Factors Driving Users’ Engagement in Patient Social Network Systems


1
Information System Study Program, Faculty of Science and Technology, Universitas Airlangga, Surabaya 60115, Indonesia
2
Research Center for Quantum Engineering Design, Faculty of Science and Technology, Universitas Airlangga, Surabaya 60115, Indonesia
3
Faculty of Computer and Mathematical Sciences, Perlis Branch, Arau Campus, Universiti Teknologi MARA, Perlis 02600, Malaysia
4
Department of Computer Science and Information Engineering, Asia University, Taichung City 41354, Taiwan
*
Author to whom correspondence should be addressed.
Informatics 2021, 8(1), 8; https://doi.org/10.3390/informatics8010008
Submission received: 11 December 2020
/
Revised: 1 February 2021
/
Accepted: 5 February 2021
/
Published: 9 February 2021
(This article belongs to the Section Health Informatics)
Abstract
:Participatory medicine and e-health help to promote health literacy among non-medical professionals. Users of e-health systems actively participate in a patient social network system (PSNS) to share health information and experiences with other users with similar health conditions. Users’ activities provide valuable healthcare resources to develop effective participatory medicine between patients, caregivers, and medical professionals. This study aims to investigate the factors of patients’ engagement in a PSNS by integrating and modifying an existing behavioral model and information system model (i.e., affective events theory (AET) and self-determination theory (SDT)). The AET is used to model the structure, the affective aspects of the driven behavior, and actual affective manifestation. The SDT is used to model interest and its relations with behavior. The data analysis and model testing are based on structural equation modeling, using responses from 428 users. The results indicate that interest and empathy promote users’ engagement in a PSNS. The findings from this study suggest recommendations to further promote users’ participation in a PSNS from the sociotechnical perspective, which include sensitizing and constructive engagement features. Furthermore, the data generated from a user’s participation in a PSNS could contribute to the study of clinical manifestations of disease, especially an emerging disease.
1. Introduction
Participatory medicine and e-health have encouraged non-medical professionals to participate in healthcare activities or simply to lead a healthier lifestyle. A study by Pew Internet revealed that one in three adults in the United States accessed the Internet to search for a diverse range of health topics and concerns [1]. Another study within the Australian region suggested that 80% of the Internet users sought for information about health online [2]. The trend is also rising in other regions, such as in Scotland [3] and Taiwan [4]. Other studies have examined health information seeking behavior based on medical and physiological perspectives [5,6], consumer’s characteristics [7,8,9,10], and social contexts [11,12].
In addition to health information seeking on the Internet, users also actively participated in a patient social network system (PSNS), a virtual platform for informal health communities where members can find others with similar health issues [13] and exchange detailed data about symptoms, treatments, and experiences related to specific diseases [14]. Patients with chronic diseases were reported to be more active in engaging in PSNSs [15,16]. Chronic diseases refer to long-duration conditions that last one year or more, require continuing medical attention, and generally progress slowly [17]. There are four main types of chronic diseases according to the World Health Organization (WHO): cardiovascular diseases, cancers, chronic respiratory diseases, and diabetes. Managing chronic diseases is difficult for both patients and physicians [18]. Treatments of complex and chronic diseases are usually long-term, including post-surgery therapies and medication. Some of the challenges are insufficient physicians’ time spent on each patient, the communication gap between patients and physicians, the decline of patients’ adherence to medical advice, and the treatment burden in the long-term [19].
In response to treatment management challenges, patients and families seek additional health resources in PSNSs by taking part in participatory e-health activities, such as joining discussion groups in PSNSs to learn from others who have similar health issues, post in PSNSs to share their experiences and treatments, and provide emotional support between patients. Patients can also share health data (e.g., symptoms, treatments, health conditions, and medical test results) in a specific format that facilitates further analysis. In addition to the benefits to patient care, PSNSs provide valuable data sources for medical professionals and researchers to study clinical manifestations of a disease based on posts and health data shared by patients. Some examples of PSNSs are PatientsLikeMe (www.patientslikeme.com accessed on 11 December 2020), Ben’s Friends (bensfriends.org accessed on 11 December 2020), Society for Participatory Medicine (participatorymedicine.org accessed on 11 December 2020), and BrainTalk Communities for neurological disease (braintalkcommunities.org accessed on 11 December 2020).
User engagement (both participation and contribution) will benefit the patient communities. It characterizes the community and creates valuable healthcare resources to inform participatory medicine, as it is a practice that involves patients, caregivers, and medical professionals. Similar to other online communities, patient engagement in a PSNS is voluntary and defines the sustainability of the community. Previous studies have shown that there are underlying motivations and factors that drive the continuous engagement of a community member in online activities. Participating in an online community can be motivated by several different factors, such as satisfaction from helping other people [20], altruism [21], self-development [22], and reputation building [23]. In a study of health communities focusing on infertility, such participation included posting support for others (which may be driven by socioemotional motivation) and acknowledging support from others (which may be driven by motivations to seek information) [24]. The latter may strengthen the sense of community connectedness and sustainability. Another study of knowledge sharing in social media reveals that perceived online attachment, perceived online relationship commitment, and altruism had significantly positive impacts on one’s participation in knowledge sharing activities [21].
This study aims to investigate the motivations to participate in a PSNS and the forms of engagement therein. Understanding patients’ motivations and examining what factors drive users to engage in a patient community is a key analysis subject in online health community studies. User engagement not only defines the community’s sustainability, but it is also one of the most challenging issues in community development. In the case of PSNSs, user empathy is an important factor that motivates engagement in virtual social interactions. Another motivation to participate in PSNSs is the need for health information sharing, because understanding health concepts might be more difficult than other topics.
2. Theoretical Framework
2.1. User’s Engagement in Online Communities
User engagement refers to all users’ participation and involvement in an information system [25,26]. It emphasizes the state of connectedness and involvement between users and between users and the systems [27]. In an online community, user engagement is essential for the effectiveness and sustainability of a community [28]. The dynamic nature of engagement platforms, such as online communities, enables iterative processes of resource exchange and social connections that co-create value [29,30], thus heightening engagement among users at the cognitive and emotional levels [28].
In a PSNS, user engagement reflects the behaviors of participation and contribution between its users, which are comprised of patients, families, caregivers, and medical professionals. Engagement activities in a PSNS include e-health activities, such as discussing a specific disease, comorbidity, or home treatment, in addition to calling for online consultation with medical professionals. Since participation in a PSNS is voluntary, identifying factors that influence user engagement and incorporating these factors in managing the PSNS would improve the community’s outcomes and enhance the community’s sustainability. Based on the modification of affective events theory (AET) and self-determination theory (SDT), this paper examines the contributing factors that influence user engagement in a PSNS. AET offers a theoretical framework to explain the behavioral motivators underlying the relationship between a user’s interest to engage in a patient community and the use of a PSNS, while SDT provides a broad framework to study a user’s motivation to engage in health activities in a PSNS.
