Local and Widespread Pressure Pain Hyperalgesia Is Not Side Specific in Females with Unilateral Neck Pain that Can Be Reproduced during Passive Neck Rotation

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
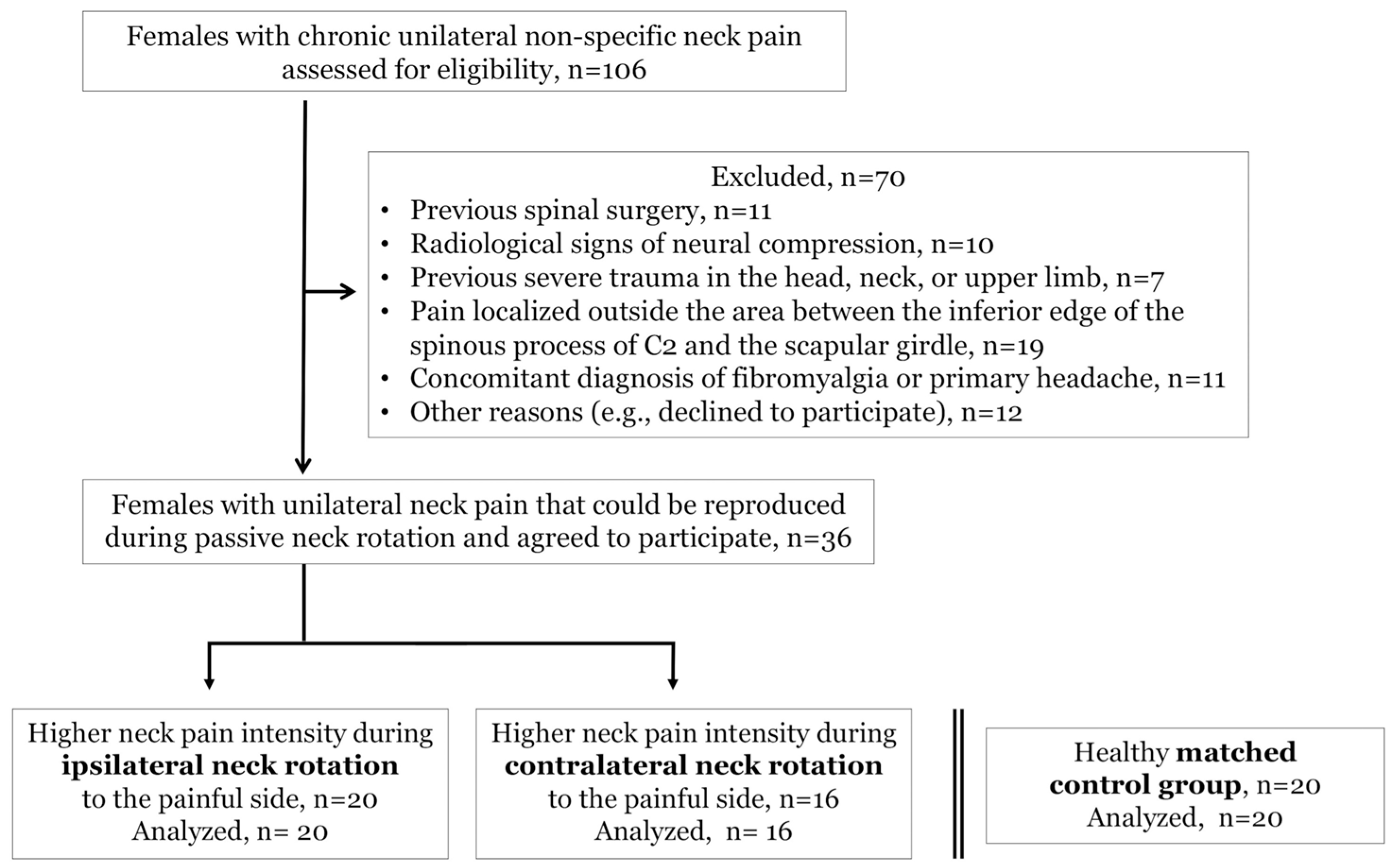
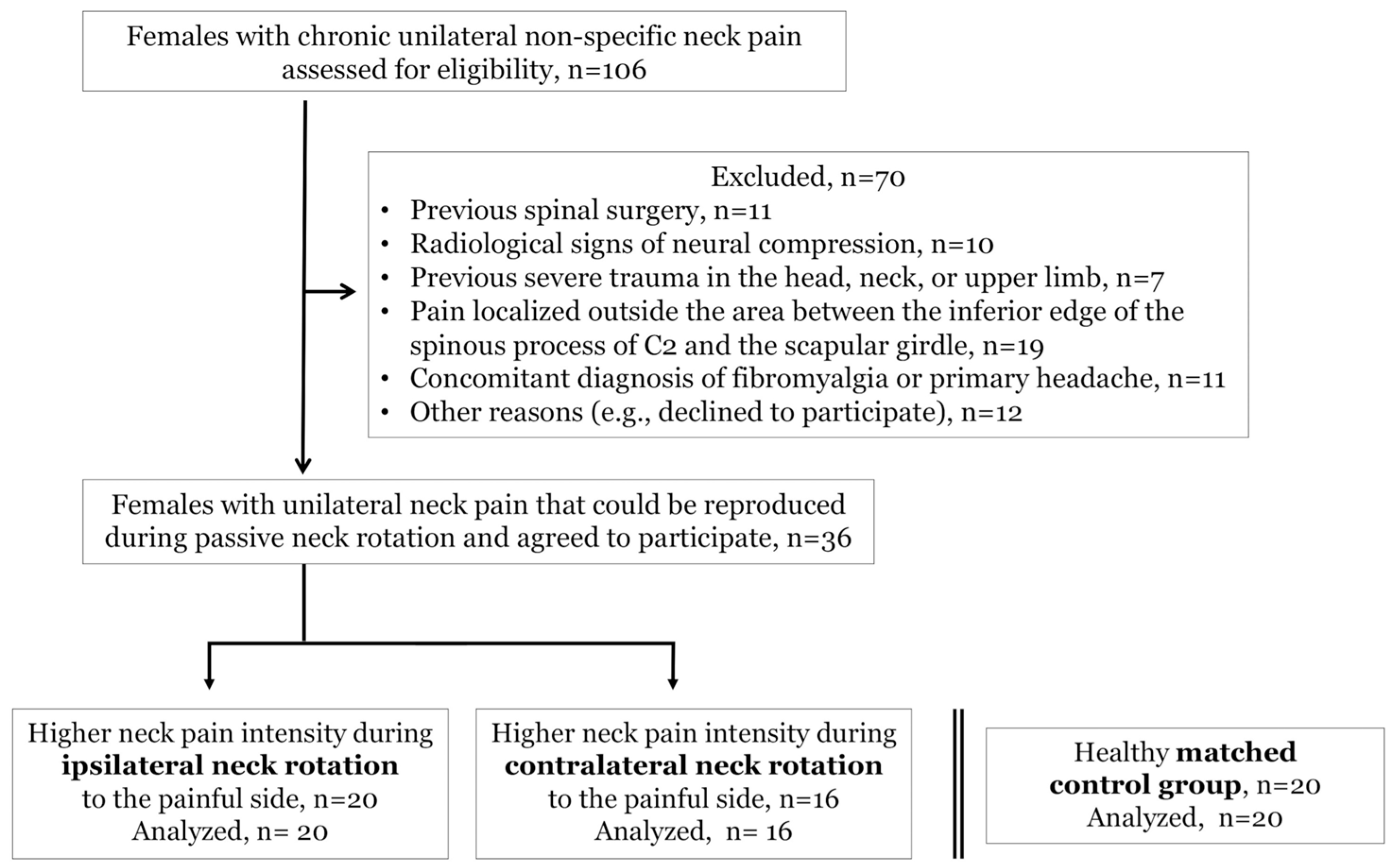
2.2. Participants
2.3. Study Protocol
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Pressure Pain Sensitivity in Females with and without Unilateral Non-Specific Neck Pain
4.2. Pressure Pain Sensitivity in Females with Unilateral Non-Specific Neck Pain
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fejer, R.; Kyvik, K.O.; Hartvigsen, J. The prevalence of neck pain in the world population: A systematic critical review of the literature. Eur. Spine J. 2006, 15, 834–848. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, A.; Coggeshall, M. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef]
- Driessen, M.T.; Lin, C.W.; van Tulder, M.W. Cost-effectiveness of conservative treatments for neck pain: A systematic review on economic evaluations. Eur. Spine J. 2012, 21, 1441–1450. [Google Scholar] [CrossRef] [PubMed]
- Merskey, H.E. Classification of chronic pain. Descriptions of chronic pain syndromes and definitions of pain terms. Pain Suppl. 1986, 3, S1–S226. [Google Scholar]
- Walton, D.M.; Kwok, T.S.; Mehta, S.; Loh, E.; Smith, A.; Elliott, J.; Kamper, S.J.; Kasch, H.; Sterling, M. Cluster analysis of an international pressure pain threshold database identifies 4 meaningful subgroups of adults with mechanical neck pain. Clin. J. Pain 2017, 33, 422–428. [Google Scholar] [CrossRef]
- Malfliet, A.; Kregel, J.; Cagnie, B.; Kuipers, M.; Dolphens, M.; Roussel, N.; Meeus, M.; Danneels, L.; Bramer, W.M.; Nijs, J. Lack of evidence for central sensitization in idiopathic, non-traumatic neck pain: A systematic review. Pain Physician 2015, 18, 223–236. [Google Scholar] [PubMed]
- Neziri, A.Y.; Limacher, A.; Jüni, P.; Radanov, B.P.; Andersen, O.K.; Arendt-Nielsen, L.; Curatolo, M. Ranking of tests for pain hypersensitivity according to their discriminative ability in chronic neck pain. Reg. Anesth. Pain Med. 2013, 38, 308–320. [Google Scholar] [CrossRef]
- Walton, D.M.; Macdermid, J.C.; Nielson, W.; Teasell, R.W.; Reese, H.; Levesque, L. Pressure pain threshold testing demonstrates predictive ability in people with acute whiplash. J. Orthop. Sports Phys. Ther. 2011, 41, 658–665. [Google Scholar] [CrossRef]
