CD45RC Expression of Circulating CD8+ T Cells Predicts Acute Allograft Rejection: A Cohort Study of 128 Kidney Transplant Patients

 ,
,
Abstract
:1. Introduction
2. Material and Methods
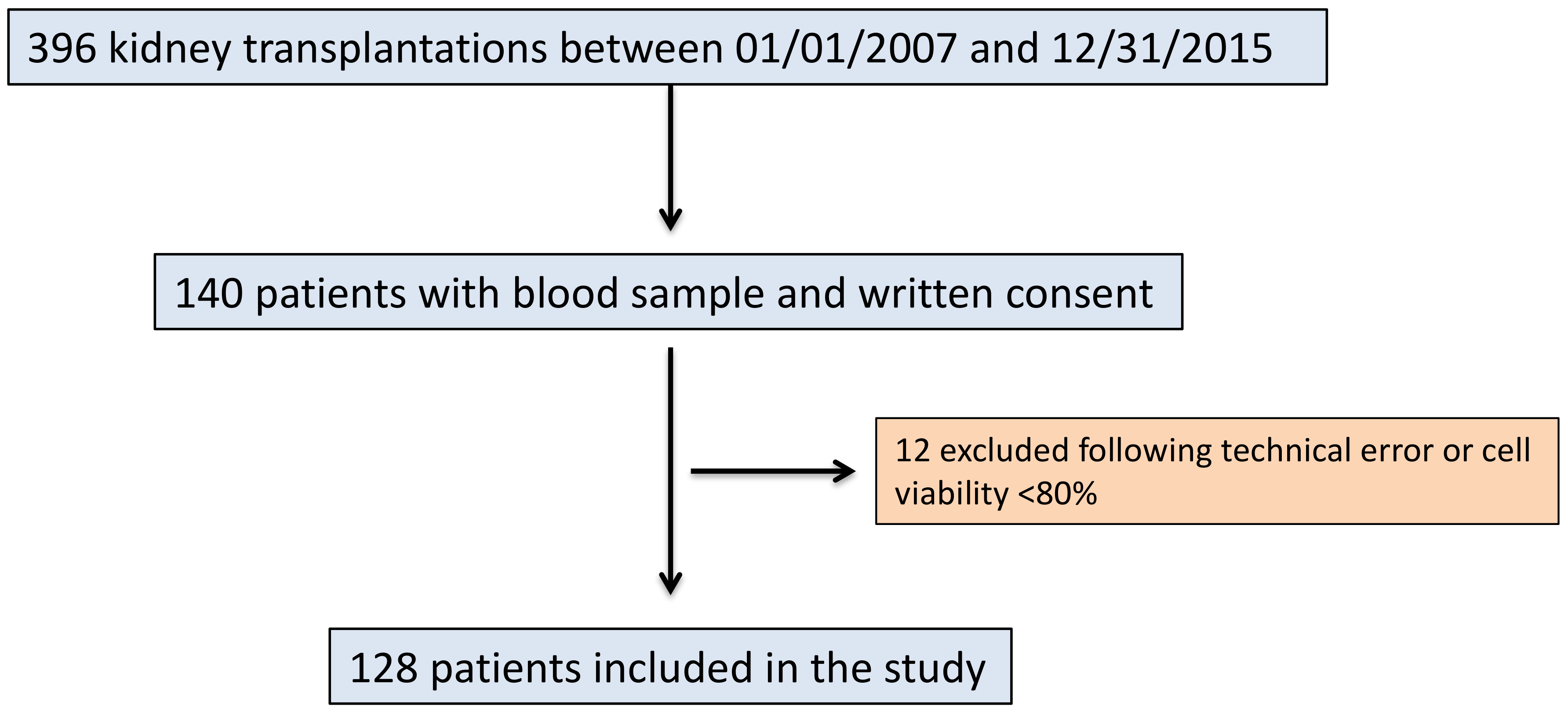
2.1. Study Design and Aim
2.2. Immunosuppressive Regimens
2.3. Data Collection and Definitions
2.4. Sample Collection
2.5. Antibodies and Flow Cytometry Analysis
2.6. CD45RC+ T Cell Purification and T Cell Proliferation Analyses
2.7. Statistical Analysis
3. Results
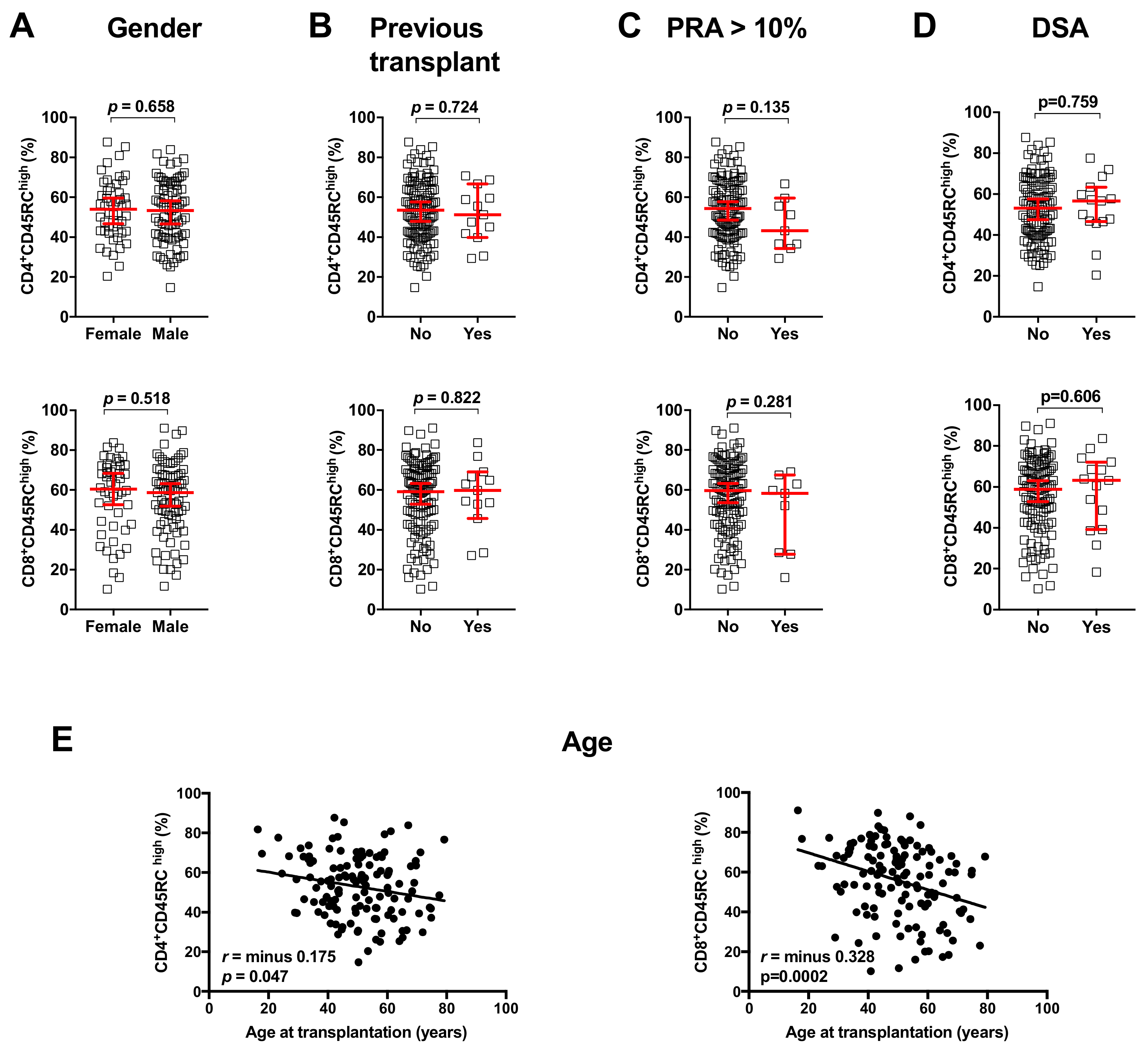
3.1. Characteristics of the Population
3.2. Acute Rejection Episodes
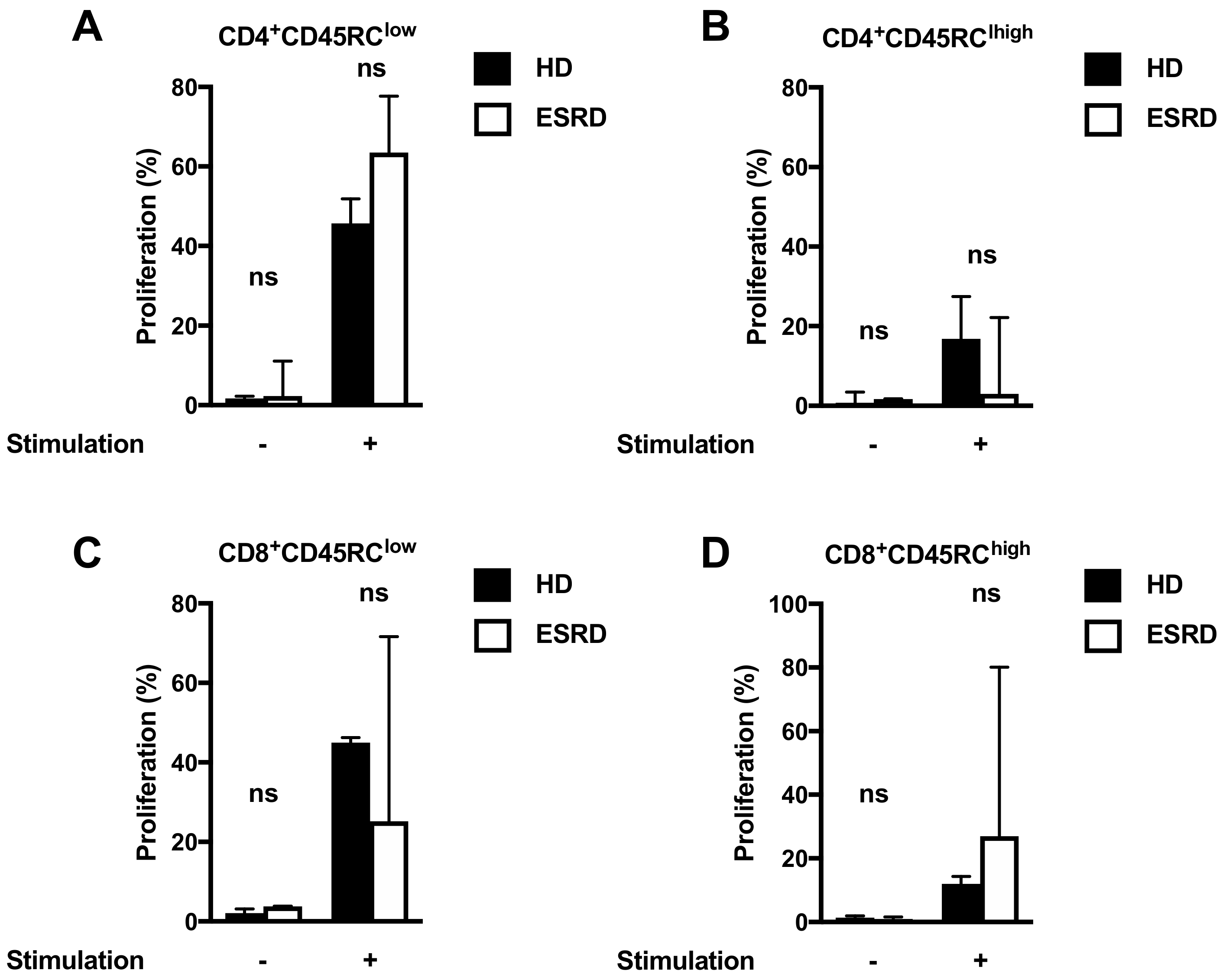
3.3. Proliferative Capacities of CD45RC T Cells
3.4. Association between CD45RC Expression on T Cells and Acute Rejection
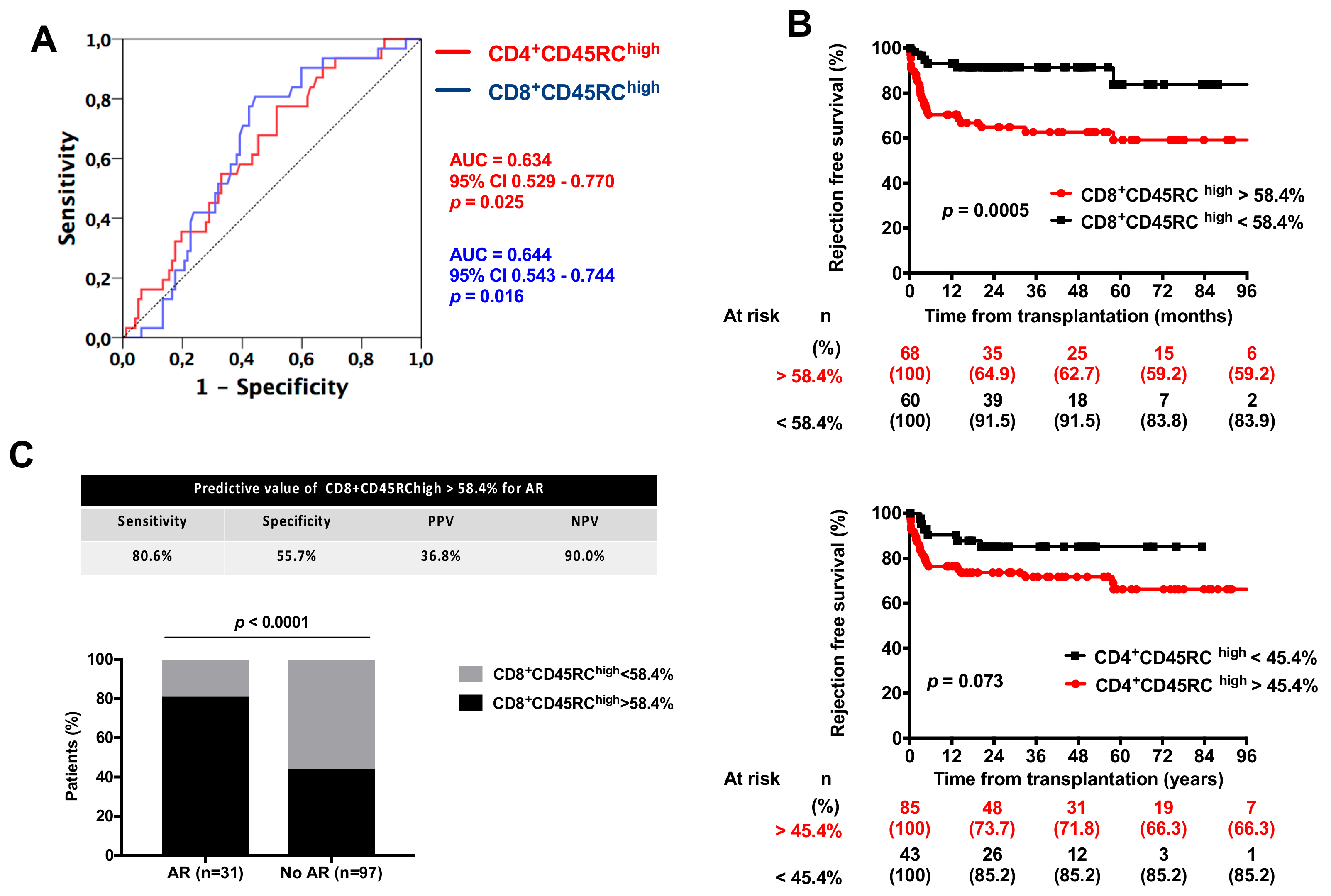
3.5. Value of CD45RC Expression on T Cell for Acute Rejection Prediction
4. Discussion
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
| ABMR | antibody-mediated rejection |
| AR | acute rejection |
| ATG | anti-thymocytes globulins |
| DSA | Donor specific anti-HLA antibodies |
| HD | healthy donors |
| PRA | panel reactive antibody |
| PBMC | plasma blood mononuclear cells |
| ROC | receiver operating curve |
| TCMR | T-cell-mediated rejection |
References
- Nankivell, B.J.; Alexander, S.I. Rejection of the kidney allograft. N. Engl. J. Med. 2010, 363, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Loupy, A.; Lefaucheur, C. Antibody-mediated rejection of solid-organ allografts. N. Engl. J. Med. 2018, 379, 1150–1160. [Google Scholar] [CrossRef] [PubMed]
