected from the common wisdom, but could be either left or right in a given person [9]. I realized that I might be able to accomplish the same effect by simply blocking a person’s vision so that he could see out only one of the lateral visual fields. I did not notice a difference, but that day when I went to my private practice, I asked a Vietnam veteran who had reenlisted three times for frontline combat and suffered severe PTSD for which he was being treated. When I asked him to look out of his left lateral visual field, he appeared quite stressed and said, “That plant behind you looks like the jungle!” I asked him to look out the other side, and he said, “No, that’s a nice-looking plant.” In my experience over 26 years, I have found that over 80% of my patients have a noticeable difference between sides such as one side has an anxiety level of at least 2 of 10 points higher than the other side. Often there is a 5-point difference. My experiences with my patients were described in my book, Of Two Minds [4]. This idea that people can have two very different experiences depending on which lateral visual field they look out of has been difficult for the academy to find credible as it is so far from our unaided experience. However, I found that my patients not only had more anxiety on one side, but also, I often looked critical (like the patient’s critical mother) on one side and supportive on the other. Photographs of other people also looked critical on the same side as I did. On that side, the patient’s attitude about himself also was more negative and he would be prone to develop cravings for drugs or gambling if these were a problem for him. To make this everyday observation clearer, the I will present part of a published transcript [3] of a former patient who had a severe drug problem that was well treated. I asked the patient to return to my office to try the lateral visual field test (LVFT), which had not yet been discovered when the patient was in treatment.
“Can you describe the difference between how you feel on this side versus the other side?” I asked.“I’m more relaxed on this side. The other side I was a little more uptight.”“Let’s put the other pair back on. How do you feel?”“Same as before. Not as comfortable as the other side. Not a good sign here. I’m just thinking about things I did in the past and everything about me then. I don’t really think about anybody but myself and the abuse, some of the things I’ve been through in life. This is not what I want to remember. Not good. Can I take them off now?”“Now I just want to ask you one more question. Can you relate these uncomfortable feelings to your father?”“I don’t know. I was never comfortable around my father. With these glasses on it’s sort of like dealing with him again because it’s always the unknown, and it’s always a pressure and a problem. Yeah, you feel the unknown, you have the tension…”“Let’s put the other glasses on [right brain].”“More relaxed. More focused. Clearer.”“Now if you think of your father on this side.”“I can deal with him on this side. I know how to handle him now, and I don’t think he’d get me upset, and I wouldn’t do the counterproductive things if I looked at him out of this side all the time. I’d feel more pity for him and for the relationship, and I don’t think I’d want to abuse myself by using drugs.”“What would someone have to do to you to get you to use drugs, feeling the way you do on this side?”“I don’t think it’s an option on this side.”“Would they have to have a gun on something?”“Oh, yeah, they’d have to do some extreme things.”“On the other side?”“Yeah, I could see myself doin’ it on the other side.”
What I found was that most of my patients, like the one in the transcript, clearly had two very different agencies or minds with very different experiences, which led to very different choices and wills and behaviors. The patient described is typical of approximately 50% percent of patients in having such a robust response; another 30% have a clinically useful but not as robust a response, and approximately 10 to 20% have no response. Clearly, the patients with a robust response, like the patient presented, have two agencies.
The patient in the transcript was still suffering (on one side) his trauma from his difficult relationship with a father, who was experienced as severely critical. If the patient’s more childlike mind dominated, then he would return to his choice of using large amounts of cocaine, which is a choice, based on his experience of intolerable pain of disrespect and devaluation, as well as his childlike agency’s attempts to deal with his distress. His immature mind reasons, ‘if I can’t have Father’s approval, I will act in a way that will get his disapproval and I will have control over his insults by provoking them’. The cocaine high offered some relief from his pain, but the withdrawal pain also motivated his use by attempting to control his pain and humiliation by inducing them [10]. These behaviors have rolling consequences as they lead to depression, disfunction, and criminality, all intensifying his sense of defectiveness.
This patient and I worked weekly on this for 3 years, and he was able to discover his mature mind. He stopped using cocaine early on, his mature mind came to dominate, and he never used cocaine again in the time that I knew him and in the 2 years since his termination when he came in for the lateral vision test. As is clear in the transcript, his mature side has an entirely different experience from his immature side: “I can deal with him on this side. I know how to handle him now, and I don’t think he’d get me upset, and I wouldn’t do the counterproductive things if I looked at him out of this side all the time. I’d feel more pity for him and for the relationship, and I don’t think I’d want to abuse myself by using drugs.” Looking out the right visual field (left brain activation) he says, “Yeah, I could see myself doin’ it on the other side.”
Before we discuss the relation of these clinical observations to Dr. Sonne’s questions, we must first establish further that these observations are reproduceable and supported by controlled experiments, as these observations are ignored by most philosophers, with a few exceptions [11,12], and by most clinicians and academic psychologists with some exceptions [13].