- O’Leary, H.; Smart, K.M.; Moloney, N.A.; Blake, C.; Doody, C.M. Pain sensitization associated with nonresponse after physiotherapy in people with knee osteoarthritis. Pain 2018, 159, 1877–1886. [Google Scholar] [CrossRef]
- Bartley, E.J.; Fillingim, R.B. Sex differences in pain: A brief review of clinical and experimental findings. Br. J. Anaesth. 2013, 111, 52–58. [Google Scholar] [CrossRef]
- Binderup, A.T.; Arendt-Nielsen, L.; Madeleine, P. Pressure pain sensitivity maps of the neck-shoulder and the low back regions in men and women. BMC Musculoskelet. Disord. 2010, 11, 234. [Google Scholar] [CrossRef]
- Vaegter, H.B.; Palsson, T.S.; Graven-Nielsen, T. Facilitated pronociceptive pain mechanisms in radiating back pain compared with localized back pain. J. Pain 2017, 18, 973–983. [Google Scholar] [CrossRef] [PubMed]
- Javanshir, K.; Ortega-Santiago, R.; Mohseni-Bandpei, M.A.; Miangolarra-Page, J.C.; Fernández-de-Las-Peñas, C. Exploration of somatosensory impairments in subjects with mechanical idiopathic neck pain: A preliminary study. J. Manipulative Physiol. Ther. 2010, 33, 493–499. [Google Scholar] [CrossRef]
- Zaproudina, N.; Ming, Z.; Närhi, M. Sensory and sympathetic disorders in chronic non-specific neck pain. Funct. Neurol. 2015, 30, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Rose, S.J. Physical therapy diagnosis: Role and function. Phys. Ther. 1989, 69, 535–537. [Google Scholar] [CrossRef] [PubMed]
- Waeyaert, P.; Jansen, D.; Bastiaansen, M.; Scafoglieri, A.; Buyl, R.; Schmitt, M.; Cattrysse, E. Three-dimensional cervical movement characteristics in healthy subjects and subgroups of chronic neck pain patients based on their pain location. Spine 2016, 41, 908–914. [Google Scholar] [CrossRef]
- Lee, H.; Nicholoson, L.L.; Adams, R.D.; Bae, S.S. Body chart pain location and side-specific physical impairment in subclinical neck pain. J. Manipulative Physiol. Ther. 2005, 28, 479–486. [Google Scholar] [CrossRef]
- Childs, J.D.; Cleland, J.A.; Elliott, J.M.; Teyhen, D.S.; Wainner, R.S.; Whitman, J.M.; Sopky, B.J.; Godges, J.J.; Flynn, T.W.; Association, A.P.T. Neck pain: Clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopedic Section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2008, 38, A1–A34. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.; Miller, J.; D’Sylva, J.; Burnie, S.J.; Goldsmith, C.H.; Graham, N.; Haines, T.; Brønfort, G.; Hoving, J.L. Manipulation or mobilisation for neck pain. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef]
