
Comparative Clinical Characteristics, Laboratory Findings, and Outcomes of Hypoxemic and Non-Hypoxemic Patients Treated at a Makeshift COVID-19 Unit in Bangladesh: A Retrospective Chart Analysis

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Operational Definition
- (A)
- (B)
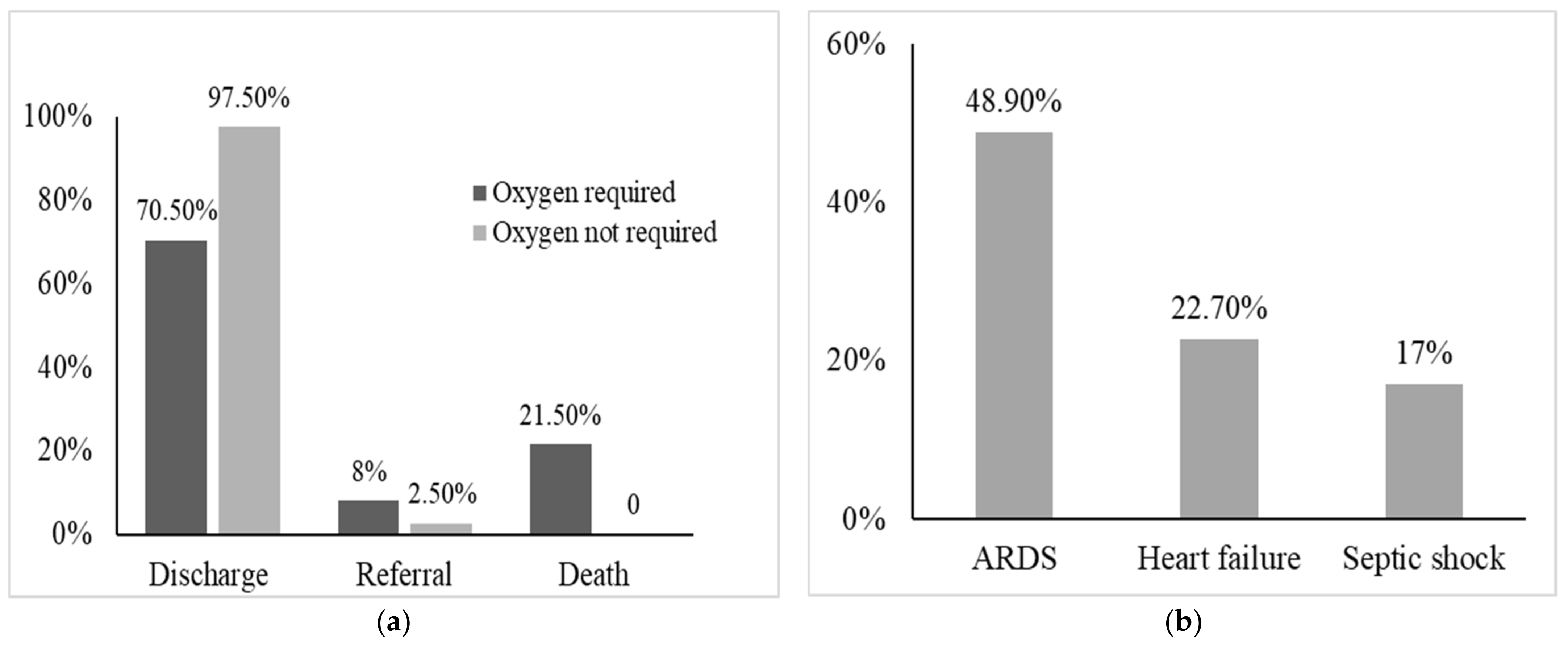
- Acute Respiratory Distress Syndrome (ARDS)
- (C)
- Heart failure
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-COVID-19—11-march-2020 (accessed on 10 February 2021).
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 5 May 2022).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard: Bangladesh. Available online: https://covid19.who.int/region/searo/country/bd (accessed on 10 February 2021).
- Centers for Disease Control and Prevention. Symptoms of Coronavirus. Available online: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html (accessed on 10 February 2021).