2.2. Affective Events Theory
Affective events theory (AET) originally explained how employees’ emotions and their reactions to events that occurred in a workplace environment affected their performance and job satisfaction [31,32]. The accumulation of a succession of positive inducing events (uplifts) or negative inducing events (hassles) predisposes affective states in employees that, in turn, presage the attitudes toward jobs and the behavioral responses (stay or intend to quit). Work environment features (such as the competition at work, the organization culture, and physical conditions) influence judgment-driven and affect-driven behaviors directly and indirectly via work events and affectivity [32]. Judgment-driven behaviors involve the evaluation of the environmental situation and information collection that underlie the formation of work attitudes. On the other hand, affect-driven behaviors are directly influenced by emotional experiences.
When AET is applied to information systems and digital technology, work environment features are similar to the systems’ features that determine the user’s attitude toward the system or technology [32,33]. Users will develop positive attitudes (e.g., satisfaction, the willingness to continue using the system, and feeling at ease) when the feature delivers the correct functionality and required quality. On the contrary, users might get frustrated when a feature is difficult to use, missing, or not working correctly. Work events in AET can be conceptualized as any ongoing events while using the systems or technology—such as interruptions, disturbances, or errors—that might induce negative emotions. Based on types of behaviors in AET, user acceptance and the continued intention of using a system or technology are the realizations of judgment-driven behaviors, while adaptation behavior, coping behavior, and the use of a system or technology are the affective responses to events or stimuli that justify affect-driven behaviors.
AET has been widely applied to investigate the role of a user’s emotions in technology use behavior. A study in [33] showed that perceived quality and cognitive appraisal of incident handling determined the usage behaviors of digital media, and the satisfaction mediated the emotional effects in post-adoption behaviors. In another study, perceived site quality, affective reactions, and cognitive appraisal of incident handling determined e-service customer behaviors. The study also reported the significance of emotion and affect in post-adoption behaviors [32]. Using AET, a prior study built a conceptual framework to examine the influence of user affect and passion for creativity on social media [34]. The results suggested that excitement facilitated social media use in the context of special events, and user passion affected user engagement in participation in social media.
2.3. Self-Determination Theory
Self-determination theory (SDT) articulates a theoretical framework for examining human motivation, both controlled and autonomous, in cognitive and social development, as well as individual differences [35], suggesting that psychological needs fulfillment contributes to promoting a user’s engagement and intrinsic motivation in virtual environments [36,37] and online communities [38]. Controlled motivation regulates one’s behavior based on external contingencies of reward or punishment and introjected regulation, which is partially internalized and influenced by factors such as avoidance of shame and self-esteem [35]. Autonomous motivation reflects self-determined behavior because it is consistent with intrinsic goals and originates from the self [39]. When individuals act for autonomous reasons, they experience a sense of choice, personal endorsement, and satisfaction with their actions, and they persist in their behaviors without any external reinforcement [35,39].
In addition to formal theory development, SDT has been applied to many domains, including health and medicine [38,39], learning [40,41], and virtual environments [36,37,42]. A study in [39] applied self-determination theory to test the influence of autonomous and controlled motivations on the prediction of health-related behaviors. The results showed consistent effects of autonomous motivation on intentions and behavior across multiple health-related behaviors. Based on SDT, an online teacher community of practice was designed to facilitate teacher’s autonomy, competence, and relatedness needs and to support autonomous motivation [42]. Regarding the life of online communities, SDT was applied to examine the mechanism that supports autonomy, competence, and relatedness in online diabetes communities [38]. The satisfaction of these needs plays a significant role in the community’s sustainability.
3. Materials and Methods
3.1. Hypotheses Development
The first step of the research was constructing a research model based on the modification of AET and SDT [31,34,35,43] to examine the contributing factors that influence user engagement in a PSNS. AET was used to model the structure, the affective drivers (e.g., empathy), and the actual affective responses (e.g., user engagement in a PSNS). SDT was used to model what motivated user engagement in a PSNS and its relations with user behavior.
There is a link between user interest and engagement in a PSNS. User interest refers to the desire or need to explore more about a particular subject based on the rational and preferred choice made by a user. The concept of interest in this context is related to the concept of self-determination in SDT. Based on SDT, users are motivated to grow when their needs for autonomy, competence, and relatedness are fulfilled [35,39]. These psychological needs form the ability of a person to make choices and manage their own life. In the case of a PSNS, the user’s interest is one of the most important drivers that motivates the user to decide on using the system. The interest originates from intrinsic motivation and encourages users to actively conduct social interactions as the means of fulfilling their psychological needs, i.e., gaining experiential knowledge and improving their competencies by participating in discussions with other users or medical professionals, connecting to other users with similar health conditions and building the sense of community, setting and evaluating the goals of using the system. Experiential knowledge encourages users to change health behaviors, manage their diseases [13], and continue participating in a PSNS.
Participating in such a patient community may be burdensome to some extent. For example, as a content contributor, a user must ensure they provide and share only reliable and accurate health contents. Additionally, before adopting anything from the community, users must fact-check to avoid any malpractice [8]. Thus, contributing to a PSNS requires not only strong interest but also commitment. Participating in an activity based on one’s interest may generate a variety of outcomes, one of which is empathy, referring to the aptitude to understand and feel what others are experiencing and the desire to help them [44]. Empathy encourages members of a PSNS to extend their best effort, because they share the same experiences and emotions of specific health conditions. This discussion leads to the following hypotheses:
Hypothesis 1.
Interest to engage in a community positively correlates with the generation of empathy.
Hypothesis 2.
Interest to engage in a community positively impacts the use of a PSNS.
According to AET, workplace events evoke affective responses (e.g., emotional reactions) from workers that result in behavioral implications (e.g., productivity, job satisfaction, and job contentment). In the context of our study, the event refers to an individual’s engagement in a PSNS that generates and is influenced by the user’s affection. Affection dominates social interactions between members in social technologies, thus generating affect-driven judgment [32]. One of the most important embodiments of user affection in a PSNS’s social interactions is empathy. Empathy toward another member that was recently diagnosed with severe illness encourages the use of a PSNS for sharing health information and treatment experiences, leading to the following hypothesis:
Hypothesis 3.
Empathy generated by interest to engage in a community positively impacts the use of a PSNS.
Previous studies suggest that emotional factors are likely to generate interest in an activity [21,45], and this may result in the extension of affection itself. Thus, it is expected that the stronger the interest to engage in a patient community, the more extensive the use of the PSNS. However, as this relationship is regulated by the level of empathy, it should be logical to add the following hypothesis:
Hypothesis 4.
Empathy generated by an event moderates the effect of interest to engage in a PSNS.
