Assessment of the Acute Effects of Carbonated Beverage Consumption on Symptoms and Objective Markers of Gastric Reflux


1
Newcastle Research and Innovation Institute, Human Nutrition Research Centre, Devan Nair Building, Singapore 600201, Singapore
2
CSIRO Nutrition & Health Program, SAHMRI Building, North Terrace, Adelaide, SA 5000, Australia
*
Author to whom correspondence should be addressed.
Gastrointest. Disord. 2019, 1(1), 30-38; https://doi.org/10.3390/gidisord1010004
Submission received: 6 August 2018
/
Revised: 4 September 2018
/
Accepted: 11 September 2018
/
Published: 12 September 2018
{kind=link}
{kind=link}
{kind=link}
Abstract
:Previous studies have suggested that carbonated beverages may cause gastro-oesophageal reflux. Pepsin (the major enzyme secreted by the stomach) has been suggested to be an objective, acute marker of a reflux event. This pilot study aimed to investigate whether intake of carbonated beverages could affect pepsin concentration in saliva or reflux symptoms. This was assessed by a randomised, crossover trial where participants consumed 330 mL of beverage (carbonated cola, degassed cola or water) at separate visits. Saliva samples and symptom questionnaires were collected at baseline and over the 30 min postprandial period. Pepsin was detected in all saliva samples. No difference was found in the salivary pepsin concentrations between treatments at all time points. There were significantly higher scores (p > 0.05) for feelings of fullness, heartburn, urge to belch and frequency of belches after ingestion of carbonated cola than degassed cola and water. The ingestion of carbonated beverages did not appear to increase postprandial pepsin concentration in saliva compared to other beverages but did evoke higher levels of reflux-related symptoms such as fullness, heartburn and belching. This suggests carbonated beverages may cause symptoms associated with reflux but do not drive detectable levels of gastric juice to reach the oral cavity.
1. Introduction
Gastro-oesophageal reflux occurs in the majority of the population at varying frequencies and is commonly linked to symptoms such as heartburn, regurgitation, belching and difficulties with swallowing (dysphagia) [1]. Gastro-oesophageal reflux is the retrograde movement of stomach contents (gastric juice, food contents or gas) up the oesophagus and potentially beyond. Reflux may cause damage to the mucosal lining of the oesophagus and result in negative symptoms like heartburn [2]. Reflux has also been suggested to be associated with a number of other disorders of the respiratory tract [3,4]. In part, this may be mediated by the inappropriate opening or relaxation of the lower oesophageal sphincter, resulting in gastric contents passing up the oesophagus [5,6]. Risk factors for gastro-oesophageal reflux include smoking, obesity, alcohol consumption [7], physical inactivity and dietary factors [8]. Previous studies also suggested that gastric distention by gas or liquid boluses could cause transient relaxation of the lower oesophageal sphincter which is likely to increase frequency of reflux episodes [9,10]. Although, reflux of liquid stomach contents is most likely to result in measurable reflux, previous hypothesis has also suggested that the retrograde movement of gas boluses could also coat the mucosal lining of the aerodigestive tract with small volumes of aerosolized gastric juice [10].
Previous cross-sectional studies have suggested that gastro-oesophageal reflux disease patients were twice as likely to consume carbonated beverages as compared to healthy individuals, suggesting that the ingestion of carbonated beverage was associated with progression to gastro-oesophageal reflux disease [11] and that the intake of carbonated beverages was associated with aggravation of reflux-related symptoms [12]. Some previous studies suggested that the consumption of carbonated beverages significantly reduced lower oesophageal sphincter pressure (associated with an increased number of reflux episodes) compared to non-carbonated drinks [13,14], while others reported that the number of postprandial reflux events was not influenced by varying degrees of carbonation in beverages [15]. A systematic review by Johnson et al. (2010) reported that the ingestion of carbonated beverages could possibly elicit acute reduction in intra-oesophageal pH and increased rate of transient, lower oesophageal sphincter relaxations but noted limited evidence of an association with reflux symptoms [16].
The commonly used diagnostic tests to diagnose gastro-oesophageal reflux (e.g., manometry, impedance and pH monitoring) tend to be highly invasive [17,18]. The concentration of pepsin in saliva ([pepsin]saliva) had previously suggested as a biomarker for gastro-oesophageal reflux [19,20]. Pepsins are major proteolytic enzymes present in the gastric juices produced by the gastric chief cells and hence can only occur in saliva as a result of gastric contents reaching the oral cavity [21]. It appears that gastro-oesophageal reflux disease patients have higher [pepsin]saliva than healthy individuals, possibly due to more frequent or larger volumes of refluxate reaching the oral cavity in the disease condition [22,23]. Pepsin therefore seems an ideal, acute biomarker of reflux events and the authors hypothesise that higher concentrations of pepsin will be found in saliva if the intake of carbonated beverages or other “refluxogenic” food items has caused the gastric contents to reach the oral cavity. A preliminary study in non-symptomatic individuals seems a first rational step to test this hypothesis.
This study therefore aims to investigate the potential for carbonated beverages to affect [pepsin]saliva and the symptoms associated with gastro-oesophageal reflux within healthy individuals.
