An Integrated Approach, Orthodontic and Prosthetic, in a Case of Maxillary Lateral Incisors Agenesis


Department of Biomedical, Dental Science and Morphological and Functional Images, Dental School, University of Messina, Messina 98100, Italy
*
Author to whom correspondence should be addressed.
Prosthesis 2019, 1(1), 3-10; https://doi.org/10.3390/prosthesis1010002
Submission received: 28 July 2019
/
Revised: 26 August 2019
/
Accepted: 2 September 2019
/
Published: 4 September 2019
(This article belongs to the Special Issue Innovative Prosthetic Device: New Materials, Technologies and Patients' Quality of Life (QoL) Improvement)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Background: Among tooth anomalies, missing teeth is one of the most frequent, and it can be related to different therapeutical sets of problems. Often, an integrated approach that interests both orthodontists and prosthodontists is necessary, and in some cases also the periodontists. Methods: In this paper the authors report a clinical case of a 14-year-old patient, affected by maxillary bilateral incisors agenesis, molar bilateral II class and deep bite, treated in the Department of Orthodontics and Pedodontics of the University of Messina. The orthodontic treatment target was the distal movement of the maxillary molar, and the recovery of the space necessary for the prosthetic restoration of the missing lateral incisor. Maxillary molars distal movement was performed with a Distal Jet apparatus, skeletally supported by two miniscrews (Distal-Screw, American Orthodontics, Sheboygan, WI, USA). After molar relationship correction, a multi-bracket bimaxillary orthodontic appliance was bonded using Empower Brackets (American Orthodontics, Sheboygan, WI, USA). At the end of orthodontic treatment a Maryland bridge, bonded on the central incisors and cuspids, was used in order to maintain the space necessary for the insertion of dental implants in the region of 1.2 and 2.2. Results: A class II molar relationship was corrected, with an improvement of the deep bite, and the space necessary for implant insertion was recovered Conclusion: A skeletally supported Distal Jet was efficient for molar distalization, with the advantage of not having any loss of anchorage in the anterior part of the dental arch. This apparatus does not need patient compliance, have favorable aesthetics and also give the possibility to perform asymmetric activations.
1. Introduction
