
The Barriers and Facilitators to the Use of Lifestyle Apps: A Systematic Review of Qualitative Studies

 , ,
, ,
Abstract
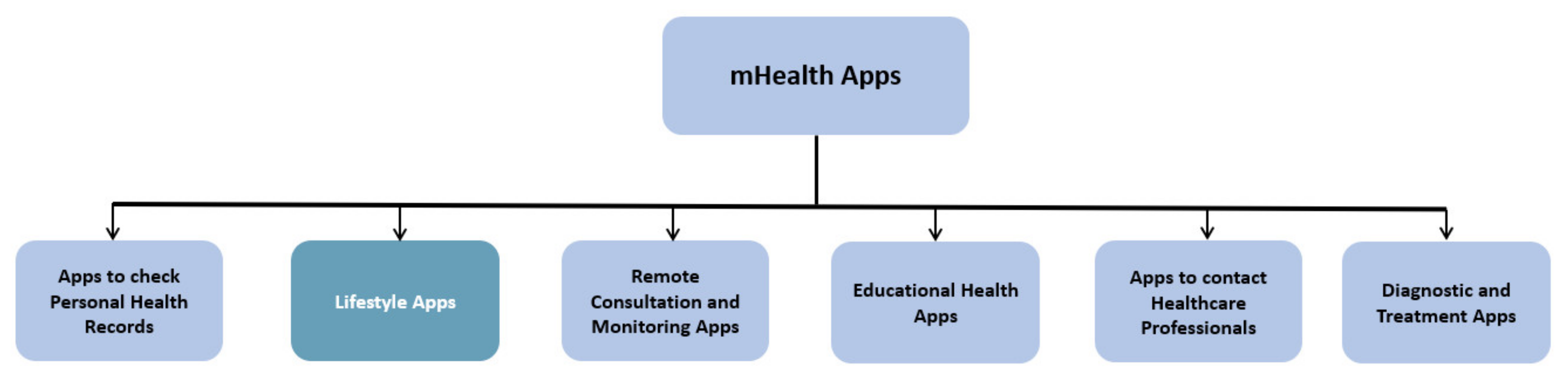
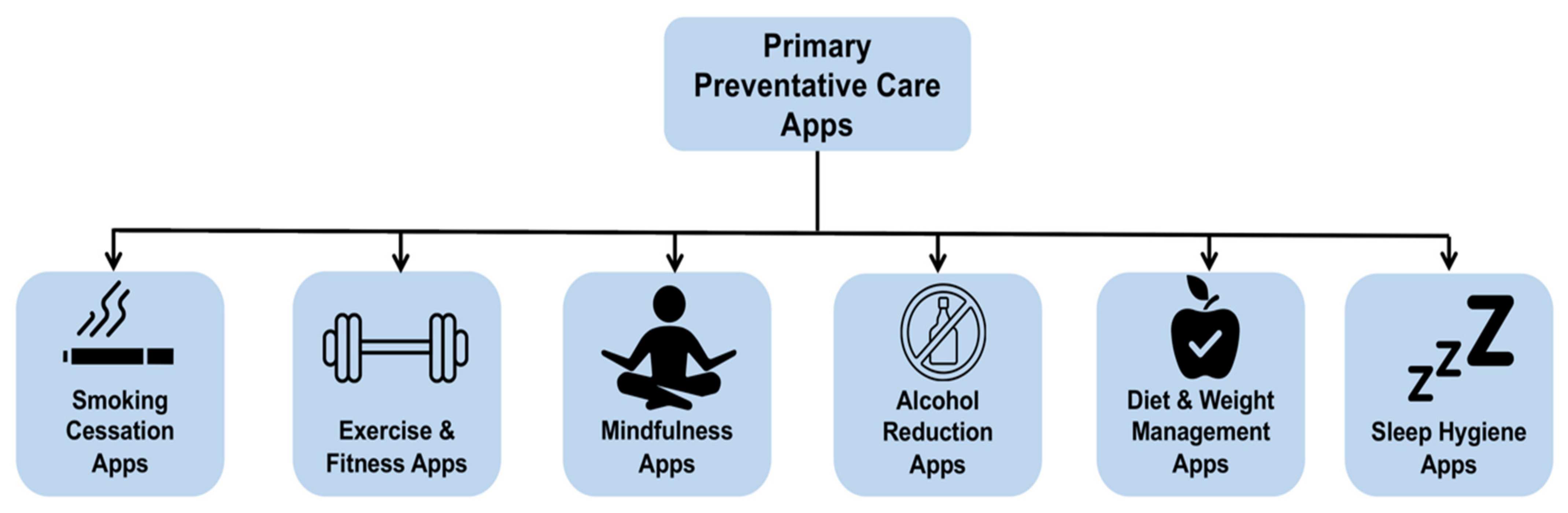
:1. Introduction
- Adoption: This concerns the ability of LAs to acquire new users.
- Engagement: This describes the extent to which users interact with lifestyle apps.
- Retention: This factor is strongly interlinked with engagement and describes users returning to lifestyle apps, after initial use.
