Bacillus cereus Induced Necrotizing Fasciitis Mimicking Gastroenteritis: A Case Report
by
 ,
,
Ling-Chi Lee
1,2, 
Yu-Long Chen
1,2,
Giou-Teng Yiang
1,2,
Tsu-Yi Chen
1,2,
Meng-Yu Wu
1,2,
Bo-Yang Ni
1,2 and
Ching-Hsiang Lin
1,2,* 1
Department of Emergency Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei 231, Taiwan
2
Department of Emergency Medicine, School of Medicine, Tzu Chi University, Hualien 970, Taiwan
*
Author to whom correspondence should be addressed.
Reports 2018, 1(1), 9; https://doi.org/10.3390/reports1010009
Submission received: 26 March 2018
/
Revised: 5 April 2018
/
Accepted: 6 April 2018
/
Published: 9 April 2018
{kind=link}
{kind=link}
Abstract
:Necrotizing fasciitis is a rapidly spreading inflammation of the soft tissue involving the fascia and the subcutaneous tissue. Early and aggressive surgical intervention accompanied with appropriate antibiotics are the key to improve clinical outcome in patients with necrotizing fasciitis. Here, we present the case of a 46-year-old male who presented with acute onset progressive watery diarrhea and fever for one day. The abdominal ultrasound and computed tomography revealed diffuse gallbladder wall thickening with double layer sign, air density at right hepatic lobe and a small bowel edema. An intra-abdominal infection was initially suspected. However, a progressive erythematous change and bullae was found on the left thigh and lower abdomen. Progressed necrotizing fasciitis was suspected. After administration of broad antibiotics and emergency surgical intervention, the septic shock was reversed. Finally, the blood and wound culture reports revealed Bacillus cereus growth. This paper describes the clinical features of necrotizing fasciitis and highlights the Bacillus cereus-induced necrotizing fasciitis for physicians in order to promote timely intervention for septic shock.
1. Introduction
Necrotizing fasciitis is a rapidly progressing and potentially devastating infection of soft tissues. The high mortality rate was reported to be about 40–60% in previous studies [1,2]. The typical symptoms include local swelling and erythema accompanied with fever and pain. In advanced necrotizing fasciitis, the formation of bullae, skin necrosis and crepitus can be identified. Trauma, insect bites, surgical incisions are predisposing factors in a healthy host. The disease may progress rapidly in patients with immunosuppression and diabetes mellitus. Therefore, early diagnosis, timely surgical intervention and appropriate antibiotics are important tools for physicians to control progression of septic shock. This paper describes the clinical features of necrotizing fasciitis and highlights the Bacillus cereus-induced necrotizing fasciitis for physicians in order to promote timely intervention for septic shock.