- Bouatou, Y.; Viglietti, D.; Pievani, D.; Louis, K.; Duong Van Huyen, J.P.; Rabant, M.; Aubert, O.; Taupin, J.L.; Glotz, D.; Legendre, C.; et al. Response to treatment and long-term outcomes in kidney transplant recipients with acute t cell-mediated rejection. Am. J. Transplant. 2019. [Google Scholar] [CrossRef] [PubMed]
- Lebranchu, Y.; Baan, C.; Biancone, L.; Legendre, C.; Morales, J.M.; Naesens, M.; Thomusch, O.; Friend, P. Pretransplant identification of acute rejection risk following kidney transplantation. Transplant. Int. 2014, 27, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Cantarovich, D.; Vistoli, F.; Soulillou, J.P. Immunosuppression minimization in kidney transplantation. Front. Biosci. 2008, 13, 1413–1432. [Google Scholar] [CrossRef] [PubMed]
- Pascual, M.; Theruvath, T.; Kawai, T.; Tolkoff-Rubin, N.; Cosimi, A.B. Strategies to improve long-term outcomes after renal transplantation. N. Engl. J. Med. 2002, 346, 580–590. [Google Scholar] [CrossRef] [PubMed]
- Londono, M.C.; Danger, R.; Giral, M.; Soulillou, J.P.; Sanchez-Fueyo, A.; Brouard, S. A need for biomarkers of operational tolerance in liver and kidney transplantation. Am. J. Transplant. 2012, 12, 1370–1377. [Google Scholar] [CrossRef]
- Clark, M.C.; Baum, L.G. T cells modulate glycans on cd43 and cd45 during development and activation, signal regulation, and survival. Ann. N. Y. Acad. Sci. 2012, 1253, 58–67. [Google Scholar] [CrossRef]
- Hermiston, M.L.; Xu, Z.; Weiss, A. Cd45: A critical regulator of signaling thresholds in immune cells. Annu. Rev. Immunol. 2003, 21, 107–137. [Google Scholar] [CrossRef]
- Ordonez, L.; Bernard, I.; Chabod, M.; Augusto, J.F.; Lauwers-Cances, V.; Cristini, C.; Cuturi, M.C.; Subra, J.F.; Saoudi, A. A higher risk of acute rejection of human kidney allografts can be predicted from the level of cd45rc expressed by the recipients’ cd8 t cells. PLoS ONE 2013, 8, e69791. [Google Scholar] [CrossRef]