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
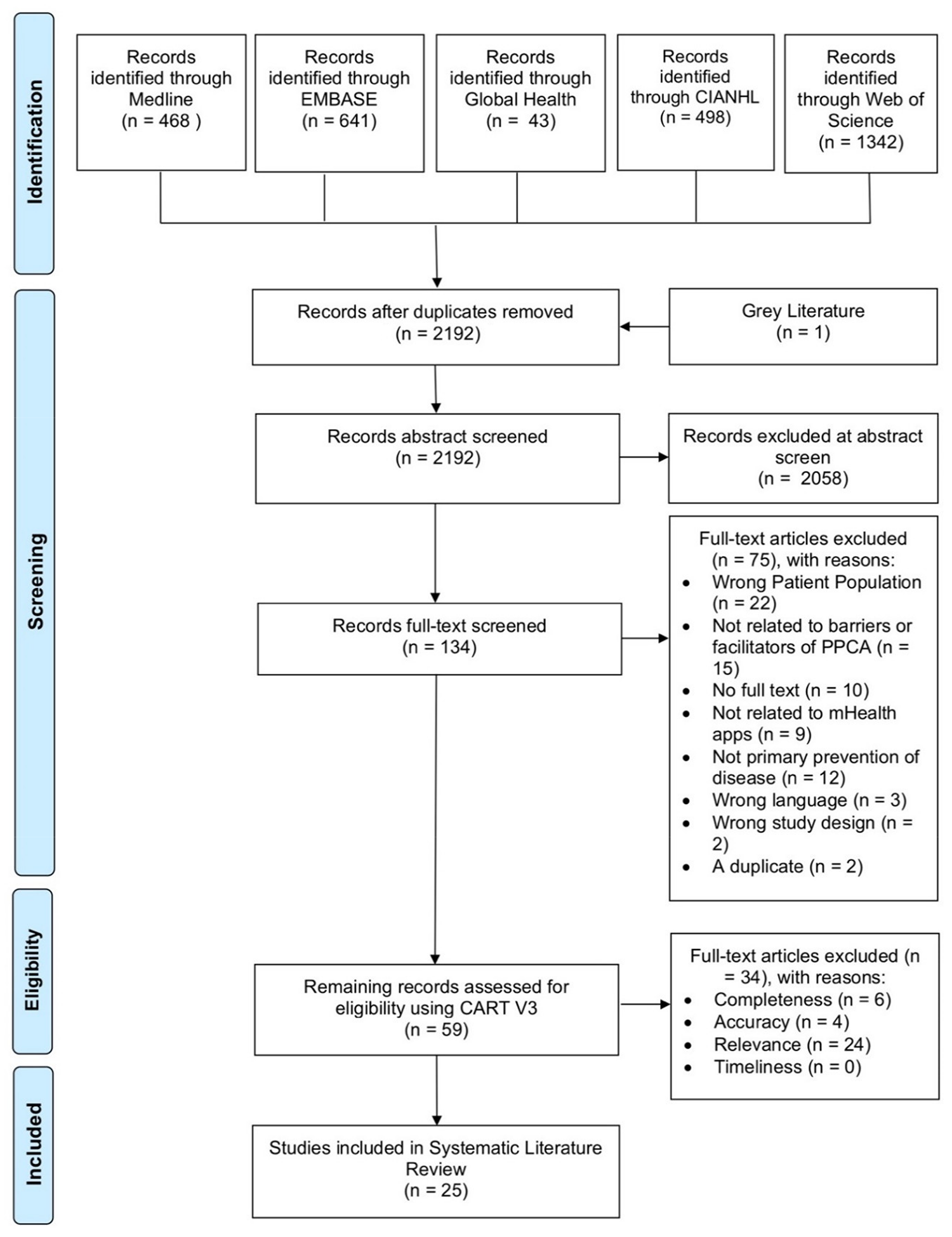
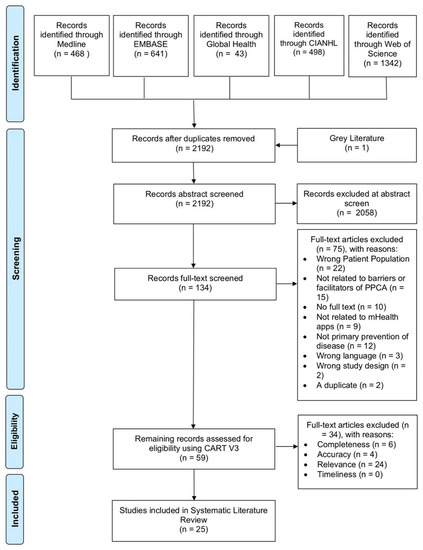
2.3. Search Results
2.4. Data Synthesis
2.5. Critical Appraisal
3. Results
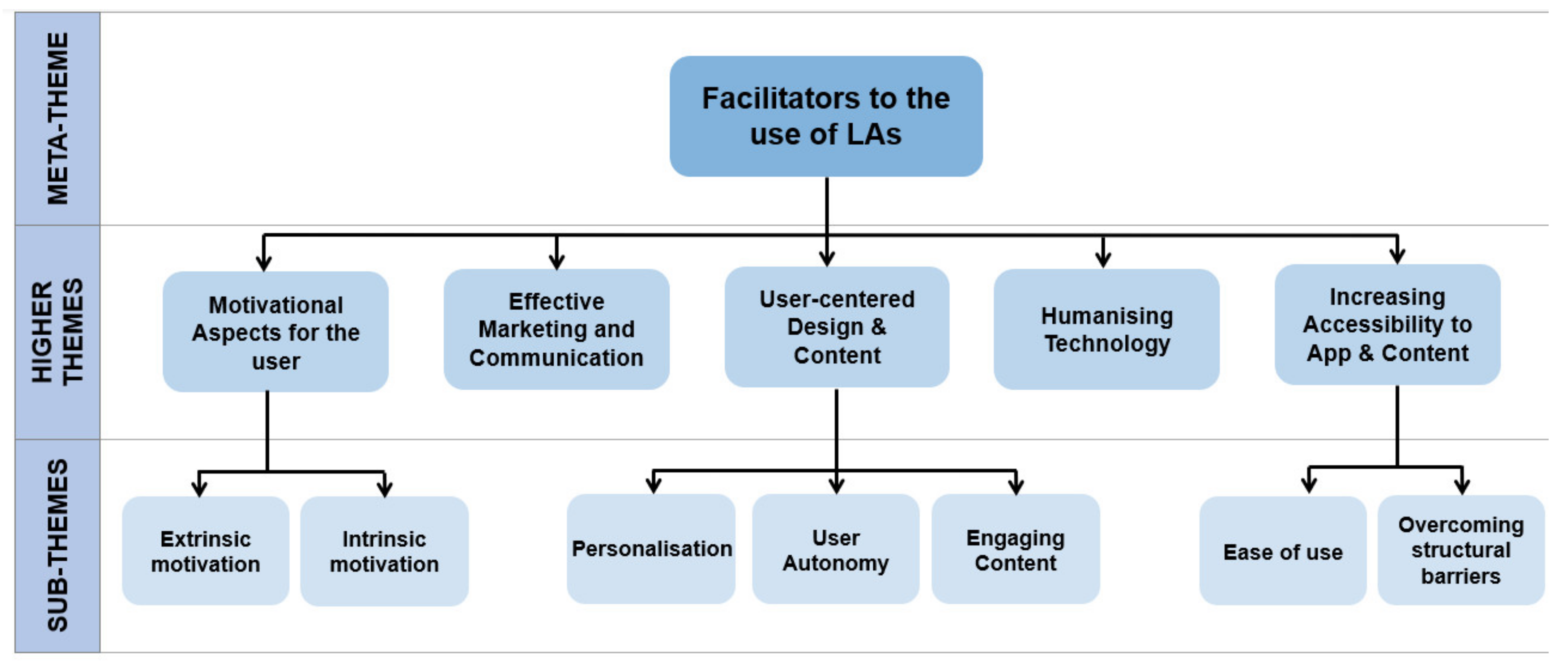
3.1. Facilitators
3.1.1. Theme 1: Motivational Aspects for the User
Intrinsic Motivation
“People are motivated from the inside”[13]
Extrinsic Motivation
“Even if it’s just a reminder. It pushes us through”[16]
3.1.2. Theme 2: Effective Marketing and Communication
“I did not go into something that I did not know”[24]
3.1.3. Theme 3: Increasing Accessibility to Apps and Content
Ease of Use
“You want the process to be as simple as possible”[15]
Overcoming Structural Barriers
“I just looked at the word straight away and I was like I can’t read that, I’m not going to even try”[30]
3.1.4. Theme 4: User-Centred Design and Content
Personalisation
“Not everyone is auditory, not everyone is visual, not everyone is kinaesthetic…”[14]
User Autonomy
“I don’t want to do X km because the app says so, but because I want to”[10]
Engaging Content
“It’s got to be different everyday”[20]
3.1.5. Theme 5: Humanising Technology
“For me, it should be…a bit more human”[10]
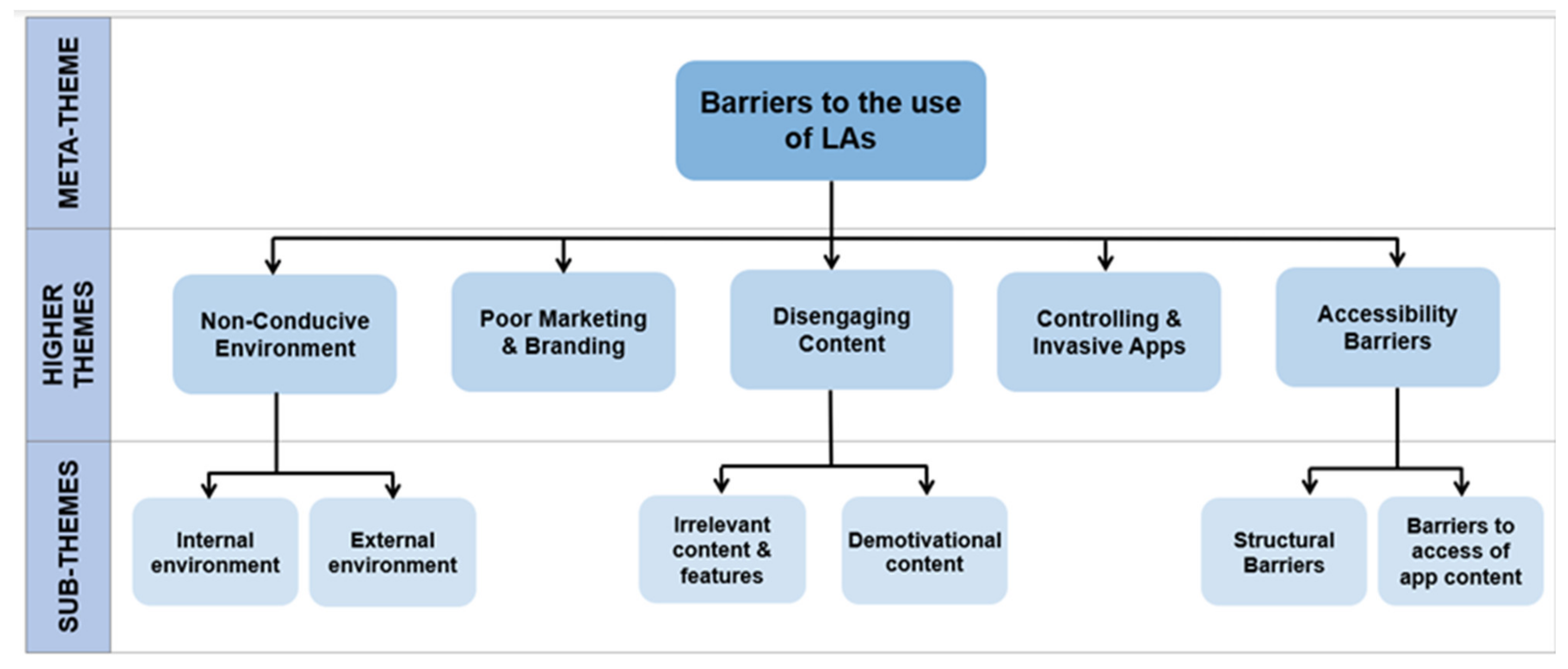
3.2. Barriers
3.2.1. Theme 1: Accessibility Barriers
Structural Barriers
“I don’t think my telephone is good enough… I will change it, but I don’t know when.”[23]
Barriers to Access of App Content
“A lot of functions are everywhere. I don’t know where to go, how I can change the functions, and where to go…” [18]
3.2.2. Theme 2: Poor Marketing and Branding:
“People just don’t know what is”[17]
3.2.3. Theme 3: Controlling and Invasive Apps
“I don’t want an electronic device telling me what to do”[6]
3.2.4. Theme 4: Disengaging Content
Irrelevant Content and Features
“What is your point…. you don’t need to tell me”[30]
Demotivational Content
“It makes me feel somehow bad”[32]
3.2.5. Theme 5: Non-Conducive Environment
External Environment
“When I feel that I have to do too many things, I feel that I cannot fit the space to do it”[14]
Internal Environment
“If you’re feeling quite stressed, probably using the app is going to be harder”[14]
4. Discussion
Limitations of Systematic Literature Review
5. Conclusions
Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Systematic Literature Review

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SPIDER | Search String |
|---|---|
| Sample | digital apps or digital applications or digital app or digital application or medical apps or medical applications or medical app or medical application or mHealth or mHealth app or mHealth application or mHealth apps or mobile health or smartphone app or smartphone apps or smartphone application or smartphone applications or mobile health apps or mobile health app or mobile health application or eHealth app or eHealth apps or eHealth applications or eHealth application or mobile apps or mobile application or mobile app or mobile applications or mobile phone app or mobile phone application or mobile phone apps or mobile phone applications or cell phones or cell phone or cell phone app or cell phone apps or cell phone application or cell phone applications) |