Tooth agenesis is probably the most frequent tooth anomaly and is strongly related to genetic patterns [1]. Maxillary lateral incisors agenesis incidence seems to be rather elevated, with values of about 6% [2]. Such a clinical condition is related to different therapeutic problems, and it is often necessary to have an integrated approach that interest both orthodontists and prosthodontists, and in some cases also the periodontists [3,4]. Teeth agenesis affects first of all the third molar, and then mandibular second premolar and maxillary lateral incisor, and among tooth agenesis the maxillary lateral incisor one is the more relevant, because of its significant impact on dental aesthetics. In cases of maxillary lateral incisors agenesis, a dental anomaly must be corrected as soon as possible, with space recovery if is it possible, in order to prevent functional effects. Differential diagnosis between impacted or a missing tooth can be obtained with a low dose CT acquisition, that provides more detailed diagnostic information without a significant increase in radiological risk for patients. If it is possible, orthodontic treatment targets the recovery of the anterior space, often lost because of the mesial shift of latero-posterior teeth; in such cases the first step of orthodontic treatment is molar distal movement. Several clinical conditions must be evaluated in order to decide if it is necessary to open or close the space for missing lateral maxillary incisors. A patient’s facial aesthetics is one of the most important factors that must be considered, and if it is necessary to improve dental support to the upper lip, the recovery of the space is strongly recommended. In cases of a reduced vertical dimension, with dental deep-bite, the recovery of the space for missing lateral incisors, with molar distal movement, is recommended in order to produce a posterior rotation of the mandible and consequently an increase of the vertical dimension of the face and a correction of dental deep-bite. Maxillary molars distal movement can be obtained with both intra- and extraoral appliances. An intraoral apparatus offers the advantage of no patient compliance, however they could produce some side effects [5,6], especially in terms of anterior anchorage lost. A no compliance apparatus includes different types of devices, such as Distal jet, Pendulum, compressed coil springs, repelling magnets, etc. Intraoral devices can be skeletally supported in order to prevent loss of dental anchorage; this type of anchorage has been proposed for the first time by Creekmore in 1983 and Jenner in 1985, but nowadays several studies are available in the literature [7,8,9] about a skeletal-supported molar distalization apparatus. Dental anchorage represents the resistance to unwanted tooth movement, and can be classified in maximum, medium and minimum. Maximum anchorage corresponds to a complete absence of movement of the anchorage unit in consequence of reactive forces applied to other teeth [10]. Such anchorage can be obtained only if the anchorage apparatus is bone supported; an example is represented by miniplates, miniscrews, palatal implants and dental implants. There is no sufficient evidence