1. Introduction
The age-related decrease in muscle mass in humans begins in the fifth decade of life [
1,
2,
3]. This muscle mass loss often coexists with low muscle strength [
4,
5], functionality [
6,
7], and higher disability [
8,
9], which in turn are related with lower quality of life [
10,
11], and higher healthcare expenses [
12], and mortality [
13,
14,
15]. Current evidence suggests that lifestyle factors are significantly associated with functionality and physical disability. For instance, physically active older adults and those engaged in exercise programs show higher functionality and lower physical disability than their less physically active counterparts [
16,
17,
18,
19,
20,
21]. Additionally, dietary factors, such as low dietary protein intake, are also associated with these outcomes, whereas older adults who consume higher amounts of protein have been reported to have higher muscle mass [
22,
23], better functionality [
24,
25] and lower disability [
26,
27] in some studies.
Currently, it is considered that older adults should consume more protein than their younger counterparts [
28,
29]. Indeed, the PROT-AGE study group recommended that older adults should consume at least 1.0 to 1.2 g protein /kg body mass/day to maintain or gain muscle mass and function [
28]. Similarly, 30 g protein or 0.4 g protein/kg body mass per meal (deemed adequate) are recommended to stimulate the muscle protein synthesis optimally [
29,
30], leading to protein accrual if it overcomes the muscle protein breakdown [
31]. These recommendations for older adults are higher than for younger adults due to several age-related factors that decrease the anabolic response to amino acids in the elderly (i.e., anabolic resistance), reducing the stimulation of muscle protein synthesis and hampering the positive protein net balance [
32,
33]. Therefore, a higher protein intake would be needed to overcome the anabolic resistance.
In addition to daily protein intake, protein distribution, and per meal content have gained interest as other factors to consider [
34,
35]. Some studies have investigated if protein intake per meal at certain doses is related to muscle mass and functionality in older adults [
36,
37,
38]. They found that the consumption of two or more meals with ≥30 g of protein each is significantly associated with higher leg muscle mass and leg strength [
36], and <30 g of protein at specific meals is associated with lower functionality [
37]. Nonetheless, these results have not been consistent [
38].
While muscle mass, muscle strength, and functionality are strong predictors of physical disability [
7,
9,