2. Case Presentation Section
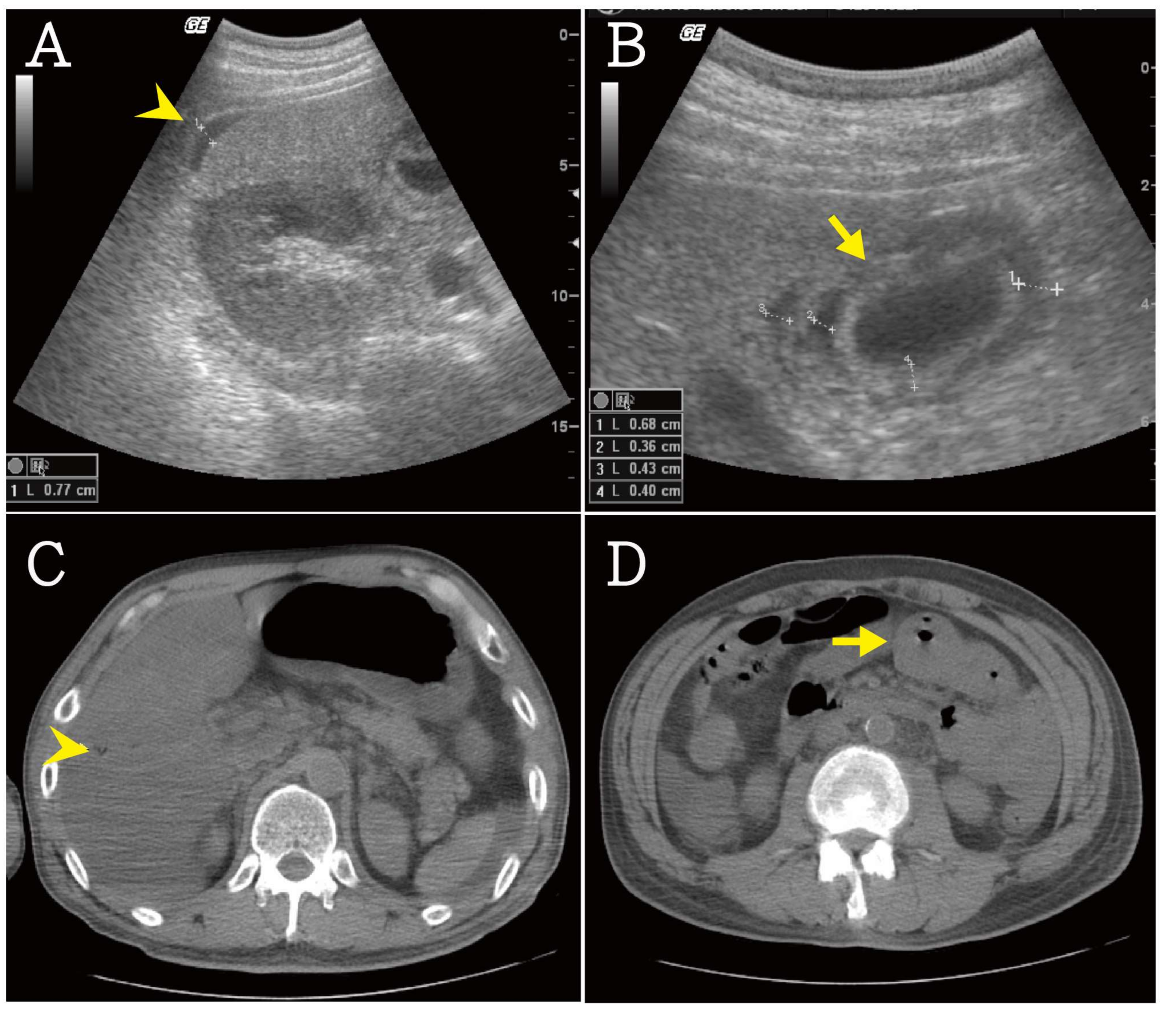
A 46-year-old male presented with acute onset progressive watery diarrhea and fever for one day. He had a history of chronic obstructive pulmonary disease without regular control. There was no history of trauma. He remembered that watery diarrhea occurred after eating expired canned food. He was not suffering from productive cough, chest pain, abdominal pain, frequency, urgency, or dysuria. His temperature was 38.1 °C, respiratory rate was 40/min, heart rate was 179/min, and blood pressure could not be measured at emergency department. The severe hypotension, fever, and acute delirium were noted. The Glasgow Coma Scale revealed E4V2M5. On physical examination, the sclera was mild icteric and bilateral coarse breath sound. The whole abdomen tenderness was noted. The murphy sign was negative and McBurney’s point demonstrated no tenderness. Hyperactive bowel sound was recorded. The laboratory evaluation included: white cell count of 1790/µL (band form neutrophils 10.0%, segment form neutrophils 13.0%, lymphocytes 60.0%, eosinophils 0.0%, and monocytes 5.0%), hemoglobin 10.5 g/dL, platelet counts 62000/mL, creatinine 2.4 mg/dL, alanine aminotransferase 30 U/L, total bilirubin 5.21 mg/dL, albumin 1.2 g/dL, lipase 132 IU/L, CK-MB 185 IU/L, troponin I 0.08 µg/L, sodium 133 mmole/L, potassium 3.6 mmole/L, C-reaction peptide 1.47 mg/dL. The arterial blood gas analysis revealed pH: 7.243, pCO2: 22.1 mmHg, pO2: 267.8 mmHg, HCO3: 9.3 mmole/L, ABE: −15.9 mmole/L, BEecf: −18.0 mmole/L, and O2 saturation: 99.7%. The urinalysis results showed a red cell count of 2–5/HPF and white cell count of 0–2/HPF. The plain film showed pulmonary infiltration at the bilateral upper lung field. The abdominal ultrasound showed diffuse gallbladder wall thickening with peri-gallbladder fluid accumulation presenting double layer sign (Figure 1A,B). The computed tomography of the abdomen showed fatty infiltration of the liver with air density at the right hepatic lobe and the wall edema was noted at the small bowel accompanied by mild ascites (Figure 1C,D). Under the clinical symptoms and images, intra-abdominal infection inducing septic shock was initially suspected.