2. Results
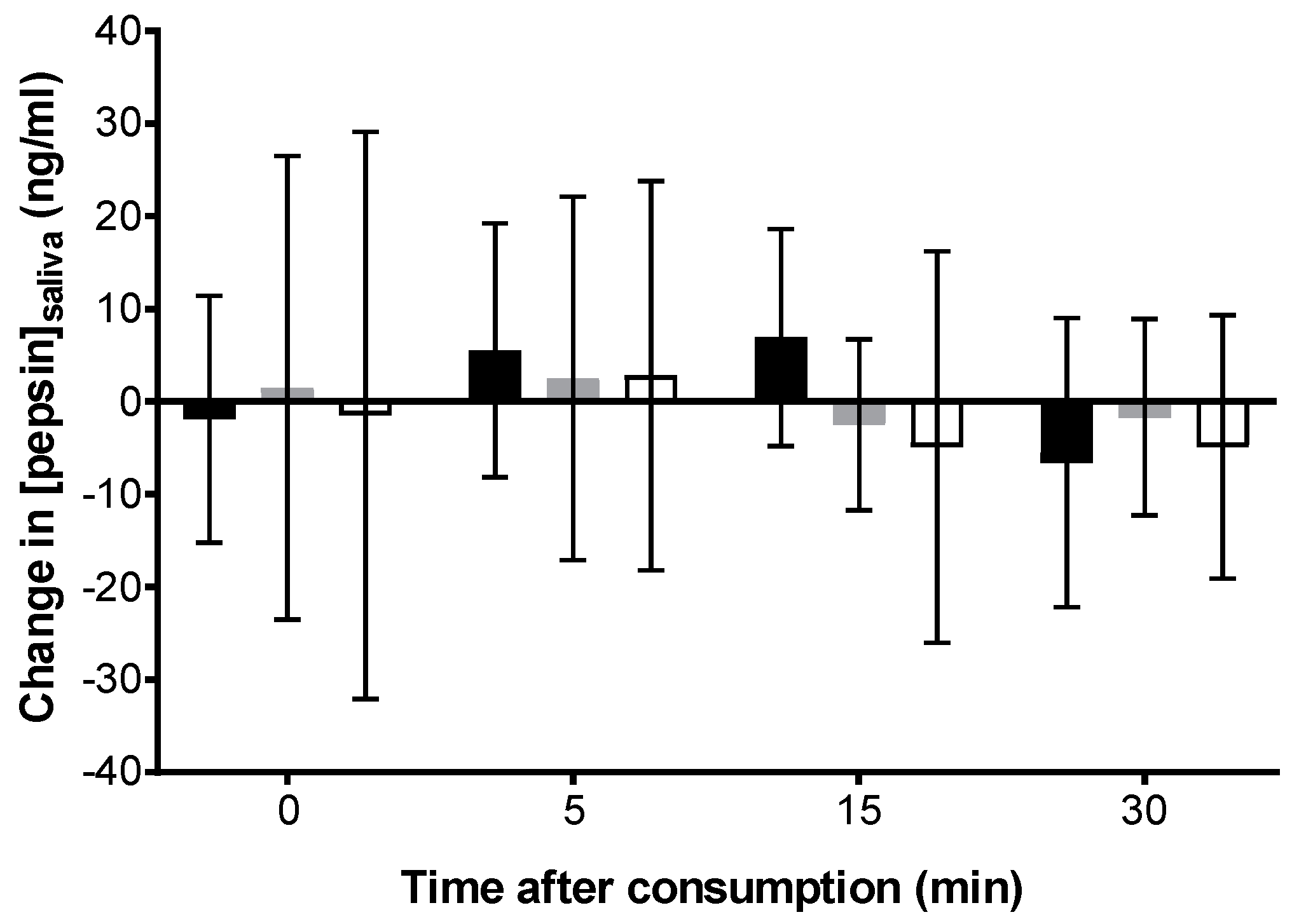
Ten healthy participants were recruited in this study (seven females and three males), between 21 and 38 years old. A total of 150 samples were collected (each participant provided five samples during each visit; total of three visits), and pepsin was detected in all the saliva samples; above the minimum detection limit of 1 ng/mL [24]. Data are presented below as the change in salivary pepsin concentrations from baseline (median ± interquartile range ng/mL) between pre- and post-ingestion (at time points; 0, 5, 15 and 30 min) of the three beverages (Figure 1). No statistically significant difference (p > 0.05) was found between the changes in salivary pepsin concentrations at all time points after ingestion of the three beverages. In addition, there were no significant differences in [pepsin]saliva concentration after ingestion of beverage over the 30 min monitoring period (see Figure 1).
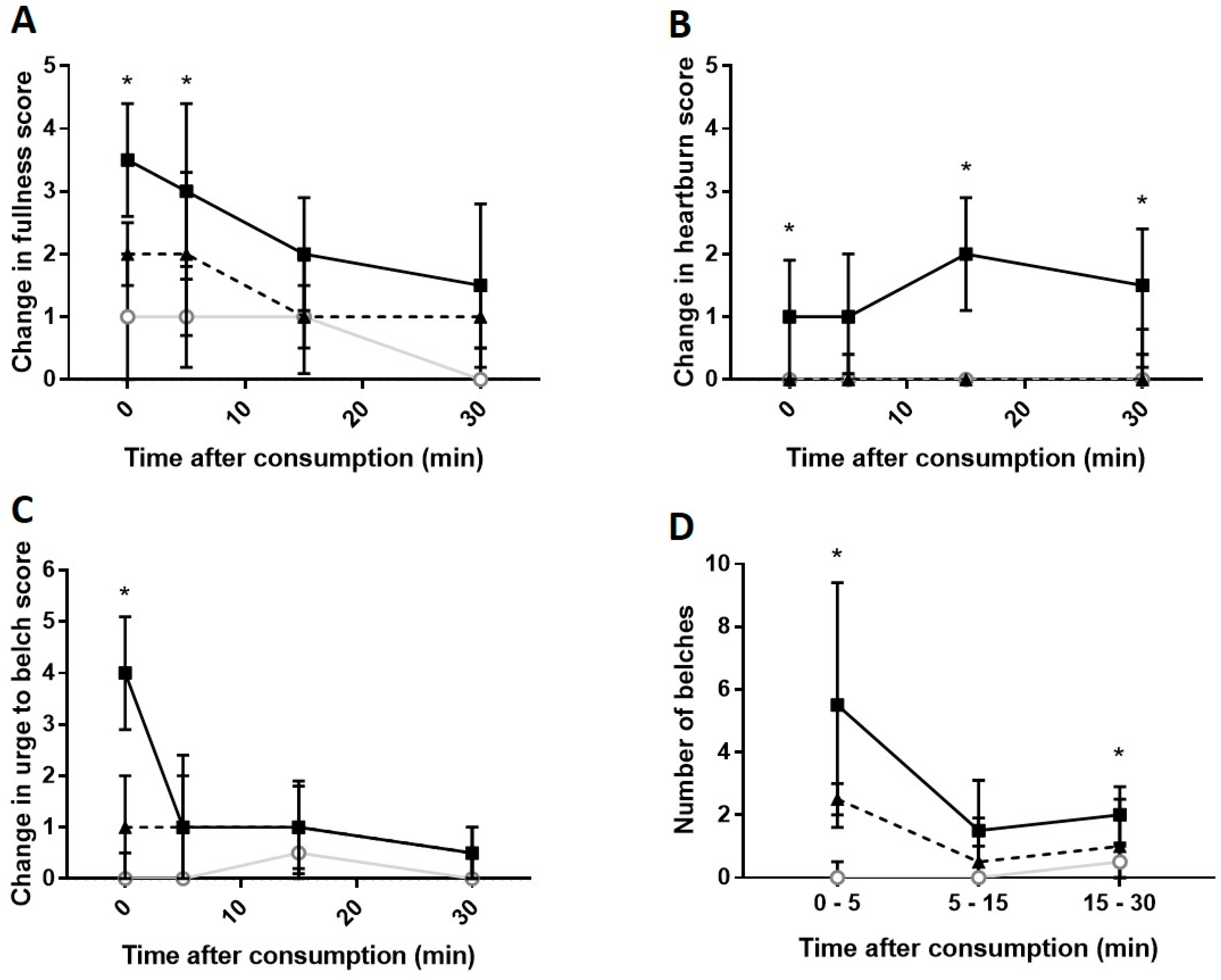
The responses of participants’ perception of reflux-associated symptoms (feeling of fullness, feeling of heartburn, urge to belch and frequency of belching) are presented in Figure 2A–D. There were no significant changes to all other symptoms (i.e., urge to cough, churning of stomach/borborygmi and breathing difficulties/choking episodes) measured within the questionnaire (data not presented).
The perceived feeling of fullness after ingestion of carbonated cola was the highest at all measured time-points but statistical differences were only observed between carbonated cola and water 0 (p = 0.005) and 5 (p = 0.03) min after ingestion (Figure 2A). No statistically significant differences were noted between median values for carbonated vs. degassed cola and degassed cola vs. water. The scores for changes in perceived feeling of heartburn after ingestion of beverage is shown in Figure 2B. Degassed cola and water did not elicit median changes in symptoms of heartburn at all post-ingestion time-points. Perceived heartburn symptoms of carbonated cola were significantly higher than water 0 (p = 0.032), 15 (p = 0.0007) and 30 min (p < 0.0001) after consumption and were also higher than degassed cola at two time-points (15 min: p = 0.0001 and 30 min: p = 0.027). Urge to belch (see Figure 2C) was only significantly higher than both water and degassed cola immediately after ingestion at 0 min compared to both water and degassed cola (p < 0.01).
