





Learning Curve and Comparison of Dynamic Implant Placement Accuracy Using a Navigation System in Young Professionals
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
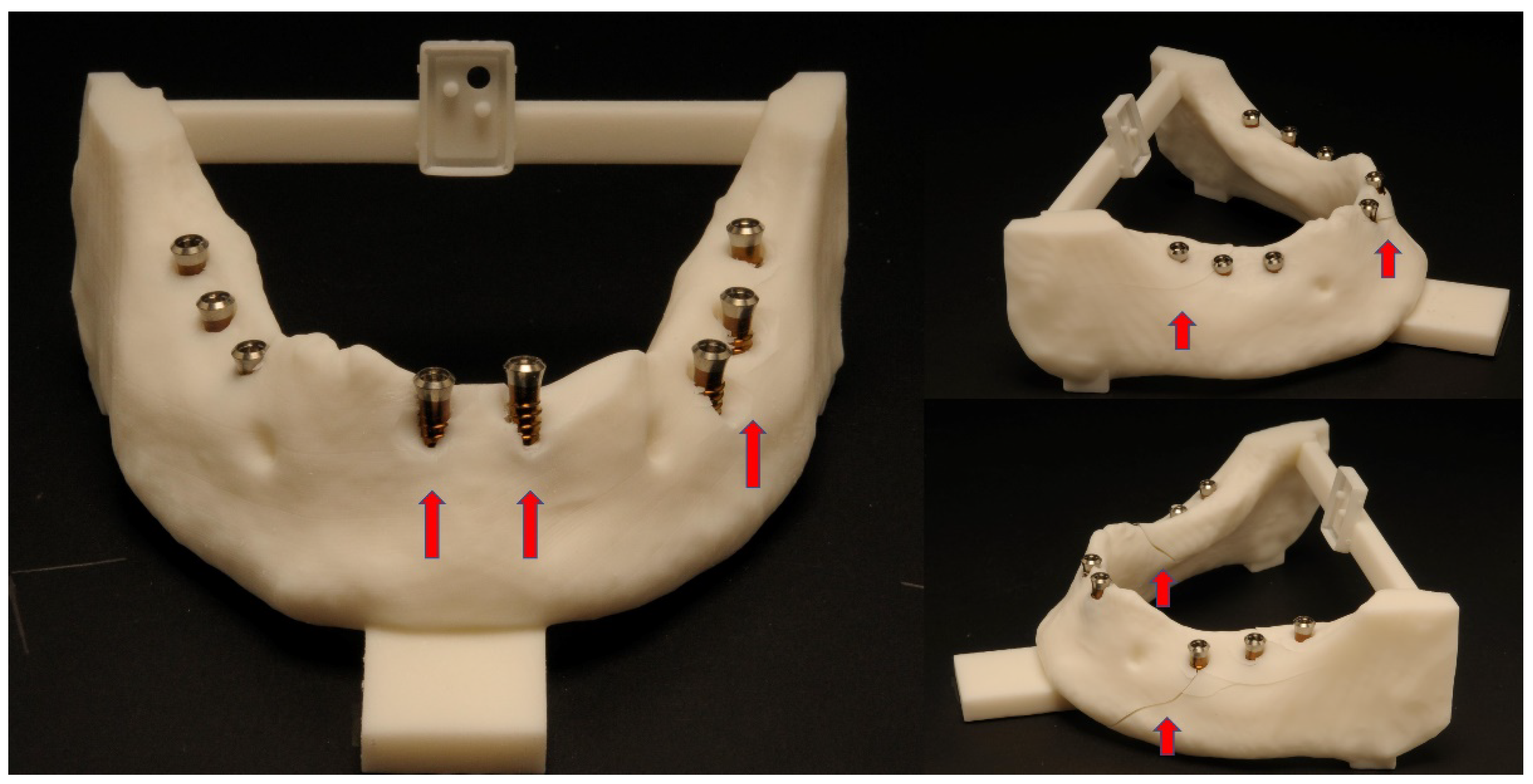
2.2. Surgical Protocol
2.3. Evaluation of the Implant Accuracy