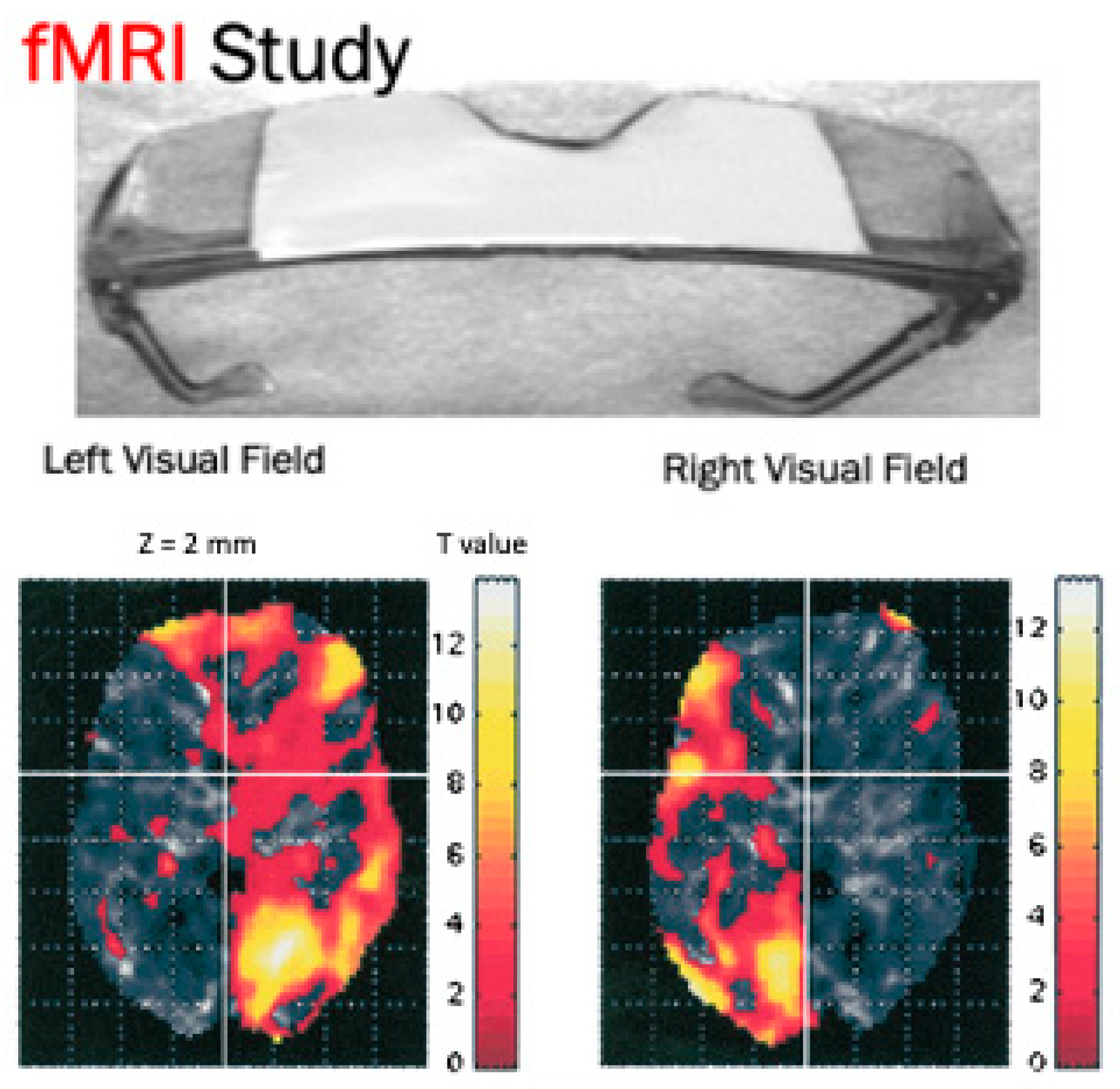
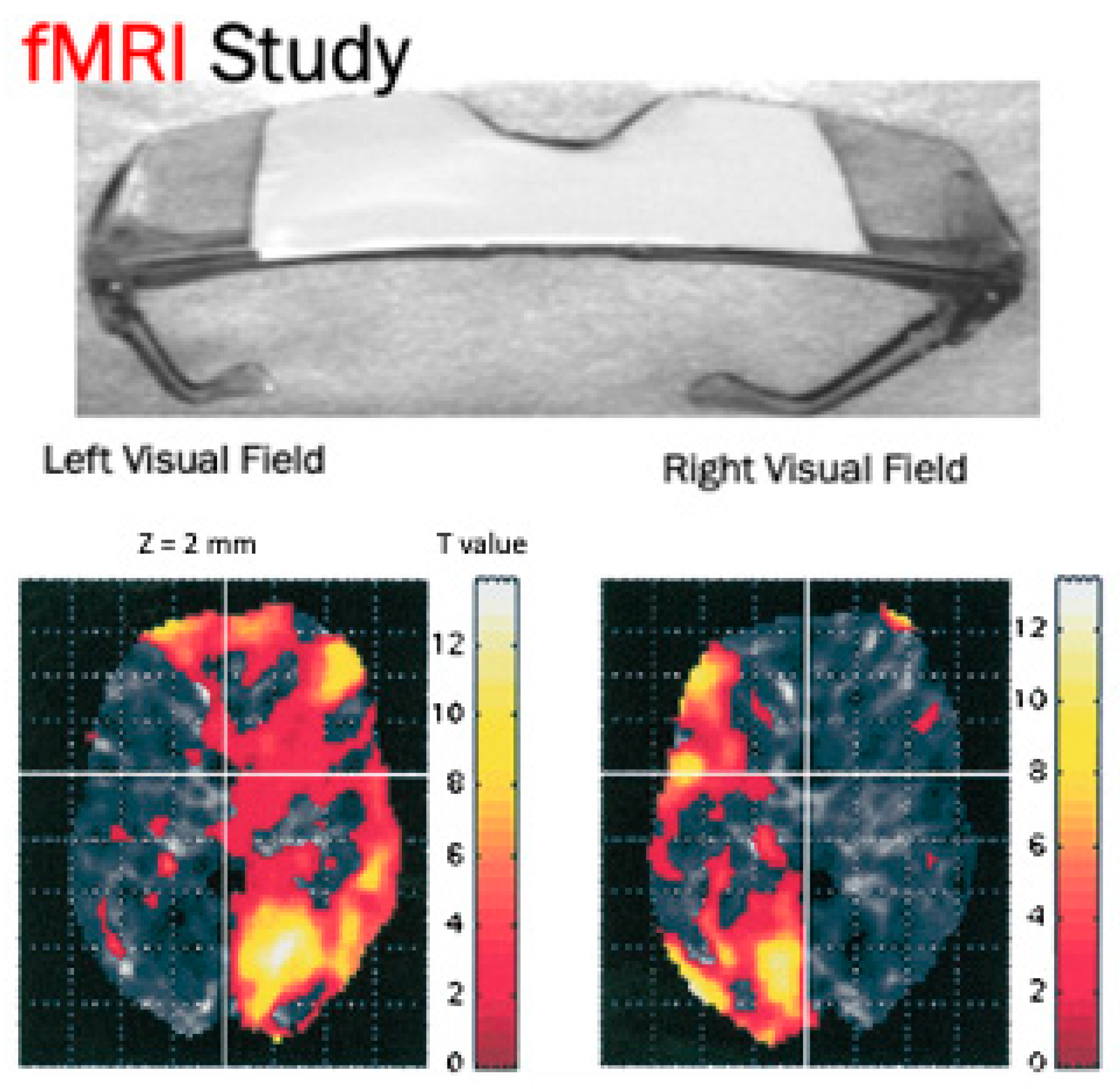
From McLean Hospital and the Harvard Medical School, my colleagues and I performed several studies to attempt to confirm that patients have different experiences out of the different lateral visual fields, and that these different experiences have to do with the activations of one cerebral hemisphere or the other. First came the clinical observations [14] such as I describe with the two patients I have mentioned. Next came studies with lateralized taped safety goggles, and taped safety goggles which were not lateralized as a control. We measured the emotional responses and EEG and ear temperature changes and reported that the lateralized goggles, but not the control goggles, induced significant lateralized emotional, EEG, and ear temperature changes [15]. We believe that the ear temperature changes were due to changes in hemispheric blood flow around the ear related to hemispheric activation. Later, we performed a brain imaging study [16], an fMRI study, which showed changes in hemispheric blood flow that occurred when the subjects looked out of one visual field and then the other for 30 s each, and then repeated that. The results are shown in Figure 1.
A second study was designed to test whether the observed or reported changes in a person’s experience with lateral vision were related to lateralized hemispheric stimulation. We did this by offering the taped lateralized goggles to 37 patients who were to undergo a 2 week course of rapid transcranial magnetic stimulation (rTMS) for depression [17]. Prior to the magnet treatment, which is a very widely used treatment for depression, each patient was asked to rate how depressed he