The frequency of belches experienced between the various time intervals after ingestion of beverage was presented in Figure 2C,D. A large proportion (69%) of the total number of belches occurred within the first 5 min after consumption of carbonated cola (median of 5.5 with an interquartile range of 1.6–9.4 belches). The number of belches was significantly higher after ingestion of carbonated cola than water (but not degassed cola) at the time intervals between 0–5 min (p = 0.042) and 15–30 min (p = 0.045).
3. Discussion
The presence of pepsin noted in all samples collected within the current study was high compared to the low proportion of pepsin-positive saliva samples (12–21%) reported in previous studies [18,25]. While the antibody-based method for estimation of [pepsin]saliva used in this study has lower detection limits (1 ng/mL) compared to other available methods (36 ng/mL) [18,25], pepsin concentrations were considerably higher than either of these limits in the study samples [24,26]. It is possible that appreciable amounts of reflux may occur during the cephalic phase of digestion [27]. While the aim of asking participants to come in fasted for this study was to ensure standardisation of the protocol, it is possible that prolonged fasting could have exacerbated secretion rates of gastric juice and possibly increased the amount of pepsin being refluxed before and during the meal. Previous studies that used [pepsin]saliva as a marker of reflux collected saliva samples at least 1–2 h after meals [18,28]. While this approach is sensible to assess background reflux levels, the authors feel that the approach utilised here is most relevant to consider acute responses to a single meal, as this aligned with the aim of the current study. Nonetheless, collecting a baseline sample well in advance (>1 h) of the meal would be prudent and further consideration of the frequency of and time period across which postprandial saliva samples are collected may be needed in future studies on the refluxogenic potential of foods.
There was a non-significant increase in [pepsin]saliva between 5 and 15 min after ingestion of the carbonated cola (Figure 1). Previous work reported significant increased episodes of refluxes detected 1 h after ingestion of 300 mL of the administered beverages (with/without carbonation), as assessed by pH impedance [15]. It is important to note that the approach of Cuomo et al. (2008) [15] is more invasive but is able to measure mass reflux of liquid and gas. While the authors still believe that pepsin is a rational biomarker to test for reflux in the upper aerodigestive tract, further work to characterise when or how gastric reflux may occur around individual meals and for how long it takes for pepsin and other refluxate to be cleared from the oral cavity is still required [29]. One approach to better understand periprandial reflux could include saliva sampling over a longer time period and more frequently around a meal, with additional sampling at other times during the day. Direct instillation of purified pepsin or gastric juice into the oral cavity of individuals does not seem feasible or particularly acceptable but safer, quantifiable protein markers with similar molecular weights to pepsin could at least be used as adjuncts to test the time taken for clearance to occur. In relation to the current findings, as pepsin was detected in all baseline samples, it may be that high “background” levels of pepsin from previous reflux events, might be expected to mask more recent reflux events.
A high degree of intra-individual variability of the pepsin content of saliva appears likely from the current preliminary findings. The amount of pepsin reaching the oral cavity, governed by the volume of gastric refluxate and the pepsin concentration therein, alongside the subsequent clearance rates (driven by factors like frequency of swallowing and salivary flow rates) are likely to impact on the measured [pepsin]saliva. The average concentration of pepsin in gastric juice has previously been suggested to be approximately 0.5 mg/mL [30]. Reflux volumes could be virtually zero (e.g., aerosolised fluid brought up with a belch) or up to around 5.0 mL outside of mass regurgitation events [31]. There is approximately 0.8 mL of saliva/moisture in the oral cavity at any one time [32], which might dilute very low volume reflux events and therefore reduce [pepsin]saliva below a detectable limit.
The previous work of Johnston et al. (2009) has highlighted that pepsin may remain adhered to mucosal surfaces long after a reflux event [33]. This would at least highlight the potential for pepsin to be present in the oral cavity after a reflux event but may not be detectable in saliva as it is still bound to the oral mucosa. Recent studies in healthy individuals have suggested unstimulated saliva production rates of approximately 700–800 μL/min which may increase by 2–3-fold during stimulation [34,35,36]. Similarly, previous estimates of swallowing frequency vary dramatically, with average numbers of swallows equating to 600 over a 24-h period [32]. While these factors may affect baseline levels of pepsin in saliva, the consumption of the 330 mL beverage would also likely act to increase aboral pepsin clearance due to the rapid transit of a high volume of fluid. There was no obvious reduction in [pepsin]saliva from baseline to time-point zero with any of the test beverages, although it is possible that reflux could have occurred during intake, as the act of consuming the drink increased the amount of pepsin being returned to the stomach. It is also possible that a single intake of 330 mL of a beverage is not large enough to result in increases in intragastric pressure or other changes that could increase the number or volume of reflux events. One approach that could be considered in future studies would be to evaluate how different volumes of foods or beverages (from a single mouthful to a large serving) impact on parameters of reflux.
Heartburn is defined as a symptom commonly associated with gastro-oesophageal reflux, especially during postprandial period, whereby individual experiences discomfort or pain (burning sensation) around the chest and lower oesophagus area [37]. The mechanism of how ingestion of foods and beverages induces heartburn during postprandial stage is not clearly understood [38]. It has been postulated that heartburn occurs during increased frequency of acid reflux as a result from ingestion of foods [39], which agreed with our findings comparing carbonated cola to water and degassed cola (see Figure 2B). A previous study reported that the consumption of carbonated drinks with lower pH resulted in increased reported heartburn scores, but the pH of carbonated beverages was not affected by the degree of carbonation [40]. Bredenoord et al. (2005) reported that pure gas reflux events (belches) was associated with decreases in pH in the oesophagus which was classified as heartburn [41]. Another study also noted that almost three quarters of acid reflux in healthy participants was caused by belching, suggesting that gas reflux may result in feelings of heartburn [42], with a previous consensus report noting that reflux symptoms could also be caused by gas reflux [43]. Further studies on the impact of gas reflux, particularly in patient groups in whom this is a major symptom, appear to be warranted. This might include the sampling and chemical analysis of the composition of belches (e.g., for acid and pepsin content).
Finally, and perhaps most importantly, it must be acknowledged that the current study was carried out in non-symptomatic individuals. While this approach appears rational before potentially triggering painful symptoms in patient groups, it is possible that the same food stimulus might elicit different effects in these two groups. While clinical guidelines make note of some common dietary factors that might exacerbate reflux-associated disease [44], further work is also required to assess whether trigger foods and beverages are common or specific to individuals within this patient group. Further information like body weight, physical activity levels, habitual alcohol intake and other lifestyle factors that could have affected the outcomes of the current study were not collected. Future approaches in this area could consider additional demographic information from participants.
A great deal of further work is required in this area, but it is hoped that the methods used in this work could be applied to develop broad and personalised recommendations to benefit the management of reflux-associated symptoms through modification of diet, physical activity and posture. Due to the small sample size involved, the findings from this study are preliminary in nature but could help inform future study design to help ensure statistical power.