in the literature about the efficiency and efficacy of different skeletal anchorage devices. For this reason, skeletal anchorage system selection is usually based on an individual preference of clinicians. In clinical practice miniscrews are the most commonly used because of their easily insertion and their elevated reported success rates, which is estimated around 80%–90% and similar to mini plate and palatal implant ones [11]. Different authors studied the ideal sites for miniscrew placement, and most of them proposed the palate as one of the better sites [12]. Palatal area offer both sufficient quality and quantity of bone for miniscrew insertion. However, the incisive canal region and the median area must be excluded, instead the para-median area present a cortical bone density and is thick enough to support the insertion of a miniscrew, and is able to bear orthopedic loads [13]. The para-median palatal area is devoid of sensible anatomical structures like blood vessels, nerves and dental root, which can create problems in miniscrew insertion. Moreover para-median palatal soft tissue thickness at the level of the third wrinkle is about 3.06 ± 0.45 mm2: This thickness offers sufficient stability for miniscrew insertion. Para-median miniscrew insertion in growing children, moreover, does not interfere with growth processes at the level of the midpalatal suture [14].
2. Materials and Methods
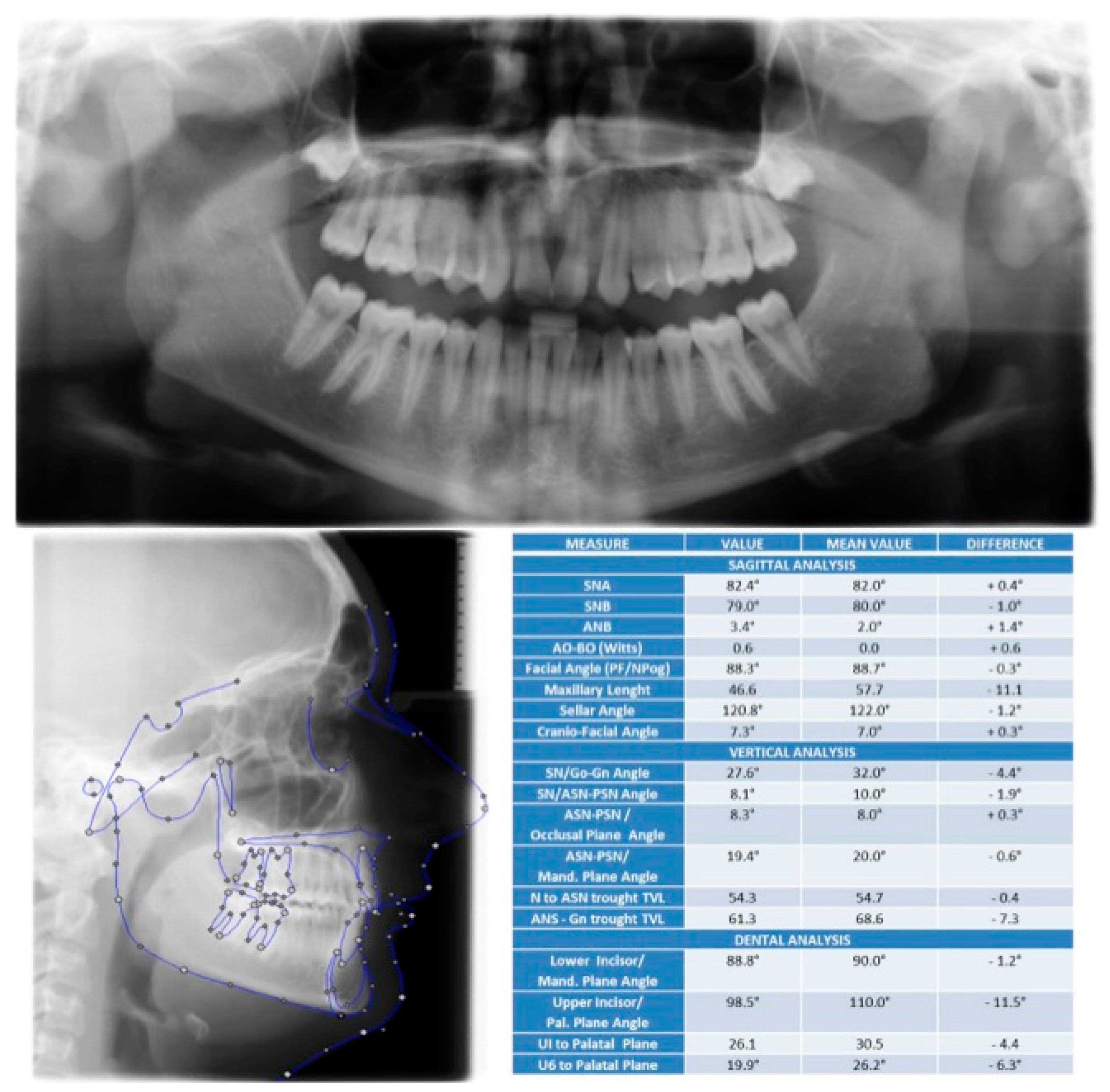
We present a clinical case of a 14-year-old patient, male, with agenesis of the maxillary lateral incisors, a bilateral II class molar relationship and deep-bite. The patient turned to the Department of Orthodontics of Messina University for a dental visit, and an orthodontic check-up was performed with photographic reports (Figure 1), Panoramic Rx and L-L head teleradiography (Figure 2), as well as a cephalometric examination and comprehending also a facial aesthetic evaluation.
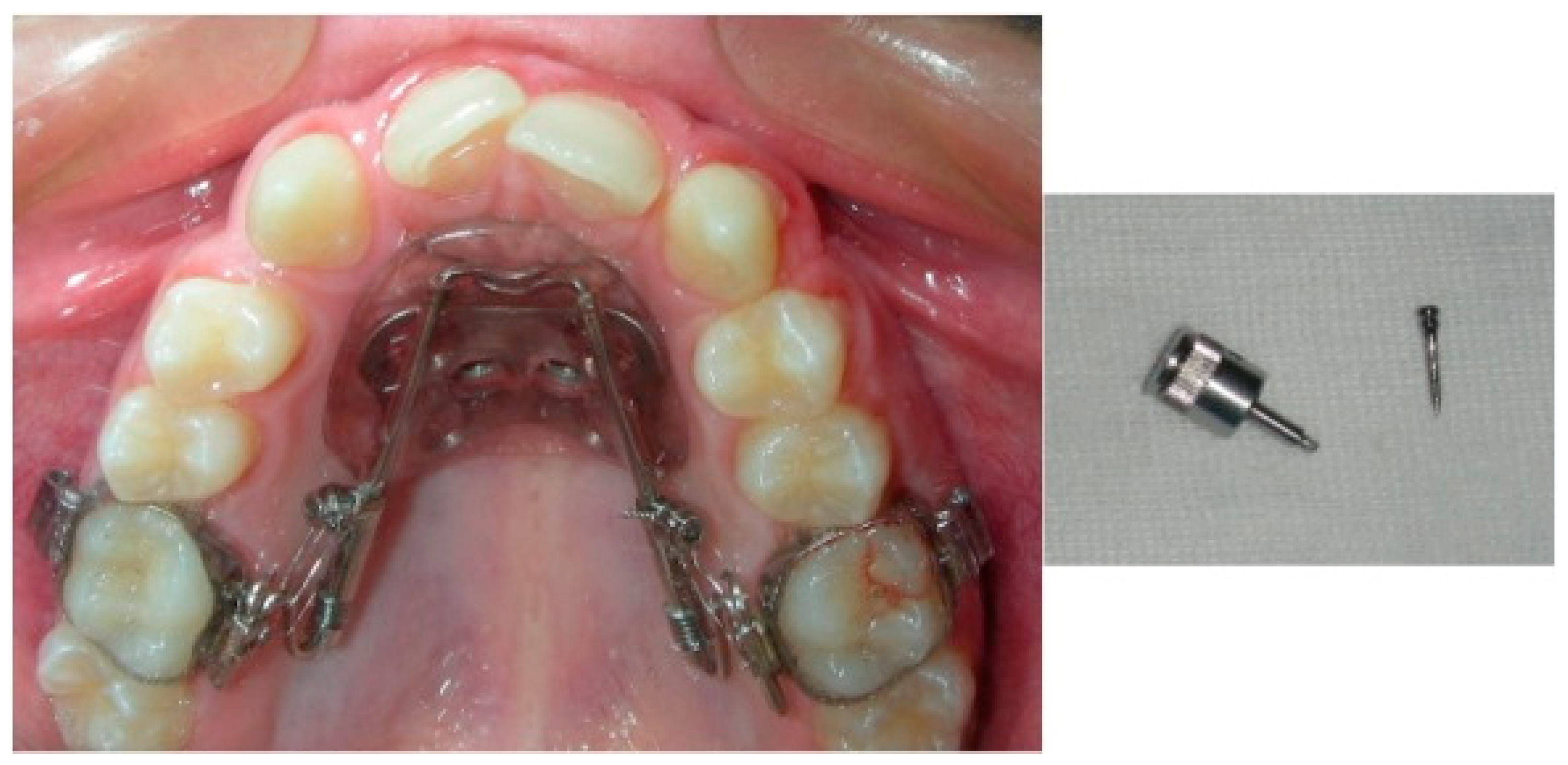
Impressions in alginate of both arches was done and dental casts were obtained in order to perform dental discrepancies analysis [15]. In order to correct dental deep-bite and improve the patient’s facial aesthetic, giving a better support to the upper lip, an orthodontic treatment plan predicted the recovery of the space necessary for the prosthetic restoration of lateral incisor agenesis. Maxillary molars distal movement as performed with a miniscrew skeletal-supported Distal Jet, called Distal-Screw (American Orthodontics, Sheboygan, WI, USA). The device presents two palatal coil springs whose compression generates forces with a distal vector over the first maxillary molars, and the effect of such forces produces distal movement of maxillary first molars. An accurate design of the apparatus and a favorable palatal anatomy, in this case produced a