| Phenomenon of Interest | (smoking cessation or drinking reduction or harmful drinking or harmful drinkers or risk drinking or risk drinkers or problem drinkers or problem drinking or excess drinking or drinking in excess or excessive drinking or binge drinking or binge drinkers or drinking cessation or at risk drinkers or lifestyle or healthy eating or eating behaviours or diet or weight control or weight management or mindfulness or meditation or stress reduction or relax or relaxed or relaxing or relaxation or sleep hygiene or sleep habits or sleep behaviour or sleep quality or personal care or wellness or self-care or calorie intake or calorie reduction or weight change or fitness or exercise or exercises or exercising or healthy living or eating habits) |
| Evaluation | (obstacle or barrier or issues or obstruction or difficulties or difficulty or deter or deterrent or drawback or hinder or hinderance or hindering or prevents or preventing or prevention or impede or problem or complication or impediment or enables or enable or enabling or enabler or aid or aiding or promote or promoting or promotion or encourage or encouraging or encouragement or help or helping or assist or assisting or ease or easing or facilitators or facilitates or facilitating or empowers or empower or empowering or empowerment) |
| Design and Research Type | (qualitative or ethnograph or phenomenal or grounded theory or hermeneutic or observation or focus group or focus groups or interview or mixed methods or mixed method or multimethod or multi-method) |
| C: completeness | Articles were eliminated if:
|
| A: accuracy | Articles were eliminated if:
|
| R: relevance | Articles were included only if:
|
| T: timeliness | Data had to be collected between 2016–2020. |

Appendix B. Critical Appraisal
| Wei Peng et al., 2016 | Simons et al., 2018 | Krishnan and Lokachari, 2019 | Ming Li Carol Seah et al., 2021 | Zhou et al., 2019 | Kanthwala, 2019 | Nurmi et al., 2020 | Jones et al., 2019 | Wu et al., 2017 | Lyzwinski et al., 2018 | Leffers. J, 2018 | Darcel et al., 2018 | Baretta, Perski & Steca, 2019 | Nikolaou et al., 2019 | Subasinghe et al., 2019 | Xiaoxiao et al., 2020 | Vaghefi and Tulu, 2019 | Castro et al., 2020 | Chandler et al., 2020 | Chen, 2018 | Nour et al., 2017 | LaPrincess et al., 2019 | Laurie, Blandford, 2016 | Leffers J et al., 2018 | Rose 2020 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Was there a clear statement of the aims of the research? | C | Y | Y | Y | Y | Y | Y | Y | Y | C | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Is a qualitative methodology appropriate? | Y | Y | Y | Y | Y | Y | Y | Y | Y | C | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Was the research design appropriate to address the aims of the research? | Y | Y | Y | Y | Y | Y | Y | Y | C | Y | Y | Y | Y | N | Y | Y | C | Y | Y | Y | Y | Y | N | C | Y |
| Was the recruitment strategy appropriate to the aims of the research? | N | C | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | C |
| Was the data collected in a way that addressed the research issue? | Y | Y | Y | C | Y | C | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | Y | Y | Y |
| Has the relationship between researcher and participants been adequately considered? | N | C | N | Y | Y | Y | N | Y | Y | Y | Y | N | C | Y | C | N | N | C | Y | N | Y | N | Y | Y | N |
| Have ethical issues been taken into consideration? | Y | Y | C | Y | Y | C | Y | Y | Y | C | Y | Y | Y | Y | Y | Y | Y | Y | Y | C | Y | C | Y | Y | Y |
| Was the data analysis sufficiently rigorous? | Y | Y | Y | Y | Y | C | Y | C | C | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Is there a clear statement of findings? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Is the research valuable | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Author & Year | Method | Sample Characteristics | Critical Appraisal |
|---|---|---|---|