The empiric antibiotics, Vancomycin, Imipenem and Ciprofloxacin, were administrated to cover Streptococcus, Staphylococcus, Aeromonas hydrophila, Vibrio vulnificus and Hemophilus influenzae. The hyperpigmentation, desquamation and formation of bullae on left thigh and lower abdomen was found (Figure 2A–D). Progressed necrotizing fasciitis was suspected and emergency surgical intervention was suggested. He received fasciotomy and debridement nine times. The culture reports showed Bacillus cereus growth in the blood and wound. After his infectious condition was stable, the skin grafting was done for left thigh and buttock wounds. Due to the stable condition, he received regular follow up at the outpatient department. An oral informed consent was obtained from the patient.
3. Discussion
Necrotizing fasciitis is a uncommon but life-threatening infection characterized by involving the subcutaneous tissue and fascia [3]. Previous studies revealed that only 15% to 34% of patients have an accurate diagnosis at admission [4,5]. The rapid destruction of tissue and inducing sepsis may lead to gross morbidity and mortality. Recent studies reported a mortality of 16.4% for community-acquired necrotizing fasciitis and 36.3% for postprocedural necrotizing infections [6,7]. Early diagnosis and aggressive surgical intervention are necessary and can significantly reduce mortality and morbidity [8]. In clinical practice, necrotizing fasciitis can be described by their anatomical locations, such as Fournier gangrene, or the depth of invasion, such as cellulitis, fasciitis, and myositis. Giuliano et al. [9] reported the classification system of pathogen: type I polymicrobial with γ-positive cocci, γ-negative rods and anaerobes; type II group A β-hemolytic streptococci, with/without combination with staphylococcal species; type III γ-negative marine organisms, especially Vibrio vulnificus. In our case, Bacillus cereus was isolated from the blood and the wound.
Bacillus cereus is a γ-positive aerobic or facultatively anaerobic rod-like bacterium, which is widespread in the environment [10]. However, Bacillus cereus can sometimes cause gastroenteritis, pneumonia, meningitis, and necrotizing fasciitis. The pathogenesis of Bacillus cereus-inducing clinical symptoms is the production of tissue-destructive exoenzymes [1]. In immunocompromised patients, the progression of Bacillus cereus infection would be more rapid and severe. Timely, appropriate antibiotic administration is very important to control the infection. The presentation of Bacillus cereus infection, such as formation of gas or gangrene, may be similar to Clostridium species, which are sensitive to penicillin group. However, Bacillus cereus are resistant to β-lactam antibiotics, including penicillins and cephalosporins, due to the production of β-lactamase [11]. The aminoglycosides, clindamycin, vancomycin, chloramphenicol, erythromycin, and fluoroquinolones are susceptible for Bacillus cereus. In addition, linezolid, daptomycin, and tigecycline are alternative and new antimicrobial treatments.
Previous studies reported that Bacillus cereus-inducing necrotizing fasciitis commonly occurred in immunosuppressed patients [12], such as diabetes mellitus [13] and liver disease [11]. In our case, the patient only had a history of chronic obstructive pulmonary disease which impairs immune systems less than other underlying disease. The event of eating expired canned food is a hint in this case. We believed that Bacillus cereus induced acute gastroenteritis and led to bacteria translocation to the soft tissue. The travel, occupation, clustering and contact history are important for physicians to survey the infection origin site. In this article, we highlighted an early diagnosis of Bacillus cereus-inducing necrotizing fasciitis which enabled early administration of an appropriate antibiotic without delay.