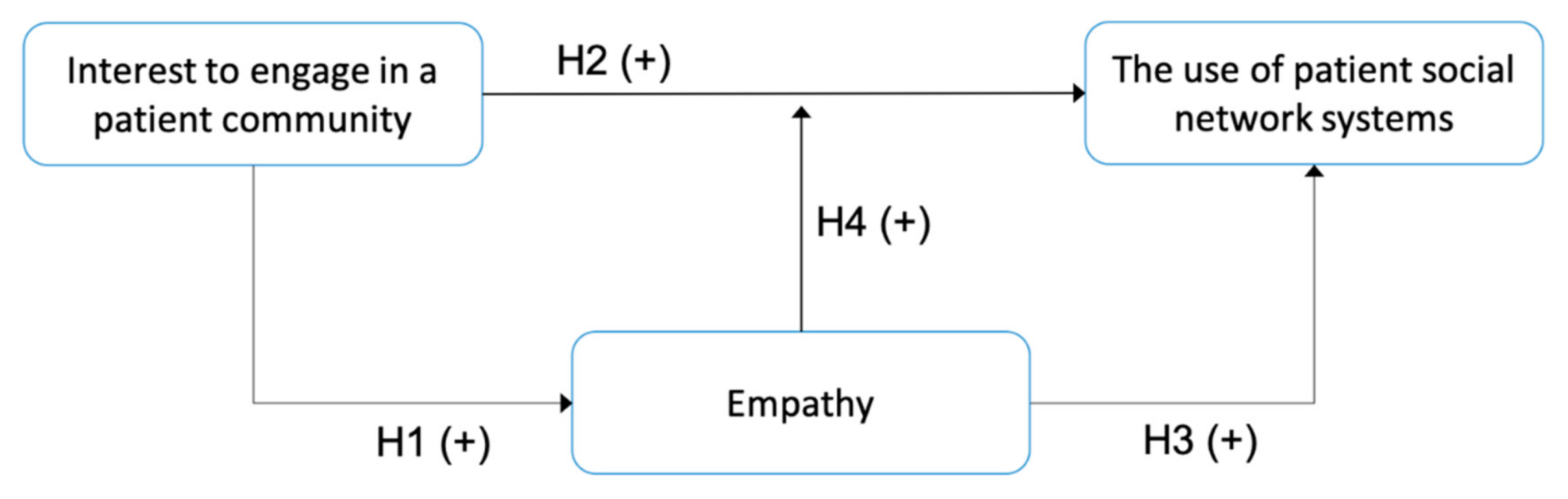
Figure 1 presents the research model based on the integration of AET and SDT.
3.2. Data Collection and Analysis
For the data collection, we conducted random sampling using a web-based survey from December 2019 to March 2020. The respondents were recruited via a link posted in several health communities on Facebook, researchers’ accounts on Facebook and Twitter, and several groups on the WhatsApp messaging application. To identify the PSNS user, we stated the respondent’s requirements on the survey description (i.e., a user of one or more PSNSs for at least one month and aged 18 years or older). As an additional step to filter eligible respondents, the survey was preceded by a set of questions about PSNS usage. If the respondent had never used any PSNS before, then he or she could not proceed further. The survey set consisted of demographics profile questions and a behavioral questionnaire, which was developed based on the integration of AET and SDT model instruments. All the proposed constructs were measured using a six-point Likert scale (i.e., strongly disagree, disagree, slightly disagree, slightly agree, agree, and strongly agree). The complete survey is provided in Supplementary Material File S1.
Before the data collection, the survey draft was reviewed and revised by two experts: one health informatics practitioner and one public health expert. We conducted a pretest to 25 selected respondents to assess the readability and clarity of the questions. Subsequently, we submitted the data collection protocol to the Health Research Ethical Committee of the Faculty of Public Health at Universitas Airlangga. As the study recorded only non-identifiable information about the respondents and involved only negligible risk (i.e., there was no foreseeable risk or discomfort to respondents), the study fell under the ethical exemption category.
The collected data were analyzed and modeled based on partial least square structural equation modeling (PLS-SEM) using SmartPLS3 software [46]. Following [47], PLS-SEM was selected because the purpose of this study was to identify the factors characterizing a user’s engagement in a PSNS. The data analysis assessed the measurement model and estimated the parameters of the structural model. Drawing on the PLS-SEM evaluation, we analyzed the results, explored the implications, and proposed recommendations to improve users’ experiences when using PSNSs.
4. Results
Following the PLS-SEM method, the results include sample and demographic profiles that characterize the participants, the measurement model, and the structural model.
4.1. Respondent Profiles
The number of minimum samples for the data collection was calculated based on Slovin’s formula [48], as shown in Equation (1):
where n is the minimum sample size, N is the population size, and e is the margin of error.
The population size for this data collection was estimated to be over 800,000. Two of the most popular PSNSs, PatientsLikeMe (www.patientslikeme.com accessed on 11 December 2020) and Ben’s Friends (bensfriends.org accessed on 11 December 2020), recorded approximately 800,000 members in December 2019. The margin of error was set to 0.05, resulting in 399,804 ≈ 400 respondents as the minimum sample size. Following the disseminated survey’s link, a total of 627 respondents accessed and started the survey, but only 450 respondents completed the survey (71.8% completion rate). Of these, 22 responses were discarded following inconsistent and invalid answers, resulting in a final sample of 428 responses. Hence, the data analysis and model testing were based on the 428 valid responses. The complete profiles of the respondents are presented in Table 1.
The majority of the respondents engaged in the patient community were patients (61.45%). Most respondents reported using a PSNS weekly (36.21%) or monthly (34.35%). More than half of the respondents were aged between 41 and 50 years (40.65%). The gender profile was in line with a prior study confirming the specific role of females in the family and society healthcare [14].
4.2. Measurement Model Evaluation
The measurement model tested the validity and reliability of the proposed constructs. A robust construct had to go through a convergent validity test and a discriminant validity test. The results in Table 2 show that the loading factors for all indicators exceeded 0.7, and the average variance extracted (AVE) for all constructs was more than 0.5, indicating a favorable convergent validity [47,49].
The results in Table 3 demonstrate a satisfied discriminant validity, as indicated by the cross-loading of each variable being larger than 0.7 and the square root of each construct’s AVE being larger than its correlations with other constructs [47,49]. The reliability test evaluated the internal consistency; one of the methods involved calculating the composite reliability. The reliability test was considered acceptable, since the composite reliability of each construct in Table 3 exceeded 0.7 [47].
