Differences in Exposure to Nicotine, Tobacco-Specific Nitrosamines, and Volatile Organic Compounds among Electronic Cigarette Users, Tobacco Smokers, and Dual Users from Three Countries

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedures and Participants
2.2. Questionnaire Measures
2.3. Biomarker Measurements
2.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. Patterns of E-Cigarette Use and Cigarette Smoking across Countries
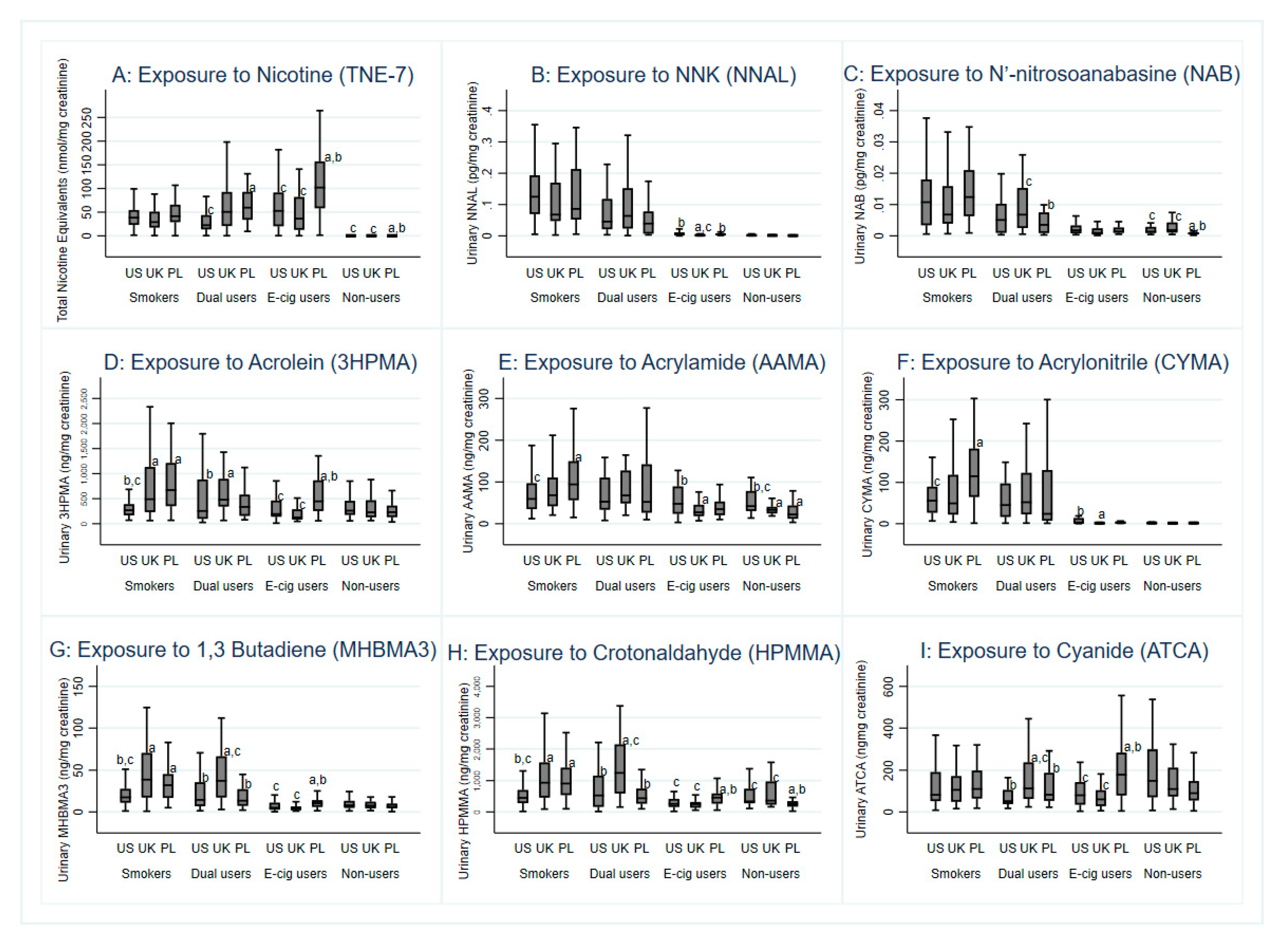
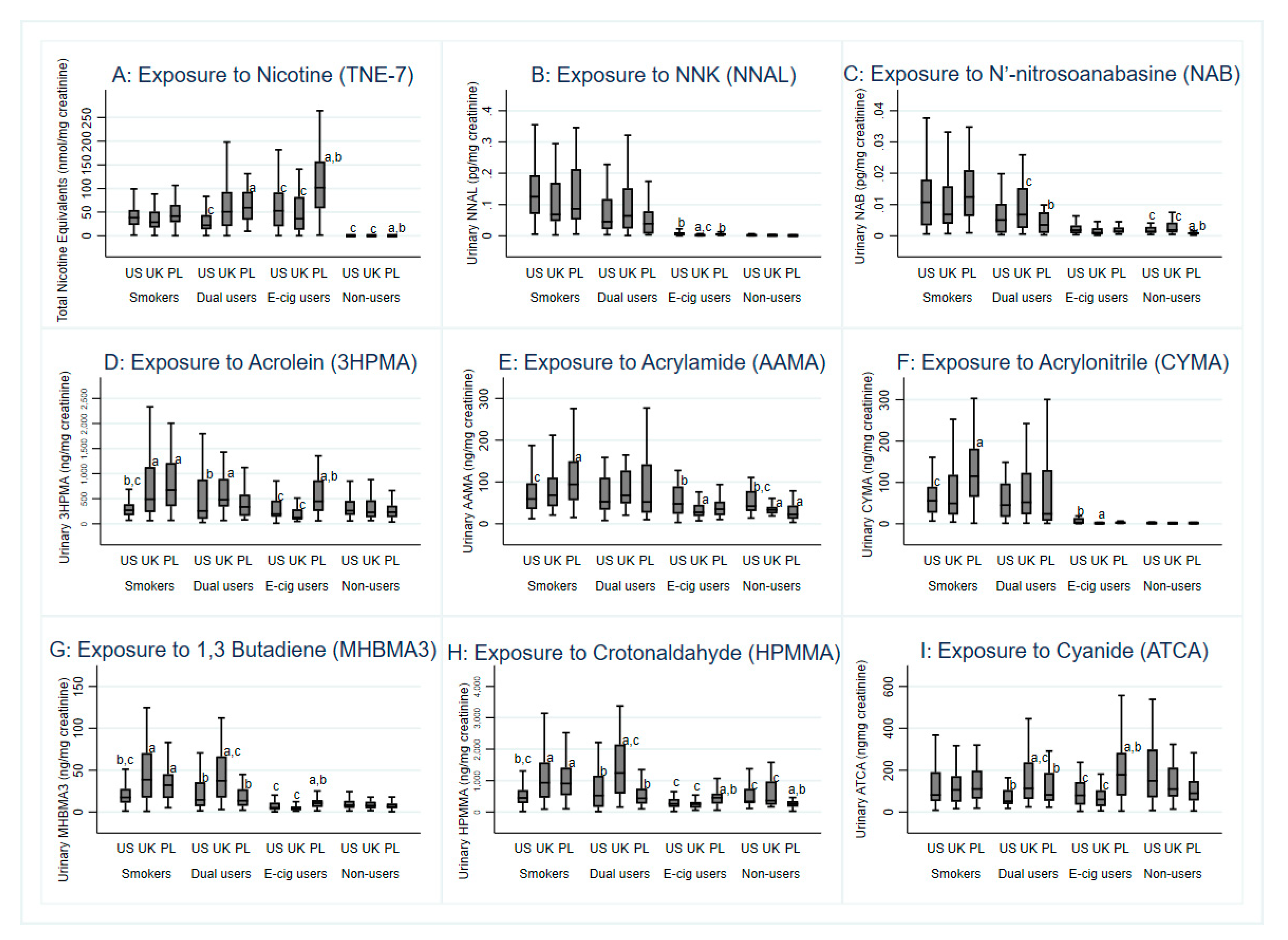
3.3. Nicotine Intake
3.4. Toxicant Exposure
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Academies of Science, Engineering, and Medicine. Public Health Consequences of E-Cigarettes; National Academies Press: Washington, DC, USA, 2018. Available online: https://www.ncbi.nlm.nih.gov/books/NBK507187/ (accessed on 14 August 2018).
- Goniewicz, M.L.; Gawron, M.; Smith, D.M.; Peng, M.; Jacob, P.; Benowitz, N.L. Exposure to Nicotine and Selected Toxicants in Cigarette Smokers Who Switched to Electronic Cigarettes: A Longitudinal Within-Subjects Observational Study. Nicotine Tob. Res. 2017, 19, 160–167. [Google Scholar] [CrossRef] [Green Version]
- Goniewicz, M.L.; Smith, D.M.; Edwards, K.C.; Blount, B.C.; Caldwell, K.L.; Feng, J.; Wang, L.; Christensen, C.; Ambrose, B.; Borek, N.; et al. Comparison of Nicotine and Toxicant Exposure in Users of Electronic Cigarettes and Combustible Cigarettes. JAMA Netw. Open. 2018, 1, e185937. [Google Scholar] [CrossRef] [Green Version]
- Shahab, L.; Goniewicz, M.L.; Blount, B.C.; Brown, J.; McNeill, A.; Alwis, K.U.; Feng, J.; Wang, L.; West, R. Nicotine, Carcinogen, and Toxin Exposure in Long-Term E-Cigarette and Nicotine Replacement Therapy Users: A Cross-sectional Study. Ann. Intern. Med. 2017, 166, 390–400. [Google Scholar] [CrossRef] [Green Version]
- Wagner, K.A.; Flora, J.W.; Melvin, M.S.; Avery, K.C.; Ballentine, R.M.; Brown, A.P.; McKinney, W.J. An evaluation of electronic cigarette formulations and aerosols for harmful and potentially harmful constituents (HPHCs) typically derived from combustion. Regul. Toxicol. Pharmacol. 2018, 95, 153–160. [Google Scholar] [CrossRef]
- Dawkins, L.; Cox, S.; Goniewicz, M.; McRobbie, H.; Kimber, C.; Doig, M.; Kośmider, L. ‘Real-world’ compensatory behaviour with low nicotine concentration e-liquid: Subjective effects and nicotine, acrolein and formaldehyde exposure. Addiction 2018, 113, 1874–1882. [Google Scholar] [CrossRef] [Green Version]
- Smith, D.M.; Christensen, C.; van Bemmel, D.; Borek, N.; Ambrose, B.; Ervies, G.; Niaura, R.; Edwards, K.C.; Stanton, C.; Blount, B.C.; et al. Biomarkers of Exposure Among Dual Users of Tobacco Cigarettes and e-Cigarettes: Findings from the Population Assessment of Tobacco and Health (PATH) Study, Wave 1, 2013–2014. In Proceedings of the Society for Research on Nicotine and Tobacco (SRNT) Annual Meeting, San Francisco, CA, USA, 20–23 February 2019. [Google Scholar]
- O’Connor, R.J.; Fix, B.V.; McNeill, A.; Goniewicz, M.L.; Bansal-Travers, M.; Heckman, B.W.; Cummings, K.M.; Hitchman, S.; Borland, R.; Hammond, D.; et al. Characteristics of nicotine vaping products used by participants in the 2016 ITC Four Country Smoking and Vaping Survey. Addiction 2019, 114 (Suppl. 1), 15–23. [Google Scholar] [CrossRef] [Green Version]
