
The Effect of Peri-Implant Therapy on the Expression of Th17-Related Cytokines in Patients with Peri-Implant Mucositis and Peri-Implantitis: A Prospective Longitudinal Study

 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Study Setting
- Being systemically healthy or having controlled systemic conditions;
- Being partially edentulous, with at least two osseointegrated implants affected by peri-implant disease (PID);
- Having implant prosthetics that have been in function for a minimum of six months.
- Had received periodontal or peri-implant treatment within six months before the study commencement;
- Were pregnant or breastfeeding;
- Were smokers;
- Had taken antibiotics and anti-inflammatories within the last three months;
- Had taken antiresorptive drugs within the last two years;
- Had undergone radiotherapy, chemotherapy, or iodine therapy within the last two years.
2.2. Clinical Examination
2.3. Peri-Implant Crevicular Fluid Collection
2.4. Peri-Implant Therapy
2.5. Multiplex Assay
2.6. Statistical Analyses
3. Results
3.1. Demographic Data
3.2. Clinical Results
3.3. Description of Implants
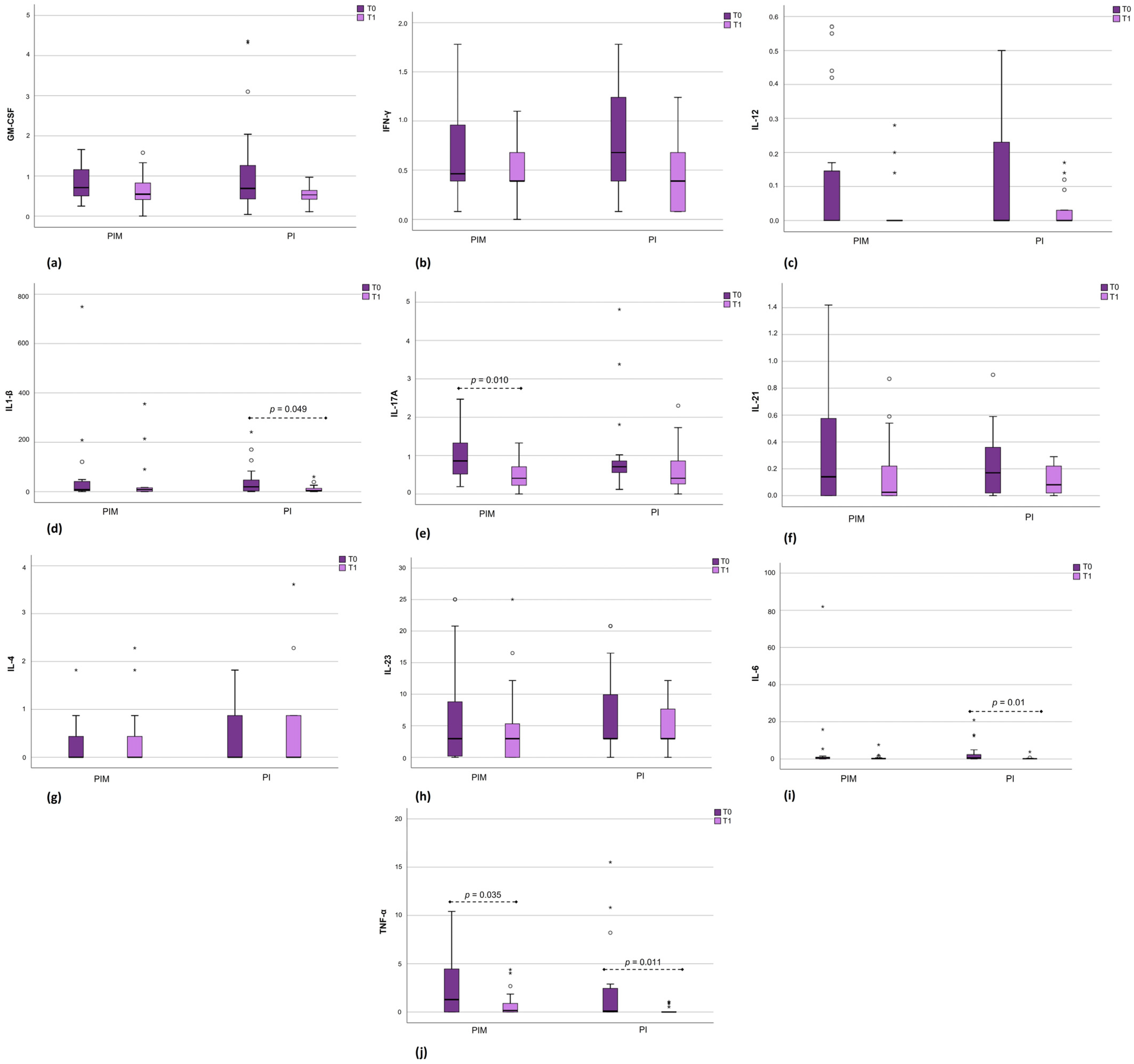
3.4. Immunological Results
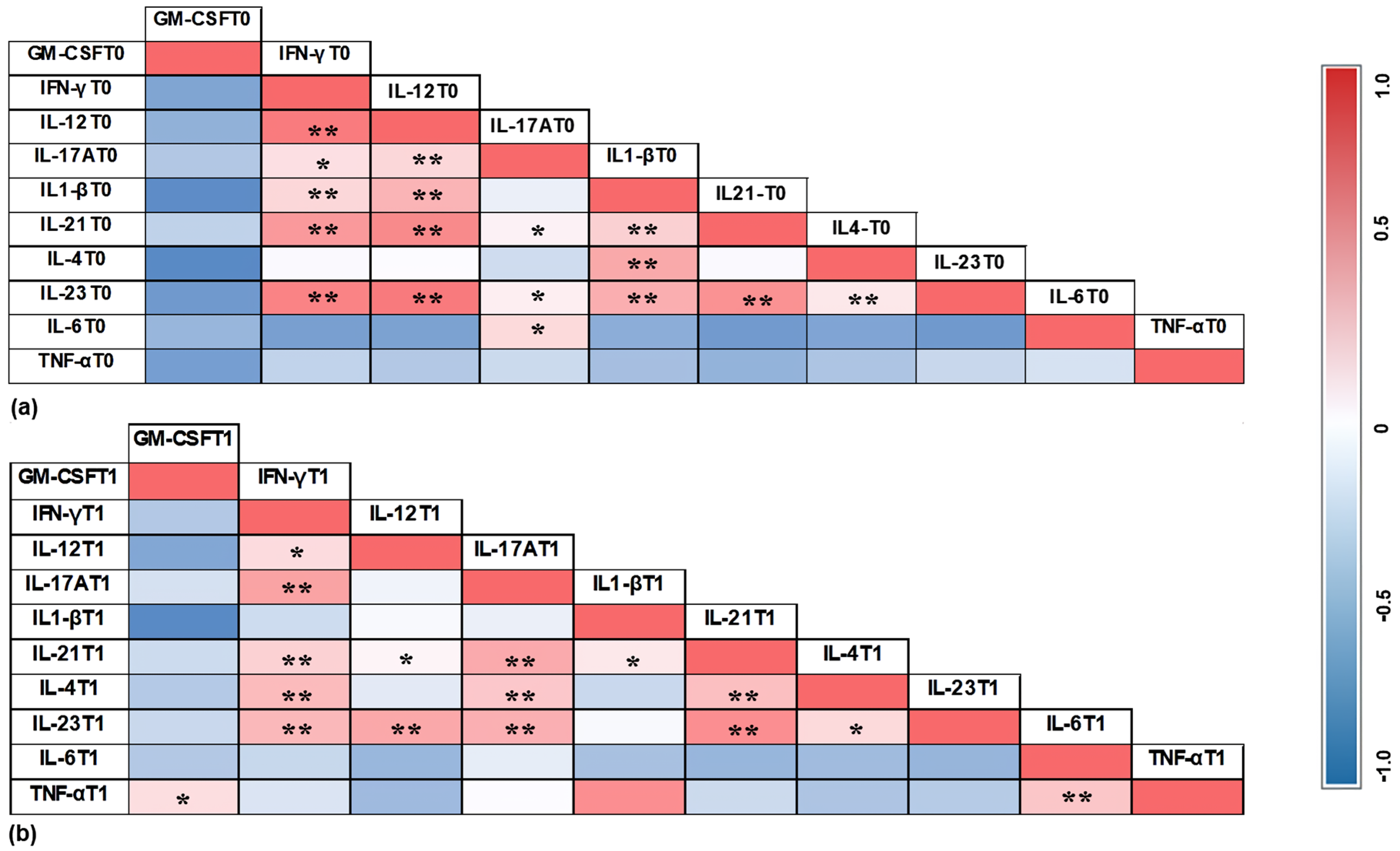
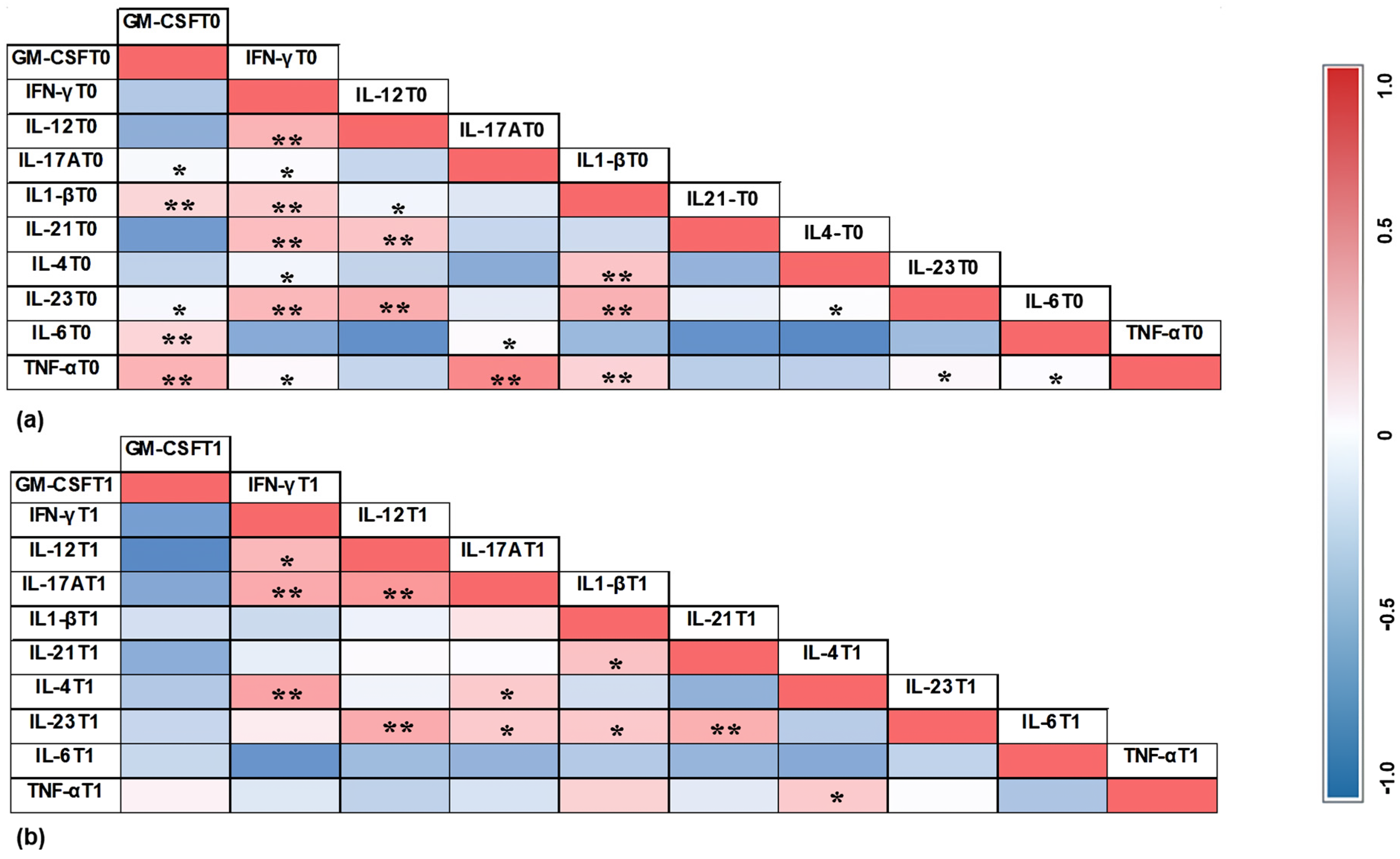
3.5. Correlation Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J. Clin. Periodontol. 2018, 45, 286–291. [Google Scholar] [CrossRef]
- Gargallo-Albiol, J.; Tavelli, L.; Barootchi, S.; Monje, A.; Wang, H.L. Clinical sequelae and patients’ perception of dental implant removal: A cross-sectional study. J. Periodontol. 2021, 92, 823–832. [Google Scholar] [CrossRef]
- Lee, C.T.; Huang, Y.W.; Zhu, L.; Weltman, R. Prevalences of peri-implantitis and peri-implant mucositis: Systematic review and meta-analysis. J. Dent. 2017, 62, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Schaller, D.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Berglundh, T. Peri-implantitis—Onset and pattern of progression. J. Clin. Periodontol. 2016, 43, 383–388. [Google Scholar] [CrossRef]
- Darby, I. Risk factors for periodontitis & peri-implantitis. Periodontol. 2000 2022, 90, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Diaz, P.; Gonzalo, E.; Villagra, L.J.G.; Miegimolle, B.; Suarez, M.J. What is the prevalence of peri-implantitis? A systematic review and meta-analysis. BMC Oral Health 2022, 22, 449. [Google Scholar] [CrossRef] [PubMed]
- Chmielewski, M.; Pilloni, A. Current Molecular, Cellular and Genetic Aspects of Peri-Implantitis Disease: A Narrative Review. Dent. J. 2023, 11, 134. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, M.G.; Pimentel, S.P.; Ribeiro, F.V.; Cirano, F.R.; Casati, M.Z. Host response and peri-implantitis. Braz. Oral Res. 2019, 33, e066. [Google Scholar] [CrossRef] [PubMed]
- Troen, B.R. Molecular mechanisms underlying osteoclast formation and activation. Exp. Gerontol. 2003, 38, 605–614. [Google Scholar] [CrossRef]
- Markou, E.; Eleana, B.; Lazaros, T.; Antonios, K. The influence of sex steroid hormones on gingiva of women. Open Dent. J. 2009, 5, 114–119. [Google Scholar] [CrossRef]