Author Contributions
Ling-Chi Lee, Yu-Long Chen, and Giou-Teng Yiang wrote the paper and contributed to the organization of figure; Tsu-Yi Chen and Meng-Yu Wu provided conceptual input; Bo-Yang Ni and Ching-Hsiang Lin proofread and organized the manuscript. All authors reviewed the final version of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hutchens, A.; Gupte, A.; McAuliffe, P.F.; Schain, D.; Soldevila-Pico, C.; Knapik, J.A.; Fujita, S.; Mozingo, D.W.; Richards, W.T. Bacillus cereus necrotizing fasciitis in a patient with end-stage liver disease. Surg. Infect. 2010, 11, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Minnaganti, V.R.; Patel, P.J.; Iancu, D.; Schoch, P.E.; Cunha, B.A. Necrotizing fasciitis caused by Aeromonas hydrophila. Heart Lung J. Crit. Care 2000, 29, 306–308. [Google Scholar] [CrossRef] [PubMed]
- Puvanendran, R.; Huey, J.C.M.; Pasupathy, S. Necrotizing fasciitis. Can. Fam. Phys. 2009, 55, 981–987. [Google Scholar]
- Wong, C.H.; Chang, H.C.; Pasupathy, S.; Khin, L.W.; Tan, J.L.; Low, C.O. Necrotizing fasciitis: Clinical presentation, microbiology, and determinants of mortality. J. Bone Jt. Surg. Am. Vol. 2003, 85, 1454–1460. [Google Scholar] [CrossRef]
- Hefny, A.F.; Eid, H.O.; Al-Hussona, M.; Idris, K.M.; Abu-Zidan, F.M. Necrotizing fasciitis: A challenging diagnosis. Eur. J. Emerg. Med. 2007, 14, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Frazee, B.W.; Fee, C.; Lynn, J.; Wang, R.; Bostrom, A.; Hargis, C.; Moore, P. Community-acquired necrotizing soft tissue infections: A review of 122 cases presenting to a single emergency department over 12 years. J. Emerg. Med. 2008, 34, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.T.; Saadai, P.; Greenstein, A.; Divino, C.M. Postprocedural necrotizing fasciitis: A 10-year retrospective review. Am. Surg. 2008, 74, 405–409. [Google Scholar] [PubMed]
- Voros, D.; Pissiotis, C.; Georgantas, D.; Katsaragakis, S.; Antoniou, S.; Papadimitriou, J. Role of early and extensive surgery in the treatment of severe necrotizing soft tissue infection. Br. J. Surg. 1993, 80, 1190–1191. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.; Lewis, F., Jr.; Hadley, K.; Blaisdell, F.W. Bacteriology of necrotizing fasciitis. Am. J. Surg. 1977, 134, 52–57. [Google Scholar] [CrossRef]
- Bottone, E.J. Bacillus cereus, a Volatile Human Pathogen. Clin. Microbiol. Rev. 2010, 23, 382–398. [Google Scholar] [CrossRef] [PubMed]
- Sada, A.; Misago, N.; Okawa, T.; Narisawa, Y.; Ide, S.; Nagata, M.; Mitsumizo, S. Necrotizing fasciitis and myonecrosis “synergistic necrotizing cellulitis” caused by Bacillus cereus. J. Dermatol. 2009, 36, 423–426. [Google Scholar] [CrossRef] [PubMed]
- Boulinguez, S.; Viraben, R. Cutaneous Bacillus cereus infection in an immunocompetent patient. J. Am. Acad. Dermatol. 2002, 47, 324–325. [Google Scholar] [CrossRef] [PubMed]
- Michelotti, F.; Bodansky, H.J. Bacillus cereus causing widespread necrotising skin infection in a diabetic person. Pract. Diabetes 2015, 32, 169–170. [Google Scholar] [CrossRef]
Figure 1.
(A,B) The abdominal ultrasound showed diffuse gallbladder wall thickening with peri-gallbladder fluid accumulation (arrow head) presenting double layer sign (arrow); (C,D) The fatty infiltration of liver with air density (arrow head) at right hepatic lobe and the wall edema of small bowel (arrow) accompanied with mild ascites were noted in abdominal computed tomography scan.
Figure 1.
(A,B) The abdominal ultrasound showed diffuse gallbladder wall thickening with peri-gallbladder fluid accumulation (arrow head) presenting double layer sign (arrow); (C,D) The fatty infiltration of liver with air density (arrow head) at right hepatic lobe and the wall edema of small bowel (arrow) accompanied with mild ascites were noted in abdominal computed tomography scan.