felt out of each lateral visual field. Thirty-five of the 37 patients felt more depressed on one side than the other. rTMS is always applied clinically to stimulate the left side of the head at either 10 hz, or with 2 Hz on the right side, which is inhibitory. This is based on the imbalance theory, which associates depression always with the left hemisphere. My colleagues and I [18] wrote a very detailed critique of this theory and found it to be deficient. We believe that in approximately 50% of patients, the left hemisphere is more associated with depression. According to the Dual-Brain theory, we reasoned that if the rTMS was stimulating a healthier hemisphere, then the stimulation should be beneficial, but if the vision test indicated that they felt more depression when looking out the right visual field, suggesting that the left hemisphere was more depressed, then the patients would not be expected to do well. That is, we predicted that the 20 patients, who at baseline felt less depressed when looking out the right visual field than the left, would do well as the treatment was stimulating a less depressed cerebral hemisphere. We predicted that the 15 patients who felt more depressed when looking out the right visual field than the left would not do well as the treatment was stimulating a more depressed hemisphere. Two weeks after the 2 week course of rTMS, the group that we predicted to do well had a 42% decrease on their Hamilton Depression Rating Scores, while the group that we predicted to do poorly had an 11% decrease, and the difference was highly significant statistically and clinically. A few years ago, we replicated the study with a Canadian rTMS clinic and obtained almost identical results [19].