4. Materials and Methods
Following ethical approval by Newcastle University Faculty of Science, Agriculture and Engineering Ethics committee (16-BRO-049, approval date 6 September 2016). Following informed consent, a total of 10 healthy participants (21–38 years old) were recruited by convenience sampling for this randomised, crossover pilot study. The low number of participants used here is not expected to ensure statistical power of the findings but was aimed at developing the methodological approach. Individuals were excluded from taking part if they had history of gastro-oesophageal reflux disease, persistent associated symptoms such as heartburn and regurgitation, or were currently experiencing an upper airways infection.
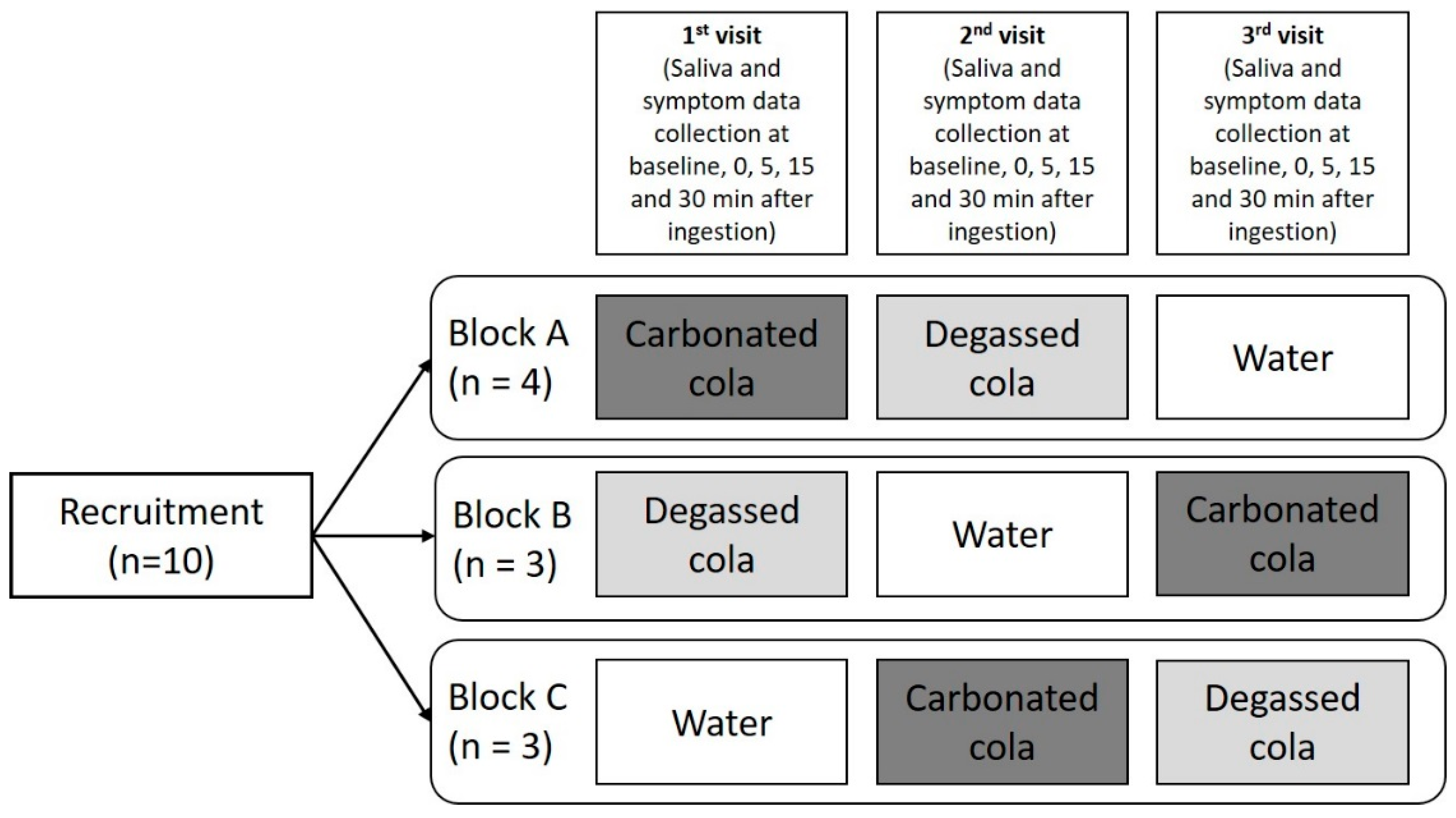
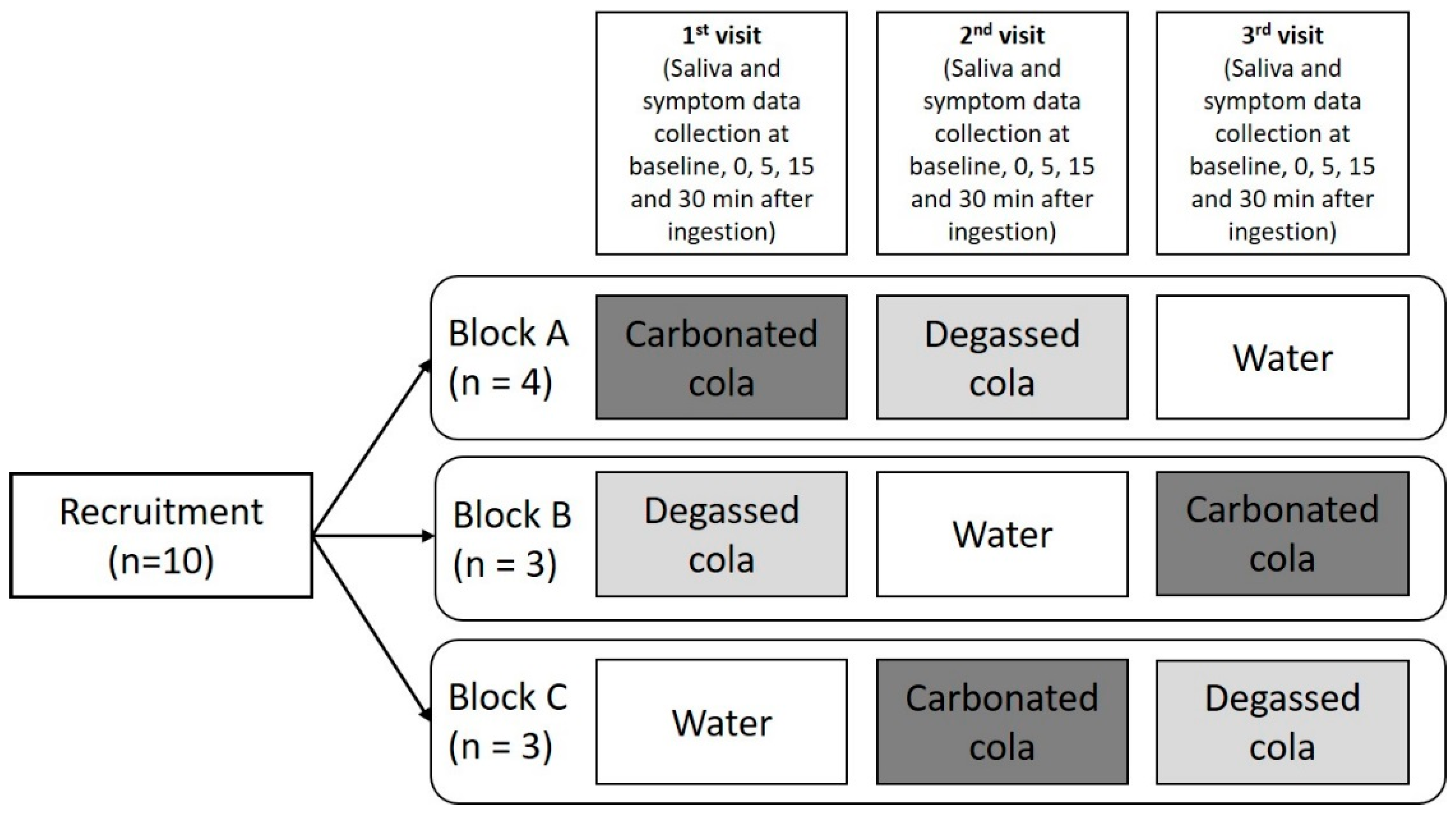
Participants were requested to attend three separate visits during the study after an overnight fast prior to each session (consumption of plain water was allowed on the morning of the study visits). Participants were randomly allocated to consume the beverage in three different orders (see Figure 3) while seated. Three hundred and thirty mL (a common volume for canned beverages) of each beverage was served at approximately 4 °C in a plastic cup based on their randomly allocated group. The beverages were chilled overnight in the fridge at approximately. Participants were asked to drink the given beverages within 5 min, although the exact time taken to consume the drink was not recorded.