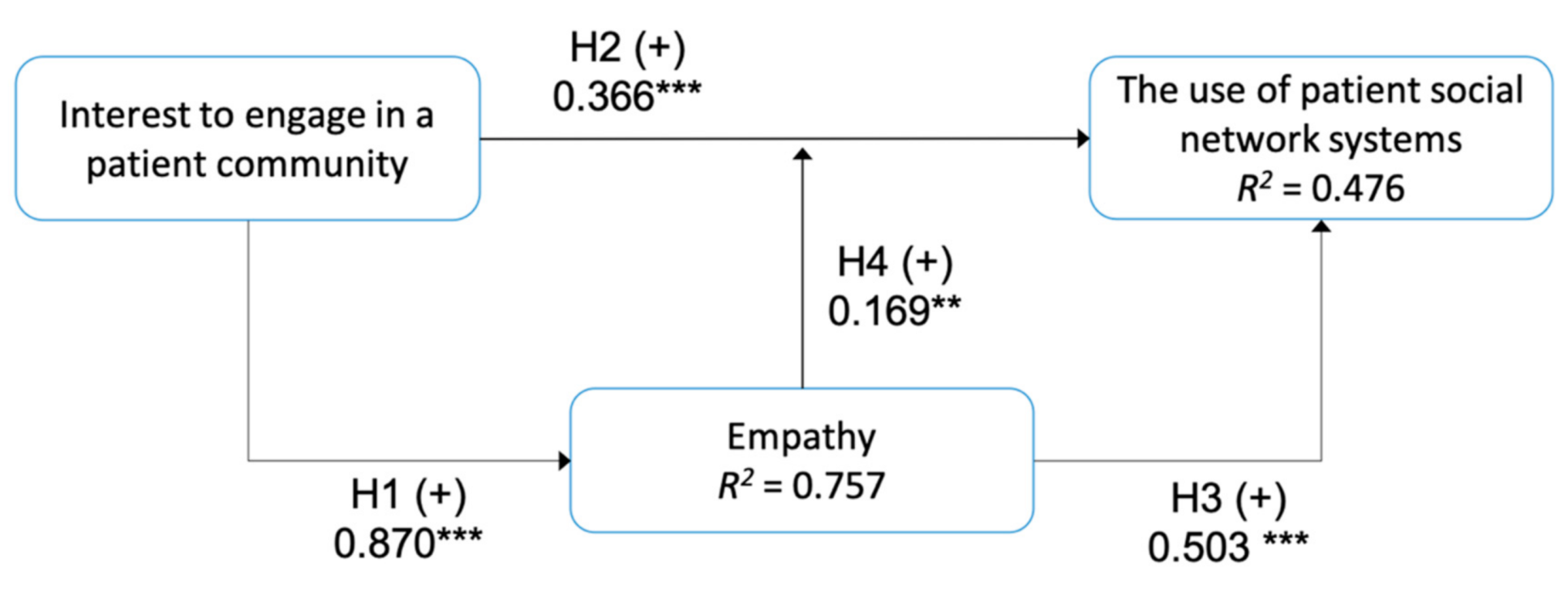
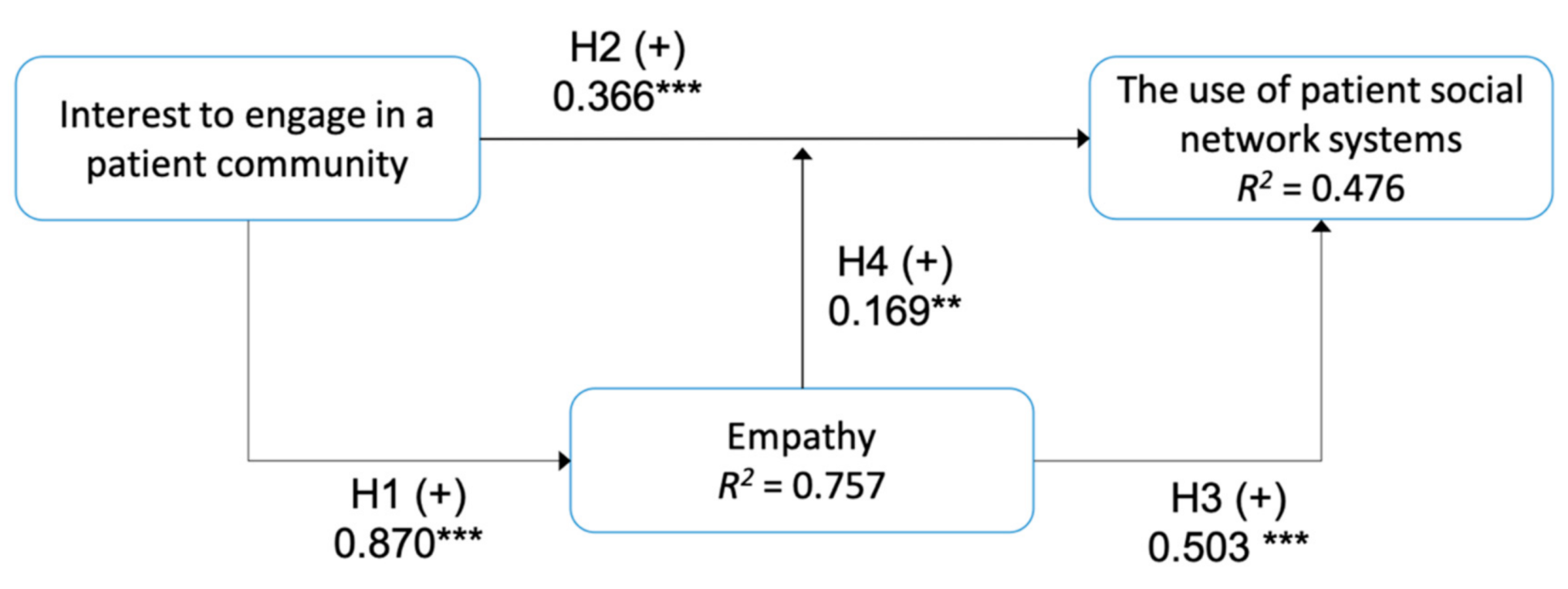
4.3. Structural Model and Hypotheses Test
The structural model assessment comprised the coefficient of determination (R2), the predictive sample reuse technique (Stone Geisser’s Q2), the effect size (f2), and the path coefficients. R2 measured the share of variance in a dependent (endogenous) construct; thus, it provided the model predictive power [50,51]. The R2 values ranged between 0 to 1, with a higher value indicating higher predictive power. The R2 values for empathy and the use of patient social network systems constructs were 0.757 and 0.476, respectively. The second assessment, Q2, evaluated the predictive validity of a model using PLS. A Q2 value larger than zero for a specific dependent construct indicates the path’s model for this particular construct [47], with a value higher than 0.5 indicating a substantial predictive model. The Q2 values for empathy and the use of patient social network system constructs were 0.503 and 0.355, respectively. The next assessment was measuring the effect sizes f2 of the relationships between the constructs. As a guideline, the f2 values ranged from 0.02 to 0.150, 0.150 to 0.350, and larger than 0.350, exhibiting weak, medium, and large effect sizes [52]. In this study, the f2 values for the relationships between constructs ranged from 0.159 to 1.114 (medium to large effect), as shown in Table 4.
The last assessment was testing the relationships among the hypothesized constructs and observable variables based on path coefficients, the statistical significance, and the t-values, as shown in Table 4. There was a positive relationship between interest to engage and empathy (path coefficient = 0.870, p < 0.001), which confirmed H1. The results also revealed that interest to engage (path coefficient = 0.366, p < 0.001) and empathy (path coefficient = 0.503, p < 0.001) had positive impacts on the use of PSNSs, thus supporting H2 and H3. Lastly, the moderation effect of empathy on interest to engage in PSNSs was significant (path coefficient = 0.169, p < 0.01), hence verifying H4. The structural model results are summarized in Figure 2.