- Ordonez, L.; Bernard, I.; L’Faqihi-Olive, F.E.; Tervaert, J.W.; Damoiseaux, J.; Saoudi, A. Cd45rc isoform expression identifies functionally distinct t cell subsets differentially distributed between healthy individuals and aav patients. PLoS ONE 2009, 4, e5287. [Google Scholar] [CrossRef] [PubMed]
- Subra, J.F.; Cautain, B.; Xystrakis, E.; Mas, M.; Lagrange, D.; Van Der Heijden, H.; Van De Gaar, M.J.; Druet, P.; Fournie, G.J.; Saoudi, A.; et al. The balance between cd45rchigh and cd45rclow cd4 t cells in rats is intrinsic to bone marrow-derived cells and is genetically controlled. J. Immunol. 2001, 166, 2944–2952. [Google Scholar] [CrossRef] [PubMed]
- Garnier, A.S.; Planchais, M.; Riou, J.; Jacquemin, C.; Ordonez, L.; Saint-Andre, J.P.; Croue, A.; Saoudi, A.; Delneste, Y.; Devys, A.; et al. Pre-transplant cd45rc expression on blood t cells differentiates patients with cancer and rejection after kidney transplantation. PLoS ONE 2019, 14, e0214321. [Google Scholar] [CrossRef] [PubMed]
- Haas, M.; Sis, B.; Racusen, L.C.; Solez, K.; Glotz, D.; Colvin, R.B.; Castro, M.C.; David, D.S.; David-Neto, E.; Bagnasco, S.M.; et al. Banff 2013 meeting report: Inclusion of c4d-negative antibody-mediated rejection and antibody-associated arterial lesions. Am. J. Transplant. 2014, 14, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Xystrakis, E.; Cavailles, P.; Dejean, A.S.; Cautain, B.; Colacios, C.; Lagrange, D.; van de Gaar, M.J.; Bernard, I.; Gonzalez-Dunia, D.; Damoiseaux, J.; et al. Functional and genetic analysis of two cd8 t cell subsets defined by the level of cd45rc expression in the rat. J. Immunol. 2004, 173, 3140–3147. [Google Scholar] [CrossRef] [PubMed]