39], to the best of our knowledge, the approach to the association between per-meal protein intake and physical disability have not been studied in older adults. Therefore, the purpose of this study was to analyze the association between adequate protein intake per meal and physical disability on daily living activities in Mexican adults aged 60 years or older.
4. Discussion
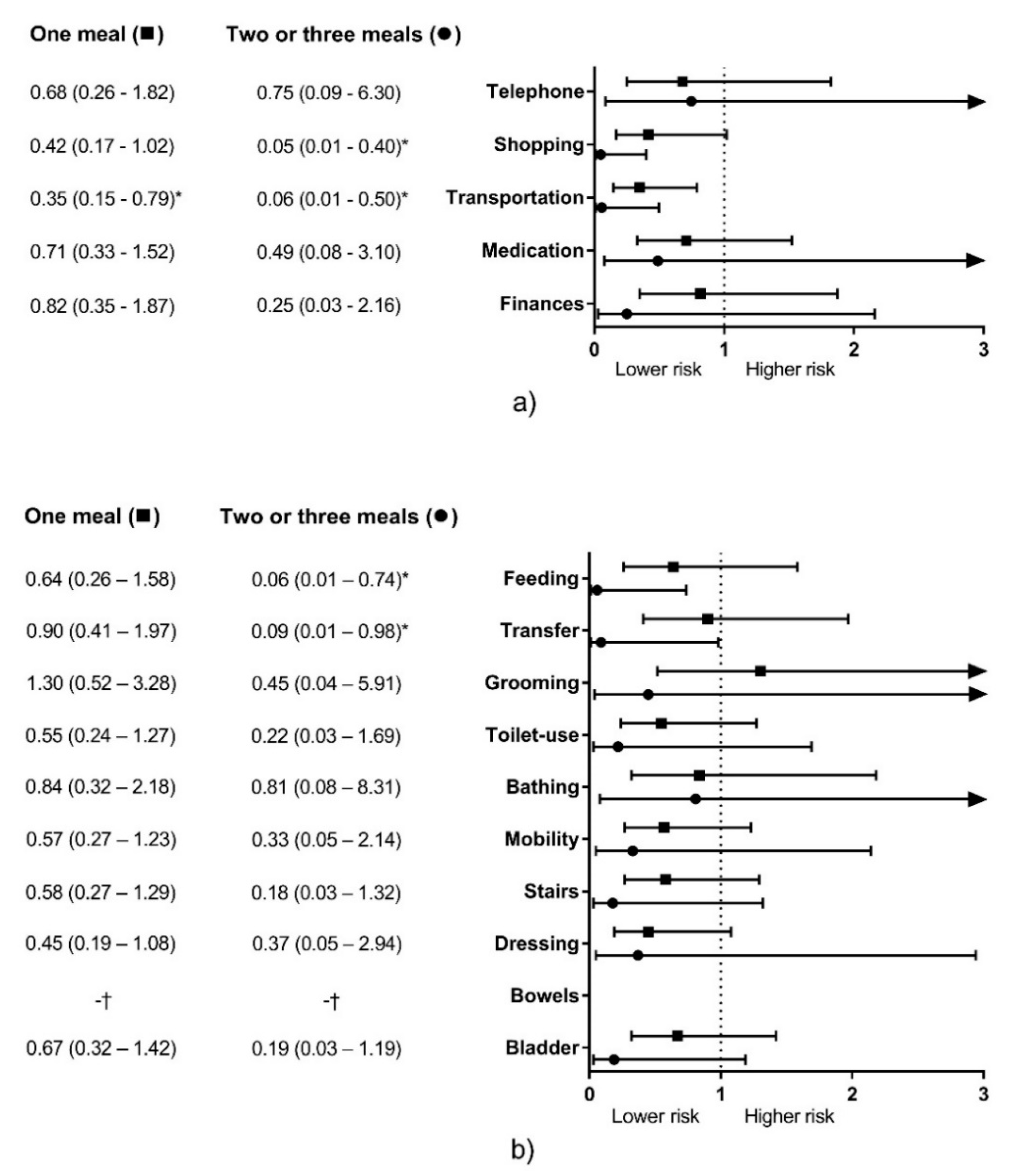
In this study, we observed that consuming two or three meals per day with ≥30 g protein each was significantly associated with lower physical disability risk for two IADL items and two ADL items. Conversely, eating one meal with this protein content was associated with one IADL item only (
Figure 1).
To our knowledge, no previous studies have analyzed the association between per-meal protein intake for a certain amount and physical disability. However, there are other studies with a similar approach [
36,
38]. In this regard, Loenneke et al. [
36] reported that older adults consuming two or more meals with ≥30 g protein showed higher leg lean mass and leg strength than those consuming one or zero meals with this criterion. We believe that consuming two or three meals with this protein content was associated with a lower risk of physical disability for more items than consuming one meal because the benefit over muscle mass and strength is bigger for two or more meals with this protein dose than with one meal [
36]. Therefore, it is possible that the benefits of muscle mass and strength observed with consuming one meal are not enough to decrease the risk of disability, as happened with two or three meals.
Additionally, high protein intake is associated with a lower age-related decrease in muscle mass and muscle strength [
24,
48,
49], and consuming more meals above this threshold is associated with higher total protein intake (
Table 3). Therefore, eating two or more meals with ≥30 g of protein each might be helpful to decrease the age-related decline on lean mass and functionality to a higher level than one meal [
35,
50], which could lead to a lower risk of physical disability [
26].
On the other hand, Gingrich et al. [
38] reported that consuming two or more meals with ≥0.4 g protein/kg was not significantly associated with muscle mass, muscle strength, nor muscle power in older adults. The results of Gingrich et al. may differ from previous studies and ours because they evaluated a sample of healthier older adults (subjects with >10 points in the short physical performance battery, <5% unintended weight loss the last three months, ≈96% of the sample was well-nourished, and diabetes and impaired glucose regulation as the only clinical concerns). Indeed, the authors suggested that this kind of protein recommendation would be necessary for older adults with poorer health status.