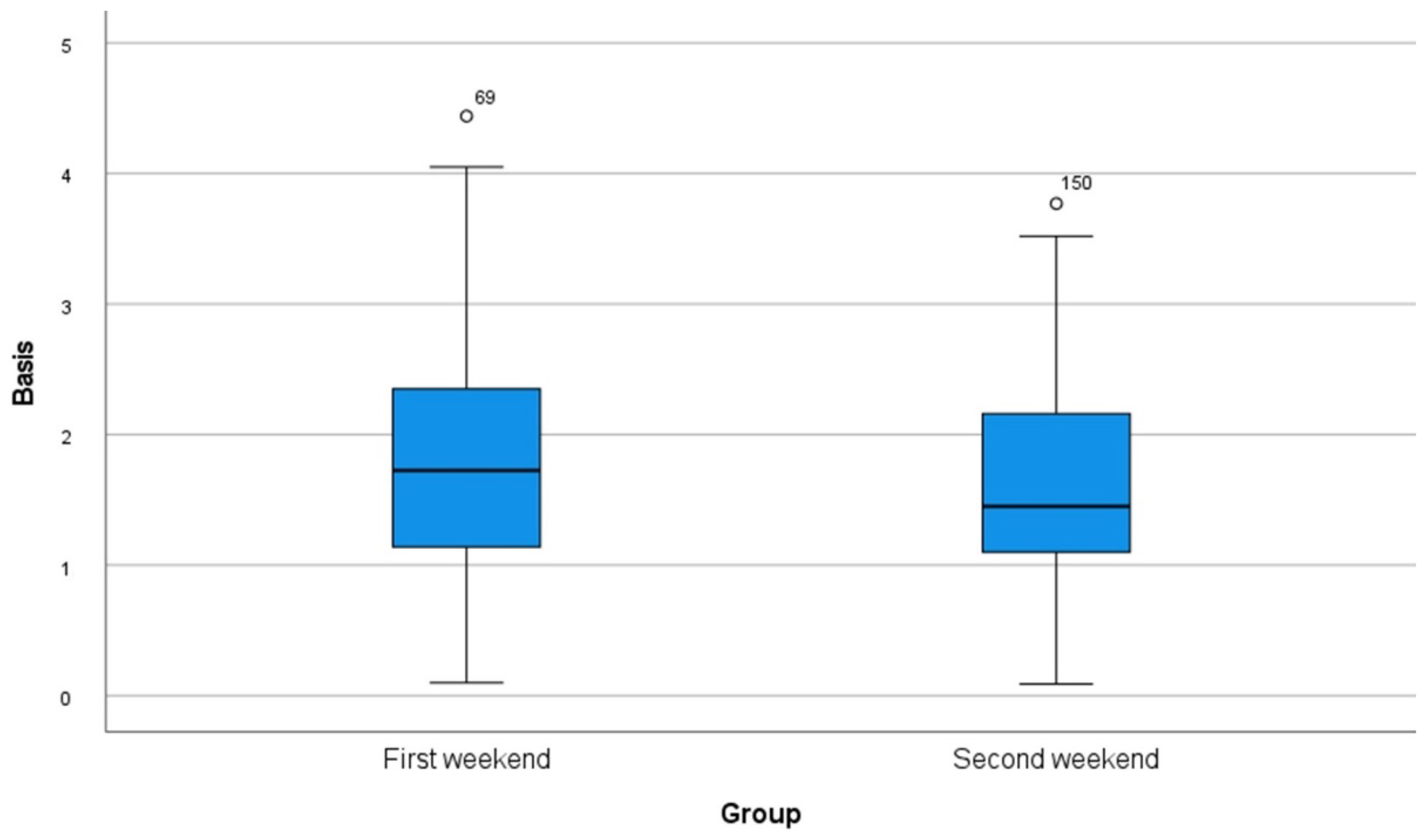
- Total error at the basis/entry point (vestibular, lingual, mesial, distal deviation);