| Nikolaou et al., 2019 | Survey + focus groups | Survey, n = 2285 Focus group, n = 719 young individuals aged 13–24 | Unrepresentative sample: Global study in 6 countries but only conducted focus groups in English. Therefore, only those capable of speaking English recruited, which may reflect high educational standards; thus, views may not necessarily be reflective of non-English speakers in those countries. |
| Chandler R. et. al, 2020 | Focus groups | n = 23 | Small sample size. |
| Poor recruitment methods -> Only one of the 4 focus groups targeted the ideal age group for the proposed mobile app. | |||
| Black women involved all from a similar community; therefore, results of this study can only be generalized to women of a similar demographic. | |||
| Only focus groups used; therefore, high susceptibility to biases such as halo effect and the dominance effect. | |||
| Laurie and Blandford, 2016 | Semi-structured interviews | n = 16 | Study design limits the data that could have been collected: i.e., data were only gathered at start and end of study, meaning that experiences during the actual study were not looked into. |
| HAWTHORNE EFFECT Lack of consistency in exit interview technique, i.e., later changed to become more open and participant directed. | |||
| Small sample size. Unrepresentative: results cannot be generalised in context of wider population.
| |||
| Nour.M et al., 2017 | Focus group | Focus group n = 32 | Solely focus-group-based methodology; therefore, vulnerable to biases such as groupthink bias. |
| Not generalizable to other age groups or individuals from different countries to Australia where culture may be different. | |||
| Nurmi et al., 2020 | Think aloud and semi-structured interviews | n = 12 | Small sample size, not representative of wider population. |
| Interviews only provided information on participants’ initial reactions to the app’s features. | |||
| Inconsistency in what was presented to individuals (app was being developed so later participants had more features to form views from). | |||
| Researcher-bias: Researchers prompted participants when they were silent for a prolonged period of time may introduce bias. | |||
| Régnier, Dugré, Darcel et al., 2018 | Questionnaires + 2 sets of Semi-structured Interviews | (pre-app use) n = 46 questionnaires to help design app n = 12 in depth interviews (users of app) n = 21 supplementary interviews (low-income individuals in general population) | Small sample size. |
| Choice of the participants was limited to individuals from underprivileged backgrounds. These individuals had a very heavy combination of constraints (e.g., budget, social integration, and language). | |||
| Lieffers. J et al., 2018 | Semi-structured interviews | n = 24 | Small sample size. |
| Unrepresentative of population: skewed sample with many participants being female and 18–30 years of age and participants being recruited from two Canadian provinces. | |||
| Lack of demographic information of participants collected; therefore, difficult to determine generalizability of results. | |||
| Wei Peng et al., 2016 | Interviews, focus groups | n = 44 | Only 5 participants outside of the university setting (lack of diversity amongst participants). These 5 participants were interviewed individually as opposed to in a focus group due to time constraints (inconsistent methodology). |
| Focus groups may introduce several biases including the halo effect. | |||
| 2/3 of the participants were female. | |||
| Not all the participants had used health apps before, and thus the discussion was based on their perceptions from examples provided by the trigger materials, which may be inconsistent from their perceptions if they actually had used health apps. | |||