- Karayannis, N.V.; Jull, G.A.; Hodges, P.W. Physiotherapy movement based classification approaches to low back pain: Comparison of subgroups through review and developer/expert survey. BMC Musculoskelet. Disord. 2012, 13, 24. [Google Scholar] [CrossRef]
- Lascurain-Aguirrebeña, I.; Newham, D.J.; Galarraga-Gallastegui, B.; Critchley, D.J. Differences in neck surface electromyography, kinematics and pain occurrence during physiological neck movements between neck pain and asymptomatic participants. A cross-sectional study. Clin. Biomech. (Bristol, Avon) 2018, 57, 1–9. [Google Scholar] [CrossRef]
- Petersen, S.M.; Wyatt, S.N. Lower trapezius muscle strength in individuals with unilateral neck pain. J. Orthop. Sports Phys. Ther. 2011, 41, 260–265. [Google Scholar] [CrossRef]
- Côté, P.; van der Velde, G.; Cassidy, J.D.; Carroll, L.J.; Hogg-Johnson, S.; Holm, L.W.; Carragee, E.J.; Haldeman, S.; Nordin, M.; Hurwitz, E.L.; et al. The burden and determinants of neck pain in workers: Results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Spine 2008, 33, S60–S74. [Google Scholar] [CrossRef]
- Bogduk, N. Neck pain. Aust. Fam. Physician 1984, 13, 26–30. [Google Scholar]
- Lluch, E.; Arguisuelas, M.D.; Coloma, P.S.; Palma, F.; Rey, A.; Falla, D. Effects of deep cervical flexor training on pressure pain thresholds over myofascial trigger points in patients with chronic neck pain. J. Manipulative Physiol. Ther. 2013, 36, 604–611. [Google Scholar] [CrossRef]
- La Touche, R.; Fernández-de-Las-Peñas, C.; Fernández-Carnero, J.; Díaz-Parreño, S.; Paris-Alemany, A.; Arendt-Nielsen, L. Bilateral mechanical-pain sensitivity over the trigeminal region in patients with chronic mechanical neck pain. J. Pain 2010, 11, 256–263. [Google Scholar] [CrossRef]
- Puentedura, E.J.; Landers, M.R.; Cleland, J.A.; Mintken, P.E.; Huijbregts, P.; Fernández-de-Las-Peñas, C. Thoracic spine thrust manipulation versus cervical spine thrust manipulation in patients with acute neck pain: A randomized clinical trial. J. Orthop. Sports Phys. Ther. 2011, 41, 208–220. [Google Scholar] [CrossRef]
