
A Randomized Controlled Trial Evaluating Integrative Psychotherapeutic Group Treatment Compared to Self-Help Groups in Functional Vertigo/Dizziness

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
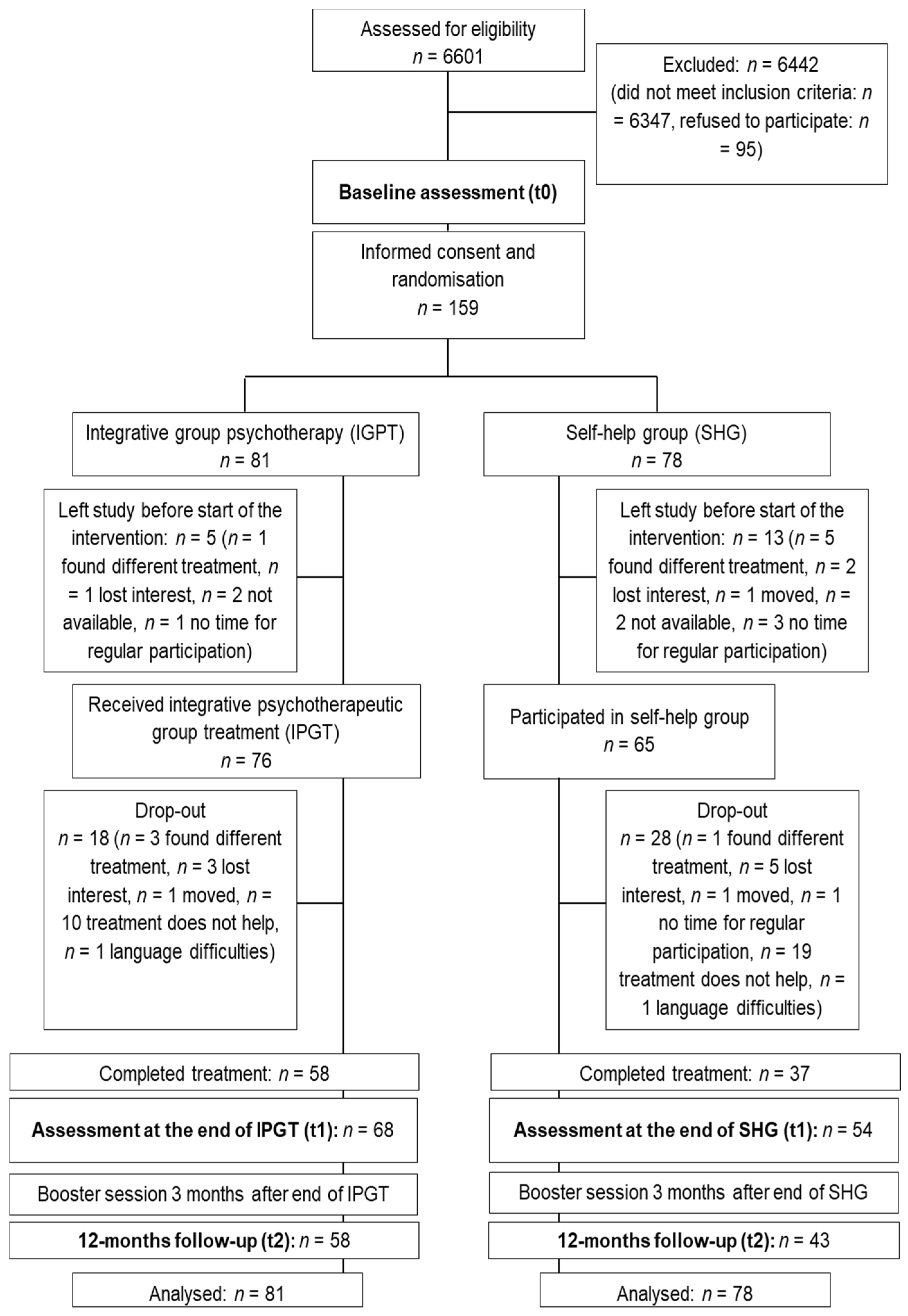
2.2. Participants
2.3. Interventions
2.4. Assessments and Outcomes
2.5. Sample Size
2.6. Randomization and Blinding
2.7. Ethical Issues
2.8. Statistical Analyses
3. Results
3.1. Changes in Primary and Secondary Outcomes
3.2. Linear Mixed Model Analyses
4. Discussion
5. Conclusions
- -
- We investigated the efficacy of an integrative psychotherapeutic group intervention (IPGT) for patients with functional vertigo and dizziness symptoms in comparison to an active control condition, a moderated self-help group (SHG).
