Social Prescribing Programmes to Prevent or Delay Frailty in Community-Dwelling Older Adults

 ,
,  ,
, {kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
- Any physical activity programmes such as: exercise, dance, gym-based activities, guided or health walks, swimming or aqua therapy, team sports and cycling.
- Any nutrition intervention including but not limited to: diet clubs, food clubs, cooking clubs, cooking courses, lunch clubs, weight management and diet therapy.
- Psychosocial support such as: social support groups, psychoeducation, physical activity, peer-support groups, befriending, day clubs and social skill training.
2.3. Study Identification
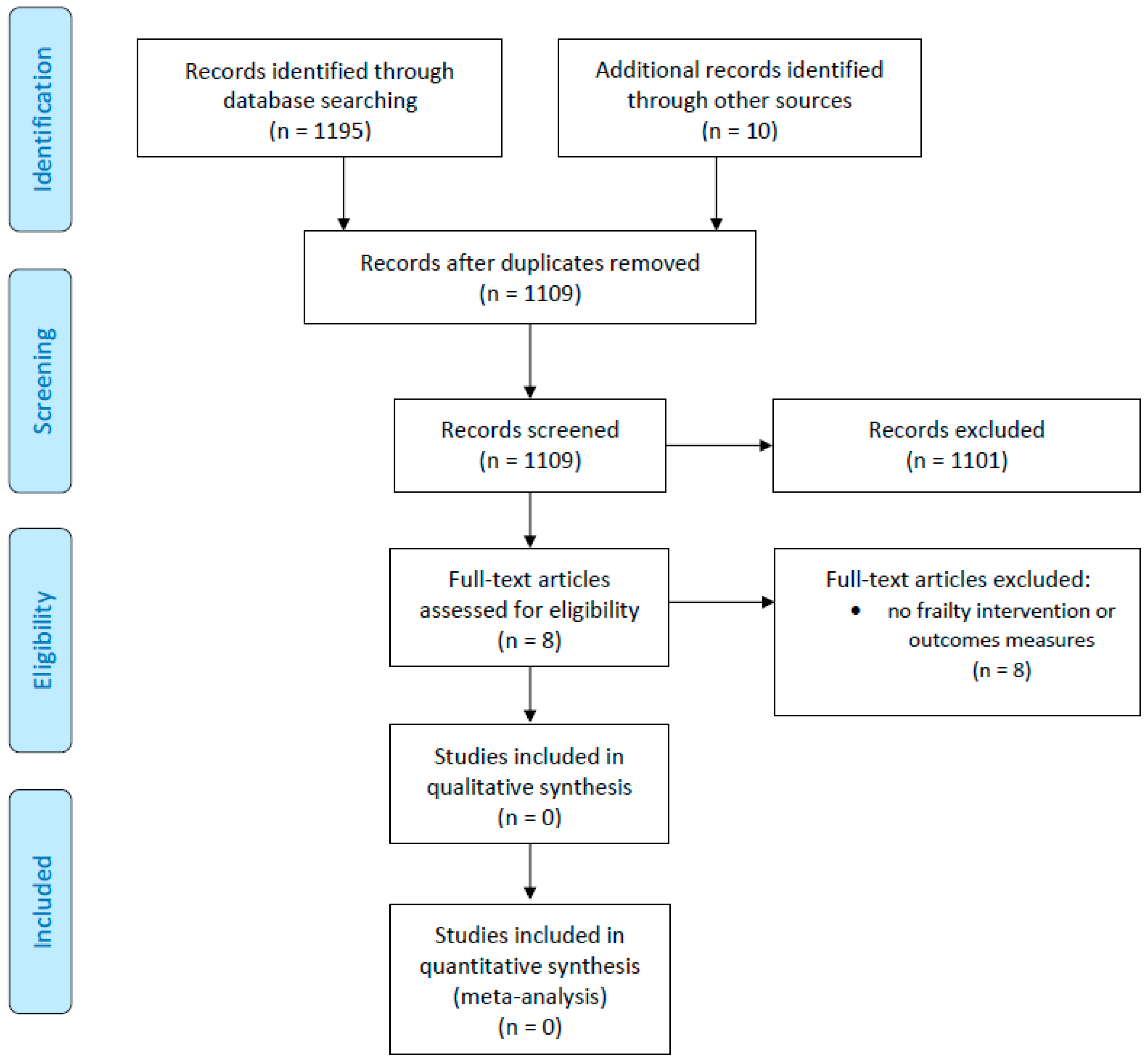
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Han, L.; Clegg, A.; Doran, T.; Fraser, L. The impact of frailty on healthcare resource use: A longitudinal analysis using the Clinical Practice Research Datalink in England. Age Ageing 2019, 48, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Luger, E.; Dorner, T.E.; Haider, S.; Kapan, A.; Lackinger, C.; Schindler, K. Effects of a home-based and volunteer-administered physical training, nutritional, and social support program on malnutrition and frailty in older persons: A randomized controlled trial. J. Am. Med. Dir. Assoc. 2016, 17, 671.e9–671.e16. [Google Scholar] [CrossRef] [PubMed]
- Turner, G.; Clegg, A.; British Geriatrics Society; Age UK; Royal College of General Practitioners. Best practice guidelines for the management of frailty: A British Geriatrics Society, Age UK and Royal College of General Practitioners report. Age Ageing 2014, 43, 744–747. [Google Scholar] [CrossRef] [PubMed]
- Rempel, E.S.; Wilson, E.N.; Durrant, H.; Barnett, J. Preparing the prescription: A review of the aim and measurement of social referral programmes. BMJ Open 2017, 7, e017734. [Google Scholar] [CrossRef] [PubMed]
- Pescheny, J.V.; Pappas, Y.; Randhawa, G. Facilitators and barriers of implementing and delivering social prescribing services: A systematic review. BMC Health Serv. Res. 2018, 18, 86. [Google Scholar] [CrossRef] [PubMed]