resultant line of forces close to the maxillary molar’s center of resistance. A traditional Distal Jet produces a reactive force with undesired side effects on the anterior teeth. The use of a bone-anchored device eliminates the problems related to the reactive forces discharged on the anterior teeth, because they are absorbed by the maxillary bone [16]. The Distal-Screw was placed using two screws with an 11 mm length, inserted in the para-median area of the palate, and the maximum activation of the coil spring was done in order to perform maxillary molar distal movement and overcome the resistance offered by second and third maxillary molars (Figure 3).
The miniscrew insertion procedure is really simple, as it does not need a gingival flap and can be performed with local anesthesia; in this case both the screws showed a good primary stability and was immediately loaded. The para-median palatal area is an ideal zone for TADS insertion, thanks to its easy access, the presence of keratinized soft tissues and a low risk of dental damage or vessels/nerve injury. Miniscrews must be inserted at the level of the third palatal wrinkle; several studies [17,18,19] report that this area can be considered as a safety zone for TADS insertion. Maxillary molar distal movement was completed in about seven months, reaching a bilateral molar I class relationship (Figure 4).
In order to lead the correction of maxillary molar distal tipping, with a greater distal movement of the crown compared to the root one, an overcorrection of the molar class relationship was done.
An orthodontic multi-bracket appliance was bonded and, in order to reduce the frictional forces between the slot and the arches and obtain a shorter treatment time [20,21], self-ligating mechanics were used (Empower, AO, Sheboygan, WI, USA) (Figure 5).
Once the initial phases of alignment and leveling were completed, an 0.017 inch × 0.025 inch Thermal Nickel–Titanium wire (American Orthodontics, Sheboygan, WI, USA) and two coil springs were positioned between the maxillary central incisors and cuspids, in order to produce canines’ distal movement and complete the recovery of the space necessary for the prosthetic restoration of the lateral incisors agenesis. Once the canine distal movement was completed, with the achievement of a bilateral canine I class relationship, a traditional archwire sequence was done, with rectangular stainless-steel wires for a full Tip and Torque expression, and B-Titanium wires for occlusal finishing. After the debonding of the multibrackets appliance, a metallic fixed retainer canine-to-canine was bonded in the lower arch, instead of in the maxillary arch, in order to maintain the space recovered for the following insertion of the dental implant, and a Maryland bridge was bonded at the level of the lateral incisors (Figure 6).