- Goniewicz, M.L.; Kuma, T.; Gawron, M.; Knysak, J.; Kosmider, L. Nicotine Levels in Electronic Cigarettes. Nicotine Tob. Res. 2012, 15, 158–166. [Google Scholar] [CrossRef] [Green Version]
- Kosmider, L.; Jackson, A.; Leigh, N.; O’Connor, R.; Goniewicz, M.L. Circadian Puffing Behavior and Topography among E-cigarette Users. Tob. Regul. Sci. 2018, 4, 41–49. [Google Scholar] [CrossRef]
- Wei, B.; Feng, J.; Rehmani, I.J.; Miller, S.; McGuffey, J.E.; Blount, B.C.; Wang, L. A high-throughput robotic sample preparation system and HPLC-MS/MS for measuring urinary anatabine, anabasine, nicotine and major nicotine metabolites. Clin. Chim. Acta 2014, 436, 290–297. [Google Scholar] [CrossRef] [Green Version]
- Alwis, K.U.; Blount, B.C.; Britt, A.S.; Patel, D.; Ashley, D.L. Simultaneous analysis of 28 urinary VOC metabolites using ultra high performance liquid chromatography coupled with electrospray ionization tandem mass spectrometry (UPLC-ESI/MSMS). Anal. Chim. Acta 2012, 750, 152. [Google Scholar] [CrossRef]
- Xia, B.; Xia, Y.; Wong, J.; Nicodemus, K.J.; Xu, M.; Lee, J.; Guillot, T.; Li, J. Quantitative analysis of five tobacco-specific N-nitrosamines in urine by liquid chromatography-atmospheric pressure ionization tandem mass spectrometry. Biomed. Chromatog. 2014, 28, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, M.L.; Eisner, M.D.; Lazcano-Ponce, E.; Zielinska-Danch, W.; Koszowski, B.; Sobczak, A.; Havel, C.; Jacob, P.; Benowitz, N.L. Comparison of urine cotinine and the tobacco-specific nitrosamine metabolite 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol (NNAL) and their ratio to discriminate active from passive smoking. Nicotine Tob. Res. 2011, 13, 202–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hornung, R.W.; Reed, L.D. Estimation of Average Concentration in the Presence of Nondetectable Values. Appl. Occup. Environ. Hyg. 1990, 5, 46–51. [Google Scholar] [CrossRef]
- Hecht, S.S.; Carmella, S.G.; Kotandeniya, D.; Pillsbury, M.E.; Chen, M.; Ransom, B.W.S.; Vogel, R.I.; Thompson, E.; Murphy, S.E.; Hatsukami, D.K. Evaluation of toxicant and carcinogen metabolites in the urine of e-cigarette users versus cigarette smokers. Nicotine Tob. Res. 2015, 17, 704–709. [Google Scholar] [CrossRef]
- Voos, N.; Kaiser, L.; Mahoney, M.C.; Bradizza, C.M.; Kozlowski, L.T.; Benowitz, N.L.; O’Connor, R.J.; Goniewicz, M.L. Randomized within-subject trial to evaluate smokers’ initial perceptions, subjective effects and nicotine delivery across six vaporized nicotine products. Addiction 2019, 114, 1236–1248. [Google Scholar] [CrossRef]
- Czoli, C.D.; Fong, G.T.; Goniewicz, M.L.; Hammond, D. Biomarkers of exposure among “dual users” of tobacco cigarettes and electronic cigarettes in Canada. Nicotine Tob. Res. 2018. [Google Scholar] [CrossRef]
- Lorkiewicz, P.; Riggs, D.W.; Keith, R.J.; Conklin, D.J.; Xie, Z.; Sutaria, S.; Lynch, B.; Srivastava, S.; Bhatnagar, A. Comparison of Urinary Biomarkers of Exposure in Humans Using Electronic Cigarettes, Combustible Cigarettes, and Smokeless Tobacco. Nicotine Tob. Res. 2018. [Google Scholar] [CrossRef]
