Uninterrupted Dabigatran Administration Provides Greater Inhibition against Intracardiac Activation of Hemostasis as Compared to Vitamin K Antagonists during Cryoballoon Catheter Ablation of Atrial Fibrillation

 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Population
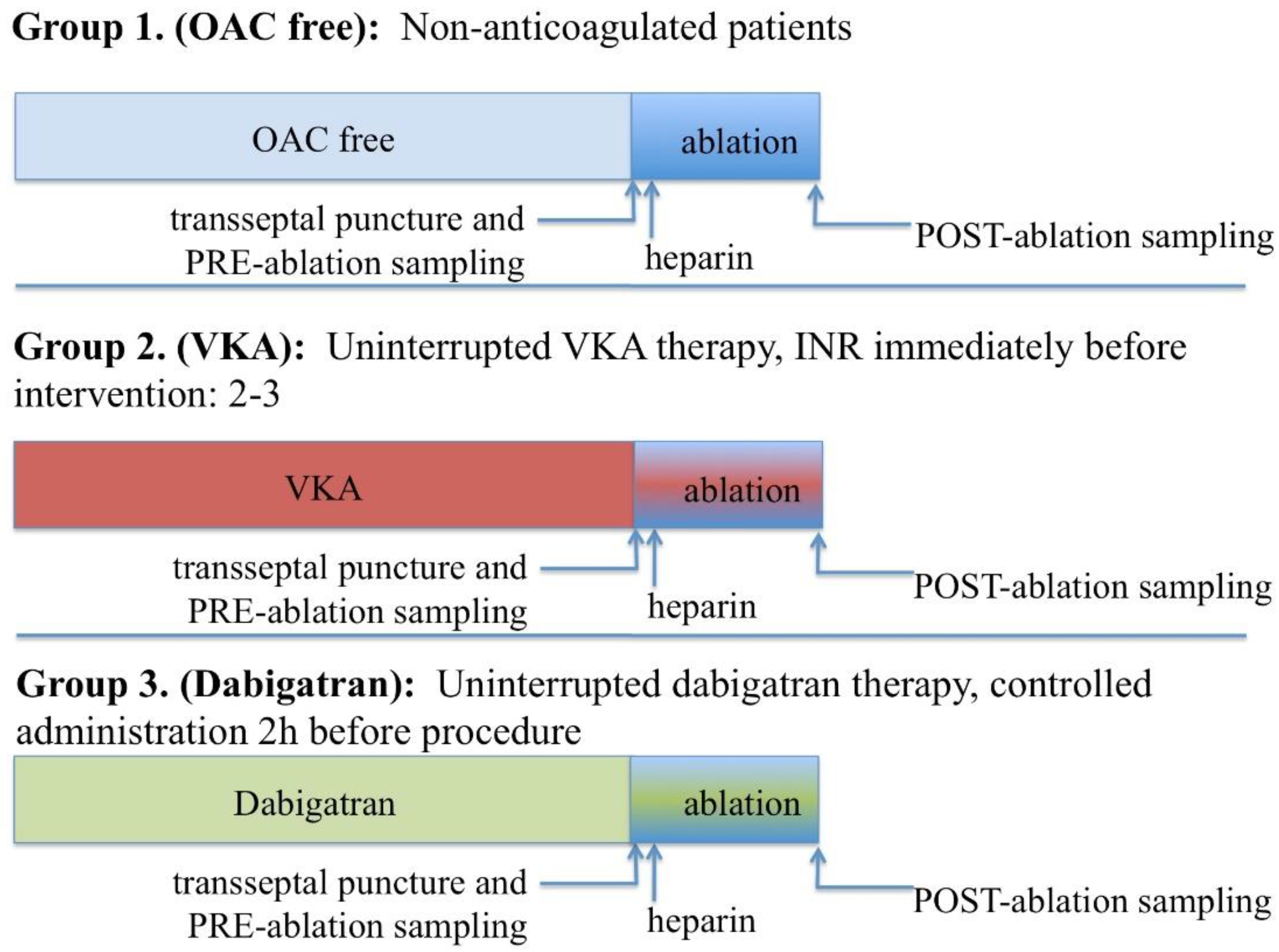
2.2. Pre-Procedure Anticoagulation and Ablation Procedure
- No anticoagulation (OAC free group). All patients on no anticoagulation were considered low risk for thromboembolism (CHA2DS2-VASC-score 0–2).
- Uninterrupted vitamin K antagonist for at least 30 days pre-ablation to maintain a therapeutic international normalised ratio (INR) between 2–3, which was confirmed on the morning of the procedure (VKA group). In case the morning INR level was measured out of the therapeutic range, ablation was postponed and VKA dose adjusted as required.
- Dabigatran 150 mg BID for at least 30 days with the last dose given 2 h prior to the procedure (Dabigatran group). Dabigatran was administered to all patients exactly 2 h before the scheduled start of the ablation, by the form of controlled pill intake as inspected by a nurse.