5. Discussion
The use of social media and a PSNS for health-related purposes is prevalent among users in health sectors. Understanding patients’ motivations and examining what factors drive them to engage in a patient community is a key form of analysis in online health community studies. To optimize the benefits of PSNS for e-patient activities, this study examined how users leverage such systems. The findings from this study demonstrate that the proposed model, constructed from the integration of AET and SDT, was able to characterize a user’s engagement behavior in using a PSNS for e-patient activities. This discussion subchapter is organized into two themes: (1) the factors affecting user engagement in a PSNS, and (2) the implications and future studies.
5.1. Factors Affecting a User’s Engagement in a PSNS
This study explored the contributing factors that lead users to use a PSNS based on the integration of AET and SDT. Consistent with H1, the results indicated that interest to engage in a patient community may generate or intensify empathy. The higher the interest is, the greater the effort performed, and it contributes to the development of self-knowledge efficacy. One of the main factors influencing knowledgeable users to continue their participation in a PSNS is empathy, manifested itself as either (1) an understanding of how others feel and what they might be thinking, commonly referred to as a cognitive empathy, or (2) concerns with another individual’s emotions or emotional empathy.
The support of H2 suggests that interest affects the use of a PSNS. Creating and contributing to the body of health materials in patient communities involves meticulous research and a high understanding of specific health topics by education or by experience. It requires an intense cognitive effort, especially for non-medical professionals, to produce reliable and accurate health materials. The desire to help others may encourage users to make such an intensive effort when engaging in a PSNS. This finding is in line with prior studies in community of practice (CoP) suggesting that interest is one of the key factors of CoP sustainability [53], because it drives learning processes and knowledge sharing among members. Users also appraised the information made by community members to be more valuable and applicable because they share the same object of interest and emotional value [54], especially in a health community. From the social perspective, the sense of belonging to a community may strengthen the user’s interest to engage in that particular community. Users conduct social interactions (i.e., e-patient activities) in a PSNS because they want to nurture a satisfactory relationship with other users, especially those with similar conditions.
The positive correlation between empathy and the engagement in a PSNS in H3 shows that empathy motivates users to engage in PSNS activities, particularly as a contributor. Suffering from a disease, especially a life-threatening one, has major impacts on a patient’s life, such as the change in physical and physiological conditions, the adjustment of aspiration, lifestyle, and work. In most cases, patients and even family members develop psychiatric disorders following a chronic disease diagnosis. This situation is perceived to be distressing; hence, it could generate the feeling of empathy toward others who recently have been diagnosed with a chronic disease. This empathy evokes the desire to help others, which is demonstrated by users’ contributions and continuous engagement. This finding is also consistent with previous studies reporting that empathy is one of the motivational factors that encourages users to contribute in an online community by sharing health materials (e.g., information, answers to questions, knowledge, and experiences) [45,55]. The presence of interest and empathy may amplify users’ motivation to participate in a PSNS, as shown by H4 acceptance. Several studies reported that emotional factors, such as empathy, and interest directly contributed to continual user engagement [38,54,56].
5.2. Implications
In light of rising e-patient movement and health information sharing using PSNSs, this study should inform future behavioral studies. The contributing factors that affect the use of a PSNS can inform relevant stakeholders for developing and updating the general features in a PSNS (e.g., data sharing about symptoms, treatments, and conditions; dedicated search tools based on symptoms and treatments to facilitate a patient’s connection; data visualization of a user’s health profile; and discussion forums) from the sociotechnical perspective. Addressing the sociotechnical perspective in a PSNS should incorporate a holistic approach [57] that includes sensitizing features and constructive engagement features. The sensitizing feature is designed to sensitize the user to the concerns of other users and to help others perceive the benefits of the systems. This feature includes intelligent forms that minimize users’ cognitive loads and helps users complete the form correctly (e.g., a form that consists of an open question and rating scale questions, describing the quality or characteristics of the main question, and empathetic interfaces, such as incorporating empathy maps to design the system and a display menu with empathetic messages that inform users how they can contribute to others). The constructive engagement feature aims to encourage users to participate in e-patient activities in a PSNS. This feature includes data visualization based on user health profiles and advanced search tools that facilitate multiple symptoms and multiple treatments.
User interest in participating in a patient community can be fostered by adding acknowledgement features and advanced personalization to connect patients with similar conditions. This feature can be beneficial to promote user participation and to cultivate user empathy while participating in patient social networks. Some advanced personalization may include emotion recognition based on users’ textual analysis and the improvement of patient recommender systems based on multiple parameters.
Given the current situation of the coronavirus disease 2019 (COVID-19) global pandemic, identifying factors affecting user engagement in a PSNS has become increasingly significant. Since COVID-19 is an emerging disease [58] with a wide range of symptoms [59], researchers are struggling to understand the disease for further clinical management and supportive treatment [60]. The contribution of users and patients in sharing their conditions could help medical professionals and researchers to study the clinical manifestations, symptoms, and other epidemiology characteristics. For users and the general public, users who engage more with the system might gain greater benefits [14], such as managing the symptoms better, learning other users’ experiences, and receiving emotional support from other users or survivors.
5.3. Limitations and Future Studies
Although most of the results supported the goals of this study, there are some limitations of this study. Future works are required to corroborate and validate the results further. First, this study did not include the moderation effect of sociodemographic variables. Prior studies have examined the impacts of demographic characteristics and e-health literacy on e-patient behaviors [15,16]. Hence, it is advisable to investigate the moderation effect of other variables, such as gender, age group, educational attainment, and cultural traits, in future research. Second, we did not investigate further the behavior of patients with chronic diseases. Several studies have reported that patients with chronic diseases were more likely to participate in online discussions for information and emotional support [16,20]. Thus, additional studies are recommended to examine how patients with chronic diseases use PSNSs to support their long-term treatment. Third, this study only adopted part of AET (i.e., affect-driven behavior). Future research could investigate the judgment-driven behavior that motivates continual user engagement in a PSNS.
For model refinement, other constructs, such as personal health knowledge and e-health literacy, might be necessary to understand user engagement in a PSNS thoroughly. Future studies are also recommended to incorporate other physiological theories, such as protection motivation theory (PMT) or the health belief model (HBM), and information systems models, such as health information quality, service quality, and task technology fit.
6. Conclusions
This study examined the influence of affect-driven behavior (i.e., empathy) and interest on user engagement in the adoption of patient social network systems. The users’ behavior was defined based on the contributing factors that motivated them to participate in online patient communities. Interest to engage in a patient community and empathy affect the use of a PSNS. The interest motivates users to actively participate in a PSNS as a means of fulfilling their psychological needs (i.e., gaining experiential knowledge and improving their competencies). The next factor, empathy toward another member that was recently diagnosed with a chronic disease, evokes the desire to help others, because they have gone through the same experiences. These factors are expected to amplify and sustain user participation, since contributing to health-related communities as a non-medical professional requires intense cognitive efforts.