- McRobbie, H.; Phillips, A.; Goniewicz, M.L.; Smith, K.M.; Knight-West, O.; Przulj, D.; Hajek, P. Effects of Switching to Electronic Cigarettes with and without Concurrent Smoking on Exposure to Nicotine, Carbon Monoxide, and Acrolein. Cancer Prev. Res. 2015, 8, 873–878. [Google Scholar] [CrossRef] [Green Version]
- Faroon, O.; Roney, N.; Taylor, J.; Ashizawa, A.; Lumpkin, M.H.; Plewak, D.J. Acrolein health effects. Toxicol. Ind. Health 2008, 24, 447–490. [Google Scholar] [CrossRef]
- Henning, R.J.; Johnson, G.T.; Coyle, J.P.; Harbison, R.D. Acrolein Can Cause Cardiovascular Disease: A Review. Cardiovasc. Toxicol. 2017, 17, 227–236. [Google Scholar] [CrossRef]
- Chang, C.M.; Edwards, S.H.; Arab, A.; Del Valle-Pinero, A.Y.; Yang, L.; Hatsukami, D.K. Biomarkers of Tobacco Exposure: Summary of an FDA-Sponsored Public Workshop. Cancer Epidemiol. Biomark. Prev. 2017, 26, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovreglio, P.; Barbieri, A.; Carrieri, M.; Sabatini, L.; Fracasso, M.E.; Doria, D.; Drago, I.; Basso, A.; D’Errico, M.N.; Bartolucci, G.B.; et al. Validity of new biomarkers of internal dose for use in the biological monitoring of occupational and environmental exposure to low concentrations of benzene and toluene. Int. Arch. Occup. Environ. Health 2010, 83, 341–356. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L.; Hukkanen, J.; Jacob, P., 3rd. Nicotine chemistry, metabolism, kinetics and biomarkers. In Nicotine Psychopharmacology; Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |

{kind=link}
| US | UK | Poland | p-value | |
|---|---|---|---|---|
| E-Cigarette-Only Users | n = 48 | n = 36 | n = 40 | |
| Age (years, mean±SD) | 40.5 (14.2) | 38.5 (11.1) | 40.3 (11.8) | 0.740 |
| Sex (% (n)) | ||||
| Male | 60.4 (29) | 80.6 (29) c | 47.5 (19) b | 0.010 |
| Female | 39.6 (19) | 19.4 (7) c | 52.5 (21) b | |
| Ethnicity (% (n)) | ||||
| White | 93.6 (44) | 83.3 (30) c | 100 (40) b | 0.020 |
| Non-White | 6.4 (3) | 16.7 (6) c | 0 b | |
| Education (% (n)) | ||||
| Low | 50.0 (23) | 50.0 (18) | 47.5 (19) | 0.967 |
| High | 50.0 (23) | 50.0 (18) | 52.5 (21) | |
| Type of e-cigarette device used (% (n)) | ||||
| Disposable | 0 (0) | 0 (0) | 0 (0) | <0.001 |
| Replaceable cartridge model | 4.2 (2) | 16.7 (6) | 2.5 (1) | |
| Refillable tank model | 85.4 (41) b | 36.1 (13) a,c | 97.5 (39) b | |
| Other | 10.4 (5) b | 47.2 (17) a,c | 0 (0) b | |
| Nicotine concentration in liquid used (% (n)) | ||||
| No nicotine | 4.2 (2) | 0 (0) | 0 (0) | 0.141 |
| Very low nicotine (1–4mg) | 10.4 (5) | 2.9 (1) | 0 (0) | |
| Low nicotine (6–9 mg) | 25.0 (12) | 20.6 (7) | 22.5 (9) | |
| Medium nicotine (10–15 mg) | 27.1 (13) | 29.4 (10) | 22.5 (9) | |
| High nicotine (16–24 mg) | 27.1 (13) | 47.1 (16) | 45.0 (18) | |
| Very high nicotine (>24 mg) | 6.3 (3) | 0 (0) | 10.0 (4) | |
| Estimated number of puffs per day (mean ± SD) | 183.5 (258.1) c | 120.4 (81.6) | 43.6 (38.4) a | 0.003 |
| Dual Users | n = 28 | n = 36 | n = 31 | |
| Age (years, mean±SD) | 38.6 (15.1) | 39.3 (13.1) | 33.6 (13.2) | 0.198 |
| Sex (% (n)) | ||||
| Male | 53.6 (15) | 69.4 (25) | 41.9 (13) | 0.075 |
| Female | 46.4 (13) | 30.6 (11) | 58.1 (18) | |
| Ethnicity (% (n)) | ||||
| White | 82.1 (23) c | 75.0 (27) c | 100 (31) a,b | 0.014 |
| Non-White | 17.9 (5) c | 25.0 (9) c | 0 (0) a,b | |
| Education (% (n)) | ||||
| Low | 71.4 (20) | 50.0 (18) | 56.7 (17) | 0.219 |