- Siegenthaler, A.; Eichenberger, U.; Schmidlin, K.; Arendt-Nielsen, L.; Curatolo, M. What does local tenderness say about the origin of pain? An investigation of cervical zygapophysial joint pain. Anesth. Analg. 2010, 110, 923–927. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; de la Llave-Rincón, A.I.; Fernández-Carnero, J.; Cuadrado, M.L.; Arendt-Nielsen, L.; Pareja, J.A. Bilateral widespread mechanical pain sensitivity in carpal tunnel syndrome: Evidence of central processing in unilateral neuropathy. Brain 2009, 132, 1472–1479. [Google Scholar] [CrossRef]
- Beltran-Alacreu, H.; López-de-Uralde-Villanueva, I.; Calvo-Lobo, C.; Fernández-Carnero, J.; Touche, R. Clinical features of patients with chronic non-specific neck pain per disability level: A novel observational study. Rev. Assoc. Med. Bras. (1992) 2018, 64, 700–709. [Google Scholar] [CrossRef] [Green Version]
- Chess, L.E.; Gagnier, J. Risk of bias of randomized controlled trials published in orthopaedic journals. BMC Med. Res. Methodol. 2013, 13, 76. [Google Scholar] [CrossRef]
- Wan, A.K.; Rainville, P.; O’Leary, S.; Elphinston, R.A.; Sterling, M.; Larivière, C.; Sullivan, M.J.L. Validation of an index of sensitivity to movement-evoked pain in patients with whiplash injuries. Pain Rep. 2018, 3, e661. [Google Scholar] [CrossRef]
- Andrade Ortega, J.A.; Delgado Martínez, A.D.; Almécija Ruiz, R. Validation of the Spanish version of the Neck Disability Index. Spine 2010, 35, E114–E118. [Google Scholar] [CrossRef]
- MacDermid, J.C.; Walton, D.M.; Avery, S.; Blanchard, A.; Etruw, E.; McAlpine, C.; Goldsmith, C.H. Measurement properties of the neck disability index: A systematic review. J. Orthop. Sports Phys. Ther. 2009, 39, 400–417. [Google Scholar] [CrossRef]
- Vanderweeën, L.; Oostendorp, R.A.; Vaes, P.; Duquet, W. Pressure algometry in manual therapy. Man. Ther. 1996, 1, 258–265. [Google Scholar] [CrossRef]
- Chesterton, L.S.; Sim, J.; Wright, C.C.; Foster, N.E. Interrater reliability of algometry in measuring pressure pain thresholds in healthy humans, using multiple raters. Clin. J. Pain 2007, 23, 760–766. [Google Scholar] [CrossRef]
- Ylinen, J.; Nykänen, M.; Kautiainen, H.; Häkkinen, A. Evaluation of repeatability of pressure algometry on the neck muscles for clinical use. Man. Ther. 2007, 12, 192–197. [Google Scholar] [CrossRef]
- Hidalgo-Lozano, A.; Fernández-de-las-Peñas, C.; Calderón-Soto, C.; Domingo-Camara, A.; Madeleine, P.; Arroyo-Morales, M. Elite swimmers with and without unilateral shoulder pain: Mechanical hyperalgesia and active/latent muscle trigger points in neck-shoulder muscles. Scand. J. Med. Sci. Sports 2013, 23, 66–73. [Google Scholar] [CrossRef]