| Wu et al., 2017 | Semi-structured interviews (think aloud) | n = 10 | No quantitative data to support engagement measurements. Not generalisable to other digital interventions. Small sample size. Input (despite being think aloud) from the interviewer might have influenced the users. Participants were compensated. |
| Vaghefi and Tulu, 2019 | Interviews and diary entries | Pre-use and post-use interview: 17 participants, 193 diaries from same 17 participants | More than half of the participants were female, used an iPhone, and were highly motivated to take care of their health—generalisability might be called into question, especially if you consider income and pre-usage motivation as factors. Extremely subjective in terms of data collected—would have been better if there was objective data to compare against. Only focused on health and wellness apps—not extended to other types of apps. Participants were compensated and all came from the same environment (university). Sent daily reminders to users to remind them to log in the diary—their influence was not kept to a minimum. Small sample size. |
| Jones et al., 2019 | Focus groups | Focus group, n = 15 | Small sample size. |
| Only mothers included-not fathers/other carers, e.g., grandparents. From 1 geographical area. | |||
| Castro et al., 2020 | Focus groups | n = 17 | Enrolled only people over 40 with high social vulnerability—did not compare across different demographics and incomes. Active people spoke more in the focus group than the non-active people; therefore, the design of the app will be skewed towards preferences of active rather than non-active participants. |
| LaPrincess C. Brewer, 2019 | Focus groups and survey | Focus group 23, co-design 13, survey 36 | Small sample size. |
| Most participants are women (but this is inherent to AA church). | |||
| Ming Li Carol Seah et al., 2021 | Focus-group interviews | n = 8 | App was only used for 3 days. |
| Small sample size of university students’ perspectives on mindfulness and mHealth. | |||
| Subasinghe et al., 2019 | Focus-group questionnaire | Focus group = 4 questionnaire = 23 | Greater education and older participants are over-represented. Small sample size. Short follow up in usability. |
| Lieffers, J., 2018 | Interviews | n = 26 | Small sample size. |
| Way interviewees were recruited (email to users) means that they are more likely to give feedback. | |||
| Primarily female and 18–50 years of age; however, this distribution generally reflects the overall population of eaTracker users. | |||
| Data on education level, income, and ethnicity were not collected from participants. | |||
| Huan Chen, 2018 | Interview | n = 20 | The data are specific to the culture (Chinese) and may not be generalizable. All citizens came from urbanised locations, so the barriers and facilitators might be different. |
| Xiaoxiao et al., 2020 | Questionnaire, interviews | Questionnaire n = 379 Interviews n = 10 | Sample is unrepresentative (mostly female, college-educated, and tech-savvy). The cross-sectional data do not allow for the analysis of predictive power in understanding people’s post-adoptive behaviours |
| Dario Baretta, Olga Perski, Patrizia Steca, 2019 | Semi structured interviewed | Baseline n = 20, after 2 weeks n = 17 | Heterogeneity amongst digital-literacy abilities of the sample group. |
| Kanthawala, S. | Semi-structured interview (think-aloud) | Interviews: n = 19 | Participants were highly educated and from the same city. Digital literacy was not assessed. |