| High | 28.6 (8) | 50.0 (18) | 43.3 (13) | |
| Type of e-cigarette device used (% (n)) | ||||
| Disposable | 3.6 (1) | 19.4 (7) c | 0 (0) b | <0.001 |
| Replaceable cartridge model | 10.7 (3) | 36.1 (13) c | 3.2 (1) b | |
| Refillable tank model | 85.7 (24) b | 30.6 (11) a,c | 96.8 (30) b | |
| Other | 0 (0) | 13.9 (5) | 0 (0) | |
| Nicotine concentration in liquid used (% (n)) | ||||
| No nicotine | 0 (0) | 0 (0) | 0 (0) | 0.797 |
| Very low nicotine (1–4 mg) | 3.6 (1) | 4.3 (1) | 0 (0) | |
| Low nicotine (6–9 mg) | 17.9 (5) | 8.7 (2) | 16.1 (5) | |
| Medium nicotine (10–15 mg) | 37.5 (10) | 26.1 (6) | 41.9 (13) | |
| High nicotine (16–24 mg) | 35.7 (10) | 52.2 (12) | 38.7 (12) | |
| Very high nicotine (>24 mg) | 7.1 (2) | 8.7 (2) | 3.2 (1) | |
| Estimated number of e-cigarette puffs per day (mean ± SD) | 65.9 (125.8) | 79.5 (75.9) | 23.6 (13.2) | 0.053 |
| Reported number of cigarettes smoked per day (mean ± SD) | 9.4 (6.0) | 11.9 (9.6) c | 6.8 (6.8) b | 0.038 |
| Cigarette-Only Smokers | n = 45 | n = 37 | n = 45 | |
| Age (years, mean ± SD) | 50.1 (11.5) b,c | 34.4 (14.0) a,c | 43 (11.9) a,b | <0.001 |
| Sex (% (n)) | ||||
| Male | 48.9 (22) | 56.8 (21) | 40.0 (18) | 0.316 |
| Female | 51.1 (23) | 43.2 (16) | 60.0 (27) | |
| Ethnicity (% (n)) | ||||
| White | 65.9 (29) c | 83.8 (31) c | 100 (45) a,b | <0.001 |
| Non-white | 34.1 (15) c | 16.2 (6) c | 0 (0) a,b | |
| Education (% (n)) | ||||
| Low | 62.8 (27) | 67.6 (25) | 51.1 (23) | 0.286 |
| High | 37.2 (16) | 32.4 (12) | 48.9 (22) | |
| Reported number of cigarettes smoked per day (mean ± SD) | 15.7 (11.4) | 13.9 (9.0) | 16.3 (6.3) | 0.469 |
| Parent Compound | Biomarker | US (n = 48) | UK (n = 36) | Poland (n = 40) | p-Value |
|---|---|---|---|---|---|
| Nicotine Metabolites (ng/mg creatinine) | |||||
| Nicotine | Nicotine Equivalence (nmol/mg) | 35.81 c (24.98–51.33) | 27.36 c (17.85–41.92) | 81.34 a,b (54.47–121.45) | 0.002 |
| trans-3′-Hydroxycotinine (HCTT) | 3239.25 (2208.17–4751.76) | 2334.34 c (1482.06–3676.73) | 7273.45 a,b (4747.35–11143.70) | 0.002 | |
| Cotinine (COTT) | 1710.08 c (1191.35–2454.66) | 1331.44 c (867.38–2043.79) | 3882.26 a,b (2595.98–5805.89) | 0.002 | |
| Nicotine (NICT) | 457.22 c (316.74–659.98) | 422.20 c (273.22–652.41) | 1205.23 a,b (800.89–1813.69) | 0.001 | |
| Cotinine N-oxide (COXT) | 214.18 c (147.90–310.15) | 150.78 c (97.20–233.87) | 459.79 a,b (304.46–694.37) | 0.002 | |
| Nicotine 1′-oxide (NOXT) | 430.34 c (289.21–640.33) | 403.70 c (252.01–646.69) | 1209.91 a,b (777.28–1883.36) | 0.001 | |
| Norcotinine (NCTT) | 48.70 c (34.46–68.83) | 29.64 c (19.66–44.67) | 94.29 a,b (64.14–138.59) | 0.001 | |
| Nornicotine (NNCT) | 27.57 c (20.56–36.98) | 18.10 c (12.78–25.63) | 67.00 a,b (48.32–92.89) | <0.001 | |
| Minor Tobacco Alkaloids (ng/mg creatinine) | |||||
| Anabasine (ANBT) | Anabasine (ANBT) | 1.33 c (0.93–1.89) | 1.08 c (0.71–1.63) | 4.66 a,b (3.15–6.87) | <0.001 |
| Anatabine (ANTT) | Anatabine (ANTT) | 0.76 c (0.49–1.15) | 0.81 c (0.48–1.34) | 2.46 a,b (1.53–3.94) | 0.001 |
| Tobacco-Specific Nitrosamines (TSNAs) (pg/mg creatinine) | |||||
| 4-methylnitrosamino)-4-(3-pyridyl)-1-butanone (NNK) | 4-methylnitrosamino)-4-(3-pyridyl)-1-butanol (NNAL) | 5.14 b (3.63–7.26) | 1.74 a,c (1.15–2.62) | 4.82 b (3.26–7.12) | <0.001 |