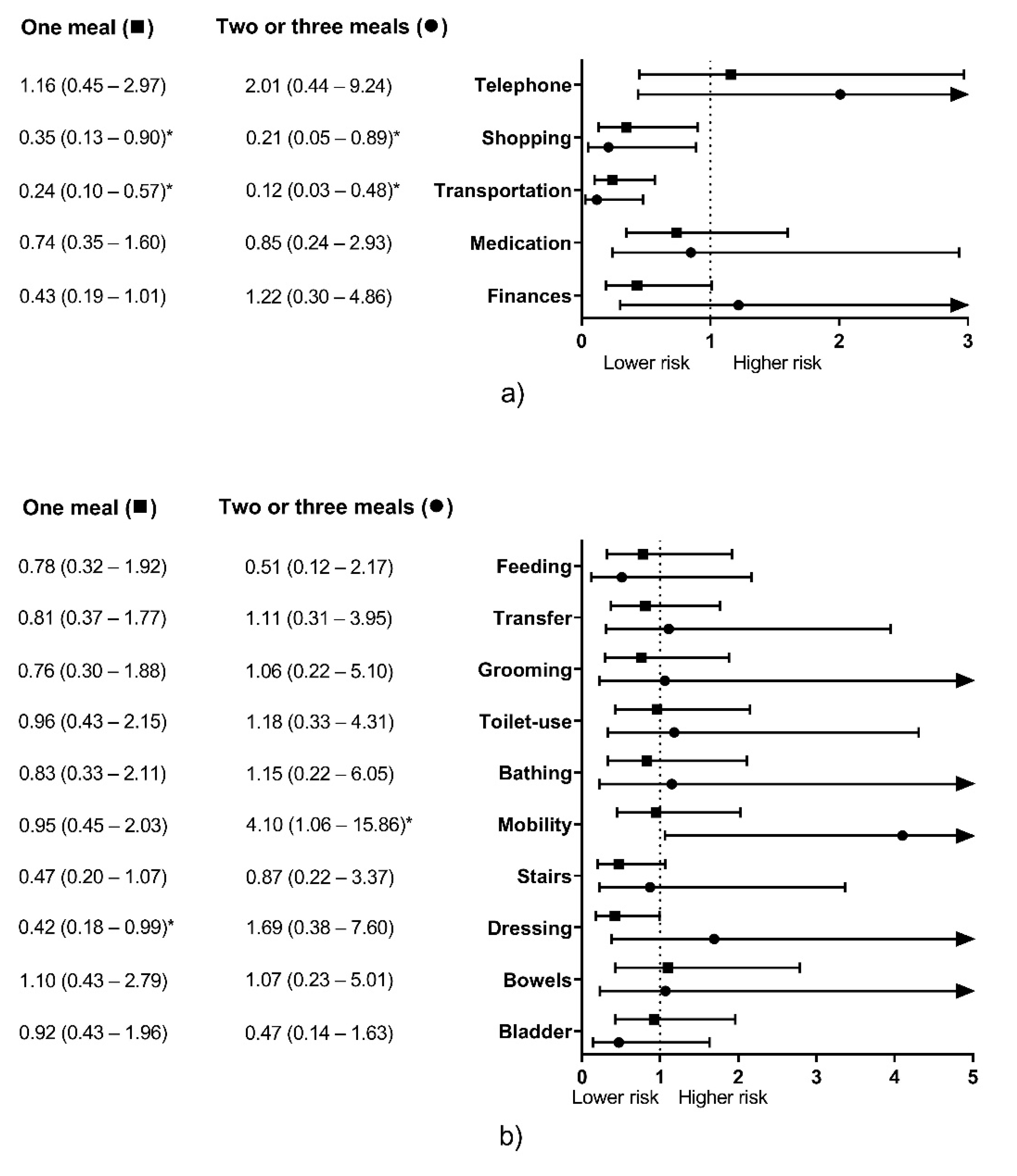
When meals were evaluated with the ≥0.4 g protein/kg threshold, there were conflicting results. Consuming 1M and +2M containing ≥0.4 g protein/kg were significantly associated with lower physical disability risk for two IADL items, Shopping, and Transportation (
Figure 2a). Conversely, consuming 1M was associated with lower physical disability risk for one ADL item (Dressing), and eating +2M was associated with higher physical disability risk for one ADL item (Mobility) (
Figure 2b). Other studies also reported conflicting results with protein intake and other disability-associated variables (e.g., low skeletal muscle mass). Gregorio et al. [
25] and Beasley et al. [
51] reported that older adults consuming >0.8 g protein/kg/d showed lower skeletal muscle mass than those consuming protein below this threshold, and Isanejad et al. [
24] reported that sarcopenic women ate more relative protein (g/kg/d) than their non-sarcopenic counterparts. It is possible that higher relative protein intake is observed in sarcopenic or disabled people because of their lower body weight [
52]. However, their relative protein intake would still not be enough to stimulate muscle protein synthesis optimally. It is recommended that older people with undernutrition or another chronic illness eat more protein (1.2 to 1.5 g/kg/d) to overcome the possible anabolic resistance derived from their condition [
28]. We believe that the same could happen for per-meal protein intake. Due to chronic illness may lead to inactivity and inflammation, higher protein dosage per meal could be needed to overcome the anabolic resistance and contribute to the higher daily protein intake [
53].