| Krishnan and Lokachari, 2019 | Focus groups, interviews | Focus Groups: n = 12, Interview: n = 12 | Dominance effect (a dominant individual shapes the discussion), halo effect (the perceived status of a group member influences the discussion), and groupthink (the members in a group tend to think similarly to maintain group cohesion), among several others (Mukherjee et al., 2015). Not generalisable to other age groups. Needs to be backed up by empirical data. |
| Zhou et al., 2019 | Questionnaire, semi-structured interview | n = 117 (survey), n = 117 (semi-structured interviews) | Not generalisable to the entire population (e.g., sick and the elderly). Not applicable to other countries where regulations/cultures might be different. |
| Simons et al., 2018 | Focus groups, semi-structured interviews | Interviews n = 10 Focus groups n = 34 | App is specifically adapted to the Flemish lower-educated working young adults, which limits its generalizability. |
| Lynnette Nathalie Lyzwinski et al., 2019 | Focus group, written feedback | n = 8 | This is a single qualitative exploratory study with a participatory pilot design at one university campus with a mostly female sample. |
| The purposive nature of the study required some previous experience with general health apps and some idea of mindfulness, which limited the pool of interest and eligibility. Funding limitations also restricted this to a small pilot participatory study. | |||
| Johanna Friederike Rose 2020 May 2020 | Interviews | n = 11 | Small sample size: All highly educated, higher proportion of men, recruited via snowball technique, all between 22–28. |
| Furthermore, studying people that a researcher knows personally might lead to compromises in the researcher’s ability to disclose information and raises issues of an imbalance of power between the inquirer and the participants. Interviewees first language varied—communication barriers |
References
- Mobile for Development. The State of Mobile Internet Connectivity Report 2020. Available online: https://www.gsma.com/r/somic/ (accessed on 24 August 2021).
- Vaghefi, I.; Tulu, B. The Continued Use of Mobile Health Apps: Insights from a Longitudinal Study. JMIR mHealth uHealth 2019, 7, e12983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nouri, R.; Kalhori, S.R.N.; Saeedi, M.G.; Marchand, G.; Yasini, M. Criteria for assessing the quality of mHealth apps: A systematic review. J. Am. Med. Inform. Assoc. 2018, 25, 1089–1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pires, I.M.; Marques, G.; Garcia, N.M.; Flórez-Revuelta, F.; Ponciano, V.; Oniani, S. A Research on the Classification and Applicability of the Mobile Health Applications. J. Pers. Med. 2020, 10, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castle-Clarke, S.; Imison, C. The Digital Patient: Transforming Primary Care; Nuffield Trust: London, UK, 2016. Available online: http://www.digitalfutures.manchester.ac.uk/media/1691/nuffield-report.pdf (accessed on 23 August 2021).
- McKay, F.H.; Wright, A.; Shill, J.; Stephens, H.; Uccellini, M. Using Health and Well-Being Apps for Behavior Change: A Systematic Search and Rating of Apps. JMIR Mhealth Uhealth 2019, 7, e11926. [Google Scholar] [CrossRef] [PubMed]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qual. Health Res. 2012, 22, 1435–1443. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Jahns, R.-G. The mHealth Apps Market Is Getting Crowded. 2017. pp. 1–6. Available online: https://research2guidance.com/mhealth-app-market-getting-crowded-259000-mhealth-apps-now/ (accessed on 23 August 2021).