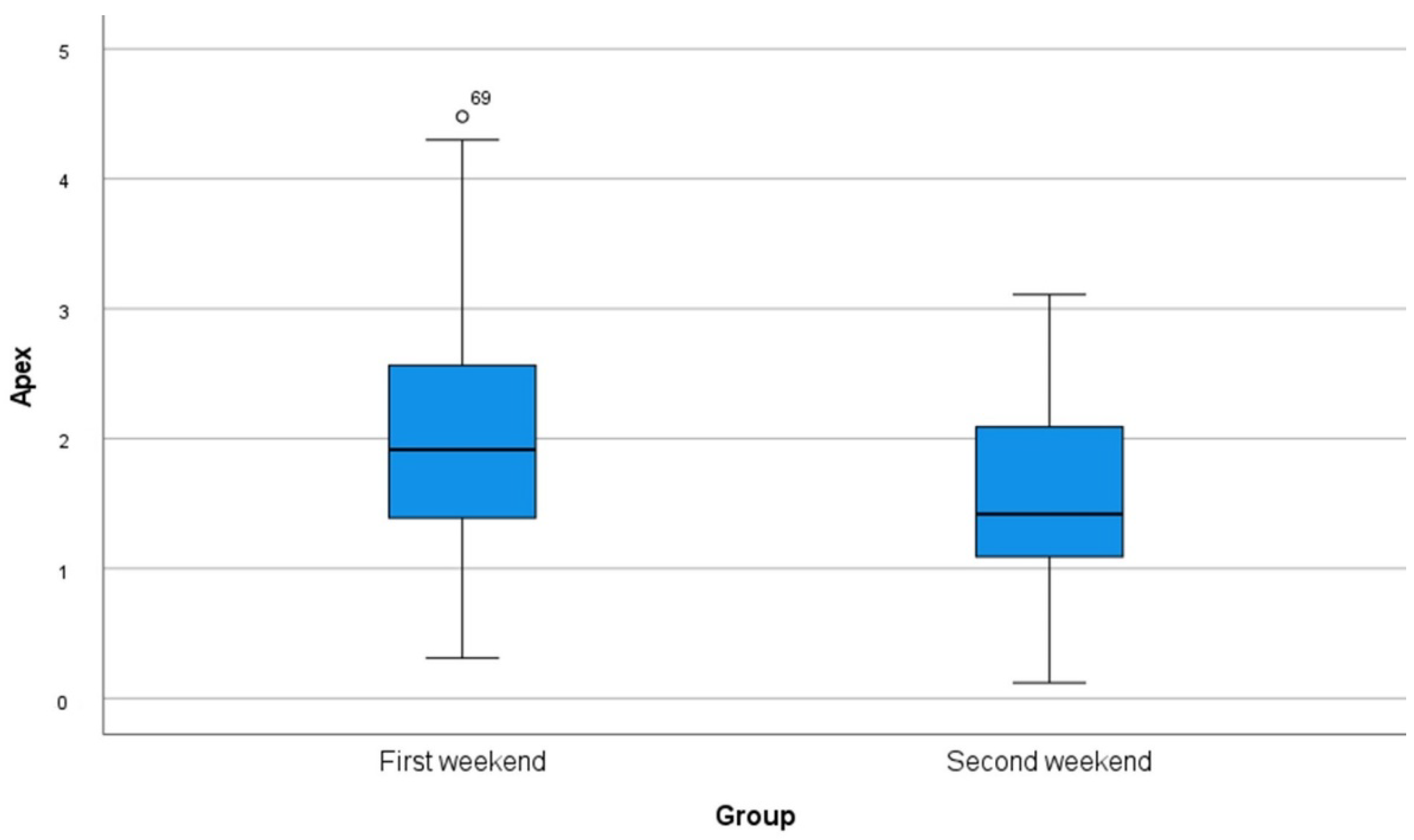
- Total error at the apex (cranial, caudal deviation);
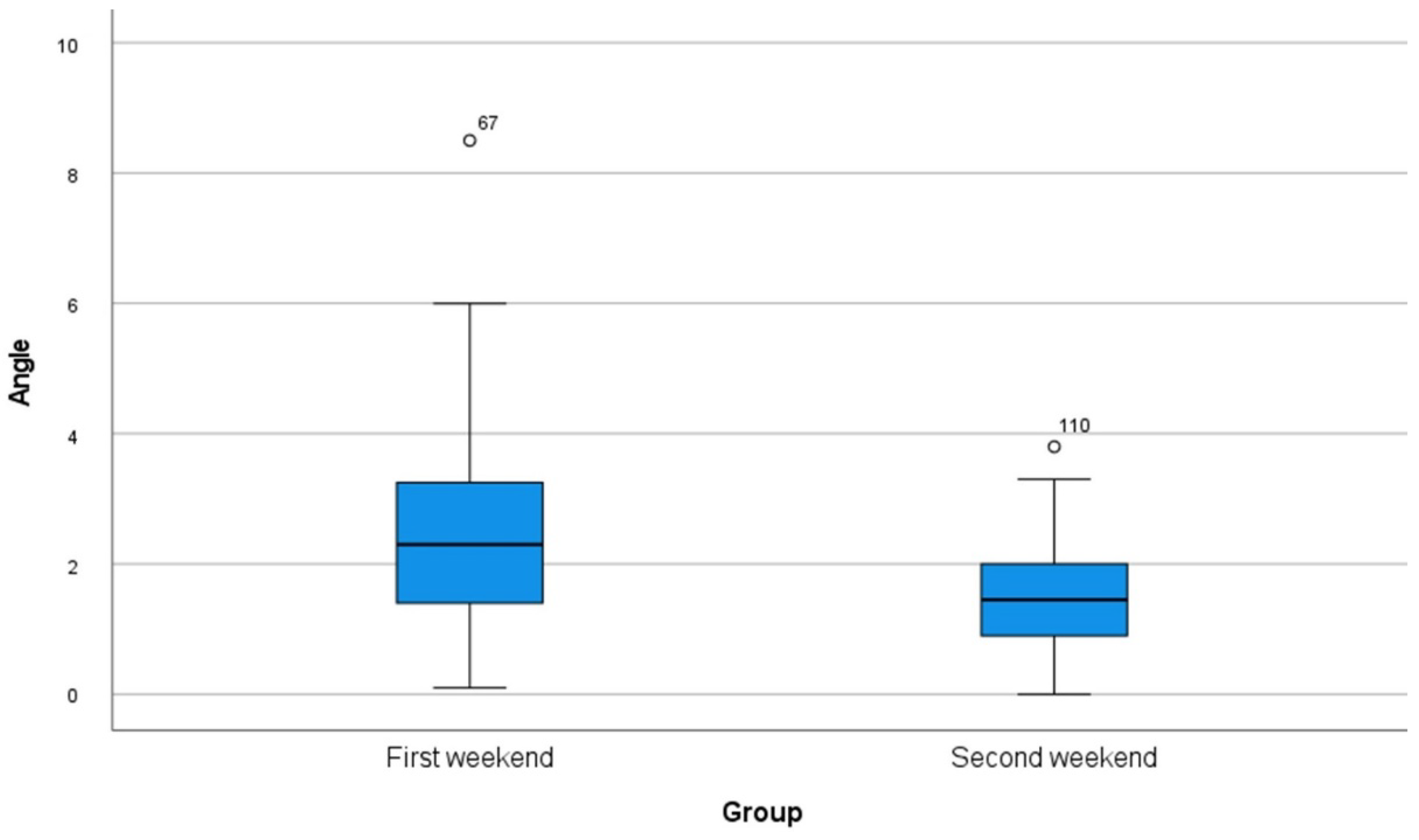
- Angular error.