3. Results
Thanks to the combined use of a skeletal-supported molar distalization apparatus and a multibracket self-ligating orthodontic appliance, in eighteen months of treatment the following clinical results were achieved: A bi-maxillary dental crowding correction, bilateral molars and cuspids I class relationship, overjet and overbite correction, dental midlines coincidence, occlusal plane correction, and recovery of the space necessary for the prosthetic restoration of maxillary lateral incisors agenesis.
4. Discussion
In the reported clinical case we decided to open the space necessary for the prosthetic restoration of lateral incisors agenesis in order to satisfy parents’ request and above all for the correction of dental deep-bite and to improve the patient’s facial aesthetic, giving a better support to the upper lip. The distal movement of maxillary molars provided a distal rotation of the mandible, with an increase in the facial vertical dimension and a correction of dental deep-bite. The effect of the no-compliance molar distalization device is a combination of distal crown movement and following tipping correction. Several factors can influence treatment results: Age, molar relationship (cusp–cusp or full II class) and the eruption of a second maxillary molar. Different studies support the hypothesis that molar distalization with a no-compliance apparatus is more efficient in cases of unerupted second molars. However, first molar distal movement is achievable also in cases where second molars have erupted [22]. In such cases, third molar extraction can be suggested. In the therapy note proposed in this study, first molar distal movement was reached, despite the age of the patient and the eruption of the second molars. A systematic review performed in 2011 by Fudalej and Antoszewska [23] regarding the effectiveness of an orthodontic distalizer reinforced with a temporary skeletal anchorage, demonstrated that a skeletally supported device reduces the side effect characteristics of a dental supported apparatus. This review moreover demonstrated that skeletal anchorage, both with implants, screws or miniplates, also increase the molar distalization rate, where Maxillary molars distal movement was between 3.9 mm and 6.4 mm without any loss of anchorage in the anterior part of the maxillary arch. Antonarikis and Kiliaridis [6] found in their systematic review that tooth-supported devices could produce a maxillary molar distal movement of about 2.9 mm with an undesired maxillary incisor mesial tipping of 1.8 mm. The amount of maxillary molar distal movement can be lost both for the necessary correction of crown distal tipping and a root mesial one, and during the following retraction of the anterior teeth. Skeletally anchored devices, differently than tooth-borne ones, can be used as a reinforcement for maxillary molar anchorage during the phase of anterior teeth retraction. A non-integrated temporary anchored device has to be preferred with respect to the osseo-integrated ones; the first one present several clinical advantages, such as simple insertion, immediate loading, a lower cost and less discomfort to the patients. A skeletal-supported device also reduces the possibility of side effects on the TMJ [24,25] characteristic of other devices with extra-dental discharge of reactive forces such as TEO. The pain induced by miniscrew insertion can be easily controlled with a common anti-inflammatory drug [26]. The disadvantages in the use of TAD can be represented by the necessity of a more detailed radiological investigation of the patient [27] and the risk for dental root and periapical damages [28].
5. Conclusions
According to the clinical outcomes obtained in the study case, the following conclusions can be affirmed:
- A skeletally anchored Distal Jet is effective and efficient for maxillary molar distal movement, offering the advantage of no side effects in the anterior part of the arch.
- The miniscrew insertion and removal procedure is really simple, fast and painless for the patient. Moreover, soft tissues have not developed inflammation or bleeding.
- Molar distal movement was obtained in a few months with a final distal tipping and rotation of the crowns; no vertical changes were observed.
- A distal screw presents several clinical advantages such as no patient compliance, good aesthetics, predictable outcomes and the possibility of asymmetric effects.
- Thanks to a specific design, a distal screw also allows the spontaneous distal drift of premolars induced by o transept periodontal fibers stretching.
- A distal screw can also be used as an anchorage device during the following phase of treatment of anterior teeth retraction, in order to avoid side effects on the maxillary molars.