- -
- Results indicate substantial and long-lasting improvements in the primary and nearly all secondary outcome measures assessing vertigo-related impairment, vertigo, symptom severity, mental HRQoL, and depression in both groups.
- -
- Unexpectedly, we did not see superior effects of IPGT compared to SHG. Hence, our results point at the potentially beneficial aspects of SHGs for our patient group. Therefore, assisting patients in establishing networks with others suffering from the same or similar condition may help to improve patient outcome.
- -
- It should be noted that while drop-out rates were generally high, patient acceptance was considerably higher in IPGT compared to SHG.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grill, E.; Heuberger, M.; Strobl, R.; Saglam, M.; Holle, R.; Linkohr, B.; Ladwig, K.-H.; Peters, A.; Schneider, E.; Jahn, K.; et al. Prevalence, Determinants, and consequences of vestibular hypofunction. results from the KORA-FF4 survey. Front. Neurol. 2018, 9, 1076. [Google Scholar] [CrossRef] [Green Version]
- Neuhauser, H. Epidemiologie von Schwindelerkrankungen. Nervenarzt 2009, 80, 887–894. [Google Scholar] [CrossRef]
- Neuhauser, H.; von Brevern, M.; Radtke, A.; Lezius, F.; Feldmann, M.; Ziese, T.; Lempert, T. Epidemiology of vestibular vertigo A neurotologic survey of the general population. Neurology 2005, 65, 898–904. [Google Scholar] [CrossRef]
- Neuhauser, H.; Radtke, A.; von Brevern, M.; Lezius, F.; Feldmann, M.; Lempert, T. Burden of dizziness and vertigo in the community. Arch. Intern. Med. 2008, 168, 2118–2124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dieterich, M.; Staab, J.P. Functional dizziness: From phobicpostural vertigo and chronic subjective dizziness to persistent postural-perceptual dizziness. Curr. Opin. Neurol. 2017, 30, 107–113. [Google Scholar] [CrossRef]
- Lahmann, C.; Henningsen, P.; Brandt, T.; Strupp, M.; Jahn, K.; Dieterich, M.; Eckhardt-Henn, A.; Feuerecker, R.; Dinkel, A.; Schmid, G. Psychiatric comorbidity and psychosocial impairment among patients with vertigo and dizziness. J. Neurol. Neurosurg. Psychiatry 2015, 86, 302–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Limburg, K.; Sattel, H.; Dinkel, A.; Radziej, K.; Becker-Bense, S.; Lahmann, C. Course and predictors of DSM-5 somatic symptom disorder in patients with vertigo and dizziness symptoms—A longitudinal study. Compr. Psychiatry 2017, 77, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Limburg, K.; Sattel, H.; Radziej, K.; Lahmann, C. DSM-5 somatic symptom disorder in patients with vertigo and dizziness symptoms. J. Psychosom. Res. 2016, 91, 26–32. [Google Scholar] [CrossRef]
- Nakao, M.; Yano, E. Somatic symptoms for predicting depression: One-year follow-up study in annual health examinations. Psychiatry Clin. Neurosci. 2006, 60, 219–225. [Google Scholar] [CrossRef]
- Probst, T.; Dinkel, A.; Schmid, G.; Limburg, K.; Radziej, K.; Pieh, C.; Lahmann, C. Psychological distress longitudinally mediates the effect vertigo symptoms exert on vertigo-related handicaps—Follow-up results of the Munich diagnostic and predictor study. J. Psychosom. Res. 2017, 93, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Schmid, G.; Henningsen, P.; Dieterich, M.; Sattel, H.; Lahmann, C. Psychotherapy in dizziness: A systematic review. J. Neurol. Neurosurg. Psychiatry 2011, 82, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Edelman, S.; Mahoney, A.E.; Cremer, P.D. Cognitive behaviour therapy for chronic subjective dizziness: A randomized, controlled trial. Am. J. Otolaryngol. 2012, 33, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, A.E.; Edelman, S.; Cremer, P.D. Cognitive behaviour therapy for chronic subjective dizziness: Longer-term gains and predictors of disability. Am. J. Otolaryngol. 2013, 34, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Tschan, R.; Eckhardt-Henn, A.; Scheurich, V.; Best, C.; Dieterich, M.; Beutel, M.E. Steadfast—Effectiveness of a cognitive-behavioural self-management program for patients with somatoform vertigo and dizziness. Psychother. Psychosom. Med. Psychol. 2012, 62, 111–119. [Google Scholar] [PubMed]