| N’-nitrosoanabasine (NAB) | N’-nitrosoanabasine (NAB) |
1.7 (1.35–2.26) |
1.17 (0.85–1.58) |
1.55 (1.16–2.08) | 0.157 |
| N’-nitrosoanatabine (NAT) | N’-nitrosoanatabine (NAT) |
3.50 (2.65–4.63) |
2.97 2.14–4.13) |
4.43 (3.24–6.06) | 0.257 |
| Volatile Organic Compounds (VOCs) (ng/mg creatinine) | |||||
| Acrolein | N-Acetyl-S-(3-hydroxypropyl)-L-cysteine (3HPMA) | 218.91 c (171.19–279.91) | 169.18 c (126.40–226.42) | 436.59 a,b (332.04–574.05) | <0.001 |
| N-Acetyl-S-(2-carboxyethyl)-L-cysteine (CEMA) | 79.04 c (62.68–99.68) | 53.45 c (40.59–70.37) | 156.82 a,b (121.11–203.04) | <0.001 | |
| Acrylamide | N-Acetyl-S-(2-carbamoylethyl)-L-cysteine (AAMA) | 47.49 b (37.08–60.81) | 27.33 a (20.38–36.64) | 38.46 (29.20–50.65) | 0.026 |
| N-Acetyl-S-(2-carbamoyl-2-hydroxyethyl)-L-cysteine (GAMA) | 15.17 b,c (12.08–19.04) | 9.52 a (7.27–12.46) | 9.62 a (7.46–12.38) | 0.012 | |
| Acrylonitrile | N-Acetyl-S-(2-cyanoethyl)-L-cysteine (CYMA) | 3.75 b (2.51–5.58) | 1.38 a (0.85–2.21) | 2.90 (1.86–4.52) | 0.009 |
| Benzene | N-Acetyl-S-(phenyl)-L-cysteine (PMA) | 0.77 c (0.61–0.95) | 0.75 (0.57–0.97) | 1.14 a (0.89–1.46) | 0.035 |
| 1,3-Butadiene | N-Acetyl-S-(4-hydroxy-2-buten-1-yl)-L-cysteine (MHBMA3) | 5.22 c (3.97–6.85) | 4.30 c (3.11–5.93) | 10.11 a,b (7.46–13.69) | <0.001 |
| N-Acetyl-S-(3,4-dihydroxybutyl)-L-cysteine (DHBMA) | 206.14 c (170.16–249.72) | 151.88 c (120.99–190.66) | 392.56 a,b (317.08–486.01) | <0.001 | |
| Crotonaldehyde | N-Acetyl-S-(3-hydroxypropyl-1-methyl)-L-cysteine (HPMMA) | 251.95 c (203.88–311.34) | 227.82 c (177.26–292.81) | 421.77 a,b (333.21–533.85) | 0.002 |
| Cyanide | 2-Aminothiazoline-4-carboxylic acid (ATCA) | 67.46 c (50.60–89.92) | 66.54 c (47.32–93.56) | 121.85 a,b (88.48–167.81) | 0.017 |
| N,N-Dimethylformamide; methyl isocyanate | N-Acetyl-S-(N-methylcarbamoyl)-L-cysteine (AMCC) | 160.50 b (128.50–200.45) | 61.50 a,c (47.24–80.04) | 224.10 b (174.96–287.03) | <0.001 |
| Ethylene oxide; acrylonitrile; vinyl chloride | N-Acetyl-S-(2-hydroxyethyl)-L-cysteine (HEMA) *** |
0.55 (0.44–0.69) |
0.44 (0.33–0.57) |
0.50 (0.39–0.64) | 0.442 |
| Propylene oxide | N-Acetyl-S-(2-hydroxypropyl)-L-cysteine (2HPMA) |
39.34 (30.11–51.41) |
31.51 (22.94–43.26) |
40.75 (30.25–54.89) | 0.491 |
| Styrene | Mandelic acid (MA) |
98.37 (79.67–121.45) |
102.37 (79.73–131.43) |
134.56 (106.41–170.15) | 0.144 |
| Styrene; ethylbenzene | Phenylglyoxylic acid (PGA) | 100.57 c (79.01–128.01) | 72.03 c (54.11–95.88) | 160.44 a,b (122.64–209.88) | 0.001 |
| Toluene; benzyl alcohol | N-Acetyl-S-(benzyl)-L-cysteine (BMA) |
4.14 (3.18–5.36) |
4.84 (3.55–6.61) |
5.78 (4.31–7.74) | 0.266 |
| Xylene | 2-Methylhippuric acid (2MHA) |
17.66 (13.49–23.11) |
10.75 (7.81–14.78) |
16.73 (12.40–22.58) | 0.063 |
| 3- + 4-Methylhippuric acids (34MHA) | 134.38 b (103.81–173.94) | 50.29 a,c (37.03–68.29) | 97.28 b (72.98–129.66) | <0.001 | |
| Parent Compound | Biomarker | US (n = 28) | UK (n = 36) | Poland (n = 31) | p-Value |
|---|---|---|---|---|---|
| Nicotine Metabolites (ng/mg Creatinine) | |||||
| Nicotine | Nicotine Equivalence (nmol/mg) | 22.36 c (14.13–35.37) | 32.07 (21.04–48.89) | 53.83 a (33.85–85.56) | 0.045 |
| trans-3′-Hydroxycotinine (HCTT) | 2049.55 (1248.36–3364.91) | 2163.15 (1371.44–3411.88) | 4584.93 (2776.80–7570.42) | 0.068 | |