2.3. Blood Sampling and Laboratory Investigations
2.4. Statistical Analysis
3. Results
3.1. Baseline Patient and Procedure Characteristics
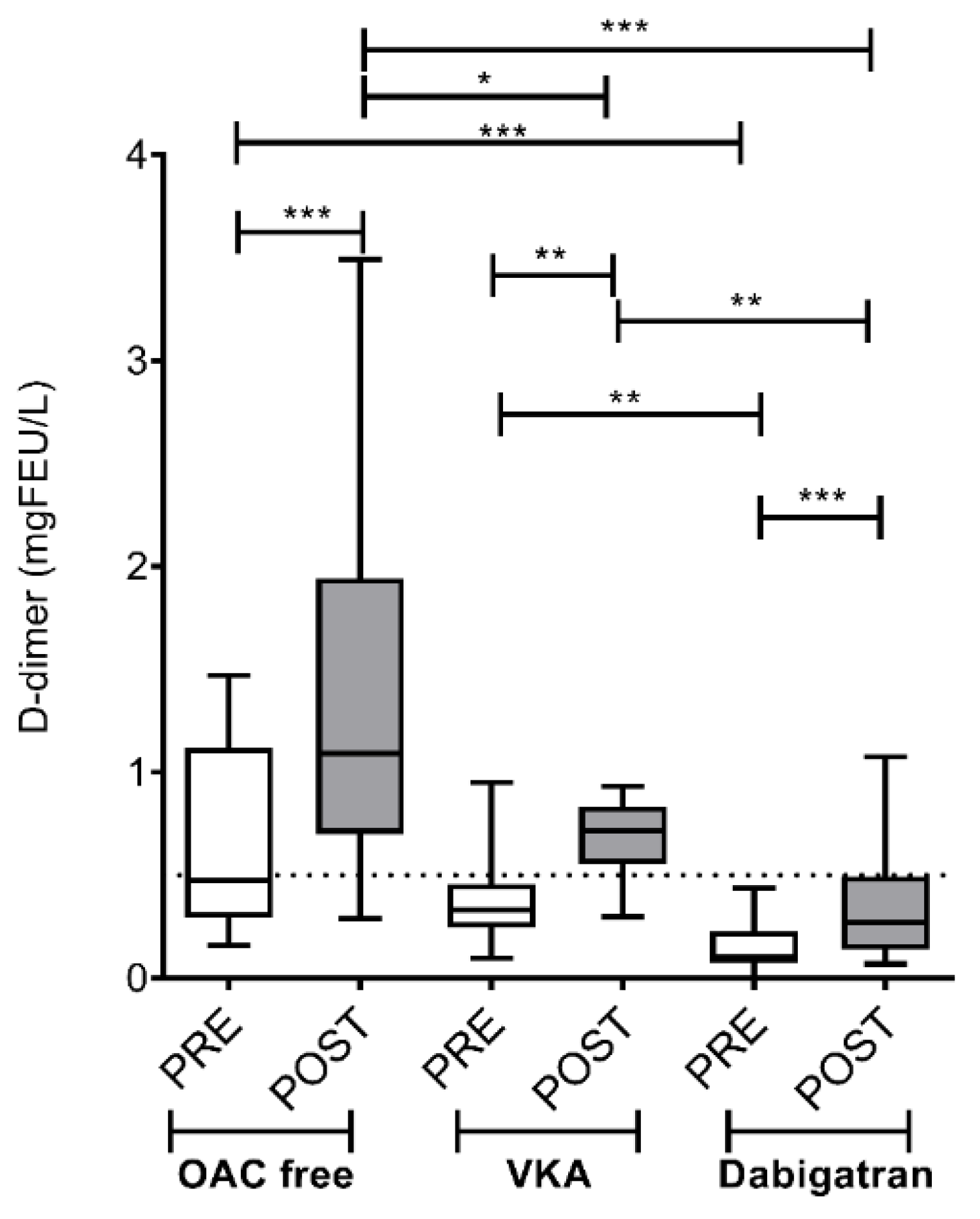
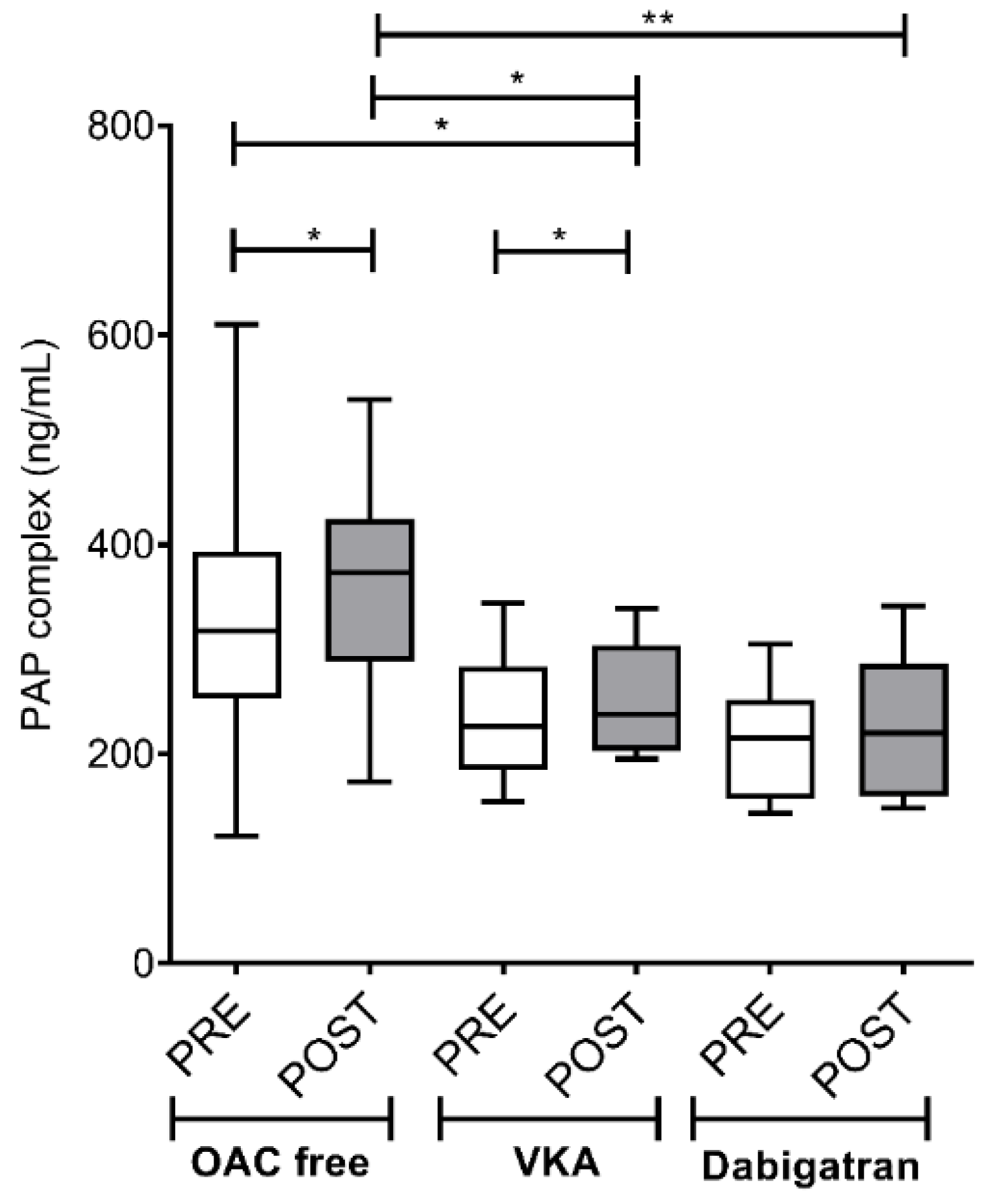
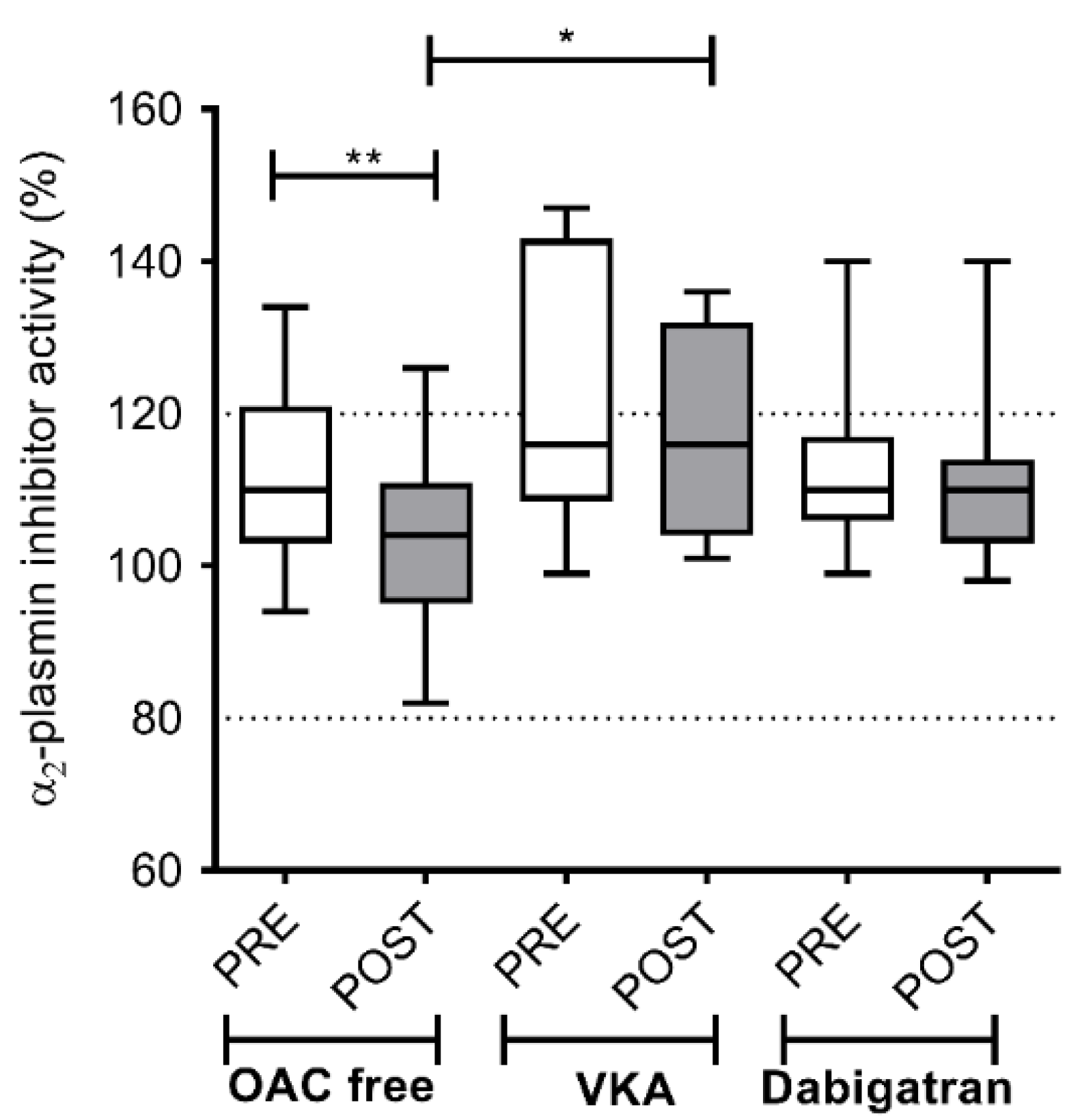
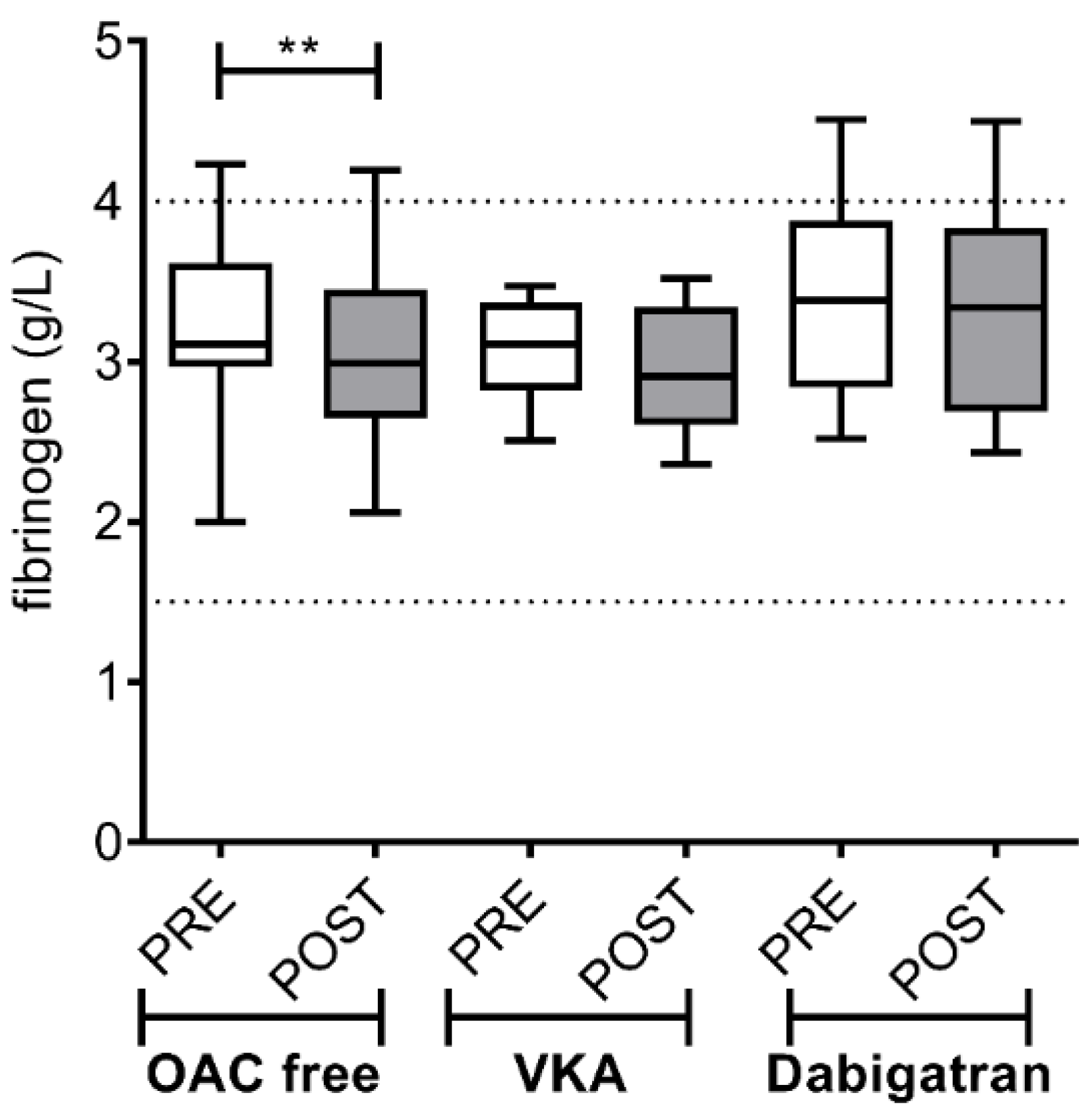
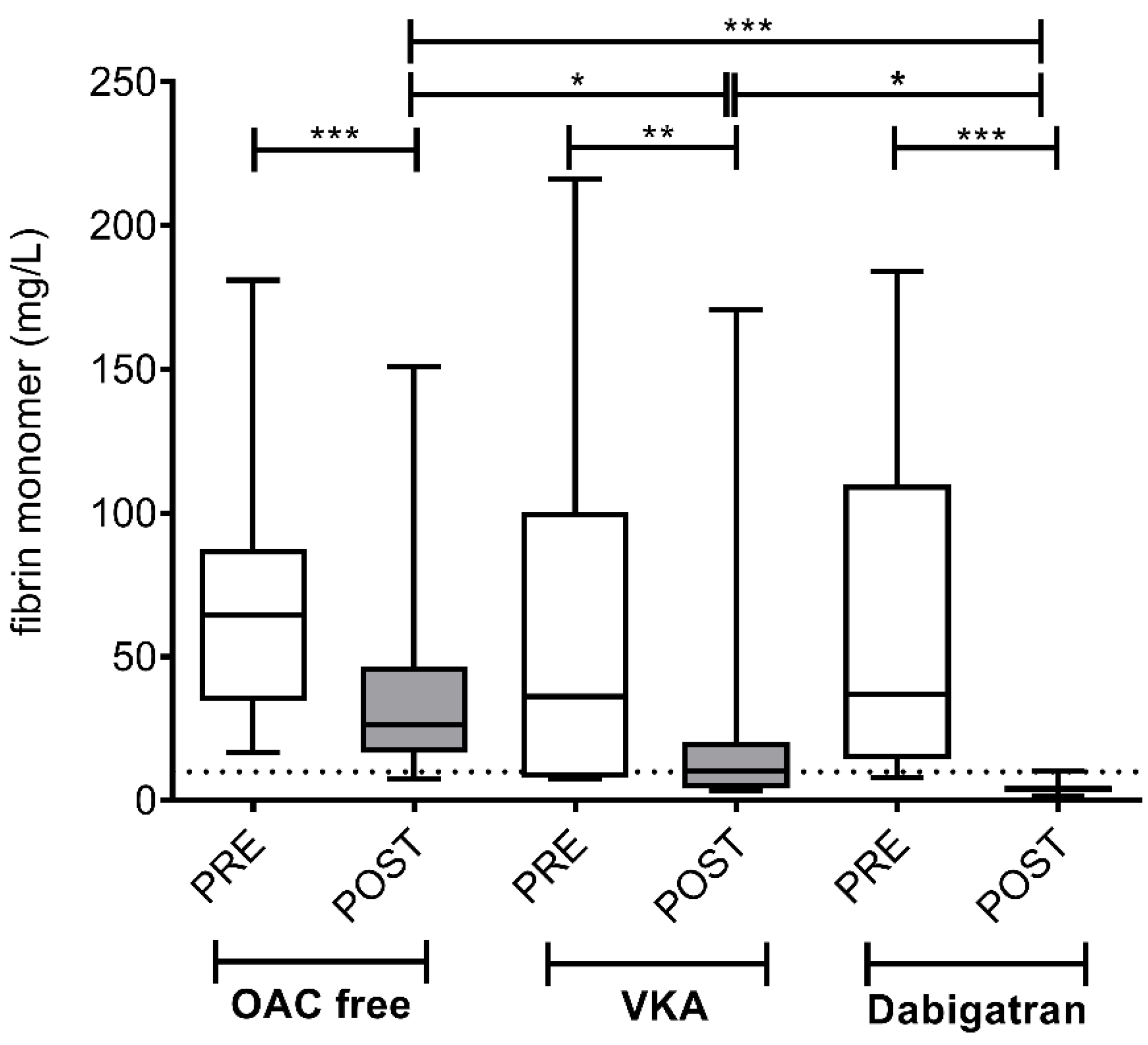
3.2. Intracardiac Activation of Hemostasis and Fibrinolysis in AF Patients before and after the Ablation Procedure: Effect of Different Pre-Procedural Anticoagulation Strategies
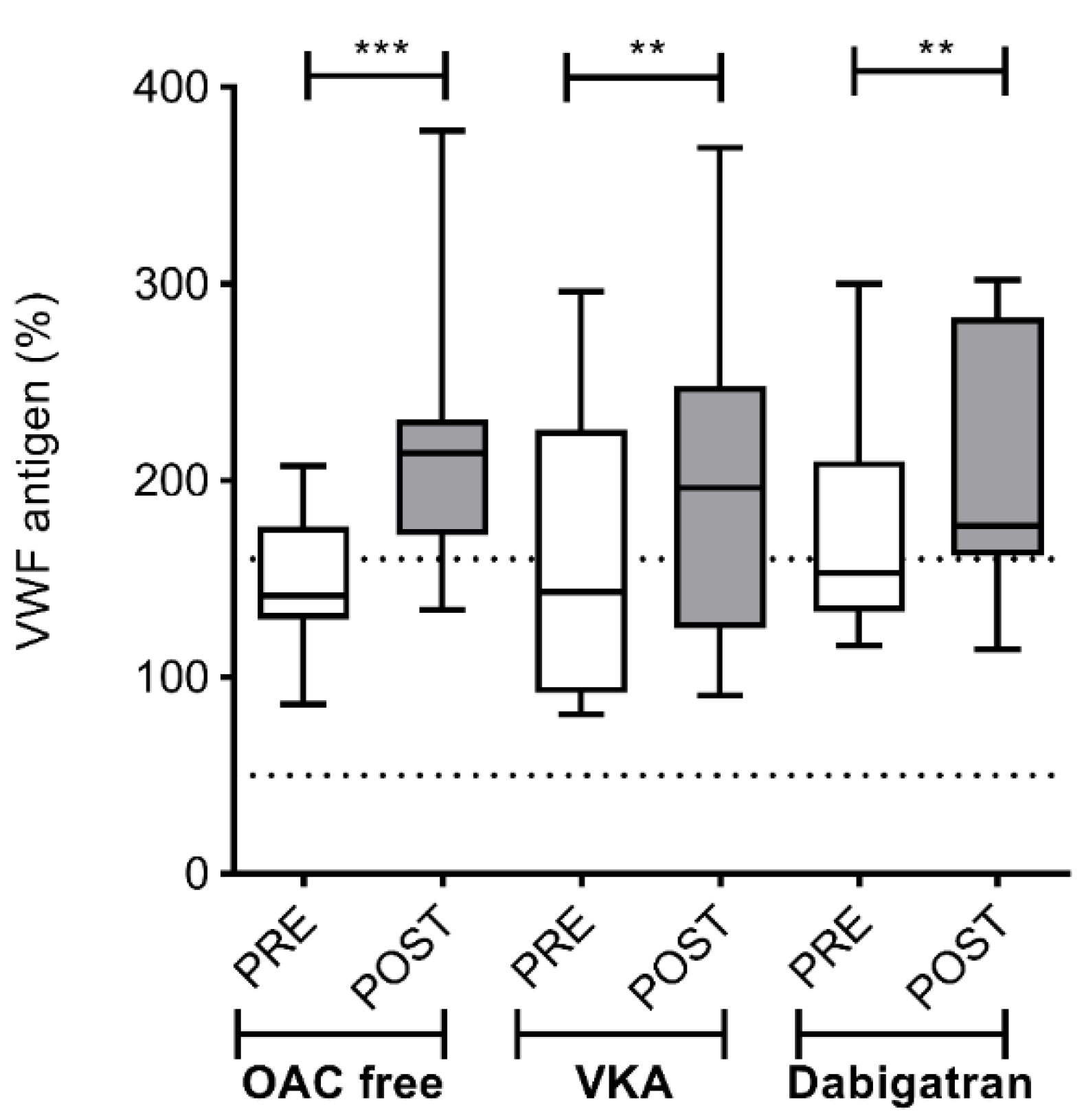
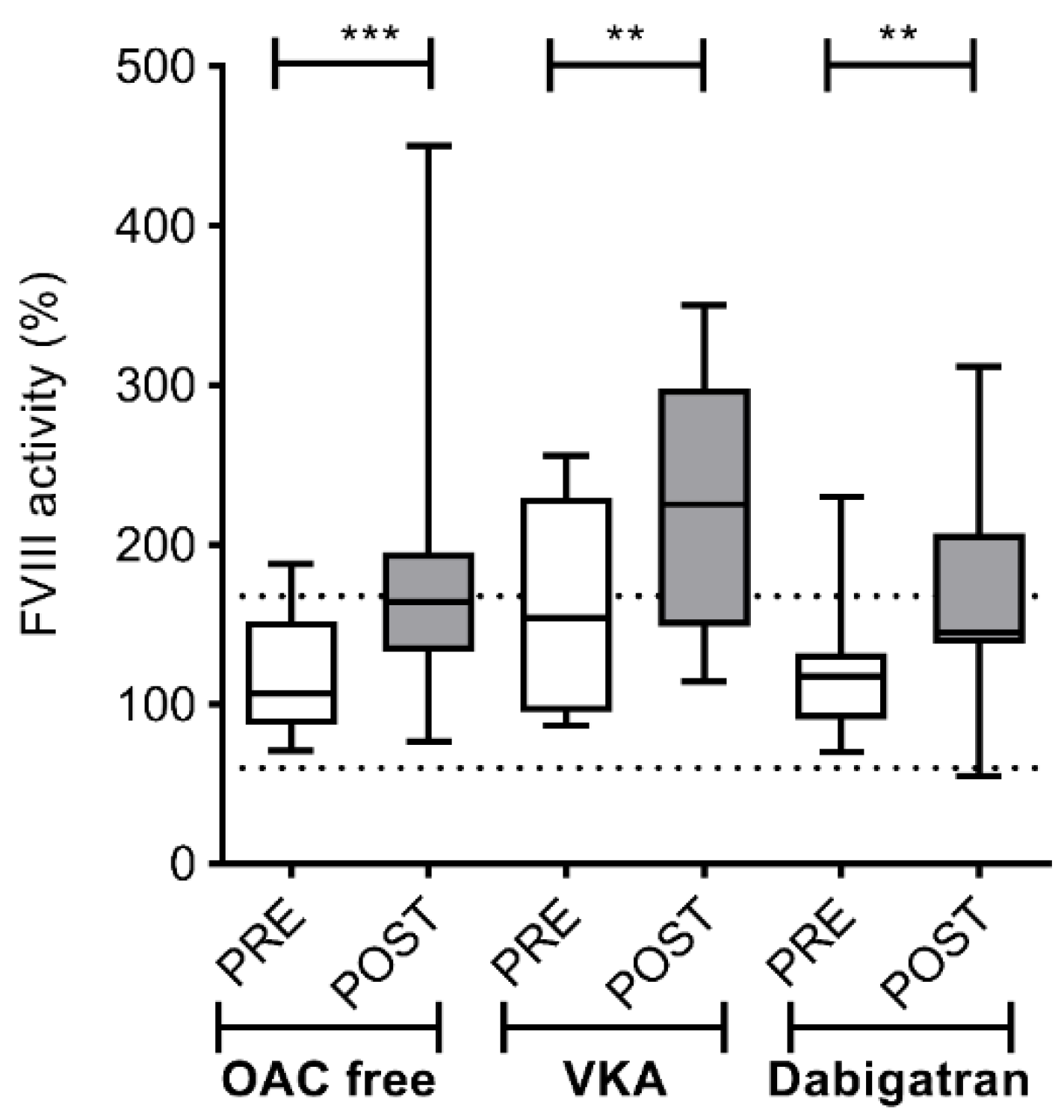
3.3. Local Endothelial Activation in the Left Atrium of AF Patients before and after the Ablation Procedure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.H.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm 2017, 14, e275–e444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuck, K.H.; Brugada, J.; Furnkranz, A.; Metzner, A.; Ouyang, F.; Chun, K.R.; Elvan, A.; Arentz, T.; Bestehorn, K.; Pocock, S.J.; et al. Cryoballoon or Radiofrequency Ablation for Paroxysmal Atrial Fibrillation. N. Engl. J. Med. 2016, 374, 2235–2245. [Google Scholar] [CrossRef] [PubMed]
- Aryana, A.; Singh, S.M.; Mugnai, G.; de Asmundis, C.; Kowalski, M.; Pujara, D.K.; Cohen, A.I.; Singh, S.K.; Fuenzalida, C.E.; Prager, N.; et al. Pulmonary vein reconnection following catheter ablation of atrial fibrillation using the second-generation cryoballoon versus open-irrigated radiofrequency: Results of a multicenter analysis. J. Interv. Card. Electrophysiol. 