2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Assche, N.; Vercruyssen, M.; Coucke, W.; Teughels, W.; Jacobs, R.; Quirynen, M. Accuracy of computer-aided implant placement. Clin. Oral Implant. Res. 2012, 23 (Suppl. S6), 112–123. [Google Scholar] [CrossRef] [PubMed]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29 (Suppl. S16), 416–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.W.; Zhao, X.E.; Yan, Q.; Xia, H.B.; Sun, Q. Dynamic navigation system-guided trans-inferior alveolar nerve implant placement in the atrophic posterior mandible: A case report. World J. Clin. Cases 2022, 10, 3907–3915. [Google Scholar] [CrossRef] [PubMed]
- Schnutenhaus, S.; Edelmann, C.; Rudolph, H.; Luthardt, R.G. Retrospective study to determine the accuracy of template-guided implant placement using a novel nonradiologic evaluation method. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, e72–e79. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Tallarico, M.; Radovanovic, S.; Delibasic, B.; Covani, U.; Rakic, M. Distinguishing predictive profiles for patient-based risk assessment and diagnostics of plaque induced, surgically and prosthetically triggered peri-implantitis. Clin. Oral Implant. Res. 2016, 27, 1243–1250. [Google Scholar] [CrossRef]
- Wei, S.M.; Zhu, Y.; Wei, J.X.; Zhang, C.N.; Shi, J.Y.; Lai, H.C. Accuracy of dynamic navigation in implant surgery: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2021, 32, 383–393. [Google Scholar] [CrossRef]
- D’Haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontology 2000 2017, 73, 121–133. [Google Scholar] [CrossRef]
- Kim, S.G.; Lee, W.J.; Lee, S.S.; Heo, M.S.; Huh, K.H.; Choi, S.C.; Kim, T.I.; Yi, W.J. An advanced navigational surgery system for dental implants completed in a single visit: An in vitro study. J. Cranio Maxillofac. Surg. 2015, 43, 117–125. [Google Scholar] [CrossRef]
- Greenstein, G.; Tarnow, D. The mental foramen and nerve: Clinical and anatomical factors related to dental implant placement: A literature review. J. Periodontol. 2006, 77, 1933–1943. [Google Scholar] [CrossRef]
- Gargallo-Albiol, J.; Barootchi, S.; Salomo-Coll, O.; Wang, H.L. Advantages and disadvantages of implant navigation surgery. A systematic review. Ann. Anat. Anat. Anz. 2019, 225, 1–10. [Google Scholar] [CrossRef]
- Spille, J.; Jin, F.; Behrens, E.; Acil, Y.; Lichtenstein, J.; Naujokat, H.; Gulses, A.; Florke, C.; Wiltfang, J. Comparison of implant placement accuracy in two different preoperative digital workflows: Navigated vs. pilot-drill-guided surgery. Int. J. Implant. Dent. 2021, 7, 45. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, A.; Pulijala, Y. The application of virtual reality and augmented reality in Oral & Maxillofacial Surgery. BMC Oral Health 2019, 19, 238. [Google Scholar] [CrossRef] [Green Version]
- Golob Deeb, J.; Bencharit, S.; Carrico, C.K.; Lukic, M.; Hawkins, D.; Rener-Sitar, K.; Deeb, G.R. Exploring training dental implant placement using computer-guided implant navigation system for predoctoral students: A pilot study. Eur. J. Dent. Educ. 2019, 23, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.M.; Lan, T.H.; Pan, C.Y.; Lee, H.E. Dental implant navigation system guide the surgery future. Kaohsiung J. Med. Sci. 2018, 34, 56–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques-Guasch, J.; Rodriguez-Bauza, R.; Satorres-Nieto, M.; Wang, H.L.; Hernandez-Alfaro, F.; Gargallo-Albiol, J. Accuracy of dynamic implant navigation surgery performed by a novice operator. A preliminary study in a cadaveric model. Int. J. Comput. Dent. 2022, 0, b2588207. [Google Scholar] [CrossRef]