- Directorate General of Health Services. National Guidelines on Clinical Management of Coronavirus Disease 2019 (COVID-19). 2020. Available online: https://old.dghs.gov.bd/index.php/bd/publication/guideline (accessed on 5 November 2020).
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease Is Suspected: Interim Guidance, 13 March 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Kache, S.; Chisti, M.J.; Gumbo, F.; Mupere, E.; Zhi, X.; Nallasamy, K.; Nakagawa, S.; Lee, J.H.; di Nardo, M.; de la Oliva, P.; et al. COVID-19 PICU guidelines: For high- and limited-resource settings. Pediatr. Res. 2020, 88, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Karim, M.M.; Ross, A.G.; Hossain, M.S.; Clemens, J.D.; Sumiya, M.K.; Phru, C.S.; Rahman, M.; Zaman, K.; Somani, J.; et al. A five-day course of ivermectin for the treatment of COVID-19 may reduce the duration of illness. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2021, 103, 214–216. [Google Scholar] [CrossRef] [PubMed]
- Izcovich, A.; Peiris, S.; Ragusa, M.; Tortosa, F.; Rada, G.; Aldighieri, S.; Reveiz, L. Bias as a source of inconsistency in ivermectin trials for COVID-19: A systematic review. Ivermectin’s suggested benefits are mainly based on potentially biased results. J. Clin. Epidemiol. 2022, 144, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Chen, R.; Liang, W.; Jiang, M.; Guan, W.; Zhan, C.; Wang, T.; Tang, C.; Sang, L.; Liu, J.; Ni, Z. Risk factors of fatal outcome in hospitalized subjects with coronavirus disease 2019 from a nationwide analysis in China. Chest 2020, 158, 97–105. [Google Scholar] [CrossRef]
- Lin, W.T.; Hung, S.H.; Lai, C.C.; Wang, C.Y.; Chen, C.H. The impact of neutralizing monoclonal antibodies on the outcomes of COVID-19 outpatients: A systematic review and meta-analysis of randomized controlled trials. J. Med. Virol. 2022, 94, 2222–2229. [Google Scholar] [CrossRef]
- Dessie, Z.G.; Zewotir, T. Mortality-related risk factors of COVID-19: A systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect. Dis. 2021, 21, 855. [Google Scholar] [CrossRef]
- Oliveira, E.; Parikh, A.; Lopez-Ruiz, A.; Carrilo, M.; Goldberg, J.; Cearras, M.; Fernainy, K.; Andersen, S.; Mercado, L.; Guan, J. ICU outcomes and survival in patients with severe COVID-19 in the largest health care system in central Florida. PLoS ONE 2021, 16, e0249038. [Google Scholar] [CrossRef]