2016, 47, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Kuck, K.H.; Albenque, J.P.; Chun, K.J.; Furnkranz, A.; Busch, M.; Elvan, A.; Schluter, M.; Braegelmann, K.M.; Kueffer, F.J.; Hemingway, L.; et al. Repeat Ablation for Atrial Fibrillation Recurrence Post Cryoballoon or Radiofrequency Ablation in the FIRE AND ICE Trial. Circ. Arrhythm Electrophysiol. 2019, 12, e007247. [Google Scholar] [CrossRef] [PubMed]
- Hoyt, H.; Bhonsale, A.; Chilukuri, K.; Alhumaid, F.; Needleman, M.; Edwards, D.; Govil, A.; Nazarian, S.; Cheng, A.; Henrikson, C.A.; et al. Complications arising from catheter ablation of atrial fibrillation: Temporal trends and predictors. Heart Rhythm 2011, 8, 1869–1874. [Google Scholar] [CrossRef]
- Oral, H.; Chugh, A.; Ozaydin, M.; Good, E.; Fortino, J.; Sankaran, S.; Reich, S.; Igic, P.; Elmouchi, D.; Tschopp, D.; et al. Risk of thromboembolic events after percutaneous left atrial radiofrequency ablation of atrial fibrillation. Circulation 2006, 114, 759–765. [Google Scholar] [CrossRef] [Green Version]
- Lee, G.; Sparks, P.B.; Morton, J.B.; Kistler, P.M.; Vohra, J.K.; Medi, C.; Rosso, R.; Teh, A.; Halloran, K.; Kalman, J.M. Low risk of major complications associated with pulmonary vein antral isolation for atrial fibrillation: Results of 500 consecutive ablation procedures in patients with low prevalence of structural heart disease from a single center. J. Cardiovasc. Electrophysiol. 2011, 22, 163–168. [Google Scholar] [CrossRef]
- Aagaard, P.; Briceno, D.; Csanadi, Z.; Mohanty, S.; Gianni, C.; Trivedi, C.; Nagy-Balo, E.; Danik, S.; Barrett, C.; Santoro, F.; et al. Atrial Fibrillation Ablation and Stroke. Cardiol. Clin. 2016, 34, 307–316. [Google Scholar] [CrossRef]