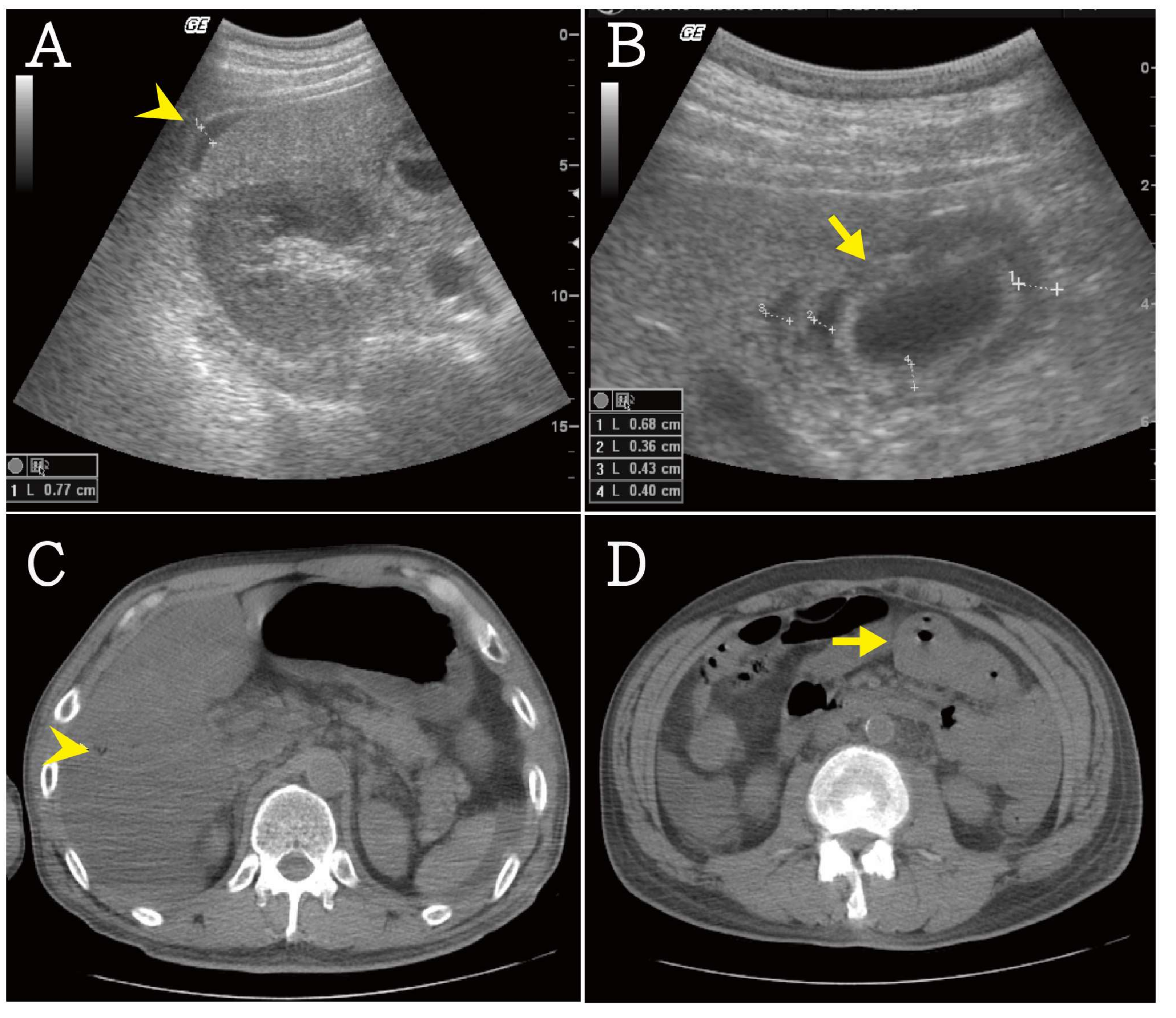
Figure 2.
(A–D) The hyperpigmentation, desquamation and formation of bullae were noted on left thigh and lower abdomen. The yellowish pus was founded during fasciotomy.
Figure 2.
(A–D) The hyperpigmentation, desquamation and formation of bullae were noted on left thigh and lower abdomen. The yellowish pus was founded during fasciotomy.

© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lee, L.-C.; Chen, Y.-L.; Yiang, G.-T.; Chen, T.-Y.; Wu, M.-Y.; Ni, B.-Y.; Lin, C.-H. Bacillus cereus Induced Necrotizing Fasciitis Mimicking Gastroenteritis: A Case Report. Reports 2018, 1, 9. https://doi.org/10.3390/reports1010009
AMA Style
Lee L-C, Chen Y-L, Yiang G-T, Chen T-Y, Wu M-Y, Ni B-Y, Lin C-H. Bacillus cereus Induced Necrotizing Fasciitis Mimicking Gastroenteritis: A Case Report. Reports. 2018; 1(1):9. https://doi.org/10.3390/reports1010009
Chicago/Turabian StyleLee, Ling-Chi, Yu-Long Chen, Giou-Teng Yiang, Tsu-Yi Chen, Meng-Yu Wu, Bo-Yang Ni, and Ching-Hsiang Lin. 2018. "Bacillus cereus Induced Necrotizing Fasciitis Mimicking Gastroenteritis: A Case Report" Reports 1, no. 1: 9. https://doi.org/10.3390/reports1010009