- Sellares, J.; De Freitas, D.G.; Mengel, M.; Reeve, J.; Einecke, G.; Sis, B.; Hidalgo, L.G.; Famulski, K.; Matas, A.; Halloran, P.F. Understanding the causes of kidney transplant failure: The dominant role of antibody-mediated rejection and nonadherence. Am. J. Transplant. 2012, 12, 388–399. [Google Scholar] [CrossRef] [PubMed]
- Halloran, P.F.; Chang, J.; Famulski, K.; Hidalgo, L.G.; Salazar, I.D.; Merino Lopez, M.; Matas, A.; Picton, M.; De Freitas, D.; Bromberg, J.; et al. Disappearance of t cell-mediated rejection despite continued antibody-mediated rejection in late kidney transplant recipients. J. Am. Soc. Nephrol. 2015, 26, 1711–1720. [Google Scholar] [CrossRef]
- Randhawa, P. T-cell-mediated rejection of the kidney in the era of donor-specific antibodies: Diagnostic challenges and clinical significance. Curr. Opin. Organ Transplant. 2015, 20, 325–332. [Google Scholar] [CrossRef]
- Krisl, J.C.; Alloway, R.R.; Shield, A.R.; Govil, A.; Mogilishetty, G.; Cardi, M.; Diwan, T.; Abu Jawdeh, B.G.; Girnita, A.; Witte, D.; et al. Acute rejection clinically defined phenotypes correlate with long-term renal allograft survival. Transplantation 2015, 99, 2167–2173. [Google Scholar] [CrossRef]
- Lefaucheur, C.; Gosset, C.; Rabant, M.; Viglietti, D.; Verine, J.; Aubert, O.; Louis, K.; Glotz, D.; Legendre, C.; Duong Van Huyen, J.P.; et al. T cell-mediated rejection is a major determinant of inflammation in scarred areas in kidney allografts. Am. J. Transplant. 2018, 18, 377–390. [Google Scholar] [CrossRef]