- Armstrong, R.; Kane, A.; Kursumovic, E.; Oglesby, F.; Cook, T.M. Mortality in patients admitted to intensive care with COVID-19: An updated systematic review and meta-analysis of observational studies. Anaesthesia 2021, 76, 537–548. [Google Scholar] [CrossRef]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J. Development and validation of a clinical risk score to predict the occurrence of critical illness in hospitalized patients with COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef]
- Caramelo, F.; Ferreira, N.; Oliveiros, B. Estimation of risk factors for COVID-19 mortality-preliminary results. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Parohan, M.; Yaghoubi, S.; Seraji, A.; Javanbakht, M.H.; Sarraf, P.; Djalali, M. Risk factors for mortality in patients with Coronavirus disease 2019 (COVID-19) infection: A systematic review and meta-analysis of observational studies. Aging Male 2021, 23, 1416–1424. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Choi, K.W.; Chau, T.N.; Tsang, O.; Tso, E.; Chiu, M.C.; Tong, W.L.; Lee, P.O.; Ng, T.K.; Ng, W.F.; Lee, K.C. Outcomes and prognostic factors in 267 patients with severe acute respiratory syndrome in Hong Kong. Ann. Intern. Med. 2003, 139, 715–723. [Google Scholar] [CrossRef] [Green Version]
- Hong, K.-H.; Choi, J.-P.; Hong, S.-H.; Lee, J.; Kwon, J.-S.; Kim, S.-M.; Park, S.Y.; Rhee, J.-Y.; Kim, B.-N.; Choi, H.J. Predictors of mortality in Middle East respiratory syndrome (MERS). Thorax 2018, 73, 286–289. [Google Scholar] [CrossRef]
- Opal, S.M.; Girard, T.D.; Ely, E.W. The immunopathogenesis of sepsis in elderly patients. Clin. Infect. Dis. 2005, 41, S504–S512. [Google Scholar] [CrossRef] [Green Version]
- Shinkai, S.; Konishi, M.; Shephard, R.J. Aging and immune response to exercise. Can. J. Physiol. Pharmacol. 1998, 76, 562–572. [Google Scholar] [CrossRef]
- Shaw, A.C.; Goldstein, D.R.; Montgomery, R.R. Age-dependent dysregulation of innate immunity. Nat. Rev. Immunol. 2013, 13, 875–887. [Google Scholar] [CrossRef] [Green Version]
- Omar, S.; Clarke, R.; Abdullah, H.; Brady, C.; Corry, J.; Winter, H.; Touzelet, O.; Power, U.F.; Lundy, F.; McGarvey, L.P. Respiratory virus infection up-regulates TRPV1, TRPA1 and ASICS3 receptors on airway cells. PLoS ONE 2017, 12, e0171681. [Google Scholar] [CrossRef] [Green Version]
- Cavallazzi, R.; Ramirez, J.A. Influenza and viral pneumonia. Clin. Chest Med. 2018, 39, 703–721. [Google Scholar] [CrossRef]