- Severino, V.O.; Beghini, M.; de Araújo, M.F.; de Melo, M.L.R.; Miguel, C.B.; Rodrigues, W.F.; Pereira, S.A.d.L. Expression of IL-6, IL-10, IL-17 and IL-33 in the peri-implant crevicular fluid of patients with peri-implant mucositis and peri-implantitis. Arch. Oral Biol. 2016, 72, 194–199. [Google Scholar] [CrossRef]
- Petković, A.B.; Matić, S.M.; Stamatović, N.V.; Vojvodić, D.V.; Todorović, T.M.; Lazić, Z.R.; Kozomara, R.J. Proinflammatory cytokines (IL-1beta and TNF-alpha) and chemokines (IL-8 and MIP-1alpha) as markers of peri-implant tissue condition. Int. J. Oral Maxillofac. Surg. 2010, 39, 478–485. [Google Scholar] [CrossRef]
- Faot, F.; Nascimento, G.G.; Bielemann, A.M.; Campão, T.D.; Leite, F.R.; Quirynen, M. Can peri-implant crevicular fluid assist in the diagnosis of peri-implantitis? A systematic review and meta-analysis. J. Periodontol. 2015, 865, 631–645. [Google Scholar] [CrossRef]
- Delucchi, F.; Canepa, C.; Canullo, L.; Pesce, P.; Isola, G.; Menini, M. Biomarkers from Peri-Implant Crevicular Fluid (PICF) as Predictors of Peri-Implant Bone Loss: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 3202. [Google Scholar] [CrossRef] [PubMed]
- Askar, M. T helper subsets & regulatory T cells: Rethinking the paradigm in the clinical context of solid organ transplantation. Int. J. Immunogenet. 2014, 41, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Iwakura, Y.; Nakae, S.; Saijo, S.; Ishigame, H. The roles of IL-17A in inflammatory immune responses and host defense against pathogens. Immunol. Rev. 2008, 226, 57–79. [Google Scholar] [CrossRef]
- Korn, T.; Bettelli, E.; Oukka, M.; Kuchroo, V.K. IL-17 and Th17 Cells. Annu. Rev. Immunol. 2009, 27, 485–517. [Google Scholar] [CrossRef] [PubMed]
- Giro, G.; Tebar, A.; Franco, L.; Racy, D.; Bastos, M.F.; Shibli, J.A. Treg and TH17 link to immune response in individuals with peri-implantitis: A preliminary report. Clin. Oral Investig. 2021, 25, 1291–1297. [Google Scholar] [CrossRef]
- Teixeira, M.K.S.; Lira-Junior, R.; Telles, D.M.; Lourenço, E.J.V.; Figueredo, C.M. Th17-related cytokines in mucositis: Is there any difference between peri-implantitis and periodontitis patients? Clin. Oral Implant. Res. 2017, 28, 816–822. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Salvi, G.E.; Mombelli, A.; Loup, P.J.; Heitz, F.; Kruger, E.; Lang, N.P. Supportive peri-implant therapy following anti-infective surgical peri-implantitis treatment: 5-year survival and success. Clin. Oral Implant. Res. 2018, 29, 1–6. [Google Scholar] [CrossRef]
- Schwarz, F.; Jepsen, S.; Obreja, K.; Galarraga-Vinueza, M.E.; Ramanauskaite, A. Surgical therapy of peri-implantitis. Periodontol. 2000 2022, 88, 145–181. [Google Scholar] [CrossRef] [PubMed]
- Verket, A.; Koldsland, O.C.; Bunaes, D.; Lie, S.A.; Romandini, M. Non-surgical therapy of peri-implant mucositis-Mechanical/physical approaches: A systematic review. J. Clin. Periodontol. 2023, 26, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Ramanauskaite, A.; Daugela, P.; Juodzbalys, G. Treatment of peri-implantitis: Meta-analysis of findings in a systematic literature review and novel protocol proposal. Quintessence Int. 2016, 47, 379–393. [Google Scholar] [CrossRef]