- Schmid, D.A.; Allum, J.H.; Sleptsova, M.; Gross, S.; Gaab, J.; Welge-Lüssen, A.; Schaefert, R.; Langewitz, W. Effects of a program of cognitive-behavioural group therapy, vestibular rehabilitation, and psychoeducational explanations on patients with dizziness and no quantified balance deficit, compared to patients with dizziness and a quantified balance deficit. J. Psychosom. Res. 2018, 105, 21–30. [Google Scholar] [CrossRef]
- Toshishige, Y.; Kondo, M.; Kabaya, K.; Watanabe, W.; Fukui, A.; Kuwabara, J.; Nakayama, M.; Iwasaki, S.; Furukawa, T.A.; Akechi, T. Cognitive-behavioural therapy for chronic subjective dizziness: Predictors of improvement in Dizziness Handicap Inventory at 6 months posttreatment. Acta Otolaryngol. 2020, 140, 827–832. [Google Scholar] [CrossRef]
- Kuwabara, J.; Kondo, M.; Kabaya, K.; Watanabe, W.; Shiraishi, N.; Sakai, M.; Toshishige, Y.; Ino, K.; Nakayama, M.; Iwasaki, S.; et al. Acceptance and commitment therapy combined with vestibular rehabilitation for persistent postural-perceptual dizziness: A pilot study. Am. J. Otolaryngol. 2020, 41, 102609. [Google Scholar] [CrossRef]
- Baydan, M.; Yigit, O.; Aksoy, S. Does vestibular rehabilitation improve postural control of subjects with chronic subjective dizziness? PLoS ONE 2020, 15, e0238436. [Google Scholar] [CrossRef]
- Stikkelbroek, Y.; Bodden, D.H.; Deković, M.; van Baar, A.L. Effectiveness and cost effectiveness of cognitive behavioural therapy (CBT) in clinically depressed adolescents: Individual CBT versus treatment as usual (TAU). BMC Psychiatry 2013, 13, 314. [Google Scholar] [CrossRef] [Green Version]
- Holmberg, J.; Karlberg, M.; Harlacher, U.; Rivano-Fischer, M.; Magnusson, M. Treatment of phobic postural vertigo. J. Neurol. 2006, 253, 500–506. [Google Scholar] [CrossRef]
- Lahmann, C.; Henningsen, P.; Dieterich, M.; Radziej, K.; Schmid, G. Tailored care for somatoform vertigo/dizziness: Study protocol for a randomised controlled trial evaluating integrative group psychotherapy. J. Neurol. 2015, 262, 1867–1875. [Google Scholar] [CrossRef] [PubMed]
- Radziej, K.; Schmid-Mühlbauer, G.; Limburg, K.; Lahmann, C. Tailored Care for Functional Vertigo/Dizziness—An Integrative Group Psychotherapy Approach. Psychother. Psychosom. Med. Psychol. 2017, 67, 245–251. [Google Scholar]
- Sattel, H.; Lahmann, C.; Gündel, H.; Guthrie, E.; Kruse, J.; Noll-Hussong, M.; Ohmann, C.; Ronel, J.; Sack, M.; Sauer, N.; et al. Brief psychodynamic interpersonal psychotherapy for patients with multisomatoform disorder: Randomised controlled trial. Br. J. Psychiatry 2012, 200, 60–67. [Google Scholar] [CrossRef]
- Jacob, R.G.; Redfern, M.S.; Furman, J.M. Space and motion discomfort and abnormal balance control in patients with anxiety disorders. J. Neurol. Neurosurg. Psychiatry 2009, 80, 74–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schniepp, R.; Wuehr, M.; Huth, S.; Pradhan, C.; Brandt, T.; Jahn, K. Gait characteristics of patients with phobic postural vertigo: Effects of fear of falling, attention, and visual input. J. Neurol. 2014, 261, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Schniepp, R.; Wuehr, M.; Pradhan, C.; Novozhilov, S.; Krafczyk, S.; Brandt, T.; Jahn, K. Nonlinear Variability of Body Sway in Patients with Phobic Postural Vertigo. Front. Neurol. 2013, 4, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wuehr, M.; Brandt, T.; Schniepp, R. Distracting attention in phobic postural vertigo normalizes leg muscle activity and balance. Neurology 2017, 88, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Wuehr, M.; Pradhan, C.; Novozhilov, S.; Krafczyk, S.; Brandt, T.; Jahn, K.; Schniepp, R. Inadequate interaction between open—and closed—loop postural control in phobic postural vertigo. J. Neurol. 2013, 260, 1314–1323. [Google Scholar] [CrossRef]
- Structured Clinical Interview for DSM-IV. Available online: http://hdl.handle.net/11858/00-001M-0000-000E-AAB2-2 (accessed on 28 April 2021).