- Casap, N.; Nadel, S.; Tarazi, E.; Weiss, E.I. Evaluation of a navigation system for dental implantation as a tool to train novice dental practitioners. J. Oral Maxillofac. Surg. 2011, 69, 2548–2556. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Yao, Y.; Yang, X. Effect of a dynamic navigation device on the accuracy of implant placement in the completely edentulous mandible: An in vitro study. J. Prosthet. Dent. 2022; in press. [Google Scholar] [CrossRef]
- Gillot, L.; Cannas, B.; Friberg, B.; Vrielinck, L.; Rohner, D.; Pettersson, A. Accuracy of virtually planned and conventionally placed implants in edentulous cadaver maxillae and mandibles: A preliminary report. J. Prosthet. Dent. 2014, 112, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S.; Emery, R.W.; Lank, K.; Ryan, J. Implant Placement Accuracy Using Dynamic Navigation. Int. J. Oral Maxillofac. Implant. 2017, 32, 92–99. [Google Scholar] [CrossRef]
- Wang, W.; Zhuang, M.; Li, S.; Shen, Y.; Lan, R.; Wu, Y.; Wang, F. Exploring training dental implant placement using static or dynamic devices among dental students. Eur. J. Dent. Educ. 2022; Online ahead of print. [Google Scholar] [CrossRef]
- Jung, R.E.; Schneider, D.; Ganeles, J.; Wismeijer, D.; Zwahlen, M.; Hammerle, C.H.; Tahmaseb, A. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2009, 24, 92–109. [Google Scholar]
- Chen, C.K.; Yuh, D.Y.; Huang, R.Y.; Fu, E.; Tsai, C.F.; Chiang, C.Y. Accuracy of Implant Placement with a Navigation System, a Laboratory Guide, and Freehand Drilling. Int. J. Oral Maxillofac. Implant. 2018, 33, 1213–1218. [Google Scholar] [CrossRef]
- Lopes, A.; de Araujo Nobre, M.; Santos, D. The Workflow of a New Dynamic Navigation System for the Insertion of Dental Implants in the Rehabilitation of Edentulous Jaws: Report of Two Cases. J. Clin. Med. 2020, 9, 421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittwer, G.; Adeyemo, W.L.; Schicho, K.; Birkfellner, W.; Enislidis, G. Prospective randomized clinical comparison of 2 dental implant navigation systems. Int. J. Oral Maxillofac. Implant. 2007, 22, 785–790. [Google Scholar]
- Gurdan, Z.; Szalma, J. Evaluation of the success and complication rates of self-drilling orthodontic mini-implants. Niger. J. Clin. Pract. 2018, 21, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Gurdan, Z.; Vajta, L.; Toth, A.; Lempel, E.; Joob-Fancsaly, A.; Szalma, J. Effect of pre-drilling on intraosseous temperature during self-drilling mini-implant placement in a porcine mandible model. J. Oral Sci. 2017, 59, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Stefanelli, L.V.; DeGroot, B.S.; Lipton, D.I.; Mandelaris, G.A. Accuracy of a Dynamic Dental Implant Navigation System in a Private Practice. Int. J. Oral Maxillofac. Implant. 2019, 34, 205–213. [Google Scholar] [CrossRef]
- Emery, R.W.; Merritt, S.A.; Lank, K.; Gibbs, J.D. Accuracy of Dynamic Navigation for Dental Implant Placement-Model-Based Evaluation. J. Oral Implantol. 2016, 42, 399–405. [Google Scholar] [CrossRef]
- Ochandiano, S.; Garcia-Mato, D.; Gonzalez-Alvarez, A.; Moreta-Martinez, R.; Tousidonis, M.; Navarro-Cuellar, C.; Navarro-Cuellar, I.; Salmeron, J.I.; Pascau, J. Computer-Assisted Dental Implant Placement Following Free Flap Reconstruction: Virtual Planning, CAD/CAM Templates, Dynamic Navigation and Augmented Reality. Front. Oncol. 2021, 11, 754943. [Google Scholar] [CrossRef]
- Cassetta, M.; Bellardini, M. How much does experience in guided implant surgery play a role in accuracy? A randomized controlled pilot study. Int. J. Oral Maxillofac. Surg. 2017, 46, 922–930. [Google Scholar] [CrossRef]