I made many attempts to convince rTMS clinics to stimulate according to the LVFT, but none would agree to do it. Therefore, I looked for a more portable method of stimulating a particular cerebral hemisphere, and after a successful pilot study [20], I tried unilateral transcranial photobiomodulation, near infrared mode, over the positive hemisphere in my private practice as an off-label intervention. I found that 81% had positive clinical responses, of which 62% had very remarkable responses to the treatment as illustrated in the following published transcript [21].
Before utPBM treatmentDr: So, looking at this angry man, tell me what you’re feeling.Pt: Feel scared.Dr: How scared, say from 0 to 10?Pt: I’d say 8 or 9.Dr: Now, I notice you seem to be shaking.Pt: Yeah, I know. It’s not because I’m trying to do it on purpose.Dr: I know, but that’s an example of how stressed you feel.Pt: Yeah, extremely stressed.Dr: Let’s try to treat you.After 4 Minute utPBM treatmentDr: You’re not shaking now.Pt: No.Dr: What your stress level?Pt: I would say 4, less than when I walked in the door. I would say less than half of what it was before the treatment, then it was a 10.
My results from my practice led me to initiate two double-blinded, randomized controlled trials (RCT), both of which showed highly significant positive results in participants who had a past or present history of opioid use disorder (OUD) and had, on entry, an opioid craving level of at least 4 of 10 on an opioid craving scale [22]. Both studies recruited the majority of participants from Craigslist.com (accessed on 15 February 2021). None were known to the researchers. The first study was a within-subject trial in which participants came for three sessions. The first was a treatment with either an active 4 min, near infrared LED at 250 mW/cm2 treatment, or a placebo device which was identical to the active but had foil over the LED so that the participants could feel warmth but receive no photons. The participants were tested with the LVFT as in the rTMS studies to determine which hemisphere had the more positive hemispheric emotional valence (HEV). They also used a computer test that was designed to measure their HEVs. All the treatments, active and placebo, were given on the forehead over the cerebral hemisphere with the more positive HEV. In the first study, approximately half the participants received the active treatment, at the first treatment, and the rest received the placebo. The second week they received the opposite treatment from that which they received at week one. The third weekly visit was a follow-up of the second week’s treatment. The results show that a week after the active treatment there was 51% decrease in OCS, but only a 16% decrease after the placebo treatments, and the differences were highly significant statistically with a high effect size of 0.73.
In the second study, which was funded by the National Institute on Drug Abuse and the HEAL Initiative, a group of 20 participants received the active treatment twice a week for 4 weeks with three follow-ups, while a further 19 received the placebo treatments. From baseline to the third follow-up, the active treatment group had a mean decrease in opioid cravings of 72% and the placebo group had a decrease of 30%; the differences were highly significant statistically with an effect size of 1.2. There were also highly significant decreases in opioid use and in anxiety levels in the active group compared to the placebo. This study is in submission for publication and its data file is presented in a supplementary file to the paper.
In my practice, as a part of the patient’s psychotherapy, the LED is placed over the negative hemisphere; this causes the same kind of negative qualitative change as the lateral vision, only larger. As with the LVFT, placing the LED over the negative hemisphere alters the patients experiences but does not cause any harm or adverse reactions, and the patient is always treated on the positive side as his last treatment. The positive hemispheric changes are also much greater with the LED than with the lateralized goggles. In the first RCT, we treated the negative hemisphere before the positive hemisphere, and there was a significant reduction in cravings when the positive hemisphere was stimulated compared to the negative when the participants were given the active treatment. There was no difference when the treatment to the two sides was with the placebo treatment. In both RCTs we had no side-effects at all, and in the extensive literature there have been no significant adverse reactions [23,24].
All of the preceding discussion is to assert that, in healthy controls and in patients and in study participants, people are usually of two minds or agencies, one associated with one brain hemisphere, and one with the other. The discussion that follows will address how the findings of Dual-brain Psychology relate to questions about agency, will, consciousness, brain regions, psychopathologies, and their treatments.
2. Discussion
If the Introduction robustly supports my assertion that we are of two minds, each associated with one brain hemisphere, then what meaning does this have for the investigation of consciousness? The most obvious implication is that a cerebral hemisphere is capable of generating a mind. We know that patients who underwent a hemispherectomy retain their human personality [25,26]. Wada studies, in which one hemisphere at a time is anesthetized prior to brain surgery to locate language sites, often show very different personalities when one hemisphere is anesthetized and the other awake [27,28]. As these minds are often very different in terms of experience, will, and behavior, we need to look at the hemisphere, and not the whole brain, when thinking about consciousness. Each hemisphere has component parts, but taken together, each is capable of a distinct self (each with the same birth date, address, and social security number). Radden [11] defines each of two minds within a person as each mind’s having a separate, distinguishable pattern of motivation and behavior. Each would have a different pattern of physical and emotional characteristics and moral dispositions. This is exactly what I have observed in my practice and research as I described above. To this, I add that each such “self” is related to one hemisphere, and I think that assertion is well supported as described above.
If we see that activating one hemisphere with lateral visual field stimulation, or with UtPBM, induces a dramatic change as described in the person’s experience, will, choice, and behavior, then how would this change in experience, will, choice, and behavior be explained? Each hemisphere resides in the same skull. The person goes through life seeing the same events, has the same blood trans versing its arteries and veins, the same parents, and yet each has its own agency.