Therefore, the amount of 30 g protein/meal could be more useful for predicting physical disability than the 0.4 g protein/kg/meal criterion in a cross-sectional design. The former significantly predicted physical disability in two items for both IADL and ADL each (
Figure 1), while the latter significantly predicted disability for two IADL items, and showed conflicting results for two ADL items (
Figure 2).
However, experimental studies have demonstrated that both protein dosages (i.e., 30 g/meal; 0.4 g/kg/meal) optimally stimulate muscle protein synthesis in older adults [
29,
30]. When muscle protein synthesis overcomes muscle protein breakdown, it leads to positive muscle protein balance, and therefore, protein accretion [
31], which translates into muscle mass maintenance or increase if resistance exercise is performed [
54]. Due to low muscle mass is significantly associated with weakness [
5] and reduced lower limb functionality [
55], the association of adequate protein intake per meal with physical disability may be mediated by its role over muscle mass [
36]. Therefore, prospective studies should investigate if consuming protein above these thresholds are linked with the incidence of physical disability and its association with muscle mass.
The association between protein intake and lower physical disability risk may also be mediated by its role in decreasing body fat [
26,
51,
56]. As we get older, there is an increase in body fat and fat infiltration into the muscle [
57], which leads to decreased muscle quality, strength, and functionality [
6,
24,
58,
59]. Additionally, the lower body fat showed with high protein intake in comparison with lower protein intake [
26,
51], would lead to lessening the pro-inflammatory state observed in subjects with high body fat [
60], which also has been reported to mediate the association between muscle strength decline and protein intake in older adults [
61]. However, we did not evaluate body composition in this study. Further research should address the interaction between protein intake per meal and body composition and their association with physical disability.
These results could be helpful for the assessment of protein intake per meal in older adults, looking for those who eat less than two meals with ≥30 g or ≥0.4 g/kg as a risk factor before physical disability occurs. However, the interaction of protein intake doses with other variables, as total protein intake [
23,
24,
25,
26], physical activity level [
16,
17,
18,
19], and participation in exercise programs [
19,
20,
21] should also be monitored in the clinical practice as risk factors.
Even though the number of meals with an adequate protein intake was a significant risk factor for physical disability (
Figure 1 and
Figure 2), its contribution to the model was low (3.1% to 6.9%), which could be attributable to other dietary and non-dietary factors associated with muscle mass, strength, and functionality in older adults [
62,
63]. Therefore, it should be considered as a significant but complementary factor when assessing proper functionality in this population. Conversely, age was the most important predictor for physical disability in this study (8% to 29.3%) in accordance with previous studies that describe the age-related decrease in muscle mass, strength, and functionality [
4,
10,
64,
65]. Hence, the role of proper dietary protein intake in older adults is, apparently, to mitigate these age-related declines [
48,
49,
50].
It is interesting to note that adequate protein intake per meal was associated with physical disability for ambulatory items (i.e., Shopping and Transportation) in IADL, while it did not predict disability for other more cognitive-related items (
Figure 1a and
Figure 2a). Possibly because the role of protein over cognition is weaker than with muscle mass and physical functioning [
66]. However, for ADL, Transfer was the only ambulatory item associated with adequate protein intake, and Feeding (a more cognitive-related item) was also significantly associated with adequate protein intake (
Figure 1b). These differences might be attributable to how disability was considered for each questionnaire, where IADL accepts some degree of difficulty in performing daily living activities and still considers the subject is functional [
41], but for ADL, the subject has to report no difficulty to be deemed functional [
42].