- Baretta, D.; Perski, O.; Steca, P. Exploring Users’ Experiences of the Uptake and Adoption of Physical Activity Apps: Longitudinal Qualitative Study. JMIR mHealth uHealth 2019, 7, e11636. [Google Scholar] [CrossRef] [Green Version]
- Guest, G.; MacQueen, K.; Namey, E. Applied Thematic Analysis; SAGE: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Kumar, A.; Mhaskar, R.; Emmanuel, P.; Mishra, S.; Patel, S.; Naik, E. Critical appraisal skills are essential to informed decision-making. Indian J. Sex. Transm. Dis. AIDS 2009, 30, 112–119. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Xu, X. Continuous use of fitness apps and shaping factors among college students: A mixed-method investigation. Int. J. Nurs. Sci. 2020, 7, S80–S87. [Google Scholar] [CrossRef]
- Laurie, J.; Blandford, A. Making time for mindfulness. Int. J. Med. Inform. 2016, 96, 38–50. [Google Scholar] [CrossRef]
- Peng, W.; Kanthawala, S.; Yuan, S.; Hussain, S.A. A qualitative study of user perceptions of mobile health apps. BMC Public Health 2016, 16, 1158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro, P.C.; Romano, L.B.; Frohlich, D.; Lorenzi, L.J.; Campos, L.B.; Paixão, A.; Bet, P.; Deutekom, M.; Krose, B.; Dourado, V.Z.; et al. Tailoring digital apps to support active ageing in a low income community. PLoS ONE 2020, 15, e0242192. [Google Scholar] [CrossRef] [PubMed]
- Lyzwinski, L.N.; Caffery, L.; Bambling, M.; Edirippulige, S. University Students’ Perspectives on Mindfulness and mHealth: A Qualitative Exploratory Study. Am. J. Health Educ. 2018, 49, 341–353. [Google Scholar] [CrossRef]
- Seah, M.L.C.; Koh, K.T. The efficacy of using mobile applications in changing adolescent girls’ physical activity behaviour during weekends. Eur. Phys. Educ. Rev. 2020, 27, 113–131. [Google Scholar] [CrossRef]
- Simons, D.; De Bourdeaudhuij, I.; Clarys, P.; De Cocker, K.; Vandelanotte, C.; Deforche, B. A Smartphone App to Promote an Active Lifestyle in Lower-Educated Working Young Adults: Development, Usability, Acceptability, and Feasibility Study. JMIR mHealth uHealth 2018, 6, e44. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Tombor, I.; Shahab, L.; West, R. Usability testing of a smoking cessation smartphone application (‘SmokeFree Baby’): A think-aloud study with pregnant smokers. Digit. Health 2017, 3, 29942594. [Google Scholar] [CrossRef] [Green Version]
- Nour, M.; Chen, J.; Allman-Farinelli, M.; Leung, M.; Fazzino, T. Young Adults’ Engagement with a Self-Monitoring App for Vegetable Intake and the Impact of Social Media and Gamification: Feasibility Study. JMIR Form. Res. 2019, 3, e13324. [Google Scholar] [CrossRef]
- Gerke, S.; Stern, A.D.; Minssen, T. Germany’s digital health reforms in the COVID-19 era: Lessons and opportunities for other countries. NPJ Digit. Med. 2020, 3, 94. [Google Scholar] [CrossRef]
- Régnier, F.; Dugré, M.; Darcel, N.; Adamiec, C. Providing a Smart Healthy Diet for the Low-Income Population: Qualitative Study on the Usage and Perception of a Designed Cooking App. JMIR mHealth uHealth 2018, 6, e11176. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, G.; Lokachari, P.S. Adoption of health and fitness apps by mobile users: Interactive qualitative analysis. In Proceedings of the 2019 Portland International Conference on Management of Engineering and Technology (PICMET), Portland, OR, USA, 25–29 August 2019; pp. 3–10. [Google Scholar]
- Nikolaou, C.K.; Tay, Z.; Leu, J.; Rebello, S.A.; Morenga, L.T.; Van Dam, R.M.; Lean, M.E.J. Young People’s Attitudes and Motivations Toward Social Media and Mobile Apps for Weight Control: Mixed Methods Study. JMIR mHealth uHealth 2019, 7, e11205. [Google Scholar] [CrossRef] [Green Version]
- Rose, J. Using the Bad for Something Good” Exploring the Possible Paradox of Meditation Apps in Light of Digital Stress. DIVA. 2021. Available online: http://www.diva-portal.org/smash/record.jsf?pid=diva2%3A1446414&dswid=6017 (accessed on 25 August 2021).
- Brewer, L.C.; Hayes, S.N.; Caron, A.R.; Derby, D.A.; Breutzman, N.S.; Wicks, A.; Raman, J.; Smith, C.M.; Schaepe, K.S.; Sheets, R.E.; et al. Promoting cardiovascular health and wellness among African-Americans: Community participatory approach to design an innovative mobile-health intervention. PLoS ONE 2019, 14, e0218724. [Google Scholar] [CrossRef] [PubMed]
- Lieffers, J.R.; Arocha, J.F.; Grindrod, K.; Hanning, R.M. Experiences and Perceptions of Adults Accessing Publicly Available Nutrition Behavior-Change Mobile Apps for Weight Management. J. Acad. Nutr. Diet. 2017, 118, 229–239.e3. [Google Scholar] [CrossRef] [PubMed]
- Kanthawala, S.; Joo, E.; Kononova, A.; Peng, W.; Cotten, S. Folk theorizing the quality and credibility of health apps. Mob. Media Commun. 2018, 7, 175–194. [Google Scholar] [CrossRef]
- Jones, F.; Whitehouse, A.; Dopson, A.; Palaghias, N.; Aldiss, S.; Gibson, F.; Shawe, J. Reducing unintentional injuries in under fives: Development and testing of a mobile phone app. Child Care Health Dev. 2019, 46, 203–212. [Google Scholar] [CrossRef]
- Nurmi, J.; Knittle, K.; Ginchev, T.; Khattak, F.; Helf, C.; Zwickl, P.; Castellano-Tejedor, C.; Lusilla-Palacios, P.; Costa-Requena, J.; Ravaja, N.; et al. Engaging Users in the Behavior Change Process With Digitalized Motivational Interviewing and Gamification: Development and Feasibility Testing of the Precious App. JMIR mHealth uHealth 2020, 8, e12884. [Google Scholar] [CrossRef]
- Chandler, J.; Cumpston, M.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions. 2021. Available online: https://training.cochrane.org/handbook (accessed on 25 August 2021).