- Wazni, O.M.; Beheiry, S.; Fahmy, T.; Barrett, C.; Hao, S.; Patel, D.; Di Biase, L.; Martin, D.O.; Kanj, M.; Arruda, M.; et al. Atrial fibrillation ablation in patients with therapeutic international normalized ratio: Comparison of strategies of anticoagulation management in the periprocedural period. Circulation 2007, 116, 2531–2534. [Google Scholar] [CrossRef]
- Di Biase, L.; Burkhardt, J.D.; Santangeli, P.; Mohanty, P.; Sanchez, J.E.; Horton, R.; Gallinghouse, G.J.; Themistoclakis, S.; Rossillo, A.; Lakkireddy, D.; et al. Periprocedural stroke and bleeding complications in patients undergoing catheter ablation of atrial fibrillation with different anticoagulation management: Results from the Role of Coumadin in Preventing Thromboembolism in Atrial Fibrillation (AF) Patients Undergoing Catheter Ablation (COMPARE) randomized trial. Circulation 2014, 129, 2638–2644. [Google Scholar] [CrossRef] [Green Version]
- Csanadi, Z.; Nagy-Balo, E.; Danik, S.; Barrett, C.; Burkhardt, J.D.; Sanchez, J.; Santangeli, P.; Santoro, F.; Di Biase, L.; Natale, A. Cerebrovascular Complications Related to Atrial Fibrillation Ablation and Strategies for Periprocedural Stroke Prevention. Card. Electrophysiol. Clin. 2014, 6, 111–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cappato, R.; Marchlinski, F.E.; Hohnloser, S.H.; Naccarelli, G.V.; Xiang, J.; Wilber, D.J.; Ma, C.S.; Hess, S.; Wells, D.S.; Juang, G.; et al. Uninterrupted rivaroxaban vs. uninterrupted vitamin K antagonists for catheter ablation in non-valvular atrial fibrillation. Eur. Heart J. 2015, 36, 