Author Contributions
Conceptualization, M.P. and R.N.; methodology, A.L.; validation, A.L; formal analysis, A.M.; investigation, A.M.; data curation, A.L.; writing—original draft preparation, M.P.; writing—review and editing, M.P.; visualization, M.P.; supervision, R.N.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest
References
- Militi, D.; Militi, A.; Cutrupi, M.C.; Portelli, M.; Rigoli, L.; Matarese, G.; Salpietro, D.C. Genetic basis of non syndromic hypodontia: A DNA investigation performed on three couples of monozygotic twins about PAX9 mutation. Eur. J. Paed Dent. 2011, 12, 21–24. [Google Scholar]
- Militi, A.; Vitale, C.; Portelli, M.; Matarese, G.; Cordasco, G. Open bite anteriore con agenesia dei secondi premolari inferiori: Terapia estrattiva con utilizzo di attacchi auto leganti. Mondo Ortod. 2012, 37, 1–15. [Google Scholar] [CrossRef]
- Worsaae, N.; Jensen, B.N.; Holm, B.; Holsko, J. Tretament of severe hypodontia-oligodontia an interdisciplinary concept. Int. J. Oral Maxillofac. Surg. 2007, 36, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Vitale, C.; Militi, A.; Portelli, M.; Cordasco, G.; Matarese, G. Maxillary Canine-First Premolar transposition in the permanent dentition. J. Clin. Orth. 2009, 8, 517–523. [Google Scholar]
- Chiu, P.P.; McNamara, J.A., Jr.; Franchi, L. A comparison of two intraoral molar distalization appliances: Distal jet versus pendulum. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 353–365. [Google Scholar] [CrossRef]
- Antonarakis, G.S.; Kiliaridis, S. Maxillary molar distalization with non compliance intramaxillary appliances in Class II malocclusion. A systematic review. Angle Orthod. 2008, 78, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Gelgor, I.E.; Buyukyilmaz, T.; Karaman, A.I.; Dolanmaz, D.; Kalayci, A. Intraosseus screw-supported upper molar distalization. Angle Orthod. 2004, 74, 838–850. [Google Scholar] [PubMed]
- Kinzinger, G.S.; Gulden, N.; Yildizhan, F.; Diedrich, P.R. Efficiency of a skeletonized distal jet appliance supported by miniscrew anchorage for non compliance maxillary molar distalization. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 578–586. [Google Scholar] [CrossRef]
- Papadopoulos, M.A.; Melkos, A.B.; Athanasiou, A.E. Non compliance maxillary molar distalization with the first class appliance: A randomized controlled trial. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 586–587. [Google Scholar] [CrossRef]
- Daskalogiannakis, J. Glossary of Orthodontic Terms Leipzig; Quintessence Publishing Co.: Batavila, IL, USA, 2000. [Google Scholar]
- Tsui, W.K.; Chua, H.D.P.; Cheung, L.K. Bone anchor systems for orthodontic application: A systematic review. Int. J. Oral Maxillofac. Surg. 2012, 41, 1427–1438. [Google Scholar] [CrossRef]
- Poggio, P.M.; Incorvati, C.; Velo, S.; Carano, A. Safe zones: A guide for miniscrew positioning in the maxillary and mandibular arch. Angle Orthod. 2006, 76, 191–197. [Google Scholar] [PubMed]
- Martina, R.; Cioffi, I.; Farella, M.; Leone, P.; Manzo, P.; Matarese, G.; Portelli, M.; Nucera, R.; Cordasco, G. Transverse changes determined by rapid and slow maxillary expansion—A low-dose CT-based randomized controlled trial. Orthod. Cranio Facial. Res. 2012, 15, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Schauseil, M.; Ludwig, B.; Zorkun, B.; Hellak, A.; Korbmacher-Steiner, H. Density of the midpalatal suture after RME treatment—A retrospective comparative low-dose CT-study. Head Face Med. 2014, 10, 18. [Google Scholar] [CrossRef] [PubMed]
- Portelli, M.; Matarese, G.; Militi, A.; Cordasco, G.; Lucchese, A. A proportional correlation index for space analysis in mixed dentition derived from an Italian population sample. Eur. J. Paed Dent. 2012, 13, 113–117. [Google Scholar]
- Kinzinger, G.S.M.; Diedrich, P.R.; Bowman, S.J. Upper molar distalization with a miniscrew-supported distal jet. J. Clin. Orthod. 2006, 40, 672–678. [Google Scholar] [PubMed]