When we analyzed the dietary protein intake, we observed that most of the protein was ingested at lunch, independently of the group or the adequate protein intake criteria (
Table 3 and
Table 5) which is similar to previous studies in older adults from Mexico [
67], Germany [
38], and France [
68]. However, reports in other countries suggest that most of the daily protein is consumed at dinner [
36,
50,
69,
70,
71]. Despite these country-specific differences, it is unlikely that these differences in the timing of protein intake modulate the association between the number of meals with adequate protein intake and disability. For example, Loenneke et al. [
36] reported the number of meals with adequate protein intake was significantly related with strength and lean mass in American older adults (higher protein intake at dinner), while a similar result was observed here in Mexican population (higher protein intake at lunch). Nonetheless, Loenneke et al. [
36] reported that 32.3% of their sample did not reach the recommended 30 g protein for any meal, and 51.8% did it for only one. In this study, we reported that 61.0% of our sample did not reach this threshold at any meal, and 34.2% did it for one only. These data let us believe that Mexican older adults would be at higher risk of presenting lower lean mass, muscle strength, and a higher risk of physical disability than that observed in American population.
There is evidence suggesting an even protein distribution throughout the day is beneficial to stimulate muscle protein synthesis optimally [
72], and the protein CV has been proposed as an indicator for evaluating protein intake evenness, the lower the CV, the evener the distribution [
46]. However, we observed that the CV reported in 0M and +2M groups was similar, and a higher IPI was detected in the former group for both criteria (
Table 3 and
Table 5). Therefore, we believe this indicator should not be used alone, as there could be an even protein distribution, but daily and per-meal protein intake might not be adequate.
We previously published data about subjects participating in the same project [
37]. However, it is essential to highlight the differences between our earlier published work and the current study. While we formerly analyzed the association of timing of inadequate protein intake and functionality, we here reported that the accumulated inadequate protein intake per meal, independently of the timing, is also associated with physical disability (
Figure 1 and
Figure 2). Similarly, this study expands our knowledge about protein intake in Mexican older adults as we reported the dietary protein intake patterns depending on the number of meals with an adequate protein content (
Table 3 and
Table 5).
Although this study provides important information for the literature, some limitations must be acknowledged. Firstly, the cross-sectional design allows us to infer association between the variables, but not causality. Secondly, our data were collected by participants self-reporting over a 24 h period only and with questionnaires, which is known to lead to inaccurate data [
45,
73,
74]. However, we followed standardized protocols and administrated validated tools to decrease this issue as possible [
41,
42,
45]. Further efforts should be addressed to corroborate our results using more reliable and objective assessment methods.
Thirdly, our sample size was small, especially for the +2M group with the ≥30 g protein/meal criterion, where only nine participants composed this group (
Table 2). This small number of participants poorly represented a portion of this population and affected the statistical analysis, which is reflected in very low odds ratios and wide confidence intervals from the logistic regression (
Figure 1 and
Figure 2). However, it is possible that the low proportion of participants eating adequate amounts of protein (≥30 g) for two or more meals would be similar in other samples of Mexican older adults (≈5%). Therefore, a bigger sample size must be warranted to overcome this limitation. Similarly, there were a higher number of women than men; therefore, despite the models were adjusted by sex, these results might not be representative of men. Also, our sample was recruited from a clinical setting (a regional hospital) from the west of Mexico, and might not be representative of Mexican older adults that do not attend to a medical service (due to healthier status, or inaccessibility to public healthcare) and from other geographical regions. Thus, caution must be considered when translating these results to other populations.
It is also important to highlight that despite non-included and included participants showed similar demographic characteristics (
Table 1), the information about the physical disability of those unable to answer to questionnaires is lacking. Similarly, we do not know if the cognitive status could explain the inability of non-included participants to provide detailed dietary information and to answer questionnaires, as we did not measure it. Further studies should evaluate the cognitive status and use objective measures of functionality to overcome these limitations. Finally, the covariables used to adjust the models were not as varied as reported in other studies with “fully adjusted” models. However, we adjusted for basic covariables observed in most studies [
23,
36,
48,
49,
51,
52].

 ,
, 
{kind=link}
{kind=link}