1805–1811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Biase, L.; Lakkireddy, D.; Trivedi, C.; Deneke, T.; Martinek, M.; Mohanty, S.; Mohanty, P.; Prakash, S.; Bai, R.; Reddy, M.; et al. Feasibility and safety of uninterrupted periprocedural apixaban administration in patients undergoing radiofrequency catheter ablation for atrial fibrillation: Results from a multicenter study. Heart Rhythm 2015, 12, 1162–1168. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Haeusler, K.G.; Blank, B.; De Bono, J.; Callans, D.; Elvan, A.; Fetsch, T.; Van Gelder, I.C.; Gentlesk, P.; Grimaldi, M.; et al. Apixaban in patients at risk of stroke undergoing atrial fibrillation ablation. Eur. Heart J. 2018, 39, 2942–2955. [Google Scholar] [CrossRef] [Green Version]
- Hohnloser, S.H.; Camm, J.; Cappato, R.; Diener, H.C.; Heidbuchel, H.; Mont, L.; Morillo, C.A.; Abozguia, K.; Grimaldi, M.; Rauer, H.; et al. Uninterrupted edoxaban vs. vitamin K antagonists for ablation of atrial fibrillation: The ELIMINATE-AF trial. Eur. Heart J. 2019, 40, 3013–3021. [Google Scholar] [CrossRef]
- Lakkireddy, D.; Reddy, Y.M.; Di Biase, L.; Vanga, S.R.; Santangeli, P.; Swarup, V.; Pimentel, R.; Mansour, M.C.; D’Avila, A.; Sanchez, J.E.; et al. Feasibility and safety of dabigatran versus warfarin for periprocedural anticoagulation in patients undergoing radiofrequency ablation for atrial fibrillation: Results from a multicenter prospective registry. J. Am. Coll. Cardiol. 2012, 59, 1168–1174. [Google Scholar] [CrossRef] [Green Version]
- Calkins, H.; Willems, S.; Gerstenfeld, E.P.; Verma, A.; Schilling, R.; Hohnloser, S.H.; Okumura, K.; Serota, H.; Nordaby, M.; Guiver, K.; et al. Uninterrupted Dabigatran versus Warfarin for Ablation in Atrial Fibrillation. N. Engl. J. Med. 2017, 376, 1627–1636. [Google Scholar] [CrossRef] [Green Version]