Questionnaires (see Supplementary Materials) were provided to participants to collect information on their perception of various symptoms associated with gastro-oesophageal reflux (fullness in stomach, feeling of heartburn, urge to belch, urge to cough, churning of stomach/making noises, and breathing difficulties/choking episodes). These questions were adapted based on the questionnaires utilised in previous studies [45,46]. Belching and other symptoms were not monitored or assessed during the consumption of the test beverages. Participants were asked to rate their perception of each symptoms on a 5-point Likert scale (0–5) before ingestion and after ingestion (0, 5, 15 and 30 min) of the beverage. The scale indicates the degree of severity of the described symptom; with a higher score indicating that the symptom is more acutely problematic.
Saliva samples were collected prior to and at time points 0, 5, 15 and 30 min after ingestion of the beverage. Samples were collected in 50 mL test tubes containing 0.1 g of citric acid (preservative function) and subsequently transferred to microtubes before centrifuging at 10,000 rpm for 10 min to separate the supernatant from other components found in the saliva prior to storage at −80 °C before subsequent analysis. The saliva supernatant was diluted 1 in 5 (to reduce sample viscosity) using phosphate buffered saline pepsin analysis and was carried out using a previously described, indirect enzyme-linked, immunosorbent assay method [47]. Briefly, this 96-well plate method uses primary anti-pepsin/pepsinogen antibodies (Biodesign International, Saco, ME, USA), and secondary antibodies (anti-goat/sheep, Sigma Aldrich, Singapore), conjugated with horseradish peroxidase to quantitate the concentration of pepsin in samples. Addition of a colorimetric agent (2,2′-Azino-bis(3-ethylbenzthiazoline-6-sulfonic acid, Sigma Aldrich, Singapore) allows spectrophotometric estimation (at a wavelength of 405 nm) of pepsin concentration as a result of a green colour production.
All data were analysed using Prism 7 statistical software (GraphPad, La Jolla, CA, USA). Statistical analysis of the pepsin concentration and gastric symptoms between the three beverages were compared using Chi-square test (to assess whether relationships between variables exist) and non-parametric Kruskal Wallis test with post-hoc Dunn’s multiple test (to compare groups of data to each other). A p-value less than 0.05 was considered statistically significant.
5. Conclusions
The findings from this study are that carbonated cola does not cause detectable gastric reflux but may elicit symptoms of heartburn during this period. The approach used here is likely to be useful in evaluating the potential of a wider range of foods, beverages, nutrients and ingredients to trigger reflux, albeit with an altered baseline measurement and frequency of postprandial sampling.
Supplementary Materials
The following are available online at https://www.mdpi.com/2624-5647/1/1/4/s1.
Author Contributions
Project conceptualization, supervision and administration: I.A.B.; Data curation: S.X.L.B.; Investigation and Methodology development: S.X.L.B. and I.A.B.; Project administration, I.A.B.; Drafting, editing and review of manuscript: S.X.L.B and I.A.B.
Funding
This research received no external funding.
Acknowledgments
The authors would like to thank all participants for their valuable contribution and Lo Ee Peng for technical support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dent, J.; El-Serag, H.; Wallander, M.A.; Johansson, S. Epidemiology of gastro-oesophageal reflux disease: A systematic review. Gut 2005, 54, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Zuckerman, M.J.; Carrion, A.F. Gastro-Oesophageal Reflux Disease; BMJ Best Practice, BMJ Publishing Group Ltd.: London, UK, 2018. [Google Scholar]
- Broers, C.; Tack, J.; Pauwels, A. Review article: Gastro-oesophageal reflux disease in asthma and chronic obstructive pulmonary disease. Aliment. Pharmacol. Ther. 2018, 47, 176–191. [Google Scholar] [CrossRef] [PubMed]
- Harding, S.M.; Allen, J.E.; Blumin, J.H.; Warner, E.A.; Pellegrini, C.A.; Chan, W.W. Respiratory manifestations of gastroesophageal reflux disease. Ann. N. Y. Acad. Sci. 2013, 1300, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Boeckxstaens, G. The lower oesophageal sphincter. Neurogastroenterol. Motil. 2005, 17, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Goh, K.L.; Chang, C.S.; Fock, K.M.; Ke, M.; Park, H.J.; Lam, S.K. Gastro-oesophageal reflux disease in Asia. J. Gastroenterol. Hepatol. 2000, 15, 230–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Locke, G.R.; Talley, N.J.; Fett, S.L.; Zinsmeister, A.R.; Melton, L.J. Risk factors associated with symptoms of gastroesophageal reflux. Am. J. Med. 1999, 106, 642–649. [Google Scholar] [CrossRef]
- Nilsson, M.; Johnsen, R.; Ye, W.; Hveem, K.; Lagergren, J. Lifestyle related risk factors in the aetiology of gastro-oesophageal reflux. Gut 2004, 53, 1730–1735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holloway, R.H.; Hongo, M.; Berger, K.; McCallum, R.W. Gastric distention: A mechanism for postprandial gastroesophageal reflux. Gastroenterology 1985, 89, 779–784. [Google Scholar] [CrossRef]
- Straathof, J.; Ringers, J.; Lamers, C.; Masclee, A. Provocation of transient lower esophageal sphincter relaxations by gastric distension with air. Am. J. Gastroenterol. 2001, 96, 2317–2323. [Google Scholar] [CrossRef] [PubMed]
- Kubo, A.; Block, G.; Quesenberry, C.P.; Buffler, P.; Corley, D.A. Dietary guideline adherence for gastroesophageal reflux disease. BMC Gastroenterol. 2014, 14, 144. [Google Scholar] [CrossRef] [PubMed]
- Song, J.H.; Chung, S.J.; Lee, J.H.; Kim, Y.-H.; Chang, D.K.; Son, H.J.; Kim, J.J.; Rhee, J.C.; Rhee, P.-L. Relationship between gastroesophageal reflux symptoms and dietary factors in Korea. J. Neurogastroenterol. Motil. 2011, 17, 54. [Google Scholar] [CrossRef] [PubMed]