| Cotinine (COTT) | 967.48 c (597.39–1566.82) | 1485.78 (953.90–2314.22) | 2659.48 a (1633.10–4330.89) | 0.025 | |
| Nicotine (NICT) | 272.30 b,c (163.90–452.37) | 661.17 a (414.65–1054.23) | 753.84 a (451.13–1259.68) | 0.014 | |
| Cotinine N-oxide (COXT) | 144.81 (90.74–231.09) | 155.62 (101.27–239.14) | 286.30 (178.44–459.33) | 0.121 | |
| Nicotine 1′-oxide (NOXT) | 253.11 c (145.89–439.11) | 617.51 (372.15–1024.62) | 781.42 a (447.58–1364.25) | 0.017 | |
| Norcotinine (NCTT) | 32.57 (20.51–51.71) | 46.78 (30.58–71.55) | 69.68 (43.64–111.23) | 0.099 | |
| Nornicotine (NNCT) | 20.96 c (13.98–31.43) | 34.17 (23.55–49.58) | 51.26 a (34.03–77.21) | 0.016 | |
| Minor Tobacco Alkaloids (ng/mg creatinine) | |||||
| Anabasine (ANBT) | Anabasine (ANBT) | 2.12 (1.33–3.35) | 4.27 (2.79–6.52) | 2.86 (1.79–4.56) | 0.105 |
| Anatabine (ANTT) | Anatabine (ANTT) | 2.66 (1.54–4.56) | 5.90 (3.59-9.69) | 2.42 (1.40-4.18) | 0.051 |
| Tobacco-Specific Nitrosamines (TSNAs) (pg/mg creatinine) | |||||
| 4-methylnitrosamino)-4-(3-pyridyl)-1-butanone (NNK) | 4-methylnitrosamino)-4-(3-pyridyl)-1-butanol (NNAL) | 47.39 (30.00–74.85) | 55.80 (36.65–84.94) | 30.99 (19.51–49.20) | 0.227 |
| N’-nitrosoanabasine (NAB) | N’-nitrosoanabasine (NAB) | 3.72 (2.36–5.85) | 6.59 c (4.33–10.00) | 2.52 b (1.59–3.99) | 0.021 |
| N’-nitrosoanatabine (NAT) | N’-nitrosoanatabine (NAT) | 14.53 (8.54–24.72) | 29.53 c (18.11–48.13) | 11.04 b (6.45–18.91) | 0.040 |
| Volatile Organic Compounds (VOCs) (ng/mg creatinine) | |||||
| Acrolein | N-Acetyl-S-(3-hydroxypropyl)-L-cysteine (3HPMA) | 285.36 b (197.79–411.67) | 574.63 a (410.29–804.78) | 341.92 (236.01–495.35) | 0.025 |
| N-Acetyl-S-(2-carboxyethyl)-L-cysteine (CEMA) | 87.25 (63.61–119.66) | 141.75 (106.02–189.51) | 130.57 (94.85-179.73) | 0.079 | |
| Acrylamide | N-Acetyl-S-(2-carbamoylethyl)-L-cysteine (AAMA) | 57.08 (41.69–78.13) | 85.33 (63.93–113.88) | 51.96 (37.81–71.39) | 0.079 |
| N-Acetyl-S-(2-carbamoyl-2-hydroxyethyl)-L-cysteine (GAMA) | 16.62 (12.56–21.99) | 26.02 c (20.11–33.66) | 12.93 b (9.74–17.17) | 0.004 | |
| Acrylonitrile | N-Acetyl-S-(2-cyanoethyl)-L-cysteine (CYMA) | 36.35 (21.84–60.48) | 51.38 (32.17–82.05) | 24.93 (14.89-41.73) | 0.176 |
| Benzene | N-Acetyl-S-(phenyl)-L-cysteine (PMA) | 0.55 b (0.42–0.73) | 1.48 a,c (1.15–1.89) | 0.80 b (0.60–1.05) | <0.001 |
| 1,3-Butadiene | N-Acetyl-S-(4-hydroxy-2-buten-1-yl)-L-cysteine (MHBMA3) | 15.31 b (10.23–22.89) | 35.20 a,c (24.31–50.96) | 15.14 b (10.07–22.74) | 0.006 |
| N-Acetyl-S-(3,4-dihydroxybutyl)-L-cysteine (DHBMA) | 165.84 b,c (128.5–214.02) | 298.47 a (236.09–377.31) | 271.85 a (210.04–351.86) | 0.004 | |
| Crotonaldehyde | N-Acetyl-S-(3-hydroxypropyl-1-methyl)-L-cysteine (HPMMA) | 464.34 b (318.75–676.42) | 1211.53 a,c (857.35–1712.01) | 443.66 b (303.24–649.09) | 0.004 |
| Cyanide | 2-Aminothiazoline-4-carboxylic acid (ATCA) | 57.43 b (43.73–75.42) | 144.93 a,c (112.82–186.18) | 81.21 b (61.65–106.98) | <0.001 |
| N,N-Dimethylformamide; methyl isocyanate | N-Acetyl-S-(N-methylcarbamoyl)-L-cysteine (AMCC) | 166.42 (122.04–226.93) | 177.78 (133.68–236.42) | 219.07 (160.08–299.79) | 0.486 |
| Ethylene oxide; acrylonitrile; vinyl chloride | N-Acetyl-S-(2-hydroxyethyl)-L-cysteine (HEMA) *** | 0.85 (0.58–1.23) | 1.18 (0.83–1.66) | 0.79 (0.54–1.16) | 0.302 |