- Dos Santos Martins, B.G.; Fernandes, J.C.H.; Martins, A.G.; de Moraes Castilho, R.; de Oliveira Fernandes, G.V. Surgical and Nonsurgical Treatment Protocols for Peri-implantitis: An Overview of Systematic Reviews. Int. J. Oral Maxillofac. Implant. 2022, 37, 660–676. [Google Scholar] [CrossRef] [PubMed]
- Ichioka, Y.; Virto, L.; Nuevo, P.; Gamonal, J.D.; Derks, J.; Larsson, L.; Sanz, M.; Berglundh, T. Decontamination of biofilm-contaminated implant surfaces: An in vitro evaluation. Clin. Oral Implant. Res. 2023, 34, 1058–1072. [Google Scholar] [CrossRef] [PubMed]
- Teixeira Neves, G.S.; Elangovan, G.; Teixeira, M.K.S.; Mello-Neto, J.M.; Tadakamadla, S.K.; Lourenço, E.J.V.; Telles, D.M.; Figueredo, C.M. Peri-Implant Surgical Treatment Downregulates the Expression of sTREM-1 and MMP-8 in Patients with Peri-Implantitis: A Prospective Study. Int. J. Environ. Res. Public Health 2022, 19, 3627. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Persson, G.R.; Pirih, F.Q.; Camargo, P.M. Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J. Periodontol. 2018, 89, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar]
- Wassall, R.R.; Preshaw, P.M. Clinical and technical considerations in the analysis of gingival crevicular fluid. Periodontol. 2000 2016, 70, 65–79. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Berglundh, T.; Heitz-Mayfield, L.J.; Pjetursson, B.E.; Salvi, G.E.; Sanz, M. Consensus statements and recommended clinical procedures regarding implant survival and complications. Int. J. Oral Maxillofac. Implant. 2004, 19, 150–154. [Google Scholar]
- Khoury, F.; Keeve, P.L.; Ramanauskaite, A.; Schwarz, F.; Koo, K.T.; Sculean, A.; Romanos, G. Surgical treatment of peri-implantitis—Consensus report of working group 4. Int. Dent. J. 2019, 69, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Alassy, H.; Parachuru, P.; Wolff, L. Peri-Implantitis Diagnosis and Prognosis Using Biomarkers in Peri-Implant Crevicular Fluid: A Narrative Review. Diagnostics 2019, 9, 214. [Google Scholar] [CrossRef] [PubMed]
- Severino, V.O.; Napimoga, M.H.; de Lima Pereira, A.S. Expression of IL-6, IL-10, IL-17 and IL-8 in the peri-implant crevicular fluid of patients with peri-implantitis. Arch. Oral Biol. 2011, 56, 823–828. [Google Scholar] [CrossRef]
- de Araújo, M.F.; Filho, A.F.; da Silva, G.P.; de Melo, M.L.R.; Napimoga, M.H.; Rodrigues, D.B.R.; Alves, P.M.; Pereira, S.A.d.L. Evaluation of peri-implant mucosa: Clinical, histopathological and immunological aspects. Arch. Oral Biol. 2014, 59, 470–478. [Google Scholar] [CrossRef]
- Irie, K.; Azuma, T.; Tomofuji, T.; Yamamoto, T. Exploring the Role of IL-17A in Oral Dysbiosis-Associated Periodontitis and Its Correlation with Systemic Inflammatory Disease. Dent. J. 2023, 11, 194. [Google Scholar] [CrossRef]