I suggest that the best way to understand this is to consider that the two hemispheres have different neural connections, electrical fields, biophoton emissions, cellular metabolism, extracellular chemicals (hormones, synaptic chemicals, and growth factors), and different extra-neuronal components (glia, brain immune cells), epigenetic factors, genetic expression, and regulation. All of these components interact within each hemisphere, and no single factor leads to a self, but we can say that all of these constantly changing components are, together, brain information. That is, the brain produces information and each mind associated with each hemisphere is the momentary outcome of its brain information. What we see is that each hemisphere has different information.
Brain information acts on different levels. Much brain information never reaches the level of subjective experience, such as most cranial nerves and their ganglia. When we speak of agency, a necessary component is subjective experience. Obviously, conscious experience is a form of subjective experience and the concept of agency suggests that the agent has conscious experience, but we need to appreciate that subjective experience can also be beyond consciousness. Non-conscious experiences, long known as the unconscious in psychiatry, are experiences of which we are not conscious, but which can deeply affect us. An example would be the music score of a movie. We are often not consciously aware of the music, but it affects us. Another example would be a hypnotic suggestion [29]. In one experiment, a group of men were told under hypnosis that they were women and that they would not remember being given the suggestion [30]. When the men came out of the trance, they all argued that they were women. Of course, psychoanalysis made famous unconscious motivations that could be uncovered but were completely unappreciated by the analysand’s conscious mind. I am arguing that these unconscious motivations exist as experiences that can compel behaviors related to those experiences. The movie soundtrack is an experience that adds covertly to our experience of the movie. Of course, we are familiar with conscious experience, but as Freud and Jung and Janet pointed out [31], conscious experience sits upon non-conscious experiences.
When we are considering “will,” each agent in each hemisphere has non-conscious experiences as well as conscious motivations that affect choice. The dual-brain model suggests that each agent has different conscious and non-conscious motivations that affect its choices and behaviors. In all cases, the choice chosen will be that option, which in the view of the agent will best reduce toxic pain and enhance wellbeing. All living beings also have a tendency to choose options that enhance the prolongation of their lives, with the exception of human suicide, which can have complex motivations.
In the Dual-brain model, one hemisphere has a mind that consciously and non-consciously is more childlike and more affected by past maltreatments or traumas. Therefore, the choices of the agent in the more immature hemisphere will tend to make choices that may create more pain. The person may choose gambling, or aggressive, destructive behaviors, or substance abuse. Each of these choices might seem to an outside observer to indicate a will to induce pain, but from psychiatry we see that a more childlike mind with a history of trauma may make choices that lead to destructive behavior, such as heroin addiction which is destructive and painful and not life sustaining. However, a child’s mind thinks differently from an adult’s mind; it tends to over generalize, to urgently anticipate a return of the trauma even when its source has been removed. It tends to see few constructive options and often seeks solutions that are not intelligent. A more mature mind is able to bear and process past traumas, can envision a life without the past traumas, and can see many constructive options that can effectively enhance wellbeing and the sustenance of its life.
This shows that psychopathology comes out of the traumatized, immature mind. There are always compelling (childlike) reasons for the destructive choices and therefore the resultant psychopathology, but the reasons are the reasons of a traumatized (defined broadly as any harmful experience that the child encounters) childlike mind, which knows that the harm will be repeated and is unavoidable. When the immature hemisphere dominates, such a person will experience depression (feelings of being stuck in hopeless traumatic pain). Depression will induce choices that are different from a mind in a state of maturity and wellbeing. All affective states are motivational states, and all have a logic. For example, anxiety always results from an anticipated danger. An immature mind will anticipate danger differently from a mature mind; often, the anticipated danger is not consciously apparent, but relates to a very negative experience that has not been processed and persists in the immature hemisphere. The treatment, then, is to uncover the perspective of the immature mind and help it to realize that it is safer and more valuable than it believed. In Dual-brain Psychology, the healthy side is enlisted to aid the more troubled side. The relevant brain areas are the collective parts of the two hemispheres, which then compete for dominance or find a constructive way to cooperate.
However, this does not yet address the physical nature of subjective experience. I believe that the brain-processed information is, in itself, no more conscious than a bacterium or a plant. I assert that the complex brain information from each hemisphere does not possess subjective experience any more than the New York Times. I believe that brain information must interact with a fundamental quantum field that I have called the “subjective field” in order for its information to achieve experience, either non-consciously or consciously. I have discussed this in greater detail in an earlier paper [32], but to summarize, I suggest that possibly brain information gets translated into codes expressed ultimately in biophotons, which interact through quantum superpositions and reductions with the quantum subjective field, and that that interaction confers subjectivity upon the specific brain information that is related to the biophoton emissions. The resulting subjective experiences of the brain information impacts the brain. We know that experiences impact the brain. The same event, however, will impact the two hemispheres with their different sets of brain information and processing apparatuses and will each experience the event very differently and have different impacts. utPBM sends photons into the brain and induces significant changes to subjective experiences as described in the introduction. Do the irradiated photons from utPBM affect or amplify a biophoton code from the irradiated hemisphere, stimulating an enhancement of the dominance of that hemisphere and its associated subjective experiences and behaviors?