| Propylene oxide | N-Acetyl-S-(2-hydroxypropyl)-L-cysteine (2HPMA) | 45.65 (32.66–63.78) | 69.28 (50.94–94.22) | 44.38 (31.64–62.25) | 0.128 |
| Styrene | Mandelic acid (MA) | 129.37 b (97.75–171.21) | 228.04 a (176.26–295.02) | 157.62 (118.72–209.27) | 0.019 |
| Styrene, ethylbenzene | Phenylglyoxylic acid (PGA) | 100.85 (71.14–142.97) | 128.60 (93.31–177.24) | 124.89 (87.74–177.75) | 0.575 |
| Toluene; benzyl alcohol | N-Acetyl-S-(benzyl)-L-cysteine (BMA) | 2.75 b,c (1.97–3.82) | 6.22 a (4.59–8.43) | 5.11 a (3.65–7.13) | 0.002 |
| Xylene | 2-Methylhippuric acid (2MHA) | 30.77 (21.13–44.79) | 56.78 c (40.20–80.18) | 21.11 b (14.44–30.87) | 0.003 |
| 3- + 4-Methylhippuric acids (34MHA) | 206.80 (141.11–303.06) | 269.53 c (189.69–382.97) | 121.17 b (82.32–178.35) | 0.024 | |
| Parent Compound | Biomarker | USA (n = 45) | UK (n = 37) | Poland (n = 45) | p-Value |
|---|---|---|---|---|---|
| Nicotine Metabolites (ng/mg creatinine) | |||||
| Nicotine | Nicotine Equivalence (nmol/mg) | 27.36 (19.76–37.88) | 30.86 (21.77–43.74) | 38.53 (28.35–52.35) | 0.348 |
| Trans-3′-Hydroxycotinine (HCTT) | 2103.85 (1435.37–3083.66) | 2402.85 (1595.02–3619.83) | 2970.19 (2071.79–4258.16) | 0.465 | |
| Cotinine (COTT) | 1294.10 (930.73–1799.32) | 1451.28 (1019.39–2066.13) | 1678.40 (1230.38–2289.55) | 0.563 | |
| Nicotine (NICT) | 236.74 c (174.07–399.59) | 433.25 (277.55–676.27) | 678.44 a (458.68–1003.49) | 0.011 | |
| Cotinine n-oxide (COXT) | 159.10 (113.78–222.47) | 165.80 (115.75–237.47) | 199.44 (145.42–273.50) | 0.615 | |
| Nicotine 1′-oxide (NOXT) | 261.05 c (170.01–400.81) | 440.11 (277.95–696.85) | 655.24 a (437.48–981.39) | 0.018 | |
| Norcotinine (NCTT) | 42.25 (31.02–57.54) | 45.79 (32.88–63.75) | 53.72 (40.16–71.86) | 0.558 | |
| Nornicotine (NNCT) | 25.00 c (18.34–34.08) | 30.03 (21.54–41.86) | 47.62 a (35.56–63.75) | 0.015 | |
| Minor Tobacco Alkaloids (ng/mg creatinine) | |||||
| Anabasine (ANBT) | Anabasine (ANBT) | 2.95 (2.16–4.01) | 3.78 (2.71–5.25) | 4.78 (3.57–6.36) | 0.110 |
| Anatabine (ANTT) | Anatabine (ANTT) | 2.97 c (2.08–4.23) | 5.71 (3.90–8.34) | 6.62 a (4.74–9.23) | 0.009 |
| Tobacco-Specific Nitrosamines (TSNAs) (pg/mg creatinine) | |||||
| 4-methylnitrosamino)-4-(3-pyridyl)-1-butanone (NNK) | 4-methylnitrosamino)-4-(3-pyridyl)-1-butanol (NNAL) | 87.78 (66.94–115.08) | 94.38 (70.60–126.18) | 85.12 (65.95–109.87) | 0.878 |
| N’-nitrosoanabasine (NAB) | N’-nitrosoanabasine (NAB) | 8.38 (6.16–11.41) | 8.15 (5.86–11.34) | 8.94 (6.68–11.95) | 0.916 |
| N’-nitrosoanatabine (NAT) | N’-nitrosoanatabine (NAT) | 26.57 (18.46–38.24) | 38.73 (26.22–57.23) | 46.29 (32.84–65.23) | 0.124 |
| Volatile Organic Compounds (VOCs) (ng/mg creatinine) | |||||
| Acrolein | N-Acetyl-S-(3-hydroxypropyl)-L-cysteine (3HPMA) | 241.90 b,c (186.56–313.65) | 602.98 a (456.46–796.52) | 584.57 a (457.67–746.64) | <0.001 |
| N-Acetyl-S-(2-carboxyethyl)-L-cysteine (CEMA) | 90.03 b,c (71.77–112.92) | 160.03 a (125.53–204.02) | 154.84 a (125.07–191.68) | 0.002 | |
| Acrylamide | N-Acetyl-S-(2-carbamoylethyl)-L-cysteine (AAMA) | 54.18 c (43.74–67.12) | 79.91 (63.52–100.53) | 88.90 a (72.66–108.78) | 0.008 |