- Kashefimehr, A.; Pourabbas, R.; Faramarzi, M.; Zarandi, A.; Moradi, A.; Tenenbaum, H.C.; Azarpazhooh, A. Effects of enamel matrix derivative on non-surgical management of peri-implant mucositis: A double-blind randomized clinical trial. Clin. Oral Investig. 2017, 21, 2379–2388. [Google Scholar] [CrossRef]
- Pourabbas, R.; Khorramdel, A.; Sadighi, M.; Kashefimehr, A.; Mousavi, S.A. Effect of photodynamic therapy as an adjunctive to mechanical debridement on the nonsurgical treatment of peri-implant mucositis: A randomized controlled clinical trial. Dent. Res. J. (Isfahan) 2023, 20, 1. [Google Scholar] [CrossRef]
- Duarte, P.M.; de Mendonça, A.C.; Máximo, M.B.; Santos, V.R.; Bastos, M.F.; Nociti, F.H. Effect of anti-infective mechanical therapy on clinical parameters and cytokine levels in human peri-implant diseases. J. Periodontol. 2009, 80, 234–243. [Google Scholar] [CrossRef] [PubMed]
- de Mendonça, A.C.; Santos, V.R.; César-Neto, J.B.; Duarte, P.M. Tumor necrosis factor-alpha levels after surgical anti-infective mechanical therapy for peri-implantitis: A 12-month follow-up. J. Periodontol. 2009, 80, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Schär, D.; Wicki, B.; Eick, S.; Ramseier, C.A.; Arweiler, N.B.; Sculean, A.; Salvi, G.E. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: 12-month outcomes of a randomized controlled clinical trial. Clin. Oral Implant. Res. 2014, 25, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Elsadek, M.F. Effectiveness of two photosensitizer-mediated photodynamic therapy for treating moderate peri-implant infections in type-II diabetes mellitus patients: A randomized clinical trial. Photodiagnosis Photodyn. Ther. 2023, 43, 103643. [Google Scholar] [CrossRef]
- Ata-Ali, J.; Flichy-Fernández, A.J.; Alegre-Domingo, T.; Ata-Ali, F.; Palacio, J.; Peñarrocha-Diago, M. Clinical, microbiological, and immunological aspects of healthy versus peri-implantitis tissue in full arch reconstruction patients: A prospective cross-sectional study. BMC Oral Health 2015, 15, 43. [Google Scholar] [CrossRef] [PubMed]
- Zani, S.R.; Moss, K.; Shibli, J.A.; Teixeira, E.R.; de Oliveira Mairink, R.; Onuma, T.; Feres, M.; Teles, R.P. Peri-implant crevicular fluid biomarkers as discriminants of peri-implant health and disease. J. Clin. Periodontol. 2016, 43, 825–832. [Google Scholar] [CrossRef]
- Bhavsar, I.; Miller, C.S.; Ebersole, J.L.; Dawson, D.R., 3rd; Thompson, K.L.; Al-Sabbagh, M. Biological response to peri-implantitis treatment. J. Periodontal. Res. 2019, 54, 720–728. [Google Scholar] [CrossRef]
- Hentenaar, D.F.M.; De Waal, Y.C.M.; Vissink, A.; Van Winkelhoff, A.J.; Meijer, H.J.; Liefers, S.C.; Kroese, F.G.; Raghoebar, G.M. Biomarker levels in peri-implant crevicular fluid of healthy implants, untreated and non-surgically treated implants with peri-implantitis. J. Clin. Periodontol. 2021, 48, 590–601. [Google Scholar] [CrossRef]
- Song, L.; Jiang, J.; Li, J.; Zhou, C.; Chen, Y.; Lu, H.; He, F. The Characteristics of Microbiome and Cytokines in Healthy Implants and Peri-Implantitis of the Same Individuals. J. Clin. Med. 2022, 11, 5817. [Google Scholar] [CrossRef]