I have not yet addressed conscious subjective experiences and the self, which is always conscious. I believe that non-conscious experiences come out of an interaction between certain brain information and the subjective field. Conscious experiences are a step further than non-conscious experiences, and I feel that it must entail a similar but additional quantum field which I call the “quantum awareness field” [32]. The self (one in each hemisphere) is a complex area or construct of fields and neural connections, that emits biophoton codes [33] and is non-conscious until it interacts with the quantum awareness field to achieve consciousness. Cacha and Pozanaski [34] propose a theory of consciousness which also relies on an encoded biophoton field, non-conscious experience, and interacting fields, but the difference from my theory is that Cacha and Pozanski [35] rely on interacting energy states, “macro-quantum potential energy in a nested hierarchy.” I cannot conceive of any reasons that manipulations or interactions of known energy fields could cause consciousness. My speculation is different. It is that there exists a non-conscious subjective quantum field and a consciousness awareness quantum field, both as fundamental properties of the universe, like gravity, without known explanation. The speculation continues that certain brain information, likely ultimately in the form of biophtons representing brain information, interacts with the two subjective quantum fields to acquire subjectivity and awareness. That is, the speculation is that these, undiscovered quantum fields are fundamental and are the necessary missing ingredient to the creation of consciousness out certain brain information. A biophoton field carrying brain information is like the photon field that is emitted from a television movie. These photons go to the eyes and are decoded by the brain to create meaning in the brain, transcribed ultimately in biophoton fields of brain information, which interacts with the undiscovered quantum fields to return (all within the brain) as experience. The experience is always of the initial brain information.
The conscious experiences of the self affect the brain. All consciousness goes through the self (which is the agency) and each hemisphere has its own self. The experiences of the conscious self are the enlivenment of each self’s brain information. The selves can struggle for dominance or can cooperate. Usually, one self is more in control and present, but is always influenced by the other to a greater or lesser degree. A more mature self may dominate until the more childlike self is stimulated and empowered by some events, and the person can quickly shift from a mature personality to one that is immature and that, on a compelling impulse (first a non-conscious experience), may decide to gamble or use illicit substances, that the mature side knows from experience will not end well.
All things being equal, the more mature self is generally more moral, in so far as it is more likely to choose behaviors and dispositions that lead its and its group’s wellbeing. Therefore, morality has to do with one’s efforts to promote his mature mind’s dominance [36].
This brings up an interesting point from my theory on the conscious self [32]. There can be only one conscious self at a time. The self that is active is the dominant hemisphere. The other self recedes but, with stimulation, can become dominant and make the other self recede. The two sides can compete for dominance. That competition can be influenced by improved insight and understanding, capacity to bear, in short, the things that good psychotherapy achieves, and improves morality.
The paper focuses on consciousness and its relation to non-conscious experience, quantum field theory, and the brain. As such, Dual-Brain Psychology relates well with Freud’s emphasis on the importance of unconscious processes [37]. My work on subjective experience [32] deals extensively with non-conscious subjective experience, which has been neglected by mainstream neuroscience. A major disagreement with Freudian psychology is that I feel that much of what Freud [38] refers to as the id or the unconscious is, in my model, the conscious but immature, troubled mind associated with one hemisphere. Both hemispheres have non-conscious processing that underlies both conscious selves.
As an example, Goodman [39] describes the psychological and neurophysiological underpinnings of addiction in an insightful and comprehensive paper. The patients with any addiction are suffering motivation-reward, affect regulation, and behavioral inhibition deficiencies. In my experience in treating addiction, I would agree, but add that these deficiencies are conscious, but relate to unconscious defenses usually against early complex traumas that affect conscious mentation and behavior, but usually on only one side of the brain. As discussed, stimulating the more mature hemisphere with unilateral transcranial photobiomodulation within a few minutes usually led to a change in personality such that the person could deal more maturely with his traumas and find his cravings markedly diminished [21].
3. Conclusions
I have discussed questions about consciousness, agency, will, behavior, and ethics from the perspective of Dual-Brain Psychology, and believe that each brain hemisphere relates to a different agent, one that is more childlike and more affected by past traumas, and one that is more mature and healthier in spite of those traumas. The agents can compete for dominance and can often find, with treatment, ways of cooperating constructively. The paper also discusses the nature of subjective experience (conscious and non-conscious) and offers a novel understanding of psychopathology and its treatment.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
Not applicable.
Acknowledgments
The author acknowledges the advice and suggestions of William P. Seltzer.
Conflicts of Interest
The author is the Founder of MindLight, LLC, which intends further research and commercialization of the methods and device described in the introduction of the paper. The author has been issued two US patents which cover the method of unilateral tPBM to a positive hemisphere as described in this study: U.S. Patent No. 8303636, Methods for treating psychiatric disorders using light energy. Issued 11/06/2012, and U.S. Patent No. 8574279, Methods for treating psychiatric disorders using light energy. Issued 11/05/2013. He has filed, on 5 December 2019, a US patent application, #16/703,937, Method and Apparatus for Determining Hemispheric Emotional Valence, and on 3 August 2020, he filed a US provisional patent application #63060177, Enhanced Treatment of Brain Disorders Utilizing Coordinated Negative Suppressive Stimulation and Related Devices Designed to Achieve Treatment. The author has no other conflicts of interest.