| N-Acetyl-S-(2-carbamoyl-2-hydroxyethyl)-L-cysteine (GAMA) | 19.22 (15.52–23.80) | 22.12 (17.59–27.80) | 20.25 (16.55–24.76) | 0.714 | |
| Acrylonitrile | N-Acetyl-S-(2-cyanoethyl)-L-cysteine (CYMA) | 43.66 c (32.55–58.55) | 66.45 (48.51–91.00) | 88.88 a (67.14–117.19) | 0.006 |
| Benzene | N-Acetyl-S-(phenyl)-L-cysteine (PMA) | 0.66 (0.50–0.86) | 0.78 (0.58–1.03) | 0.74 (0.57–0.94) | 0.740 |
| 1,3-Butadiene | N-Acetyl-S-(4-hydroxy-2-buten-1-yl)-L-cysteine (MHBMA3) | 13.50 b,c (9.97–18.28) | 38.70 a (27.96–53.55) | 29.08 a (21.85–38.69) | 0.001 |
| N-Acetyl-S-(3,4-dihydroxybutyl)-L-cysteine (DHBMA) | 163.89 b,c (134.44–199.79) | 250.76 a (202.80–310.05) | 273.71 a (227.12–329.86) | 0.002 | |
| Crotonaldehyde | N-Acetyl-S-(3-hydroxypropyl-1-methyl)-L-cysteine (HPMMA) | 352.03 b,c (265.92–466.04) | 1006.22 a (744.94–1359.13) | 888.93 a (682.47–1157.83) | <0.001 |
| Cyanide | 2-Aminothiazoline-4-carboxylic acid (ATCA) | 83.59 (64.98–107.54) | 112.84 (86.14–147.81) | 102.90 (81.16–130.46) | 0.318 |
| N,N-Dimethylformamide; methyl isocyanate | N-Acetyl-S-(N-methylcarbamoyl)-L-cysteine (AMCC) | 173.99 (136.45–221.85) | 214.47 (165.30–278.28) | 264.52 (210.40–332.56) | 0.070 |
| Ethylene oxide; acrylonitrile; vinyl chloride | N-Acetyl-S-(2-hydroxyethyl)-L-cysteine (HEMA) *** | 0.86 (0.67–1.11) | 1.02 (0.77–1.34) | 1.18 (0.92–1.49) | 0.255 |
| Propylene oxide | N-Acetyl-S-(2-hydroxypropyl)-L-cysteine (2HPMA) | 49.33 (38.21–63.68) | 50.40 (38.33–66.26) | 54.85 (43.12–69.77) | 0.833 |
| Styrene | Mandelic acid (MA) | 125.58 b (102.80–153.40) | 234.14 a,c (188.94–290.15) | 161.59 b (133.82–195.11) | 0.001 |
| Styrene; ethylbenzene | Phenylglyoxylic acid (PGA) | 82.13 c (61.16–110.28) | 110.46 (80.54–151.50) | 153.52 a (116.29–202.65) | 0.018 |
| Toluene; benzyl alcohol | N-Acetyl-S-(benzyl)-L-cysteine (BMA) | 3.88 (2.94–5.11) | 4.59 (3.42–6.18) | 4.73 (3.64–6.13) | 0.599 |
| Xylene | 2-Methylhippuric acid (2MHA) | 37.26 (29.09–47.71) | 53.32 (40.90–69.50) | 35.37 (28.01–44.65) | 0.072 |
| 3- + 4-Methylhippuric acids (34MHA) | 233.85 (174.66–313.08) | 339.90 (248.62–464.69) | 198.75 (150.98–261.63) | 0.052 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, D.M.; Shahab, L.; Blount, B.C.; Gawron, M.; Kosminder, L.; Sobczak, A.; Xia, B.; Sosnoff, C.S.; Goniewicz, M.L. Differences in Exposure to Nicotine, Tobacco-Specific Nitrosamines, and Volatile Organic Compounds among Electronic Cigarette Users, Tobacco Smokers, and Dual Users from Three Countries. Toxics 2020, 8, 88. https://doi.org/10.3390/toxics8040088
Smith DM, Shahab L, Blount BC, Gawron M, Kosminder L, Sobczak A, Xia B, Sosnoff CS, Goniewicz ML. Differences in Exposure to Nicotine, Tobacco-Specific Nitrosamines, and Volatile Organic Compounds among Electronic Cigarette Users, Tobacco Smokers, and Dual Users from Three Countries. Toxics. 2020; 8(4):88. https://doi.org/10.3390/toxics8040088
Chicago/Turabian StyleSmith, Danielle M., Lion Shahab, Benjamin C. Blount, Michal Gawron, Leon Kosminder, Andrzej Sobczak, Baoyun Xia, Connie S. Sosnoff, and Maciej L. Goniewicz. 2020. "Differences in Exposure to Nicotine, Tobacco-Specific Nitrosamines, and Volatile Organic Compounds among Electronic Cigarette Users, Tobacco Smokers, and Dual Users from Three Countries" Toxics 8, no. 4: 88. https://doi.org/10.3390/toxics8040088