- Hamoui, N.; Lord, R.V.; Hagen, J.A.; Theisen, J.; DeMeester, T.R.; Crookes, P.F. Response of the lower esophageal sphincter to gastric distention by carbonated beverages. J. Gastrointest. Surg. 2006, 10, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Shukla, A.; Meshram, M.; Gopan, A.; Ganjewar, V.; Kumar, P.; Bhatia, S.J. Ingestion of a carbonated beverage decreases lower esophageal sphincter pressure and increases frequency of transient lower esophageal sphincter relaxation in normal subjects. Indian J. Gastroenterol. 2012, 31, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Cuomo, R.; Savarese, M.F.; Sarnelli, G.; Vollono, G.; Rocco, A.; Coccoli, P.; Cirillo, C.; Asciore, L.; Nardone, G.; Buyckx, M. Sweetened carbonated drinks do not alter upper digestive tract physiology in healthy subjects. Neurogastroenterol. Motil. 2008, 20, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.; Gerson, L.; Hershcovici, T.; Stave, C.; Fass, R. Systematic review: The effects of carbonated beverages on gastro-oesophageal reflux disease. Aliment. Pharmacol. Ther. 2010, 31, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Vakil, N. Test and treat or treat and test in reflux disease? Aliment. Pharmacol. Ther. 2003, 17, 57–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayat, J.O.; Gabieta-Somnez, S.; Yazaki, E.; Kang, J.-Y.; Woodcock, A.; Dettmar, P.; Mabary, J.; Knowles, C.H.; Sifrim, D. Pepsin in saliva for the diagnosis of gastro-oesophageal reflux disease. Gut 2015, 64, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Knight, J.; Lively, M.O.; Johnston, N.; Dettmar, P.W.; Koufman, J.A. Sensitive pepsin immunoassay for detection of laryngopharyngeal reflux. Laryngoscope 2005, 115, 1473–1478. [Google Scholar] [CrossRef] [PubMed]
- Samuels, T.L.; Johnston, N. Pepsin as a marker of extraesophageal reflux. Ann. Otol. Rhinol. Laryngol. 2010, 119, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Potluri, S.; Chang, A.; MacNeal, R.; Manus, C.; Parkman, H.P.; Bromer, M.; Fisher, R.; Neuman, T.; Kueppers, F.; Miller, L.S. Use of a pepsin assay in saliva and sputum to determine gastroesophageal reflux into the proximal esophagus, oral pharynx and lung. Am. J. Gastroenterol. 2001, 96, S23. [Google Scholar] [CrossRef]
- Na, S.Y.; Kwon, O.E.; Lee, Y.C.; Eun, Y.G. Optimal timing of saliva collection to detect pepsin in patients with laryngopharyngeal reflux. Laryngoscope 2016, 126, 2770–2773. [Google Scholar] [CrossRef] [PubMed]
- Sereg-Bahar, M.; Jerin, A.; Jansa, R.; Stabuc, B.; Hocevar-Boltezar, I. Pepsin and bile acids in saliva in patients with laryngopharyngeal reflux—A prospective comparative study. Clin. Otolaryngol. 2015, 40, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.M.; Robertson, A.G.N.; Bredenoord, A.J.; Brownlee, I.A.; Stovold, R.; Brodlie, M.; Forrest, I.; Dark, J.H.; Pearson, J.P.; Ward, C. Aspiration and allograft injury secondary to gastroesophageal reflux occur in the immediate post-lung transplantation period (Prospective Clinical Trial). Ann. Surg. 2013, 258, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Saritas Yuksel, E.; Hong, S.K.S.; Strugala, V.; Slaughter, J.C.; Goutte, M.; Garrett, C.G.; Dettmar, P.W.; Vaezi, M.F. Rapid salivary pepsin test: Blinded assessment of test performance in gastroesophageal reflux disease. Laryngoscope 2012, 122, 1312–1316. [Google Scholar] [CrossRef] [PubMed]
- Dolina, J.; Konečný, Š.; Ďurč, P.; Lačná, J.; Greguš, M.; Foret, F.; Skřičková, J.; Doubková, M.; Kindlová, D.; Pokojová, E.; et al. Evaluation of Important Analytical Parameters of the Peptest Immunoassay that Limit its Use in Diagnosing Gastroesophageal Reflux Disease. J. Clin. Gastroenterol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Portale, G.; Peters, J.; Hsieh, C.C.; Tamhankar, A.; Arain, M.; Hagen, J.; DeMeester, S.; DeMeester, T. When are reflux episodes symptomatic? Dis. Esophagus 2007, 20, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Wang, F.; Hu, Z.; Wu, J.; Wang, Z.; Yan, C.; Zhang, C.; Tang, J. The diagnostic value of pepsin detection in saliva for gastro-esophageal reflux disease: A preliminary study from China. BMC Gastroenterol. 2017, 17, 107. [Google Scholar] [CrossRef] [PubMed]
- Johnston, N.; Dettmar, P.W.; Ondrey, F.G.; Nanchal, R.; Lee, S.H.; Bock, J.M. Pepsin: Biomarker, mediator, and therapeutic target for reflux and aspiration. Ann. N. Y. Acad. Sci. 2018. [Google Scholar] [CrossRef] [PubMed]
- Hirschowitz, B.I. Gastric acid and pepsin secretion in patients with Barrett’s esophagus and appropriate controls. Dig. Dis. Sci. 1996, 41, 1384–1391. [Google Scholar] [CrossRef] [PubMed]
- Tipnis, N.A.; Rhee, P.L.; Mittal, R.K. Distension during gastroesophageal reflux: Effects of acid inhibition and correlation with symptoms. Am. J. Physiol. Gastrointest. Liver Physiol. 2007, 293, G469–G474. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, A.; Bardow, A.; Jensen, S.B.; Nauntofte, B. Saliva and gastrointestinal functions of taste, mastication, swallowing and digestion. Oral Dis. 2002, 8, 117–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, N.; Wells, C.W.; Samuels, T.L.; Blumin, J.H. Pepsin in nonacidic refluxate can damage hypopharyngeal epithelial cells. Ann. Otol. Rhinol. Laryngol. 2009, 118, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, P.M.; Castelo, P.M.; Carpenter, G.H.; Gavião, M.B.D. Masticatory function, taste, and salivary flow in young healthy adults. J. Oral Sci. 2016, 58, 391–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izumi, S.; Hong, G.; Iwasaki, K.; Izumi, M.; Matsuyama, Y.; Chiba, M.; Toda, T.; Kudo, T.A. Gustatory salivation is associated with body mass index, daytime sleepiness, and snoring in healthy young adults. Tohoku J. Exp. Med. 2016, 240, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Li-Hui, W.; Chuan-Quan, L.; Long, Y.; Ru-Liu, L.; Long-Hui, C.; Wei-Wen, C. Gender differences in the saliva of young healthy subjects before and after citric acid stimulation. Clin. Chim. Acta 2016, 460, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Barlow, W.J.; Orlando, R.C. The pathogenesis of heartburn in nonerosive reflux disease: A unifying hypothesis. Gastroenterology 2005, 128, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Fass, R.; Tougas, G. Functional heartburn: The stimulus, the pain, and the brain. Gut 2002, 51, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Richter, J. Heartburn, dysphagia, odynophagia, and other esophageal symptoms. In Gastrointestinal Disease, 5th ed.; WE Saunders Company: Philadelphia, PA, USA, 1993. [Google Scholar]
- Feldman, M.; Barnett, C. Relationships between the acidity and osmolality of popular beverages and reported postprandial heartburn. Gastroenterology 1995, 108, 125–131. [Google Scholar] [CrossRef]
- Bredenoord, A.J.; Smout, A.J. Physiologic and pathologic belching. Clin. Gastroenterol. Hepatol. 2007, 5, 772–775. [Google Scholar] [CrossRef] [PubMed]
- Barham, C.; Gotley, D.; Mills, A.; Alderson, D. Precipitating causes of acid reflux episodes in ambulant patients with gastro-oesophageal reflux disease. Gut 1995, 36, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Sifrim, D.; Castell, D.; Dent, J.; Kahrilas, P. Gastro-oesophageal reflux monitoring: Review and consensus report on detection and definitions of acid, non-acid, and gas reflux. Gut 2004, 53, 1024–1031. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Clinical Excellence. Dyspepsia and Gastrooesophageal Reflux Disease: Investigation and Management of Dyspepsia, Symptoms Suggestive of Gastro-Oesophageal Reflux Disease, or Both (CG184). Available online: https://www.nice.org.uk/guidance/cg184 (accessed on 12 July 2018).