References
- Schiffer, F. Cognitive Activity of the Right Hemisphere: Possible Contributions to Psychological Function. Harv. Rev. Psychiatry 1996, 4, 126–138. [Google Scholar] [CrossRef]
- Schiffer, F.; Teicher, M.H.; Papanicolaou, A.C. Evoked potential evidence for right brain activity during the recall of traumatic memories. J. Neuropsychiatry Clin. Neurosci. 1995, 7, 169–175. [Google Scholar] [CrossRef]
- Schiffer, F. Can the Different Cerebral Hemispheres Have Distinct Personalities? Evidence and Its Implications for Theory and Treatment of PTSD and Other Disorders. J. Trauma Dissociation 2000, 1, 83–104. [Google Scholar] [CrossRef]
- Schiffer, F. Of Two Minds: The Revolutionary Science of Dual-Brain Psychology; The Free Press: New York, NY, USA, 1998. [Google Scholar]
- Sperry, R.; Zaidel, E.; Zaidel, D. Self recognition and social awareness in the deconnected minor hemisphere. Neuropsychology 1979, 17, 153–166. [Google Scholar] [CrossRef] [Green Version]
- Schiffer, F.; Zaidel, E.; Bogen, J.; Chasan-Taber, S. Different psychological status in the two hemispheres of two split-brain patients. Neuropsychiatry Neuropsychol. Behav. Neurol. 1998, 11, 151–156. [Google Scholar]
- Wittling, W.; Roschmann, R. Emotion-Related Hemisphere Asymmetry: Subjective Emotional Responses to Laterally Presented Films. Cortex 1993, 29, 431–448. [Google Scholar] [CrossRef]
- Wittling, W.; Pflüger, M. Neuroendocrine hemisphere asymmetries: Salivary cortisol secretion during lateralized viewing of emotion-related and neutral films. Brain Cogn. 1990, 14, 243–265. [Google Scholar] [CrossRef]
- Wittling, W.; Schweiger, E. Neuroendocrine brain asymmetry and physical complaints. Neuropsychology 1993, 31, 591–608. [Google Scholar] [CrossRef]
- Schiffer, F. Psychotherapy of nine successfully treated cocaine abusers: Techniques and dynamics. J. Subst. Abus. Treat. 1988, 5, 131–137. [Google Scholar] [CrossRef]
- De Sousa, R.; Radden, J. Divided Minds and Successive Selves: Ethical Issues in Disorders of Identity and Personality. Philos. Phenomenol. Res. 2000, 60, 492. [Google Scholar] [CrossRef]
- Schechter, L. Self-Consciousness and ’Split’ Brains: The Minds’ I; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Schwartz, R. Internal Family Systems Therapy; Guliford: New York, NY, USA, 1995. [Google Scholar]
- Schiffer, F. Affect changes observed with right versus left lateral visual field stimulation in psychotherapy patients: Possible physiological, psychological, and therapeutic implications. Compr. Psychiatry 1997, 38, 289–295. [Google Scholar] [CrossRef]
- Schiffer, F.; Anderson, C.M.; Teicher, M.H. Electroencephalogram, bilateral ear temperature, and affect changes induced by lateral visual field stimulation. Compr. Psychiatry 1999, 40, 221–225. [Google Scholar] [CrossRef]
- Schiffer, F.; Mottaghy, F.M.; Vimal, R.L.P.; Renshaw, P.F.; Cowan, R.; Pascual-Leone, A.; Teicher, M.; Valente, E.; Rohan, M. Lateral visual field stimulation reveals extrastriate cortical activation in the contralateral hemisphere: An fMRI study. Psychiatry Res. Neuroimaging 2004, 131, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Schiffer, F.; Stinchfield, Z.; Pascual-Leone, A. Prediction of clinical response to transcranial magnetic stimulation for depression by baseline lateral visual-field stimulation. Neuropsychiatry Neuropsychol. Behav. Neurol. 2002, 15, 18–27. [Google Scholar] [PubMed]
- Schiffer, F.; Teicher, M.; Anderson, C.; Tomoda, A.; Polcari, A.; Navalta, C.; Andersen, S. Determination of hemispheric emotional valence in individual subjects: A new approach with reasearch and therapeutic implications. Behav. Brain Funct. 2007, 3, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiffer, F.; Glass, I.; Lord, J.; Teicher, M.H. Prediction of clinical outcomes from rTMS in depressed patients with lateral visual field stimulation: A replication. J. Neuropsychiatry Clin. Neurosci. 2008, 20, 194–200. [Google Scholar] [CrossRef]
- Schiffer, F.; Johnston, A.L.; Ravichandran, C.; Polcari, A.; Teicher, M.H.; Webb, R.H.; Hamblin, M.R. Psychological benefits 2 and 4 weeks after a single treatment with near infrared light to the forehead: A pilot study of 10 patients with major depression and anxiety. Behav. Brain Funct. 2009, 5, 46. [Google Scholar] [CrossRef] [Green Version]
- Schiffer, F. Unilateral Transcranial Near Infrared Treatments for Opiate Addiction in a Clinical Practice. Front. Psychiatry 2020, 11, 1–12. [Google Scholar]