- Komorowski, M.; Aberegg, S.K. Using applied lung physiology to understand COVID-19 patterns. Br. J. Anaesth. 2020, 125, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Chiumello, D.; Caironi, P.; Busana, M.; Romitti, F.; Brazzi, L.; Camporota, L. COVID-19 pneumonia: Different respiratory treatments for different phenotypes? Intensiv. Care Med. 2020, 46, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- Macintyre, S.; Samols, D.; Dailey, P. Two carboxylesterases bind C-reactive protein within the endoplasmic reticulum and regulate its secretion during the acute phase response. J. Biol. Chem. 1994, 269, 24496–24503. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W. Dysregulation of immune response in patients with coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Cao, Q.; Qin, L.; Wang, X.; Cheng, Z.; Pan, A.; Dai, J.; Sun, Q.; Zhao, F.; Qu, J. Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19): A multi-center study in Wenzhou city, Zhejiang, China. J. Infect. 2020, 80, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Koozi, H.; Lengquist, M.; Frigyesi, A. C-reactive protein as a prognostic factor in intensive care admissions for sepsis: A Swedish multicenter study. J. Crit. Care 2020, 56, 73–79. [Google Scholar] [CrossRef]
- Heuertz, R.M.; Ahmed, N.; Webster, R.O. Peptides derived from C-reactive protein inhibit neutrophil alveolitis. J. Immunol. 1996, 156, 3412–3417. [Google Scholar]
- Luo, X.; Zhou, W.; Yan, X.; Guo, T.; Wang, B.; Xia, H.; Ye, L.; Xiong, J.; Jiang, Z.; Liu, Y. Prognostic value of C-reactive protein in patients with coronavirus 2019. Clin. Infect. Dis. 2020, 71, 2174–2179. [Google Scholar] [CrossRef]
- Zhang, H.; Shi, T.; Wu, X.; Zhang, X.; Wang, K.; Bean, D.; Dobson, R.; Teo, J.T.; Sun, J.; Zhao, P. Risk Prediction for Poor Outcome and Death in Hospital In-Patients with COVID-19: Derivation in Wuhan, China and External Validation in London, UK; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar] [CrossRef]
- Jafarzadeh, A.; Jafarzadeh, S.; Nozari, P.; Mokhtari, P.; Nemati, M. Lymphopenia an important immunological abnormality in patients with COVID-19: Possible mechanisms. Scand. J. Immunol. 2021, 93, e12967. [Google Scholar] [CrossRef]
- Zhao, Q.; Meng, M.; Kumar, R.; Wu, Y.; Huang, J.; Deng, Y.; Weng, Z.; Yang, L. Lymphopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A systemic review and meta-analysis. Int. J. Infect. Dis. 2020, 96, 131–135. [Google Scholar] [CrossRef]
- Henry, B.M. COVID-19, ECMO, and lymphopenia: A word of caution. Lancet Respir. Med. 2020, 8, e24. [Google Scholar] [CrossRef]
- Lee, N.; Hui, D.; Wu, A.; Chan, P.; Cameron, P.; Joynt, G.M.; Ahuja, A.; Yung, M.Y.; Leung, C.; To, K. A major outbreak of severe acute respiratory syndrome in Hong Kong. N. Engl. J. Med. 2003, 348, 1986–1994. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Oxygen Required (n = 88) | Oxygen Not Required (n = 119) | OR, 95%CI | p Value |