- Lumbikananda, S.; Srithanyarat, S.S.; Mattheos, N.; Osathanon, T. Oral Fluid Biomarkers for Peri-Implantitis: A Scoping Review. Int. Dent. J. 2024, 74, 387–402. [Google Scholar] [CrossRef]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef] [PubMed]
- Luengo, F.; Solonko, M.; Sanz-Esporrín, J.; Sanz-Sánchez, I.; Herrera, D.; Sanz, M. Clinical, Microbiological, and Biochemical Impact of the Surgical Treatment of Peri-Implantitis-A Prospective Case Series. J. Clin. Med. 2022, 11, 4699. [Google Scholar] [CrossRef]
- Nagy, E.; Lei, Y.; Martínez-Martínez, E.; Body, S.C.; Schlotter, F.; Creager, M.; Assmann, A.; Khabbaz, K.; Libby, P.; Hansson, G.K.; et al. Interferon-γ Released by Activated CD8+ T Lymphocytes Impairs the Calcium Resorption Potential of Osteoclasts in Calcified Human Aortic Valves. Am. J. Pathol. 2017, 187, 1413–1425. [Google Scholar] [CrossRef] [PubMed]
- Danielsen, A.K.; Damgaard, C.; Massarenti, L.; Østrup, P.; Riis Hansen, P.; Holmstrup, P.; Nielsen, C.H. B-cell cytokine responses to Porphyromonas gingivalis in patients with periodontitis and healthy controls. J. Periodontol. 2023, 94, 997–1007. [Google Scholar] [CrossRef] [PubMed]
- Iyer, S.S.; Cheng, G. Role of interleukin 10 transcriptional regulation in inflammation and autoimmune disease. Crit. Rev. Immunol. 2012, 32, 23–63. [Google Scholar] [CrossRef] [PubMed]
- Abbas, A.K.; Pillai, S.; Lichtman, A.H. Imunologia Celular e Molecular, 9th ed.; Elsevier: Rio de Janeiro, Brazil, 2019; pp. 856–857. [Google Scholar]
- Güncü, G.N.; Akman, A.C.; Günday, S.; Yamalık, N.; Berker, E. Effect of inflammation on cytokine levels and bone remodelling markers in peri-implant sulcus fluid: A preliminary report. Cytokine 2012, 59, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, F.J.; Moraes Junior, M.; Lourenço, E.J.; Teles, D.M.; Figueredo, C.M. Cytokines expression in saliva and peri-implant crevicular fluid of patients with peri-implant disease. Clin. Oral Implant. Res. 2014, 25, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Huang, N.; Dong, H.; Luo, Y.; Shao, B. Th17 Cells in Periodontitis and Its Regulation by A20. Front. Immunol. 2021, 12, 742925. [Google Scholar] [CrossRef] [PubMed]
- El-Behi, M.; Ciric, B.; Dai, H.; Yan, Y.; Cullimore, M.; Safavi, F.; Zhang, G.X.; Dittel, B.N.; Rostami, A. The encephalitogenicity of T(H)17 cells is dependent on IL-1- and IL-23-induced production of the cytokine GM-CSF. Nat. Immunol. 2011, 12, 568–575. [Google Scholar] [CrossRef]
- Gay, I.C.; Tran, D.T.; Weltman, R.; Parthasarathy, K.; Diaz-Rodriguez, J.; Walji, M.; Fu, Y.; Friedman, L. Role of supportive maintenance therapy on implant survival: A university-based 17 years retrospective analysis. Int. J. Dent. Hyg. 2016, 14, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Monje, A.; Wang, H.L.; Nart, J. Association of Preventive Maintenance Therapy Compliance and Peri-Implant Diseases: A Cross-Sectional Study. J. Periodontol. 2017, 88, 1030–1041. [Google Scholar] [CrossRef] [PubMed]