- NHS. Social Prescribing. Available online: https://www.england.nhs.uk/personalisedcare/social-prescribing/ (accessed on 13 September 2019).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Bertotti, M.; Frostick, C.; Hutt, P.; Sohanpal, R.; Carnes, D. A realist evaluation of social prescribing: An exploration into the context and mechanisms underpinning a pathway linking primary care with the voluntary sector. Prim. Health Care Res. Dev. 2018, 19, 232–245. [Google Scholar] [CrossRef] [PubMed]
- Bickerdike, L.; Booth, A.; Wilson, P.M.; Farley, K.; Wright, K. Social prescribing: Less rhetoric and more reality. A systematic review of the evidence. BMJ Open 2017, 7, e013384. [Google Scholar] [CrossRef] [PubMed]
- Chaudoir, S.R.; Dugan, A.G.; Barr, C.H. Measuring factors affecting implementation of health innovations: A systematic review of structural, organizational, provider, patient, and innovation level measures. Implement. Sci. 2013, 8, 22. [Google Scholar] [CrossRef] [PubMed]
- Elston, J.; Gradinger, F.; Asthana, S.; Lilley-Woolnough, C.; Wroe, S.; Harman, H.; Byng, R. Does a social prescribing ‘holistic’ link-worker for older people with complex, multi-morbidity improve well-being and frailty and reduce health and social care use and costs? A 12-month before and after evaluation. Prim. Health Care Res. Dev. 2019, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Rogers, N.T.; Steptoe, A.; Cadar, D. Frailty is an independent predictor of incident dementia: Evidence from the English Longitudinal Study of Ageing. Sci. Rep. 2017, 7, 15746. [Google Scholar] [CrossRef] [PubMed] [Green Version]

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, T.O.; Jimoh, O.F.; Cross, J.; Allan, L.; Corbett, A.; Sadler, E.; Khondoker, M.; Whitty, J.; Valderas, J.M.; Fox, C. Social Prescribing Programmes to Prevent or Delay Frailty in Community-Dwelling Older Adults. Geriatrics 2019, 4, 65. https://doi.org/10.3390/geriatrics4040065
Smith TO, Jimoh OF, Cross J, Allan L, Corbett A, Sadler E, Khondoker M, Whitty J, Valderas JM, Fox C. Social Prescribing Programmes to Prevent or Delay Frailty in Community-Dwelling Older Adults. Geriatrics. 2019; 4(4):65. https://doi.org/10.3390/geriatrics4040065
Chicago/Turabian StyleSmith, Toby O, Oluseyi F Jimoh, Jane Cross, Louise Allan, Anne Corbett, Euan Sadler, Mizanur Khondoker, Jennifer Whitty, Jose M Valderas, and Christopher Fox. 2019. "Social Prescribing Programmes to Prevent or Delay Frailty in Community-Dwelling Older Adults" Geriatrics 4, no. 4: 65. https://doi.org/10.3390/geriatrics4040065