- Wiebe, C.; Gibson, I.W.; Blydt-Hansen, T.D.; Karpinski, M.; Ho, J.; Storsley, L.J.; Goldberg, A.; Birk, P.E.; Rush, D.N.; Nickerson, P.W. Evolution and clinical pathologic correlations of de novo donor-specific hla antibody post kidney transplant. Am. J. Transplant. 2012, 12, 1157–1167. [Google Scholar] [CrossRef]
- Moreso, F.; Carrera, M.; Goma, M.; Hueso, M.; Sellares, J.; Martorell, J.; Grinyo, J.M.; Seron, D. Early subclinical rejection as a risk factor for late chronic humoral rejection. Transplantation 2012, 93, 41–46. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | |
|---|---|
| (n = 128) | |
| Baseline Characteristics | |
| Sex (M/F) | 80/48 |
| Age (years) | 50.2 (18.0–79.2) |
| Weigh (kg) | 71.0 (41.0–115.0) |
| BMI (kg/m2) | 25.0 (17.3–40.2) |
| Original nephropathy, n (%) | |
| ADPKD | 33 (25.8) |
| IgA nephropathy | 17 (13.3) |
| Other GN | 13 (10.2) |
| TIN/urologic | 13 (10.2) |
| Vascular nephropathy/diabetic GN | 13 (10.2) |
| Vasculitis | 3 (2.3) |
| Lupus nephritis | 5 (3.9) |
| Undetermined nephropathy | 18 (14.1) |
| Others | 13 (10.2) |
| History of transplantation | |
| Pre-transplant dialysis, n (%) | 92 (71.9) |
| Previous kidney transplantation, n (%) | 13 (10.2) |
| Donor age, years | 50.0 (3.0–87.0) |
| Cold ischemia time (hours) | 16.6 (2.0–35.4) |
| HLA mismatch | |
| HLA A&B&DR | 4.0 (0–6) |
| HLA A&B | 3.0 (0–4) |
| HLA DR | 1.0 (0–2) |
| Sensitization, n (%) | |
| Nonsensitized at transplantation | 89 (69.5) |
| PRA < 10% | 30 (23.4) |
| PRA 10–20% | 1 (0.8) |
| PRA > 20% | 8 (6.2) |
| Immunosuppressive regimens | |
| Induction therapy | |
| None, n (%) | 6 (4.7) |
| Basiliximab, n (%) | 72 (56.3) |