- Frisch, E.; Vach, K.; Ratka-Krueger, P. Impact of supportive implant therapy on peri-implant diseases: A retrospective 7-year study. J. Clin. Periodontol. 2020, 47, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Astolfi, V.; Ríos-Carrasco, B.; Gil-Mur, F.J.; Ríos-Santos, J.V.; Bullón, B.; Herrero-Climent, M.; Bullón, P. Incidence of Peri-Implantitis and Relationship with Different Conditions: A Retrospective Study. Int. J. Environ. Res. Public Health 2022, 19, 4147. [Google Scholar] [CrossRef]
- Costa, F.O.; Costa, A.M.; Ferreira, S.D.; Lima, R.P.E.; Pereira, G.H.M.; Cyrino, R.M.; Oliveira, A.M.S.D.; Oliveira, P.A.D.; Cota, L.O.M. Long-term impact of patients’ compliance to peri-implant maintenance therapy on the incidence of peri-implant diseases: An 11-year prospective follow-up clinical study. Clin. Implant Dent. Relat. Res. 2023, 25, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Rösing, C.K.; Fiorini, T.; Haas, A.N.; Muniz, F.W.M.G.; Oppermann, R.V.; Susin, C. The impact of maintenance on peri-implant health. Braz. Oral Res. 2019, 33, e074. [Google Scholar] [CrossRef] [PubMed]
- Leone, F.D.; Blasi, G.; Amerio, E.; Valles, C.; Nart, J.; Monje, A. Influence of the level of compliance with preventive maintenance therapy upon the prevalence of peri-implant diseases. J. Periodontol. 2024, 95, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.L. Peri-implantitis. J. Periodontol. 2018, 89, 267–290. [Google Scholar] [CrossRef] [PubMed]
- Jia, P.; Tang, Y.; Niu, L.; Qiu, L. Clinical and radiographic outcomes of a combined surgery approach to treat peri-implantitis. Int. J. Oral Maxillofac. Surg. 2024, 53, 333–342. [Google Scholar] [CrossRef]
- Derks, J.; Ortiz-Vigón, A.; Guerrero, A.; Donati, M.; Bressan, E.; Ghensi, P.; Schaller, D.; Tomasi, C.; Karlsson, K.; Abrahamsson, I.; et al. Reconstructive surgical therapy of peri-implantitis: A multicenter randomized controlled clinical trial. Clin. Oral Implant. Res. 2022, 33, 921–944. [Google Scholar] [CrossRef] [PubMed]
- Romandini, M.; Laforí, A.; Pedrinaci, I.; Baima, G.; Ferrarotti, F.; Lima, C.; Holtzman, L.P.; Aimetti, M.; Cordaro, L.; Sanz, M. Effect of sub-marginal instrumentation before surgical treatment of peri-implantitis: A multi-centre randomized clinical trial. J. Clin. Periodontol. 2022, 49, 1334–1345. [Google Scholar] [CrossRef]
- Moraschini, V.; Kischinhevsky, I.C.C.; Sartoretto, S.C.; de Almeida Barros Mourão, C.F.; Sculean, A.; Calasans-Maia, M.D.; Shibli, J.A. Does implant location influence the risk of peri-implantitis? Periodontol. 2000 2022, 90, 224–235. [Google Scholar] [CrossRef]
- Sun, J.S.; Liu, K.C.; Hung, M.C.; Lin, H.Y.; Chuang, S.L.; Lin, P.J.; Chang, J.Z. A cross-sectional study for prevalence and risk factors of peri-implant marginal bone loss. J. Prosthet. Dent. 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Koo, K.T.; Lee, E.J.; Kim, J.Y.; Seol, Y.J.; Han, J.S.; Kim, T.I.; Lee, Y.M.; Ku, Y.; Wikesjö, U.M.; Rhyu, I.C. The effect of internal versus external abutment connection modes on crestal bone changes around dental implants: A radiographic analysis. J. Periodontol. 2012, 83, 1104–1109. [Google Scholar] [CrossRef] [PubMed]