|---|---|---|---|---|
| Age (years) (median, IQR) | 58 (51.2, 65) | 42 (35, 54) | - | <0.001 |
| Sex, male | 54 (61.4) | 74 (62.7) | 0.94 (0.53–1.66) | 0.95 |
| Days from illness onset to admission (median, IQR) | 7 (4, 8) | 5 (3, 9.5) | - | 0.54 |
| Antibiotics before hospitalization | 18 (20.5) | 18 (15.1) | 1.44 (0.70–2.97) | 0.415 |
| Presence of comorbidity | ||||
| Hypertension | 54 (61.4) | 40 (33.6) | 3.13 (1.75–5.59) | <0.001 |
| Diabetes Mellitus | 41 (46.6) | 32 (26.9) | 2.37 (1.32–4.25) | 0.005 |
| Ischemic Heart Disease | 26 (29.9) | 7 (5.9) | 6.71 (2.75–16.34) | <0.001 |
| Chronic respiratory illness (asthma and COPD) | 15 (17.4) | 18 (15.5) | 1.15 (0.54–2.43) | 0.86 |
| Hypothyroidism | 8 (9.1) | 8 (6.7) | 1.39 (0.50–3.85) | 0.713 |
| Signs and symptoms | ||||
| Fever | 70 (80.5) | 82 (68.9) | 1.85 (0.96–3) | 0.08 |
| Cough | 57 (66.3) | 76 (64.4) | 0.81 (0.46–1.41) | 0.54 |
| Sore throat | 5 (5.8) | 13 (11.1) | 0.49 (0.16–1.44) | 0.28 |
| Headache | 13 (15.1) | 25 (21.4) | 0.65 (0.31–1.36) | 0.34 |
| Diarrhea | 10 (11.6) | 12 (10.3) | 1.15 (0.47–2.80) | 0.93 |
| Shortness of breath (SOB) | 48 (54.5) | 33 (27.7) | 3.13 (1.75–5.59) | <0.001 |
| Body ache/myalgia | 8 (9.4) | 19 (16.2) | 0.53 (0.22–1.28) | 0.23 |
| Systolic blood pressure | ||||
| Normotensive, <120 mm (ref) | 30 (36.6) | 47 (42.3) | - | - |
| Pre-hypertensive (120–139) mm of hg | 31 (37.8) | 44 (39.6) | 1.10 (0.58–2.11) | 0.894 |
| Hypertension (>140 mm of hg) | 21 (25.6) | 20 (18) | 1.64 (0.76–3.53) | 0.278 |
| Diastolic Blood Pressure | ||||
| Normotensive <80 mm of hg (ref) | 48 (58.5) | 46 (41.4) | - | - |
| Pre-hypertensive (80–89) mm of hg | 21 (25.6) | 37 (33.3) | 0.54 (0.28–1.06) | 0.105 |
| Hypertension >90 mm of hg | 13 (15.9) | 28 (25.2) | 0.44 (0.20–0.96) | 0.059 |
| Temperature >38 °C | 17 (21.2) | 8 (7.1) | 3.54 (1.44–8.68) | 0.007 |
| RBS (median, IQR) | 8 (6.3,10.7) | 7.35 (5.8,10.9) | - | 0.414 |
| Tachycardia (Heart rate > 100/min) | 27 (32.5) | 20 (17.7) | 0.44 (0.22–0.86) | 0.025 |
| Tachypnoea (Respiratory rate > 30/min) | 39 (50) | 10 (9.1) | 10 (4.55–21.9) | <0.001 |
| Characteristics | Patients Required Oxygen (n = 88) | Patients Required No Oxygen (n = 119) | OR, 95% CI | p Value |
|---|---|---|---|---|
| Complete Blood Count | ||||
| Hb (g/dL) | 12.2 ± 1.6 | 12.5 ± 1.6 | - | 0.191 |
| Leukocytosis or leucopenia | 23 (28) | 9 (11.7) | 2.94 (1.26–6.86) | 0.018 |