- Simons, D.; Travell, J.; Simons, L. Myofascial pain and dysfunction: The trigger point manual, 2nd ed.; Williams & Wilkins: Baltimore, MD, USA, 1999. [Google Scholar]
- Stokes, M.; Hides, J.; Elliott, J.; Kiesel, K.; Hodges, P. Rehabilitative ultrasound imaging of the posterior paraspinal muscles. J. Orthop. Sports Phys. Ther. 2007, 37, 581–595. [Google Scholar] [CrossRef]
- Johnston, V.; Jimmieson, N.L.; Jull, G.; Souvlis, T. Quantitative sensory measures distinguish office workers with varying levels of neck pain and disability. Pain 2008, 137, 257–265. [Google Scholar] [CrossRef]
- Pedersini, P.; Negrini, S.; Cantero-Tellez, R.; Bishop, M.D.; Villafañe, J.H. Pressure algometry and palpation of the upper limb peripheral nervous system in subjects with hand osteoarthritis are repeatable and suggest central changes. J. Hand Ther. 2019. [Google Scholar] [CrossRef]
- Scott, D.; Jull, G.; Sterling, M. Widespread sensory hypersensitivity is a feature of chronic whiplash-associated disorder but not chronic idiopathic neck pain. Clin. J. Pain 2005, 21, 175–181. [Google Scholar] [CrossRef]
- Sterling, M.; Treleaven, J.; Edwards, S.; Jull, G. Pressure pain thresholds of upper limb peripheral nerve trunks in asymptomatic subjects. Physiother. Res. Int. 2000, 5, 220–229. [Google Scholar] [CrossRef]
- Nie, H.; Graven-Nielsen, T.; Arendt-Nielsen, L. Spatial and temporal summation of pain evoked by mechanical pressure stimulation. Eur. J. Pain 2009, 13, 592–599. [Google Scholar] [CrossRef]
- Prushansky, T.; Dvir, Z.; Defrin-Assa, R. Reproducibility indices applied to cervical pressure pain threshold measurements in healthy subjects. Clin. J. Pain 2004, 20, 341–347. [Google Scholar] [CrossRef]
- Chien, A.; Sterling, M. Sensory hypoaesthesia is a feature of chronic whiplash but not chronic idiopathic neck pain. Man. Ther. 2010, 15, 48–53. [Google Scholar] [CrossRef]
- Chua, N.; Timmerman, H.; Vissers, K.; OH, W.-S. Multi-modal quantitative sensory testing in patients with unilateral chronic neck pain: An exploratory study. J. Musculoskelet. Pain 2012, 20, 292–299. [Google Scholar] [CrossRef]
- Lopez-de-Uralde-Villanueva, I.; Beltran-Alacreu, H.; Fernandez-Carnero, J.; Kindelan-Calvo, P.; La Touche, R. Widespread pressure pain hyperalgesia in chronic nonspecific neck pain with neuropathic features: A descriptive cross-sectional study. Pain Physician 2016, 19, 77–88. [Google Scholar]