- Machado, L.S.; Bonfante, E.A.; Anchieta, R.B.; Yamaguchi, S.; Coelho, P.G. Implant-abutment connection designs for anterior crowns: Reliability and failure modes. Implant Dent. 2013, 22, 540–545. [Google Scholar] [CrossRef]
- Schmitt, C.M.; Nogueira-Filho, G.; Tenenbaum, H.C.; Lai, J.Y.; Brito, C.; Döring, H.; Nonhoff, J. Performance of conical abutment (Morse Taper) connection implants: A systematic review. J. Biomed. Mater. Res. A 2014, 102, 552–574. [Google Scholar] [CrossRef] [PubMed]
- Macedo, J.P.; Pereira, J.; Vahey, B.R.; Henriques, B.; Benfatti, C.A.M.; Magini, R.S.; López-López, J.; Souza, J.C.M. Morse taper dental implants and platform switching: The new paradigm in oral implantology. Eur. J. Dent. 2016, 10, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, M.K.S.; de Moraes Rego, M.R.; da Silva, M.F.T.; Lourenço, E.J.V.; Figueredo, C.M.; Telles, D.M. Bacterial Profile and Radiographic Analysis Around Osseointegrated Implants With Morse Taper and External Hexagon Connections: Split-Mouth Model. J. Oral Implantol. 2019, 45, 469–473. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Salvi, G.E.; Mombelli, A.; Faddy, M.; Lang, N.P. Anti-infective surgical therapy of peri-implantitis. A 12-month prospective clinical study. Clin. Oral Implant. Res. 2012, 23, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Carcuac, O.; Derks, J.; Charalampakis, G.; Abrahamsson, I.; Wennström, J.; Berglundh, T. Adjunctive Systemic and Local Antimicrobial Therapy in the Surgical Treatment of Peri-implantitis: A Randomized Controlled Clinical Trial. J. Dent. Res. 2016, 95, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Carcuac, O.; Derks, J.; Abrahamsson, I.; Wennström, J.L.; Petzold, M.; Berglundh, T. Surgical treatment of peri-implantitis: 3-year results from a randomized controlled clinical trial. J. Clin. Periodontol. 2017, 44, 1294–1303. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Peri-Implant Mucositis | Peri-Implantitis | p Value | |
|---|---|---|---|---|
| Participants | 37 (100%) | 20 (54.05%) | 17 (45.95%) | 0.622 |
| Gender | ||||
| Male | 15 (40.54%) | 7 (46.66%) | 8 (53.34%) | 0.457 |
| Female | 22 (59.46%) | 13 (59.1%) | 9 (40.9%) | 0.457 |
| Age | 59.14 (±10.37) | 58.65 (±11.62) | 59.70 (±9.01) | 0.219 |
| Periodontal Classification in Concomitant Periodontitis | 8 (100%) | 2 (25%) | 6 (75%) | 0.157 |
| Generalized Stage II Grade A | 1 (12.5%) | 1 (100%) | 0 (0%) | - |
| Generalized Stage III Grade A | 6 (75%) | 1 (16.67%) | 5 (83.33%) | 0.197 |
| Generalized Stage III Grade B | 1 (12.5%) | 0 (0%) | 1 (100%) | - |
| Last PIMT | ||||
| Less than a year | 8 (21.62%) | 6 (75%) | 2 (2%) | 0.157 |
| Between 1 and 2 years | 17 (45.95%) | 9 (52.94%) | 8 (47.06%) | 0.808 |
| More than 2 years | 12 (32.43%) | 5 (41.67%) | 7 (58.33%) | 0.564 |
| Baseline | T1 | p Value | |
|---|---|---|---|
| PD (mm) | 3.90 (±1.34) | 3.27 (±1.19) | 0.001 |
| CAL (mm) | 2.41 (±1.37) | 1.50 (±1.31) | <0.001 |
| % PId | 71.43 (±45.58) | 46.43 (±50.32) | 0.003 |