The findings from this study offer recommendations to further promote user participation in a PSNS from the sociotechnical perspective and a holistic approach that includes sensitizing and constructive engagement features. In addition to the benefits to patient care, user participation in a PSNS provides valuable data sources for medical professionals and researchers to study clinical manifestations of a disease, especially an emerging disease.
Supplementary Materials
The following are available online at https://www.mdpi.com/2227-9709/8/1/8/s1, S1: Online Survey.
Author Contributions
Conceptualization, I.P.; methodology, I.P.; software, I.P. and S.S.M.F.; validation, I.P., S.S.M.F., and C.-Y.H.; formal analysis, I.P.; data curation, I.P. and S.S.M.F.; writing—original draft preparation, I.P.; writing—review and editing, I.P., S.S.M.F., and C.-Y.H.; project administration, I.P. and C.-Y.H.; funding acquisition, I.P. and C.-Y.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Partnership Mandate Research Grants 2019, Universitas Airlangga, Indonesia, grant number 704/UN3/2019.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Health Research Ethical Committee of Faculty of Public Health, Universitas Airlangga (Approve project: 50-EA, date of approval: 04/02/2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical approval.
Acknowledgments
The authors sincerely thank the respondents for participating in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fox, S.; Duggan, M. Health Online 2013. Available online: http://www.pewinternet.org/2013/01/15/health-online-2013/ (accessed on 26 August 2018).
- Mc Daid, D.; Park, A.-L. Online Health: Untangling the Web. Available online: https://www.bupa.com.au/staticfiles/Bupa/HealthAndWellness/MediaFiles/PDF/LSE_Report_Online_Health.pdf (accessed on 26 August 2018).
- Moreland, J.; French, T.L.; Cumming, G.P. The Prevalence of Online Health Information Seeking Among Patients in Scotland: A Cross-Sectional Exploratory Study. JMIR Res. Protoc. 2015, 4, e4010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, F.-C.; Chiu, C.-H.; Chen, P.-H.; Miao, N.-F.; Lee, C.-M.; Chiang, J.-T.; Pan, Y.-C. Relationship Between Parental and Adolescent eHealth Literacy and Online Health Information Seeking in Taiwan. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 618–624. [Google Scholar] [CrossRef]
- Bauer, R.; Conell, J.; Glenn, T.; Alda, M.; Ardau, R.; Baune, B.T.; Berk, M.; Bersudsky, Y.; Bilderbeck, A.; Bocchetta, A.; et al. Internet use by patients with bipolar disorder: Results from an international multisite survey. Psychiatry Res. 2016, 242, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Suka, M.; Odajima, T.; Okamoto, M.; Sumitani, M.; Igarashi, A.; Ishikawa, H.; Kusama, M.; Yamamoto, M.; Nakayama, T.; Sugimori, H. Relationship between health literacy, health information access, health behavior, and health status in Japanese people. Patient Educ. Couns. 2015, 98, 660–668. [Google Scholar] [CrossRef] [PubMed]
- Puspitasari, I.; Fukui, K.-I.; Moriyama, K.; Numao, M. Predicting consumer familiarity with health topics by query formulation and search result interaction. In Proceedings of the Pacific RIM International Conference on Artificial Intelligence; Springer: Cham, Switzerland, 2014; Volume 8862, pp. 1016–1022. [Google Scholar]
- Puspitasari, I. The impacts of consumer’s health topic familiarity in seeking health information online. In Proceedings of the 2017 15th IEEE/ACIS International Conference on Software Engineering Research, Management and Applications, London, UK, 7–9 June 2017; pp. 104–109. [Google Scholar]
- Puspitasari, I.; Firdauzy, A. Characterizing Consumer Behavior in Leveraging Social Media for E-Patient and Health-Related Activities. Int. J. Environ. Res. Public Health 2019, 16, 3348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medlock, S.; Eslami, S.; Askari, M.; Arts, D.L.; Sent, D.; De Rooij, S.E.; Abu-Hanna, A. Health information-seeking behavior of seniors who use the internet: A survey. J. Med. Internet Res. 2015, 17, e10. [Google Scholar] [CrossRef]
- Lee, Y.J.; Boden-Albala, B.; Jia, H.; Wilcox, A.; Bakken, S. The association between online health information-seeking behaviors and health behaviors among hispanics in New York city: A community-based cross-sectional study. J. Med. Internet Res. 2015, 17, e261. [Google Scholar] [CrossRef]
- Song, H.; Omori, K.; Kim, J.; Tenzek, K.E.; Hawkins, J.M.; Lin, W.Y.; Kim, Y.C.; Jung, J.Y. Trusting social media as a source of health information: Online surveys comparing the United States, Korea, and Hong Kong. J. Med. Internet Res. 2016, 18, e25. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, S.; Deng, Z.; Chen, X. Knowledge sharing motivations in online health communities: A comparative study of health professionals and normal users. Comput. Human Behav. 2017, 75, 797–810. [Google Scholar] [CrossRef]
- Wicks, P.; Thorley, E.M.; Simacek, K.; Curran, C.; Emmas, C. Scaling PatientsLikeMe via a “generalized platform” for members with chronic illness: Web-based survey study of benefits arising. J. Med. Internet Res. 2018, 20, e175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, S.S.L.; Goonawardene, N. Internet health information seeking and the patient-physician relationship: A systematic review. J. Med. Internet Res. 2017, 19, e9. [Google Scholar] [CrossRef] [PubMed]
- An, L.C.; Wallner, L.; Kirch, M.A. Online Social Engagement by Cancer Patients: A Clinic-Based Patient Survey. JMIR Cancer 2016, 2, e10. [Google Scholar] [CrossRef] [Green Version]
- Bernell, S.; Howard, S.W. Use Your Words Carefully: What Is a Chronic Disease? Front. Public Heal. 2016, 4, 159. [Google Scholar] [CrossRef] [Green Version]
- Wicks, P.; Massagli, M.; Frost, J.; Brownstein, C.; Okun, S.; Vaughan, T.; Bradley, R.; Heywood, J. Sharing health data for better outcomes on patientslikeme. J. Med. Internet Res. 2010, 12, e19. [Google Scholar] [CrossRef] [Green Version]
- Sav, A.; Whitty, J.A.; McMillan, S.S.; Kendall, E.; Kelly, F.; King, M.A.; Wheeler, A.J. Treatment Burden and Chronic Illness: Who is at Most Risk? Patient 2016, 9, 559–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, X.L.; Zhou, Z.; Lee, M.K.O.; Cheung, C.M.K. Why users keep answering questions in online question answering communities: A theoretical and empirical investigation. Int. J. Inf. Manage. 2013, 33, 93–104. [Google Scholar] [CrossRef]