- Schiffer, F.; Reichmann, W.; Flynn, E.; Hamblin, M.R.; McCormack, H. A Novel Treatment of Opioid Cravings with an Effect Size of.73 for Unilateral Transcranial Photobiomodulation Over Sham. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef]
- Hamblin, M.R. Shining light on the head: Photobiomodulation for brain disorders. BBA Clin. 2016, 6, 113–124. [Google Scholar] [CrossRef] [Green Version]
- Cassano, P.; Petrie, S.R.; Hamblin, M.R.; Henderson, T.A.; Iosifescu, D.V. Review of transcranial photobiomodulation for major depressive disorder: Targeting brain metabolism, inflammation, oxidative stress, and neurogenesis. Neurophotonics 2016, 3, 031404. [Google Scholar] [CrossRef] [Green Version]
- Nahum, A.S.; Liegeois, F.J. Language after childhood hemispherectomy: A systematic review. Neurology 2020, 95, 1043–1056. [Google Scholar] [CrossRef]
- McGovern, R.A.; Moosa, A.N.V.; Jehi, L.; Busch, R.; Ferguson, L.; Gupta, A.; Gonzalez-Martinez, J.; Wyllie, E.; Najm, I.; Bingaman, W.E. Hemispherectomy in adults and adolescents: Seizure and functional outcomes in 47 patients. Epilepsia 2019, 60, 2416–2427. [Google Scholar] [CrossRef]
- Ahern, G.L.; Herring, A.M.; Tackenberg, J.; Seeger, J.F.; Oommen, K.F.; Labiner, D.M.; Weinand, M.E. The Association of Multiple Personality and Temporolimbic Epilepsy: Intracarotid Amobarbital Test Observations. Arch. Neurol. 1993, 50, 1020–1025. [Google Scholar] [CrossRef]
- Stabell, K.E.; Andresen, S.; Bakke, S.J.; Bjornaes, H.; Borchgrevink, H.M.; Heminghyt, E.; Roste, G.K. Emotional responses during unilateral amobarbital anesthesia: Differential hemispheric contributions? Acta Neurol. Scand. 2004, 110, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.-R.; Pacherie, E. Alterations of agency in hypnosis: A new predictive coding model. Psychol. Rev. 2019, 126, 133–152. [Google Scholar] [CrossRef]
- McConkey, K.M.; Szeps, A.; Barnier, A.J. Indexing the experience of sex change in hypnosis and imagination. Int. J. Clin. Exp. Hypn. 2001, 49, 123–138. [Google Scholar] [CrossRef]
- Ellenberger, H.F. The Discovery of the Unconscious: The History and Evolution of Dynamic Psychiatry; Fontana: London, UK, 1994. [Google Scholar]
- Schiffer, F. The physical nature of subjective experience and its interaction with the brain. Med. Hypotheses 2019, 125, 57–69. [Google Scholar] [CrossRef]
- Salari, V.; Valian, H.; Bassereh, H.; Bókkon, I.; Barkhordari, A. Ultraweak photon emission in the brain. J. Integr. Neurosci. 2015, 14, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Cacha, L.A.; Poznanski, R.R. Genomic instantiation of consciousness in neurons through a biophoton field theory. J. Integr. Neurosci. 2014, 13, 253–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poznanski, R.R.; Cacha, L.A.; Latif, A.; Salleh, S.; Ali, J.; Yupapin, P.; Tuszynski, J.A.; Tengku, M. Theorizing how the brain encodes consciousness based on negentropic entanglement. J. Integr. Neurosci. 2019, 18, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiffer, F. Consciousness and Good and Evil. In Proceedings of the Science of Consciousness, Tuscion, AZ, USA, 14–18 September 2020; p. 251. [Google Scholar]
- Freud, S. Introductory Lectures on Psycho-Analysis; Hogarth Press: London, UK, 1916. [Google Scholar]
- Freud, S. The Ego and the Id: 1923–1925; Hogarth Press and the Institute of Psycho-analysis: London, UK, 1962. [Google Scholar]
- Goodman, A. Neurobiology of addiction. An integrative review. Biochem. Pharmacol. 2008, 75, 266–322. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
This image shows the mean fMRI results of 7 healthy subjects as they look out of each lateral visual field. Looking out of each visual field activated relatively the contralateral hemisphere [17].
Figure 1.
This image shows the mean fMRI results of 7 healthy subjects as they look out of each lateral visual field. Looking out of each visual field activated relatively the contralateral hemisphere [17].
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Schiffer, F. A Dual Mind Approach to Understanding the Conscious Self and Its Treatment. NeuroSci 2021, 2, 224-234. https://doi.org/10.3390/neurosci2020016
AMA Style
Schiffer F. A Dual Mind Approach to Understanding the Conscious Self and Its Treatment. NeuroSci. 2021; 2(2):224-234. https://doi.org/10.3390/neurosci2020016
Chicago/Turabian StyleSchiffer, Fredric. 2021. "A Dual Mind Approach to Understanding the Conscious Self and Its Treatment" NeuroSci 2, no. 2: 224-234. https://doi.org/10.3390/neurosci2020016