- Nogami, A.; Harada, T.; Sekiguchi, Y.; Otani, R.; Yoshida, Y.; Yoshida, K.; Nakano, Y.; Nuruki, N.; Nakahara, S.; Goya, M.; et al. Safety and Efficacy of Minimally Interrupted Dabigatran vs Uninterrupted Warfarin Therapy in Adults Undergoing Atrial Fibrillation Catheter Ablation: A Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e191994. [Google Scholar] [CrossRef]
- Akar, J.G.; Jeske, W.; Wilber, D.J. Acute onset human atrial fibrillation is associated with local cardiac platelet activation and endothelial dysfunction. J. Am. Coll. Cardiol. 2008, 51, 1790–1793. [Google Scholar] [CrossRef] [Green Version]
- Willoughby, S.R.; Roberts-Thomson, R.L.; Lim, H.S.; Schultz, C.; Prabhu, A.; De Sciscio, P.; Wong, C.X.; Worthley, M.I.; Sanders, P. Atrial platelet reactivity in patients with atrial fibrillation. Heart Rhythm 2010, 7, 1178–1183. [Google Scholar] [CrossRef]
- Toth, N.K.; Csanadi, Z.; Hajas, O.; Kiss, A.; Nagy-Balo, E.; Kovacs, K.B.; Sarkady, F.; Muszbek, L.; Bereczky, Z.; Csiba, L.; et al. Intracardiac Hemostasis and Fibrinolysis Parameters in Patients with Atrial Fibrillation. BioMed Res. Int. 2017, 2017, 3678017. [Google Scholar] [CrossRef] [PubMed]
- Hajas, O.; Bagoly, Z.; Toth, N.K.; Urbancsek, R.; Kiss, A.; Kovacs, K.B.; Sarkady, F.; Nagy, A.; Olah, A.V.; Nagy, L.; et al. Intracardiac Fibrinolysis and Endothelium Activation Related to Atrial Fibrillation Ablation with Different Techniques. Cardiol. Res. Pract. 2020, 2020, 1570483. [Google Scholar] [CrossRef] [PubMed]