- Tschan, R.; Wiltink, J.; Best, C.; Beutel, M.E.; Dieterich, M.; Eckhardt-Henn, A. Deutschsprachige Validierung des Vertigo Handicap Questionnaire (VHQ) anhand einer Patientenstichprobe mit vestibulärem und somatoformem Schwindel. Psychother. Psychosom. Med. Psychol. 2010, 60, e1–e12. [Google Scholar] [CrossRef]
- Yardley, L.; Putman, J. Quantitative analysis of factors contributing to handicap and distress in vertiginous patients: A questionnaire study. Clin. Otolaryngol. 1992, 17, 231–236. [Google Scholar] [CrossRef]
- Tschan, R.; Wiltink, J.; Best, C.; Bense, S.; Dieterich, M.; Beutel, M.E.; Eckhardt-Henn, A. Validation of the German version of the Vertigo Symptom Scale (VSS) in patients with organic or somatoform dizziness and healthy controls. J. Neurol. 2008, 255, 1168–1175. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J. The PHQ-15: Validity of a New Measure for Evaluating the Severity of Somatic Symptoms. Psychosom. Med. 2002, 64, 258–266. [Google Scholar] [CrossRef] [Green Version]
- Margraf, J.; Ehlers, A. Deutschsprachige Adaptation des Beck Anxiety Inventory von AT Beck und RA Stern [German Adaptation of the Beck Anxiety Inventory by AT Beck and RA Stern]; Huber: Bern, Switzerland, 2007. [Google Scholar]
- Hautzinger, M.; Keller, F.; Kühner, C. Beck Depressions-Inventar (BDI-II); Hogrefe Verlag: Göttingen, Germany, 2006. [Google Scholar]
- Bullinger, M.; Morfeld, M.; Kohlmann, T.; Nantke, J.; van den Bussche, H.; Dodt, B.; Dunkelberg, S.; Kirchberger, I.; Krüger-Bödecker, A.; Lachmann, A.; et al. SF-36 Health Survey in Rehabilitation Research. Findings from the North German Network for Rehabilitation Research, NVRF, within the rehabilitation research funding program. Rehabilitation 2003, 42, 218–225. [Google Scholar]
- Morfeld, M.; Kirchberger, I.; Bullinger, M. SF-36 Fragebogen zum Gesundheitszustand; 2. ergänzte und überarbeitete Auflage; Hogrefe: Göttingen, Germany, 2011. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Angst, F.; Aeschlimann, A.; Angst, J. The minimal clinically important difference raised the significance of outcome effects above the statistical level, with methodological implications for future studies. J. Clin. Epidemiol. 2017, 82, 128–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, J.D.; Willett, J.B. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- IBM SPSS Statistics for Windows, Version 24.0; IBM Corp.: Armonk, NY, USA, 2016.