- Ploutz-Snyder, L.; Foley, J.; Ploutz-Snyder, R.; Kanaley, J.; Sagendorf, K.; Meyer, R. Gastric gas and fluid emptying assessed by magnetic resonance imaging. Eur. J. Appl. Physiol. Occup. Physiol. 1999, 79, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Postma, G.N.; Halum, S.L. Laryngeal and pharyngeal complications of gastroesophageal reflux disease. GI Motil. Online 2006. [Google Scholar] [CrossRef]
- Decalmer, S.; Stovold, R.; Houghton, L.A.; Pearson, J.; Ward, C.; Kelsall, A.; Jones, H.; McGuinness, K.; Woodcock, A.; Smith, J.A. Chronic cough: Relationship between microaspiration, gastroesophageal reflux, and cough frequency. Chest 2012, 142, 958–964. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Changes in salivary pepsin concentration (median ± interquartile range) between beverages ( ![Gastrointestdisord 01 00004 i001]() Carbonated cola;
Carbonated cola; ![Gastrointestdisord 01 00004 i002]() Degassed cola;
Degassed cola; ![Gastrointestdisord 01 00004 i003]() Water) over after ingestion compared to baseline (pre-ingestion). No statistically significant difference was observed at a p-value of 0.05.
Water) over after ingestion compared to baseline (pre-ingestion). No statistically significant difference was observed at a p-value of 0.05.
 Carbonated cola;
Carbonated cola;  Degassed cola;
Degassed cola;  Water) over after ingestion compared to baseline (pre-ingestion). No statistically significant difference was observed at a p-value of 0.05.
Water) over after ingestion compared to baseline (pre-ingestion). No statistically significant difference was observed at a p-value of 0.05.
Figure 1.
Changes in salivary pepsin concentration (median ± interquartile range) between beverages ( ![Gastrointestdisord 01 00004 i001]() Carbonated cola;
Carbonated cola; ![Gastrointestdisord 01 00004 i002]() Degassed cola;
Degassed cola; ![Gastrointestdisord 01 00004 i003]() Water) over after ingestion compared to baseline (pre-ingestion). No statistically significant difference was observed at a p-value of 0.05.
Water) over after ingestion compared to baseline (pre-ingestion). No statistically significant difference was observed at a p-value of 0.05.
Carbonated cola; Degassed cola; Water) over after ingestion compared to baseline (pre-ingestion). No statistically significant difference was observed at a p-value of 0.05.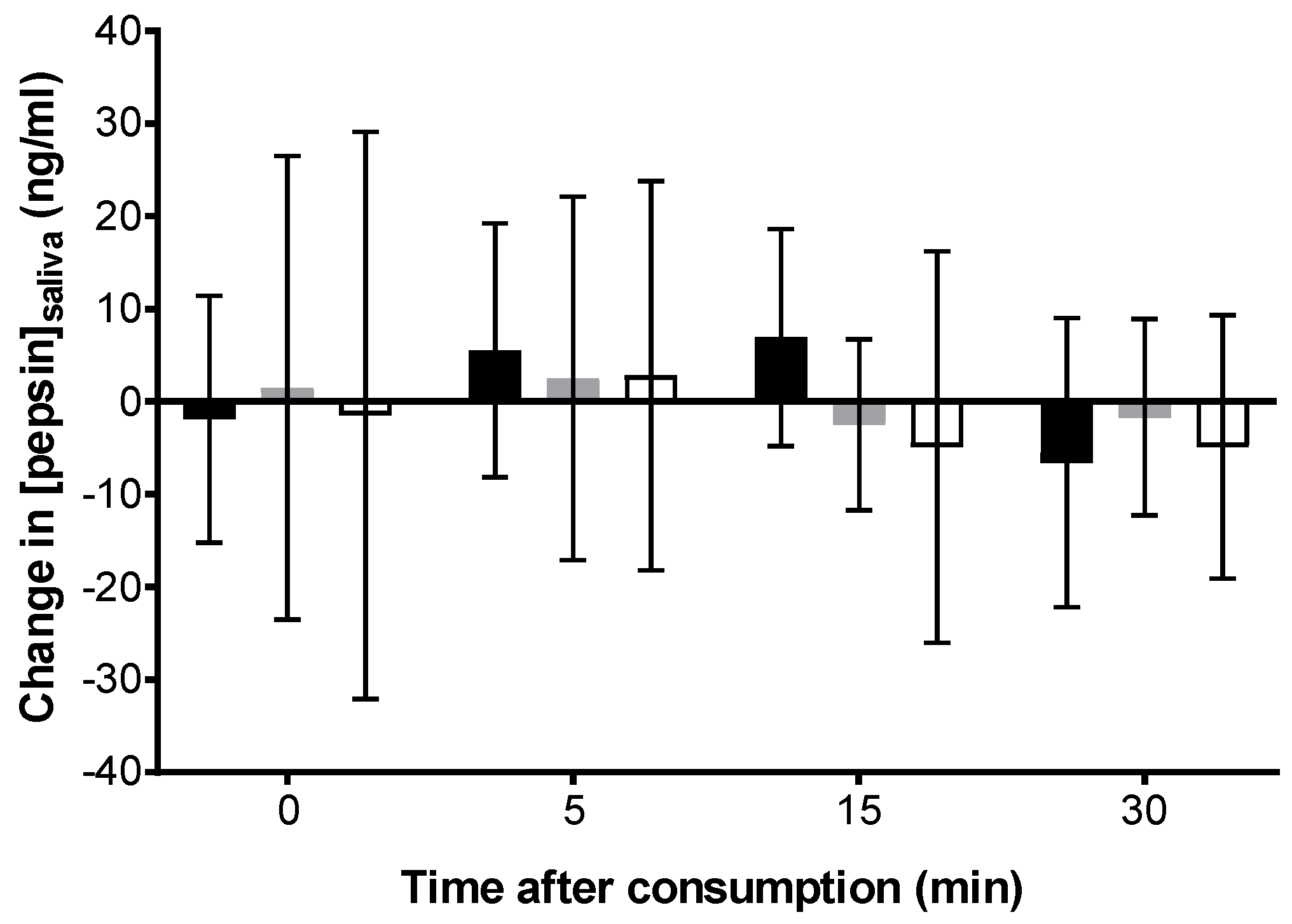
Figure 2.