- Coppieters, I.; De Pauw, R.; Kregel, J.; Malfliet, A.; Goubert, D.; Lenoir, D.; Cagnie, B.; Meeus, M. Differences between women with traumatic and idiopathic chronic neck pain and women without neck pain: Interrelationships among disability, cognitive deficits, and central sensitization. Phys. Ther. 2017, 97, 338–353. [Google Scholar] [CrossRef]
- Bragatto, M.M.; Bevilaqua-Grossi, D.; Regalo, S.C.; Sousa, J.D.; Chaves, T.C. Associations among temporomandibular disorders, chronic neck pain and neck pain disability in computer office workers: A pilot study. J. Oral. Rehabil. 2016, 43, 321–332. [Google Scholar] [CrossRef]
- Szikszay, T.M.; Luedtke, K.; Harry von, P. Increased mechanosensivity of the greater occipital nerve in subjects with side-dominant head and neck pain—A diagnostic case-control study. J. Man. Manip. Ther. 2018, 26, 237–248. [Google Scholar] [CrossRef]
- Muñoz-García, D.; López-de-Uralde-Villanueva, I.; Beltrán-Alacreu, H.; La Touche, R.; Fernández-Carnero, J. Patients with concomitant chronic neck pain and myofascial pain in masticatory muscles have more widespread pain and distal hyperalgesia than patients with only chronic neck pain. Pain Med. 2017, 18, 526–537. [Google Scholar] [CrossRef]
- Rebbeck, T.; Moloney, N.; Azoory, R.; Hübscher, M.; Waller, R.; Gibbons, R.; Beales, D. Clinical ratings of pain sensitivity correlate with quantitative measures in people with chronic neck pain and healthy controls: Cross-sectional study. Phys. Ther. 2015, 95, 1536–1546. [Google Scholar] [CrossRef]
- Sjörs, A.; Larsson, B.; Persson, A.L.; Gerdle, B. An increased response to experimental muscle pain is related to psychological status in women with chronic non-traumatic neck-shoulder pain. BMC Musculoskelet. Disord. 2011, 12, 230. [Google Scholar] [CrossRef]
- Castaldo, M.; Catena, A.; Fernández-de-Las-Peñas, C.; Arendt-Nielsen, L. Widespread pressure pain hypersensitivity, health history, and trigger points in patients with chronic neck pain: A preliminary study. Pain Med. 2019. [Google Scholar] [CrossRef]
- Graven-Nielsen, T.; Arendt-Nielsen, L. Assessment of mechanisms in localized and widespread musculoskeletal pain. Nat. Rev. Rheumatol. 2010, 6, 599–606. [Google Scholar] [CrossRef]
- Uddin, Z.; MacDermid, J.C.; Woodhouse, L.J.; Triano, J.J.; Galea, V.; Gross, A.R. The effect of pressure pain sensitivity and patient factors on self-reported pain-disability in patients with chronic neck pain. Open Orthop. J. 2014, 8, 302–309. [Google Scholar] [CrossRef]