- Ma, W.W.K.; Chan, A. Knowledge sharing and social media: Altruism, perceived online attachment motivation, and perceived online relationship commitment. Comput. Human Behav. 2014, 39, 51–58. [Google Scholar] [CrossRef]
- Xu, A.; Bailey, B.P. What Do You Think? A Case Study of Benefit, Expectation, and Interaction in a Large Online Critique Community. In Proceedings of the ACM 2012 Conference on Computer Supported Cooperative Work, CSCW’12, Seattle, WA, USA, 11–15 February 2012. [Google Scholar]
- Jin, J.; Li, Y.; Zhong, X.; Zhai, L. Why users contribute knowledge to online communities: An empirical study of an online social Q&A community. Inf. Manag. 2015, 52, 840–849. [Google Scholar]
- Welbourne, J.L.; Blanchard, A.L.; Wadsworth, M.B. Motivations in virtual health communities and their relationship to community, connectedness and stress. Comput. Human Behav. 2013, 29, 129–139. [Google Scholar] [CrossRef]
- Hwang, M.I.; Thorn, R.G. The effect of user engagement on system success: A meta-analytical integration of research findings. Inf. Manag. 1999, 35, 229–236. [Google Scholar] [CrossRef]
- Di Gangi, P.M.; Wasko, M. Social media engagement theory: Exploring the infuence of user engagement on social media usage. J. Organ. End User Comput. 2016, 28, 53–73. [Google Scholar] [CrossRef] [Green Version]
- Calder, B.J.; Malthouse, E.C.; Schaedel, U. An Experimental Study of the Relationship between Online Engagement and Advertising Effectiveness. J. Interact. Mark. 2009, 23, 321–331. [Google Scholar] [CrossRef]
- Lo Presti, L.; Testa, M.; Marino, V.; Singer, P. Engagement in healthcare systems: Adopting digital tools for a sustainable approach. Sustainability 2019, 11, 220. [Google Scholar] [CrossRef] [Green Version]
- Brodie, R.J.; Hollebeek, L.D.; Jurić, B.; Ilić, A. Customer engagement: Conceptual domain, fundamental propositions, and implications for research. J. Serv. Res. 2011, 14, 252–271. [Google Scholar] [CrossRef]
- Breidbach, C.F.; Brodie, R.; Hollebeek, L. Beyond virtuality: From engagement platforms to engagement ecosystems. Manag. Serv. Qual. 2014, 24, 592–611. [Google Scholar] [CrossRef]
- Weiss, H.M.; Cropanzano, R. Affective Events Theory: A Theoretical Discussion of the Structure, Causes and Consequences of Affective Experiences at Work; Elsevier Science/JAI Press: Greenwich, CT, USA, 1996; Volume 18. [Google Scholar]
- Luo, M.M.; Chea, S. Cognitive appraisal of incident handling, affects, and post-adoption behaviors: A test of affective events theory. Int. J. Inf. Manage. 2018, 40, 120–131. [Google Scholar] [CrossRef]
- Luo, M.M.; Chea, S.; Bui, T.X. Post-adoption behavior of digital media: The merge of U&G theory and affect event theory. In Proceedings of the Pacific Asia Conference on Information Systems, PACIS 2016, Chiayi City, Taiwan, 27 June–1 July 2016. [Google Scholar]
- Wakefield, R.; Wakefield, K. Social media network behavior: A study of user passion and affect. J. Strateg. Inf. Syst. 2016, 25, 140–156. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68. [Google Scholar] [CrossRef]
- Huang, Y.C.; Backman, S.J.; Backman, K.F.; McGuire, F.A.; Moore, D.W. An investigation of motivation and experience in virtual learning environments: A self-determination theory. Educ. Inf. Technol. 2019, 24, 591–611. [Google Scholar] [CrossRef]
- Proulx, J.N.; Romero, M.; Arnab, S. Learning Mechanics and Game Mechanics Under the Perspective of Self-Determination Theory to Foster Motivation in Digital Game Based Learning. Simul. Gaming 2017, 48, 81–97. [Google Scholar] [CrossRef]
- Zhang, Y. Understanding the sustained use of online health communities from a self-determination perspective. J. Assoc. Inf. Sci. Technol. 2016, 67, 2842–2857. [Google Scholar] [CrossRef]
- Hagger, M.S.; Sultan, S.; Hardcastle, S.J.; Chatzisarantis, N.L.D. Perceived autonomy support and autonomous motivation toward mathematics activities in educational and out-of-school contexts is related to mathematics homework behavior and attainment. Contemp. Educ. Psychol. 2015, 41, 111–123. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.K.J.; Liu, W.C.; Kee, Y.H.; Chian, L.K. Competence, autonomy, and relatedness in the classroom: Understanding students’ motivational processes using the self-determination theory. Heliyon 2019, 5, e01983. [Google Scholar] [CrossRef] [Green Version]
- Fathali, S.; Okada, T. Technology acceptance model in technology-enhanced OCLL contexts: A self-determination theory approach. Australas. J. Educ. Technol. 2018, 34. [Google Scholar] [CrossRef] [Green Version]
- Gorozidis, G.S.; Tzioumakis, Y.S.; Krommidas, C.; Papaioannou, A.G. Facebook group PETCoN (Physical Education Teacher Collaborative Network). An innovative approach to PE teacher in-service training: A self-determination theory perspective. Teach. Teach. Educ. 2020, 96, 103184. [Google Scholar] [CrossRef]
- Wang, X.; Li, Y. Users’ Satisfaction with Social Network Sites: A Self-Determination Perspective. J. Comput. Inf. Syst. 2016, 56, 48–54. [Google Scholar] [CrossRef]
- Pijnenborg, G.H.M.; Spikman, J.M.; Jeronimus, B.F.; Aleman, A. Insight in schizophrenia: Associations with empathy. Eur. Arch. Psychiatry Clin. Neurosci. 2013, 263, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Oh, S. The characteristics and motivations of health answerers for sharing information, knowledge, and experiences in online environments. J. Am. Soc. Inf. Sci. Technol. 2012, 63, 543–557. [Google Scholar] [CrossRef]
- Ringle, C.M.; Wende, S.; Becker, J.M. SmartPLS 3; SmartPLS: Bönningstedt, Germany, 2015. [Google Scholar]
- Hair, J.F., Jr.; Sarstedt, M.; Hopkins, L.; Kuppelwieser, V.G. Partial least squares structural equation modeling (PLS-SEM). Eur. Bus. Rev. 2014, 26, 106–121. [Google Scholar] [CrossRef]
- Ryan, T.P. Sample Size Determination and Power; Wiley: Hoboken, NJ, USA, 2013; ISBN 9781118439241. [Google Scholar]
- Chin, W.W. The partial least squares approach for structural equation modeling. In Modern Methods for Business Research; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1998; ISBN 9780805826777. [Google Scholar]