Changes (versus baseline) in scores of fullness (A), heartburn (B), urge to belch (C) and number of belches (D) over time after ingestion of beverages. Data presented are medians ± interquartile range. ![Gastrointestdisord 01 00004 i004]() Carbonated cola;
Carbonated cola; ![Gastrointestdisord 01 00004 i005]() Degassed cola;
Degassed cola; ![Gastrointestdisord 01 00004 i006]() Water). * Carbonated cola value statistically different from water (p < 0.05) at this time-point. Comparisons to degassed cola are presented in-text.
Water). * Carbonated cola value statistically different from water (p < 0.05) at this time-point. Comparisons to degassed cola are presented in-text.
 Carbonated cola;
Carbonated cola;  Degassed cola;
Degassed cola;  Water). * Carbonated cola value statistically different from water (p < 0.05) at this time-point. Comparisons to degassed cola are presented in-text.
Water). * Carbonated cola value statistically different from water (p < 0.05) at this time-point. Comparisons to degassed cola are presented in-text.
Figure 2.
Changes (versus baseline) in scores of fullness (A), heartburn (B), urge to belch (C) and number of belches (D) over time after ingestion of beverages. Data presented are medians ± interquartile range. ![Gastrointestdisord 01 00004 i004]() Carbonated cola;
Carbonated cola; ![Gastrointestdisord 01 00004 i005]() Degassed cola;
Degassed cola; ![Gastrointestdisord 01 00004 i006]() Water). * Carbonated cola value statistically different from water (p < 0.05) at this time-point. Comparisons to degassed cola are presented in-text.
Water). * Carbonated cola value statistically different from water (p < 0.05) at this time-point. Comparisons to degassed cola are presented in-text.
Carbonated cola; Degassed cola; Water). * Carbonated cola value statistically different from water (p < 0.05) at this time-point. Comparisons to degassed cola are presented in-text.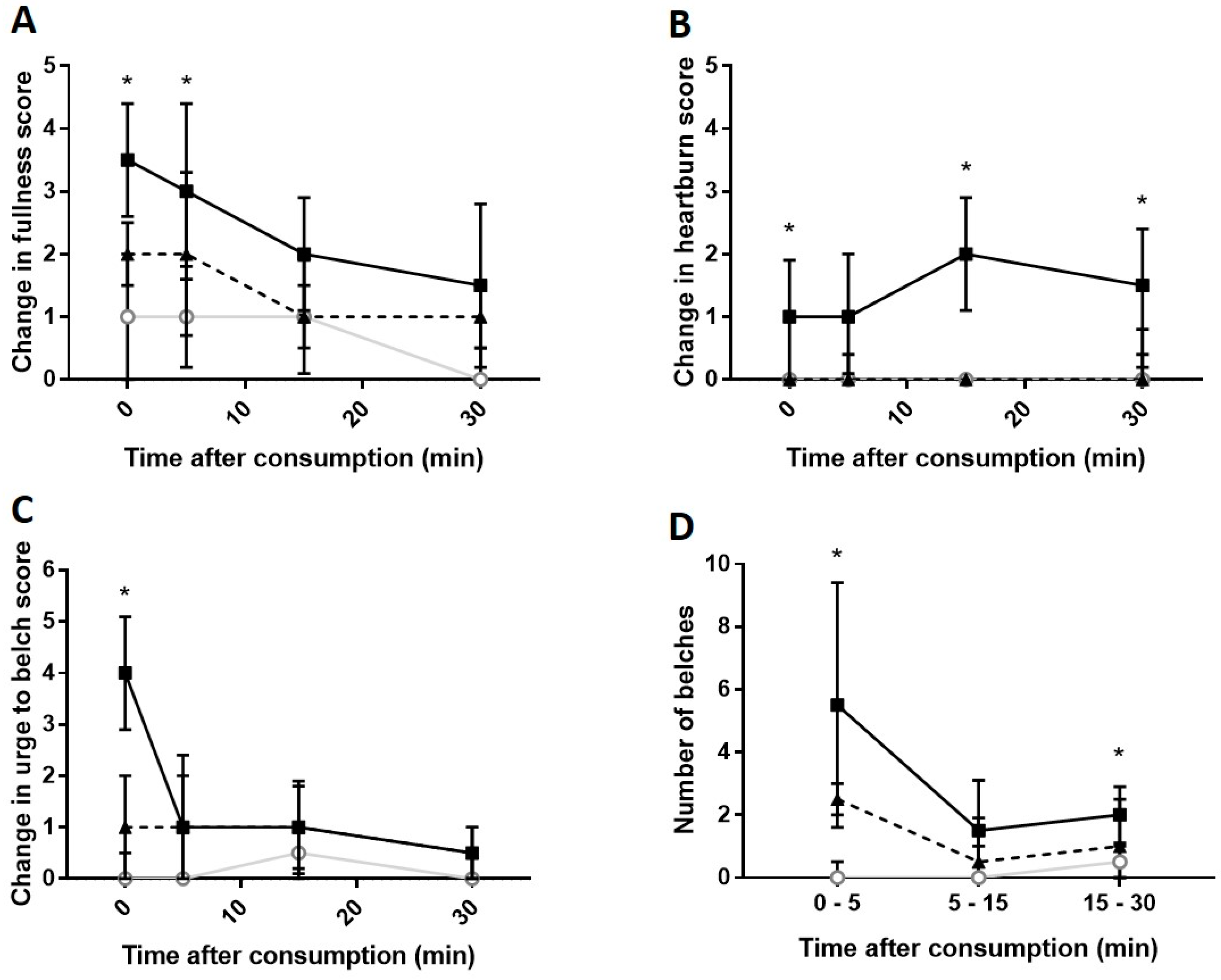
Figure 3.
Overview of the design of this randomised, crossover preliminary trial. All 10 participants completed the study.
Figure 3.
Overview of the design of this randomised, crossover preliminary trial. All 10 participants completed the study.
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lim, S.X.B.; Brownlee, I.A. Assessment of the Acute Effects of Carbonated Beverage Consumption on Symptoms and Objective Markers of Gastric Reflux. Gastrointest. Disord. 2019, 1, 30-38. https://doi.org/10.3390/gidisord1010004
AMA Style
Lim SXB, Brownlee IA. Assessment of the Acute Effects of Carbonated Beverage Consumption on Symptoms and Objective Markers of Gastric Reflux. Gastrointestinal Disorders. 2019; 1(1):30-38. https://doi.org/10.3390/gidisord1010004
Chicago/Turabian StyleLim, Shi Xiang Brandon, and Iain A. Brownlee. 2019. "Assessment of the Acute Effects of Carbonated Beverage Consumption on Symptoms and Objective Markers of Gastric Reflux" Gastrointestinal Disorders 1, no. 1: 30-38. https://doi.org/10.3390/gidisord1010004