- Bereczky, Z.; Olah, Z.; Ajzner, E.; Kappelmayer, J. [Laboratory aspects of novel oral anticoagulant treatment]. Orv. Hetil. 2017, 158, 1930–1945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shainoff, J.R.; DiBello, P.M. The circulatory half-lives of alpha-profibrin and alpha-fibrin monomer, and comparisons with other fibrin(ogen) derivatives. Thromb. Haemost. 2003, 89, 48–52. [Google Scholar]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [Green Version]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [Green Version]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef]
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Spinar, J.; et al. Edoxaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OAC Free (n = 24) | VKA (n = 11) | Dabigatran (n = 17) | p | |
|---|---|---|---|---|
| Age (years) | 51.2 ± 12.6 | 58.3 ± 10.8 | 56.3 ± 10.2 | 0.240 |
| Male, n (%) | 15 (62.5) | 8 (72.7) | 11 (64.7) | 0.838 |
| BMI (kg/m2) | 29.03 (26.68–31.49) | 29.02 (28.35–31.47) | 26.88 (24.89–30.93) | 0.558 |
| Hypertension n (%) | 13 (54.2) | 7 (63.6) | 10 (58.89) | 0.489 |
| Hypercholesterolemia n (%) | 13 (54.2) | 8 (72.7) | 7 (63.6) | 0.112 |
| Smoking n (%) | 7 (29.2) | 2 (18.2) | 4 (23.5) | 0.479 |
| Diabetes mellitus n (%) | 1 (4.2) | 2 (18.2) | 1 (5.9) | 0.386 |
| Left atrium size (mm) | 40.54 ± 5.4 | 42.30 ± 3.30 | 41.3 ± 3.6 | 0.597 |
| Left ventricular ejection fraction (%) | 57.38 ± 5.9 | 60.80 ± 8.04 | 55.93 ± 6.77 | 0.228 |
| CHA2DS2-VASC, median (IQR) | 1 (0–2) | 1 (0–3) | 1 (0–2) | 0.780 |
| INR before intervention | 0.96 ± 0.05 | 2.33 ± 0.32 | 1.18 ± 0.09 | <0.001 |