- Hair, J.F.; Risher, J.J.; Sarstedt, M.; Ringle, C.M. When to use and how to report the results of PLS-SEM. Eur. Bus. Rev. 2019, 31, 2–24. [Google Scholar] [CrossRef]
- Benitez, J.; Henseler, J.; Castillo, A.; Schuberth, F. How to perform and report an impactful analysis using partial least squares: Guidelines for confirmatory and explanatory IS research. Inf. Manag. 2020, 57, 103168. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Tseng, F.C.; Kuo, F.Y. A study of social participation and knowledge sharing in the teachers’ online professional community of practice. Comput. Educ. 2014, 72, 37–47. [Google Scholar] [CrossRef]
- Zaglia, M.E. Brand communities embedded in social networks. J. Bus. Res. 2013, 66, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Abrahamson, K.; Anderson, J.G.; Ha, S.; Widdows, R. Trust, empathy, social identity, and contribution of knowledge within patient online communities. Behav. Inf. Technol. 2013, 32, 1041–1104. [Google Scholar] [CrossRef]
- Massimi, M.; Bender, J.; Witteman, H.O.; Ahmed, O.H. Life transitions and online health communities: Reflecting on adoption, use, and disengagement. In Proceedings of the ACM Conference on Computer Supported Cooperative Work, CSCW, Baltimore, MD, USA, 15–19 February 2014; pp. 1491–1501. [Google Scholar]
- Puspitasari, I.; Jie, F. Making the Information Technology (IT) Business Alignment Works: A Framework of IT-based Competitive Strategy. Int. J. Bus. Inf. Syst. 2020, 34, 59–82. [Google Scholar] [CrossRef]
- Zheng, J. SARS-coV-2: An emerging coronavirus that causes a global threat. Int. J. Biol. Sci. 2020, 16, 1678–1685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, D.; Wu, T.; Liu, Q.; Yang, Z. The SARS-CoV-2 outbreak: What we know. Int. J. Infect. Dis. 2020, 94, 44–48. [Google Scholar] [CrossRef]
- Dalager-Pedersen, M.; Bodilsen, J. Thromboprophylaxis for medical inpatients with coronavirus disease 2019. Clin. Microbiol. Infect. 2020, 26, 1125. [Google Scholar] [CrossRef]
Figure 1.
The research model based on the integration of affective events theory (AET) and self-determination theory (SDT).
Figure 1.
The research model based on the integration of affective events theory (AET) and self-determination theory (SDT).

Figure 2.
Results of the structural model (Note: ** p < 0.01, *** p < 0.001).

{kind=link}
{kind=link}
Table 1.
Demographics profile of the respondents.
| Category | n (%), N = 428 |
|---|---|
| Age group (in years) | |
| 18–30 | 46 (10.75) |
| 31–40 | 113 (26.40) |
| 41–50 | 174 (40.65) |
| 51–60 | 79 (18.46) |
| >60 | 16 (3.74) |
| Gender | |
| Male | 181 (42.29) |
| Female | 247 (57.71) |
| Role | |
| Patient | 263 (61.45) |
| Family | 121 (28.27) |
| Caregiver | 44 (10.28) |
| Frequency of Use | |
| Daily | 36 (8.41) |
| Weekly | 155 (36.21) |
| Monthly | 147 (34.35) |
| As the need arises | 90 (21.03) |
Table 2.
Construct, measurement item, loading factor, and average variance extracted (AVE).
| Construct | Indicator | Measurement Item (Survey’s Question) | Loading Factor | AVE |
|---|---|---|---|---|
| Interest to engage in a patient community | P1 | I joined a PSNS because I would like to help other patients with similar health conditions. | 0.887 | 0.731 |
| P2 | I am interested in sharing my experience and knowledge about specific health topics to others. | 0.931 | ||
| P3 | I am willing to go the extra mile to participate in a PSNS. | 0.736 | ||
| Empathy | E1 | I can feel the distress of other patients who have just been diagnosed with a disease. | 0.840 | 0.625 |
| E2 | I am willing to share my detailed experiences coping with a disease to support other patients. | 0.884 | ||
| E3 | I open myself more to others in a PSNS. | 0.712 | ||
| E4 | I enjoy participating and having good discussions via a PSNS. | 0.790 | ||
| E5 | It feels good to know that my contribution benefits others in a PSNS. | 0.712 | ||
| Use of patient social network systems | U1 | I frequently engage in a PSNS. | 0.775 | 0.606 |
| U2 | I intend to continue using a PSNS. | 0.823 | ||
| U3 | My interest to use a PSNS is high. | 0.735 |
Table 3.
Discriminant validity test and reliability test.
| Interest to Engage in a Patient Community | Empathy | Use of Patient Social Network Systems | Composite Reliability | |
|---|---|---|---|---|
| Interest to engage in a patient community | 0.855 | 0.890 | ||
| Empathy | 0.840 | 0.790 | 0.892 | |
| Use of patient social network systems | 0.625 | 0.645 | 0.778 | 0.821 |
Table 4.
Structural model evaluation.
| Assessment | Value |
|---|---|
| Coeeficient of determination | R2 |
| Empathy | 0.757 (substantial) |
| Use of patient social network systems | 0.476 (moderate) |
| The predictive sample reuse technique | Q2 |
| Empathy | 0.503 |
| Use of patient social network systems | 0.355 |
| Effect size | f2 |
| H1: Interest to engage in a patient community → Empathy | 1.114 |
| H2: Interest to engage in a patient community → Use of patient social network systems | 0.159 |
| H3: Empathy → Use of patient social network systems | 0.413 |
| H4: Empathy -> Interest to engage in a patient community → Use of patient social network systems | 0.182 |
| Relationships among the hypothesized constructs and observable variables | Path coefficient (p value), [T-value] |
| H1: Interest to engage in a patient community → Empathy | 0.870 (p < 0.001), [46.819] |
| H2: Interest to engage in a patient community → Use of patient social network systems | 0.366 (p < 0.001), [3.480] |
| H3: Empathy → Use of patient social network systems | 0.503 (p < 0.001), [5.529] |
| H4: Empathy → Interest to engage in a patient community → Use of patient social network systems | 0.169 (p < 0.001), [4.862] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Puspitasari, I.; Fauzi, S.S.M.; Ho, C.-Y. Factors Driving Users’ Engagement in Patient Social Network Systems. Informatics 2021, 8, 8. https://doi.org/10.3390/informatics8010008
AMA Style
Puspitasari I, Fauzi SSM, Ho C-Y. Factors Driving Users’ Engagement in Patient Social Network Systems. Informatics. 2021; 8(1):8. https://doi.org/10.3390/informatics8010008
Chicago/Turabian StylePuspitasari, Ira, Shukor Sanim Mohd Fauzi, and Cheng-Yuan Ho. 2021. "Factors Driving Users’ Engagement in Patient Social Network Systems" Informatics 8, no. 1: 8. https://doi.org/10.3390/informatics8010008
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.