- Seong, H.; Bayome, M.; Lee, J.; Lee, J.Y.; Song, H.H.; Kook, Y.A. Evaluation of palatal bone density in adults and adolescent for application of skeletal anchorage devices. Angle Orthod. 2012, 4, 625–631. [Google Scholar]
- Matarese, G.; Portelli, M.; Mazza, M.; Militi, A.; Nucera, R.; Gatto, E.; Cordasco, G. Evaluation of skin dose in a low dose spiral CT protocol. Eur. J. Paed Dent. 2006, 7, 77–80. [Google Scholar]
- Cordasco, G.; Portelli, M.; Militi, A.; Nucera, R.; Lo Giudice, A.; Gatto, E.; Lucchese, A. Low-dose protocol of the spiral CT in orthodontics: Comparative evaluation of entrance skin dose with traditional X-ray techniques. Prog. Orthod. 2013, 10, 14–24. [Google Scholar]
- Lucchese, A.; Bertacci, A.; Chersoni, S.; Portelli, M. Primary enamel permeability:a SEM evaluation in vivo. Eur. J. Ped Dent. 2012, 13, 231–235. [Google Scholar]
- Matarese, G.; Nucera, R.; Militi, A.; Mazza, M.; Portelli, M.; Festa, F.; Cordasco, G. Evaluation of frictional forces during dental alignment: An experimental model with 3 nonleveled brackets. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 708–715. [Google Scholar] [CrossRef]
- Kinzinger, G.S.; Fritz, U.B.; Sander, F.G.; Diedrich, P.R. Efficiency of a pendulum appliance for molar distalization related to second and thrird molar eruption stage. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 8–23. [Google Scholar] [CrossRef] [PubMed]
- Fudalej, P.; Antoszewska, J. Are orthodontic distalizers reinforced with temporary skeletal anchorage devices effective? Am. J. Orthod. Dentofac. Orthop. 2011, 139, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Portelli, M.; Matarese, G.; Militi, A.; Logiudice, G.; Nucera, R.; Lucchese, A. Temporomandibular joint involvement in a cohort of patients with juvenile idiopatic arthritis and evaluation of the effect induced by functional orthodontic appliance: Clinical and radiographic investigation. Eur. J. Paed Dent. 2014, 15, 63–66. [Google Scholar]
- Portelli, M.; Gatto, E.; Matarese, G.; Militi, A.; Catalfamo, L.; Gherlone, E.; Lucchese, A. Unilateral condylar hyperplasia: Diagnosis, clinical aspects and operative treatment. A case report. Eur. J. Paed Dent. 2015, 16, 99–102. [Google Scholar]
- Scolari, G.; Lazzarin, F.; Fornaseri, C.; Rengo, S.; Amato, M.; Cicciù, D.; Braione, D.; Morgantini, A.; Bassetti, C.; Tramér, M.; et al. A comparison of Nimesulide Beta Cyclodextrin and Nimesulide in postoperative dental pain. Int. J. Clin. Pract. 1999, 53, 345–348. [Google Scholar] [PubMed]
- Di Lorenzo, P.; Niola, M.; Pantaleo, G.; Buccelli, C.; Amato, M. On the comparison of age determination methods based on dental development radiographic studies in a sample of Italian population. Dental Cadmos 2015, 83, 38–45. [Google Scholar] [CrossRef]
- Paduano, S.; Uomo, R.; Amato, M.; Riccitiello, F.; Simeone, M.; Valletta, R. Cyst-like periapical lesion healing in an orthodontic patient: A case report with five-year follow-up. G. Ital. Endod. 2013, 27, 95–104. [Google Scholar] [CrossRef]
Figure 1.
Pre-treatment intraoral reports.

Figure 2.
Pre-treatment X-ray exams.

Figure 3.
Palatal view of the Distal-Screw.

Figure 4.
Molar relationship after Distal-Screw.

Figure 5.
Self-ligating orthodontic appliance.

Figure 6.
Post treatment.

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Portelli, M.; Militi, A.; Logiudice, A.; Nucera, R. An Integrated Approach, Orthodontic and Prosthetic, in a Case of Maxillary Lateral Incisors Agenesis. Prosthesis 2019, 1, 3-10. https://doi.org/10.3390/prosthesis1010002
AMA Style
Portelli M, Militi A, Logiudice A, Nucera R. An Integrated Approach, Orthodontic and Prosthetic, in a Case of Maxillary Lateral Incisors Agenesis. Prosthesis. 2019; 1(1):3-10. https://doi.org/10.3390/prosthesis1010002
Chicago/Turabian StylePortelli, Marco, Angela Militi, Antonino Logiudice, and Riccardo Nucera. 2019. "An Integrated Approach, Orthodontic and Prosthetic, in a Case of Maxillary Lateral Incisors Agenesis" Prosthesis 1, no. 1: 3-10. https://doi.org/10.3390/prosthesis1010002