| Dabigatran peak (ng/mL), median (range) | - | - | 165.6 (70.6–331.9) | - |
| hsCRP (mg/L), median (IQR) | 1.4 (0.5–2.5) | 1.0 (0.5–2.5) | 1.7 (0.8–4.6) | 0.338 |
| Duration of the procedure (min) | 70.08 ± 15.7 | 78.9 ± 33.7 | 65.5 ± 22.8 | 0.155 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagoly, Z.; Hajas, O.; Urbancsek, R.; Kiss, A.; Fiak, E.; Sarkady, F.; Tóth, N.K.; Orbán-Kálmándi, R.; Kovács, K.B.; Nagy, L.; et al. Uninterrupted Dabigatran Administration Provides Greater Inhibition against Intracardiac Activation of Hemostasis as Compared to Vitamin K Antagonists during Cryoballoon Catheter Ablation of Atrial Fibrillation. J. Clin. Med. 2020, 9, 3050. https://doi.org/10.3390/jcm9093050
Bagoly Z, Hajas O, Urbancsek R, Kiss A, Fiak E, Sarkady F, Tóth NK, Orbán-Kálmándi R, Kovács KB, Nagy L, et al. Uninterrupted Dabigatran Administration Provides Greater Inhibition against Intracardiac Activation of Hemostasis as Compared to Vitamin K Antagonists during Cryoballoon Catheter Ablation of Atrial Fibrillation. Journal of Clinical Medicine. 2020; 9(9):3050. https://doi.org/10.3390/jcm9093050
Chicago/Turabian StyleBagoly, Zsuzsa, Orsolya Hajas, Réka Urbancsek, Alexandra Kiss, Edit Fiak, Ferenc Sarkady, Noémi Klára Tóth, Rita Orbán-Kálmándi, Kitti Bernadett Kovács, László Nagy, and et al. 2020. "Uninterrupted Dabigatran Administration Provides Greater Inhibition against Intracardiac Activation of Hemostasis as Compared to Vitamin K Antagonists during Cryoballoon Catheter Ablation of Atrial Fibrillation" Journal of Clinical Medicine 9, no. 9: 3050. https://doi.org/10.3390/jcm9093050