| % BoP | 100 (±0.00) | 51.79 (±50.42) | <0.001 |
| Baseline | T1 | p Value | |
|---|---|---|---|
| PD (mm) | 5.29 (±1.74) | 3.00 (±1.00) | <0.001 |
| CAL (mm) | 4.32 (±1.78) | 3.00 (±1.80) | 0.004 |
| % PId | 65.63 (±48.25) | 46.88 (±50.70) | 0.083 |
| % BoP | 100 (±0.00) | 56.25 (±50.40) | <0.001 |
| Total Number of Implants (n = 88) | Implants of PIM Group (n = 56) | Implants of PI Group (n = 32) | p-Value | ||
|---|---|---|---|---|---|
| Arch, n (%) | Upper | 40 (45.45%) | 30 (34.09%) | 10 (11.36%) | 0.002 |
| Lower | 48 (54.55%) | 26 (29.55%) | 22 (25%) | 0.564 | |
| p-value | 0.394 | 0.593 | 0.34 | ||
| Position, n (%) | Anterior (canine-canine) | 13 (14.77%) | 8 (14.28%) | 5 (15.62%) | 0.405 |
| Posterior | 75 (85.23%) | 48 (85.72%) | 27 (84.38%) | 0.015 | |
| p-value | <0.001 | <0.001 | <0.001 | ||
| Type of prosthetic platform | Morse Taper | 40 (45.45%) | 32 (57.14%) | 8 (25%) | <0.001 |
| External Hexagon | 48 (54.55%) | 24 (42.86%) | 24 (75%) | 1.000 | |
| p-value | 0.394 | 0.285 | 0.005 | ||
| Cemented or screwed | Cemented | 40 (45.45%) | 27 (48.21%) | 13 (40.62%) | 0.027 |
| Screwed | 48 (54.55%) | 29 (51.79%) | 19 (59.38%) | 0.149 | |
| p-value | 0.394 | 0.789 | 0.289 | ||
| Splinted or non-splinted | Splinted | 32 (36.37%) | 9 (16.08%) | 23 (71.88%) | 0.013 |
| Non-splinted | 56 (63.63%) | 47 (83.92%) | 9 (28.12%) | <0.001 | |
| p-value | 0.011 | <0.001 | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonçalves, L.T.d.C.; Neves, G.S.T.; da Silva, A.M.P.; Telles, D.d.M.; Figueredo, C.M.d.S.; Lourenço, E.J.V.; Teixeira, M.K.S. The Effect of Peri-Implant Therapy on the Expression of Th17-Related Cytokines in Patients with Peri-Implant Mucositis and Peri-Implantitis: A Prospective Longitudinal Study. J. Clin. Med. 2025, 14, 340. https://doi.org/10.3390/jcm14020340
Gonçalves LTdC, Neves GST, da Silva AMP, Telles DdM, Figueredo CMdS, Lourenço EJV, Teixeira MKS. The Effect of Peri-Implant Therapy on the Expression of Th17-Related Cytokines in Patients with Peri-Implant Mucositis and Peri-Implantitis: A Prospective Longitudinal Study. Journal of Clinical Medicine. 2025; 14(2):340. https://doi.org/10.3390/jcm14020340
Chicago/Turabian StyleGonçalves, Líssya Tomaz da Costa, Glaucia Schuindt Teixeira Neves, Alexandre Marques Paes da Silva, Daniel de Moraes Telles, Carlos Marcelo da Silva Figueredo, Eduardo José Veras Lourenço, and Mayla Kezy Silva Teixeira. 2025. "The Effect of Peri-Implant Therapy on the Expression of Th17-Related Cytokines in Patients with Peri-Implant Mucositis and Peri-Implantitis: A Prospective Longitudinal Study" Journal of Clinical Medicine 14, no. 2: 340. https://doi.org/10.3390/jcm14020340
APA StyleGonçalves, L. T. d. C., Neves, G. S. T., da Silva, A. M. P., Telles, D. d. M., Figueredo, C. M. d. S., Lourenço, E. J. V., & Teixeira, M. K. S. (2025). The Effect of Peri-Implant Therapy on the Expression of Th17-Related Cytokines in Patients with Peri-Implant Mucositis and Peri-Implantitis: A Prospective Longitudinal Study. Journal of Clinical Medicine, 14(2), 340. https://doi.org/10.3390/jcm14020340