- Subasinghe, A.K.; Garland, S.M.; Gorelik, A.; Tay, I.; Wark, J.D. Using Mobile Technology to Improve Bone-Related Lifestyle Risk Factors in Young Women with Low Bone Mineral Density: Feasibility Randomized Controlled Trial. JMIR Form. Res. 2019, 3, e9435. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Bao, J.; Watzlaf, V.; Parmanto, B. Barriers to and Facilitators of the Use of Mobile Health Apps from a Security Perspective: Mixed-Methods Study. JMIR mHealth uHealth 2019, 7, e11223. [Google Scholar] [CrossRef]
- Pampel, F.C.; Krueger, P.M.; Denney, J.T. Socioeconomic Disparities in Health Behaviors. Annu. Rev. Sociol. 2010, 36, 349–370. [Google Scholar] [CrossRef] [Green Version]
- Loring, B.; Robertson, A. Obesity and Inequities. 2021. Available online: https://www.euro.who.int/__data/assets/pdf_file/0003/247638/obesity-090514.pdf (accessed on 25 August 2021).
- Lucivero, F.; Jongsma, K.R. A mobile revolution for healthcare? Setting the agenda for bioethics. J. Med. Ethics 2018, 44, 685–689. [Google Scholar] [CrossRef]
- Hurst, L.; Mahtani, K.; Pluddemann, A.; Lewis, S.; Harvey, K.; Briggs, A.; Boyle, A.; Bajwa, R.; Haire, K.; Entwistle, A.; et al. Defining Healthcare in the NHS: CEBM Report. 2019. Available online: https://www.cebm.net/2019/04/defining-value-based-healthcare-in-the-nhs/%0A1 (accessed on 24 August 2021).
- Azuma, K.; Nojiri, T.; Kawashima, M.; Hanai, A.; Ayaki, M.; Tsubota, K.; TRF-Japan Study Group. Possible favorable lifestyle changes owing to the coronavirus disease 2019 (COVID-19) pandemic among middle-aged Japanese women: An ancillary survey of the TRF-Japan study using the original “Taberhythm” smartphone app. PLoS ONE 2021, 16, e0248935. [Google Scholar] [CrossRef]
- Di Domenico, S.I.; Ryan, R.M. The Emerging Neuroscience of Intrinsic Motivation: A New Frontier in Self-Determination Research. Front. Hum. Neurosci. 2017, 11, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohan, A. Has Lockdown Made Consumers More Open to Privacy. Ernst & Young. 2021. Available online: https://www.ey.com/en_uk/consulting/ey-global-consumer-privacy-survey/has-lockdown-made-consumers-more-open-to-privacy (accessed on 25 August 2021).
- Sydow, L. The Impact of Coronavirus on the Mobile Economy as Businesses Enforce Working from Home, Conferences are Postponed, Flights are Canceled, Schools are Closed, Storefronts and Restaurants Shut Their Doors and People are quarantined Inside, the World Is. 2021. Available online: https://www.appannie.com/en/insights/market-data/coronavirus-impact-mobile-economy/ (accessed on 3 November 2021).
- NHS England. Around One Million Downloads of Fitness App during Lockdown as People Stay Fit. 2020. Available online: https://www.england.nhs.uk/2020/07/around-one-million-downloads-of-fitness-app-during-lockdown-as-people-stay-fit/ (accessed on 2 December 2021).





| Sample | Smartphone users |
| Phenomenon of Interest | LA use |
| Design | Surveys and Interviews |
| Evaluation | Barriers and Facilitators |
| Research Type | Qualitative |
| Inclusion | Exclusion |
|---|---|
| Focuses on LAs | Doesn’t focus on LAs |
| Primary Research | Review articles or any form of secondary research |
| Published between 2016 and 2020 | Published before 31 December 2015 or after 1 January 2021 |
| Full article published in English | Article not published in English |
| Focuses on the barriers or facilitators to the use of LAs | Doesn’t focus on the barriers or facilitators to the use of Las |
| Qualitative Research | Quantitative Research |
| Focus on the use of short message services or mHealth apps solely used for surveillance or location tracking (e.g. Reminders for patient checkups) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shabir, H.; D’Costa, M.; Mohiaddin, Z.; Moti, Z.; Rashid, H.; Sadowska, D.; Alam, B.; Cox, B. The Barriers and Facilitators to the Use of Lifestyle Apps: A Systematic Review of Qualitative Studies. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 144-165. https://doi.org/10.3390/ejihpe12020012
Shabir H, D’Costa M, Mohiaddin Z, Moti Z, Rashid H, Sadowska D, Alam B, Cox B. The Barriers and Facilitators to the Use of Lifestyle Apps: A Systematic Review of Qualitative Studies. European Journal of Investigation in Health, Psychology and Education. 2022; 12(2):144-165. https://doi.org/10.3390/ejihpe12020012
Chicago/Turabian StyleShabir, Habiba, Matthew D’Costa, Zain Mohiaddin, Zaeem Moti, Hamza Rashid, Daria Sadowska, Benyamin Alam, and Benita Cox. 2022. "The Barriers and Facilitators to the Use of Lifestyle Apps: A Systematic Review of Qualitative Studies" European Journal of Investigation in Health, Psychology and Education 12, no. 2: 144-165. https://doi.org/10.3390/ejihpe12020012