- Uthaikhup, S.; Prasert, R.; Paungmali, A.; Boontha, K. Altered pain sensitivity in elderly women with chronic neck pain. PLoS ONE 2015, 10, e0128946. [Google Scholar] [CrossRef]
- Fernández-Carnero, J.; Fernández-de-Las-Peñas, C.; de la Llave-Rincón, A.I.; Ge, H.Y.; Arendt-Nielsen, L. Widespread mechanical pain hypersensitivity as sign of central sensitization in unilateral epicondylalgia: A blinded, controlled study. Clin. J. Pain 2009, 25, 555–561. [Google Scholar] [CrossRef]
- Sanchis, M.N.; Lluch, E.; Nijs, J.; Struyf, F.; Kangasperko, M. The role of central sensitization in shoulder pain: A systematic literature review. Semin. Arthritis Rheum. 2015, 44, 710–716. [Google Scholar] [CrossRef]
- Chiarotto, A.; Fernandez-de-Las-Peñas, C.; Castaldo, M.; Villafañe, J.H. Bilateral pressure pain hypersensitivity over the hand as potential sign of sensitization mechanisms in individuals with thumb carpometacarpal osteoarthritis. Pain Med. 2013, 14, 1585–1592. [Google Scholar] [CrossRef]
- Treleaven, J.; Chen, X.; Sarig Bahat, H. Factors associated with cervical kinematic impairments in patients with neck pain. Man. Ther. 2016, 22, 109–115. [Google Scholar] [CrossRef]
- Alsultan, F.; Cescon, C.; De Nunzio, A.M.; Barbero, M.; Heneghan, N.R.; Rushton, A.; Falla, D. Variability of the helical axis during active cervical movements in people with chronic neck pain. Clin. Biomech. (Bristol, Avon) 2019, 62, 50–57. [Google Scholar] [CrossRef]
- Lascurain-Aguirrebeña, I.; Newham, D.J.; Casado-Zumeta, X.; Lertxundi, A.; Critchley, D.J. Immediate effects of cervical mobilisations on global perceived effect, movement associated pain and neck kinematics in patients with non-specific neck pain. A double blind placebo randomised controlled trial. Musculoskelet. Sci. Pract. 2018, 38, 83–90. [Google Scholar] [CrossRef] [Green Version]
- Richards, K.V.; Beales, D.J.; Smith, A.J.; O’Sullivan, P.B.; Straker, L.M. Neck posture clusters and their association with biopsychosocial factors and neck pain in australian adolescents. Phys. Ther. 2016, 96, 1576–1587. [Google Scholar] [CrossRef]
- Rasmussen, H.; Kent, P.; Kjaer, P.; Kongsted, A. In a secondary care setting, differences between neck pain subgroups classified using the Quebec task force classification system were typically small—A longitudinal study. BMC Musculoskelet. Disord. 2015, 16, 150. [Google Scholar] [CrossRef]