| Antithymocyte globulins, n (%) | 50 (39.1) |
| Maintenance regimen | |
| Tac-based, n (%) | 102 (79.6) |
| Cyclosporin-based, n (%) | 26 (20.3) |
| MMF or MPA, n (%) | 127 (99.2) |
| Mean Follow-Up (Years) | 3.82 ± 2.22 (0.02–8.53) |
| Acute Rejection | |
| Number of patients, n (%) | 31 (24.2) |
| Mean delay to first AR (years) | 0.73 ± 1.24 (0.02–4.83) |
| Histologically proven, n (%) | 28 (90.3) |
| TCMR | 24 (85.7) |
| Borderline | 6 (25.0) |
| Grade IA | 9 (37.5) |
| Grade IB | 8 (33.3) |
| Grade IIA | 1 (4.2) |
| AMR | 1 (3.6) |
| Mixed AR | 3 (10.7) |
| Non histologically proved AR | 3 (9.7) |
| More than one AR episode | 9 (7.0) |
| DSA, n (%) | 15 (11.7) |
| Class I | 4 (26.7) |
| Class II | 11 (73.3) |
| Year 1 Post-Transplant Biological Results | |
| Serum creatinine (µmol/L) * | 141.4 ± 75.2 (60.0–716) |
| GFR (mL/min/1.73 m2) * | 53.2 ± 21.8 (7.3–123) |
| Proteinuria/Creatininuria (g/g) * | 0.25 ± 0.69 (0–5.78) |
| No AR (n = 97) | AR (n = 31) | p | BPAR (n = 28) | p | Excluding Bor AR (n = 22) | p | |
|---|---|---|---|---|---|---|---|
| Baseline Characteristics | |||||||
| Sex (M/F) | 62/35 | 18/13 | 0.558 | 16/12 | 0.514 | 12/10 | 0.413 |
| Age (years) | 50.3 (18.0–79.2) | 48.2 (23.3–66.5) | 0.301 | 48.8 (23.3–66.5) | 0.368 | 45.5 (23.3–66.5) | 0.206 |
| No pretransplant immunization, n (%) | 64 (66.0) | 25 (80.6) | 0.123 | 23 (82.1) | 0.160 | 18 (81.8) | 0.203 |
| PRA > 20%, n (%) | 7 (7.2) | 1 (3.2) | 0.679 | 1 (3.6) | 0.682 | 1 (4.5) | 1.000 |
| History of Transplantation | |||||||
| Previous kidney transplantation, n (%) | 11 (11.3) | 2 (6.5) | 0.733 | 2 (7.1) | 0.731 | 2 (9.1) | 1.000 |
| Pre-transplant dialysis, n (%) | 77 (72.2) | 22 (71.0) | 0.897 | 20 (71.4) | 0,939 | 15 (68.2) | 0.709 |