| Lymphopenia | 54 (65.9) | 18 (23.4) | 6.32 (3.15–12.7) | 0.000 |
| Platelet (×109/L) | 211.35 ± 89.8 | 229.1± 91.1 | - | 0.218 |
| CRP (mg/dL) | 9.4 (3.0, 19.9) | 1.3 (0.3, 4.5) | - | 0.001 |
| D-Dimer (pg/mL) | 659 (360.5, 1028.5) | 409.5 (277.1, 673.7) | - | 0.010 |
| Serum electrolyte | ||||
| Hyponatremia | 23 (31.9) | 8 (17.4) | 2.23 (0.9–5.53) | 0.124 |
| Hypokalemia | 18 (25.4) | 16 (34.8) | 0.64 (0.28–1.43) | 0.374 |
| Metabolic acidosis | 39 (54.9) | 9 (19.6) | 5.01 (2.11–11.91) | <0.001 |
| Normal renal function | 59 (90.8) | 37 (100) | - | 0.142 |
| Bilateral involvement in chest X-rays | 52 (67.5) | 9 (14.3) | 12.48 (5.32–29.25) | <0.001 |
| Characteristics | OR, 95% CI | p Value |
|---|---|---|
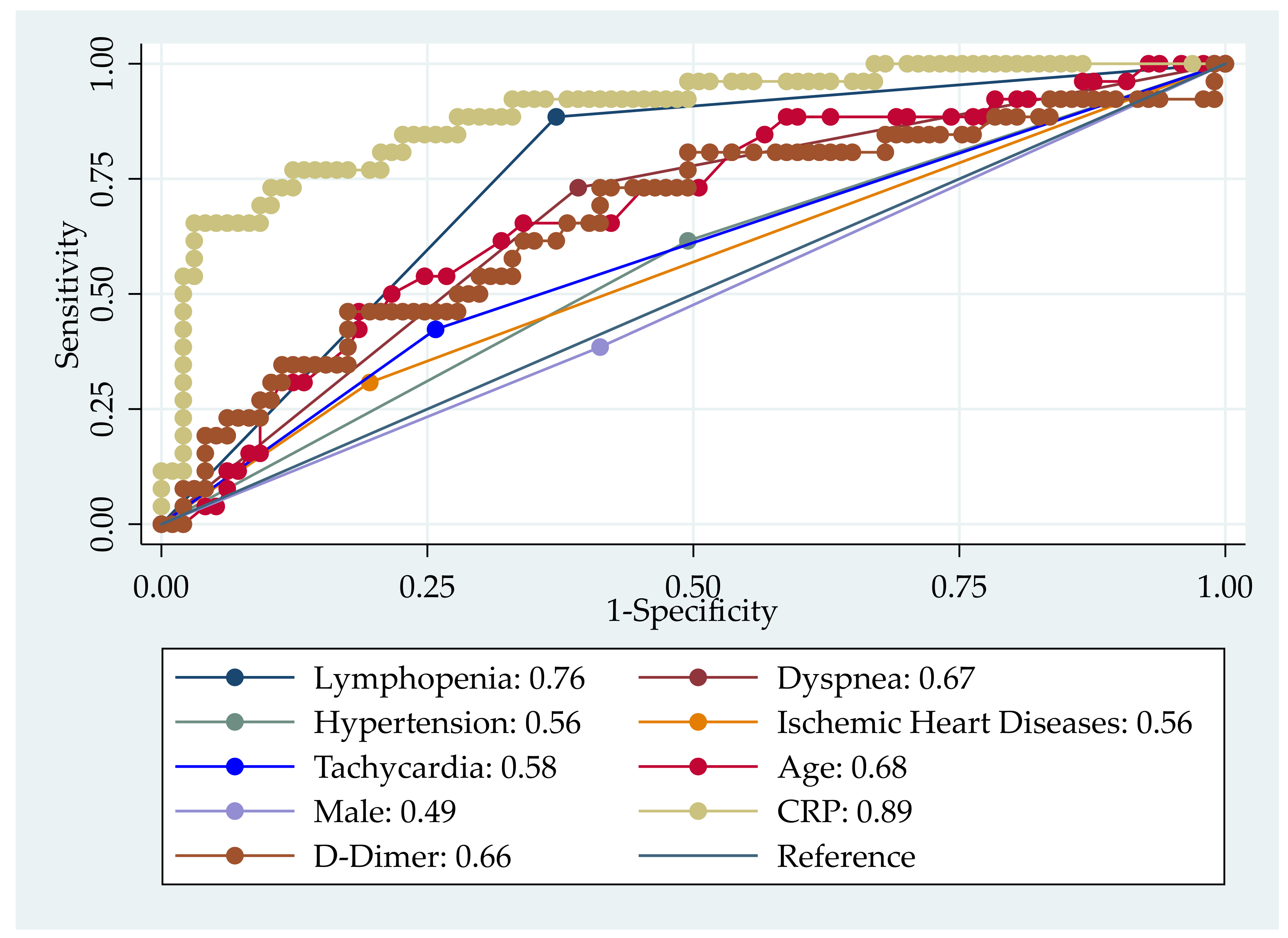
| Age | 1.07 (1.02–1.13) | 0.005 |
| Sex male | 0.54 (0.16–1.85) | 0.326 |
| Hypertension | 1.82 (0.56–5.92) | 0.319 |
| Ischemic Heart Diseases | 3.83 (0.81–18.24) | 0.091 |
| Diabetes Mellitus | 0.59 (0.15–2.24) | 0.437 |
| Dyspnea | 3.56 (1.06–11.96) | 0.040 |
| Fever | 1.16 (0.24–5.68) | 0.857 |
| Tachycardia | 1.48 (0.44–4.93) | 0.522 |
| Lymphopenia | 6.18 (1.81–21.10) | 0.004 |
| CRP | 1.13 (1.03–1.25) | 0.011 |
| D-Dimer | 1.0 (0.99–1.00) | 0.382 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarmin, M.; Mahfuz, M.; Shahrin, L.; Shaly, N.J.; Shaima, S.N.; Shikha, S.S.; Jeorge, D.H.; Islam, S.B.; Chisti, M.J.; Ahmed, T. Comparative Clinical Characteristics, Laboratory Findings, and Outcomes of Hypoxemic and Non-Hypoxemic Patients Treated at a Makeshift COVID-19 Unit in Bangladesh: A Retrospective Chart Analysis. J. Clin. Med. 2022, 11, 2968. https://doi.org/10.3390/jcm11112968
Sarmin M, Mahfuz M, Shahrin L, Shaly NJ, Shaima SN, Shikha SS, Jeorge DH, Islam SB, Chisti MJ, Ahmed T. Comparative Clinical Characteristics, Laboratory Findings, and Outcomes of Hypoxemic and Non-Hypoxemic Patients Treated at a Makeshift COVID-19 Unit in Bangladesh: A Retrospective Chart Analysis. Journal of Clinical Medicine. 2022; 11(11):2968. https://doi.org/10.3390/jcm11112968
Chicago/Turabian StyleSarmin, Monira, Mustafa Mahfuz, Lubaba Shahrin, Nusrat Jahan Shaly, Shamsun Nahar Shaima, Shamima Sharmin Shikha, Didarul Haque Jeorge, Shoeb Bin Islam, Mohammod Jobayer Chisti, and Tahmeed Ahmed. 2022. "Comparative Clinical Characteristics, Laboratory Findings, and Outcomes of Hypoxemic and Non-Hypoxemic Patients Treated at a Makeshift COVID-19 Unit in Bangladesh: A Retrospective Chart Analysis" Journal of Clinical Medicine 11, no. 11: 2968. https://doi.org/10.3390/jcm11112968