- Jiménez-Trujillo, I.; López-de-Andrés, A.; Del Barrio, J.L.; Hernández-Barrera, V.; Valero-de-Bernabé, M.; Jiménez-García, R. Gender differences in the prevalence and characteristics of pain in spain: Report from a population-based study. Pain Med. 2019. [Google Scholar] [CrossRef]
- Iyer, S.; Kim, H.J. Cervical radiculopathy. Curr. Rev. Musculoskelet. Med. 2016, 9, 272–280. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Higher NSNP during Ipsilateral Rotation (n = 20) | Higher NSNP during Contralateral Rotation (n = 16) | Control Group (n = 20) | p Value | |
|---|---|---|---|---|
| Mean age (years) | 41.1 ± 9.9 | 33.9 ± 9.3 | 36.6 ± 11.1 | 0.104 |
| Height (cm) | 162.1 ± 5.6 | 161.2 ± 5.4 | 162.1 ± 5.5 | 0.854 |
| Body Mass (kg/m2) | 24.7 ± 3.5 | 23.2 ± 3.1 | 23.4 ± 3.2 | 0.297 |
| Most painful side; right % (n) | 30% (6) | 50% (8) | N/A | 0.320 * |
| Hand dominance; right % (n) | 90% (18) | 94% (15) | 90% (18) | 0.889 |
| Pain duration (months) | 24 (6–260) † | 72 (12–264) † | N/A | 0.262 * |
| Neck Disability Index (0–50) | 15.1 ± 6.1 | 11.9 ± 4.8 | 0.7 ± 1.1 | < 0.001 |
| NPRS (neutral position) | 1.5 ± 2.1 | 2.2 ± 2.3 | N/A | 0.398 * |
| NPRS (ipsilateral rotation) | 6.3 ± 1.6 | 2.7 ± 2.4 | N/A | < 0.001 * |
| NPRS (contralateral rotation) | 3.4 ± 2.1 | 5.6 ± 1.6 | N/A | 0.001 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piña-Pozo, F.; Heredia-Rizo, A.M.; Madeleine, P.; Escobio-Prieto, I.; Luque-Carrasco, A.; Oliva-Pascual-Vaca, Á. Local and Widespread Pressure Pain Hyperalgesia Is Not Side Specific in Females with Unilateral Neck Pain that Can Be Reproduced during Passive Neck Rotation. J. Clin. Med. 2019, 8, 1246. https://doi.org/10.3390/jcm8081246
Piña-Pozo F, Heredia-Rizo AM, Madeleine P, Escobio-Prieto I, Luque-Carrasco A, Oliva-Pascual-Vaca Á. Local and Widespread Pressure Pain Hyperalgesia Is Not Side Specific in Females with Unilateral Neck Pain that Can Be Reproduced during Passive Neck Rotation. Journal of Clinical Medicine. 2019; 8(8):1246. https://doi.org/10.3390/jcm8081246
Chicago/Turabian StylePiña-Pozo, Fernando, Alberto Marcos Heredia-Rizo, Pascal Madeleine, Isabel Escobio-Prieto, Antonio Luque-Carrasco, and Ángel Oliva-Pascual-Vaca. 2019. "Local and Widespread Pressure Pain Hyperalgesia Is Not Side Specific in Females with Unilateral Neck Pain that Can Be Reproduced during Passive Neck Rotation" Journal of Clinical Medicine 8, no. 8: 1246. https://doi.org/10.3390/jcm8081246