| Donor age, years | 51.0 (3.0–87.0) | 47.0 (36.0–80.0) | 0.799 | 48 (36.0–80.0) | 0.769 | 43 (37.0–68.0) | 0.494 |
| Cold ischemia time (hours) | 17.0 (2.0–35.4) | 15.6 (2.0–32.2) | 0.434 | 15.5 (2.0–32.2) | 0.299 | 15.5 (2.0–32.2) | 0.359 |
| HLA mismatch (ABDR), n | 4.0 (0–6) | 4.0 (0–6) | 0.733 | 4.0 (0–6) | 0.495 | 4.0 (0–6) | 0.750 |
| Delayed graft function, n (%) | 22 (22.7) | 6 (19.4) | 0.658 | 5 (17.9) | 0.551 | 4 (18.2) | 0.779 |
| De novo DSA, n (%) | 12 (12.4) | 3 (9.7) | 1.000 | 3 (10.7) | 1.000 | 3 (13.6) | 1.000 |
| Immunosuppressive Regimens | |||||||
| Induction (none/Basiliximab/ATG), n (%) | 4 (4.1)/49 (50.5)/44 (45.4) | 2 (6.5)/23 (74.2)/6 (19.3) | 0.035 | 2(7.1)/21(75.0)/5(17.9) | 0.031 | 1(4.6)/16(72.7)/5(22.7) | 0.145 |
| Tacrolimus-based regimen, n (%) | 78 (80.4) | 23 (74.2) | 0.393 | 22 (78.6) | 0.752 | 16 (72.7) | 0.370 |
| Acute Rejection (all) | Yes n = 31 | No n = 97 | p |
|---|---|---|---|
| CD4+CD45RC high | 58.4 ± 13.7 | 51.2 ± 15.7 | 0.023 |
| CD8+CD45RC high | 62.5 ± 13.3 | 53.6 ± 19.3 | 0.019 |
| CD8+CD45RC int | 20.1 ± 7.7 | 23.2 ± 9.3 | 0.096 |
| CD8+CD45RC low | 17.9 ± 9.8 | 23.7 ± 14.2 | 0.035 |
| Biopsy-Proven AR * | Yes n = 28 | No n = 97 | p |
| CD4+CD45RC high | 59.2 ± 13.3 | 51.2 ± 15.7 | 0.016 |
| CD8+CD45RC high | 62.3 ± 13.0 | 53.6 ± 18.0 | 0.010 |
| CD8+CD45RC int | 20.1 ± 7.9 | 23.2 ± 9.3 | 0.117 |
| CD8+CD45RC low | 18.0 ± 10.3 | 23.7 ± 14.2 | 0.049 |
| Acute Rejection (excluding borderline AR) ** | Yes n = 22 | No n = 97 | p |
| CD4+CD45RC high | 60.0 ± 13.4 | 51.2 ± 15.7 | 0.016 |
| CD8+CD45RC high | 64.4 ± 12.2 | 53.6 ± 19.3 | 0.014 |