- Brief, J.; Edinger, D.; Hassfeld, S.; Eggers, G. Accuracy of image-guided implantology. Clin. Oral Implant. Res. 2005, 16, 495–501. [Google Scholar] [CrossRef]
- Zhan, Y.; Wang, M.; Cheng, X.; Li, Y.; Shi, X.; Liu, F. Evaluation of a dynamic navigation system for training students in dental implant placement. J. Dent. Educ. 2021, 85, 120–127. [Google Scholar] [CrossRef]
- Tang, T.; Huang, Z.; Liao, L.; Gu, X.; Zhang, J.; Zhang, X. Factors that Influence Direction Deviation in Freehand Implant Placement. J. Prosthodont. 2019, 28, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Jorba-Garcia, A.; Gonzalez-Barnadas, A.; Camps-Font, O.; Figueiredo, R.; Valmaseda-Castellon, E. Accuracy assessment of dynamic computer-aided implant placement: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 2479–2494. [Google Scholar] [CrossRef] [PubMed]
- Hassfeld, S.; Muhling, J. Computer assisted oral and maxillofacial surgery--a review and an assessment of technology. Int. J. Oral Maxillofac. Surg. 2001, 30, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Heiland, M.; Pohlenz, P.; Blessmann, M.; Werle, H.; Fraederich, M.; Schmelzle, R.; Blake, F.A. Navigated implantation after microsurgical bone transfer using intraoperatively acquired cone-beam computed tomography data sets. Int. J. Oral Maxillofac. Surg. 2008, 37, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Kunzendorf, B.; Naujokat, H.; Wiltfang, J. Indications for 3-D diagnostics and navigation in dental implantology with the focus on radiation exposure: A systematic review. Int. J. Implant. Dent. 2021, 7, 52. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Error at Basis (Mean ± SD) | Total Error at Apex (Mean ± SD) | Angular Error (Mean ± SD) | |
|---|---|---|---|
| First session | 1.80 mm ± 0.93 mm | 2.02 mm ± 0.88 mm | 2.51° ± 1.48° |
| Second session | 1.61 mm ± 0.81 mm | 1.56 mm ± 0.70 mm | 1.51° ± 0.82° |
| Very Safe | Safe | Sufficient | Unsafe | Very Unsafe | |
|---|---|---|---|---|---|
| First session How safe did you feel during implant placement? | 3 | 4 | 2 | 1 | |
| How safe did you feel with the handling of the mininavident? | 3 | 4 | 2 | 1 | |
| How safe did you feel with the field of view during operation? | 2 | 1 | 5 | 2 |
| Very Safe | Safe | Sufficient | Unsafe | Very Unsafe | |
|---|---|---|---|---|---|
| First session How safe did you feel during implant placement? | 2 | 3 | 5 | ||
| How safe did you feel with the handling of the mininavident? | 3 | 6 | 1 | ||
| How safe did you feel with the field of view during operation? | 4 | 3 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spille, J.; Helmstetter, E.; Kübel, P.; Weitkamp, J.-T.; Wagner, J.; Wieker, H.; Naujokat, H.; Flörke, C.; Wiltfang, J.; Gülses, A. Learning Curve and Comparison of Dynamic Implant Placement Accuracy Using a Navigation System in Young Professionals. Dent. J. 2022, 10, 187. https://doi.org/10.3390/dj10100187
Spille J, Helmstetter E, Kübel P, Weitkamp J-T, Wagner J, Wieker H, Naujokat H, Flörke C, Wiltfang J, Gülses A. Learning Curve and Comparison of Dynamic Implant Placement Accuracy Using a Navigation System in Young Professionals. Dentistry Journal. 2022; 10(10):187. https://doi.org/10.3390/dj10100187
Chicago/Turabian StyleSpille, Johannes, Eva Helmstetter, Paul Kübel, Jan-Tobias Weitkamp, Juliane Wagner, Henning Wieker, Hendrik Naujokat, Christian Flörke, Jörg Wiltfang, and Aydin Gülses. 2022. "Learning Curve and Comparison of Dynamic Implant Placement Accuracy Using a Navigation System in Young Professionals" Dentistry Journal 10, no. 10: 187. https://doi.org/10.3390/dj10100187