| CD8+CD45RC int | 19.7 ± 8.1 | 23.2 ± 9.3 | 0.110 |
| CD8+CD45RC low | 16.4 ± 7.9 | 23.7 ± 14.2 | 0.020 |
| Multivariate Cox Models | HR | 95% CI | p | |
|---|---|---|---|---|
| All ARs | CD8+CD45RChigh (>58.4%) | 4.04 | 1.65–9.88 | 0.002 |
| Induction (ATG) | 0.39 | 0.16–0.94 | 0.037 | |
| ARs excluding borderlines * | CD8+CD45RChigh (>58.4%) | 4.42 | 1.49–13.1 | 0.007 |
| Induction (ATG) | 0.46 | 0.17–1.25 | 0.130 | |
| Biopsy-proven ARs ** | CD8+CD45RChigh (>58.4%) | 3.59 | 1.45–8.89 | 0.006 |
| Induction (ATG) | 0.35 | 0.13–0.93 | 0.035 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lemerle, M.; Garnier, A.-S.; Planchais, M.; Brilland, B.; Delneste, Y.; Subra, J.-F.; Blanchet, O.; Blanchard, S.; Croue, A.; Duveau, A.; et al. CD45RC Expression of Circulating CD8+ T Cells Predicts Acute Allograft Rejection: A Cohort Study of 128 Kidney Transplant Patients. J. Clin. Med. 2019, 8, 1147. https://doi.org/10.3390/jcm8081147
Lemerle M, Garnier A-S, Planchais M, Brilland B, Delneste Y, Subra J-F, Blanchet O, Blanchard S, Croue A, Duveau A, et al. CD45RC Expression of Circulating CD8+ T Cells Predicts Acute Allograft Rejection: A Cohort Study of 128 Kidney Transplant Patients. Journal of Clinical Medicine. 2019; 8(8):1147. https://doi.org/10.3390/jcm8081147
Chicago/Turabian StyleLemerle, Marie, Anne-Sophie Garnier, Martin Planchais, Benoit Brilland, Yves Delneste, Jean-François Subra, Odile Blanchet, Simon Blanchard, Anne Croue, Agnès Duveau, and et al. 2019. "CD45RC Expression of Circulating CD8+ T Cells Predicts Acute Allograft Rejection: A Cohort Study of 128 Kidney Transplant Patients" Journal of Clinical Medicine 8, no. 8: 1147. https://doi.org/10.3390/jcm8081147