- Bates, D.; Mächler, M.; Bolker, B.M.; Walker, S.C. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Kristiansen, L.; Magnusson, L.H.; Juul-Kristensen, B.; Maeland, S.; Nordahl, S.H.G.; Hovland, A.L.; Sjobo, T.; Wilhelm, K. Feasibility of integrating vestibular rehabilitation and cognitive behaviour therapy for people with persistent dizziness. Pilot Feasability Study 2019, 5, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falkenström, F.; Granström, F.; Holmqvist, R. Therapeutic alliance predicts symptomatic improvement session by session. J. Couns. Psychol. 2013, 60, 317. [Google Scholar] [CrossRef] [Green Version]
- Falkenström, F.; Granström, F.; Holmqvist, R. Working alliance predicts psychotherapy outcome even while controlling for prior symptom improvement. Psychother. Res. 2014, 24, 146–159. [Google Scholar] [CrossRef]
- Mulder, R.; Murray, G.; Rucklidge, J. Common versus specific factors in psychotherapy: Opening the black box. Lancet 2017, 4, 953–962. [Google Scholar] [CrossRef]
- Nassan-Agha-Schroll, H.; Feichtinger, R.; Steidl, J.; Aigner, M. Das Symptom Schwindel im Fokus der Psychiatrie. Psychopraxis Neuropraxis 2020, 23, 36–40. [Google Scholar] [CrossRef]
- Brandt, T.; Huppert, D.; Dieterich, M. Phobic postural vertigo: A first follow-up. J. Neurol. 1994, 241, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Huppert, D.; Strupp, M.; Rettinger, N.; Hecht, J.; Brandt, T. Phobic postural vertigo. J. Neurol. 2005, 252, 564–569. [Google Scholar] [CrossRef] [PubMed]
- van Gils, A.; Schoevers, R.A.; Bonvanie, I.J.; Gelauff, J.M.; Roest, A.M.; Rosmalen, J.G. Self-help for medically unexplained symptoms: A systematic review and meta-analysis. Psychosom. Med. 2016, 78, 728–739. [Google Scholar] [CrossRef] [PubMed]
- Burlingame, G.M.; McClendon, D.T.; Alonso, J. Cohesion in group therapy. Psychotherapy 2011, 48, 34. [Google Scholar] [CrossRef] [PubMed]
- Payne, A.; Blanchard, E.B. A controlled comparison of cognitive therapy and self-help support groups in the treatment of irritable bowel syndrome. J. Consult. Clin. Psychol. 1995, 63, 779. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, E.B.; Lackner, J.M.; Sanders, K.; Krasnder, S.; Keefer, L.; Payne, A.; Gudleski, G.; Katz, L.; Rowell, D.; Sykes, M.; et al. A controlled evaluation of group cognitive therapy in the treatment of irritable bowel syndrome. Behav. Res. Ther. 2007, 45, 633–648. [Google Scholar] [CrossRef]
- Katsamanis, M.; Lehrer, P.M.; Escobar, J.I.; Gara, M.A.; Kotay, A.; Liu, R. Psychophysiological treatment for patients with medically unexplained symptoms: A randomized controlled trial. Psychosomatics 2011, 52, 218–229. [Google Scholar] [CrossRef] [Green Version]
- Thompson, K.J.; Goetting, J.C.; Staab, J.P.; Shepard, N.T. Retrospective review and telephone follow-up to evaluate a physical therapy protocol for treating persistent postural-perceptual dizziness: A pilot study. J. Vestib. Res. 2015, 25, 97–104. [Google Scholar]
- Wortman, M.S.; Lokkerbol, J.; van der Wouden, J.C.; Visser, B.; van der Horst, H.E.; Olde Hartman, T.C. Cost-effectiveness of interventions for medically unexplained symptoms: A systematic review. PLoS ONE 2018, 13, e0205278. [Google Scholar] [CrossRef]


{kind=link}
| IPGT (n = 81) | SHG (n = 78) | t or Χ2 | p | |
|---|---|---|---|---|
| Age at entry, M (SD) | 53.7 (15.4) | 53.5 (15.1) | t = −0.11 | 0.917 |
| Female, n (%) | 49 (60.5) | 49 (62.8) | Χ2 = 0.09 | 0.871 |
| Education, n (%) | Χ2 = 9.89 | 0.042 | ||
| 9th grade or less | 20 (24.7) | 14 (17.9) | ||
| 10th grade | 25 (30.9) | 19 (24.4) | ||
| High school graduate | 14 (17.3) | 17 (21.8) | ||
| University graduate | 16 (19.7) | 17 (21.8) | ||
| Missing information | 6 (7.4) | 11 (14.1) | ||
| Married, n (%) | 33 (40.7) | 42 (53.8) | Χ2 = 6.08 | 0.108 |
| Employment status, n (%) | Χ2 = 4.21 | 0.648 | ||
| Employed | 42 (51.9) | 40 (51.3) | ||
| Unemployed | 3 (3.7) | 3 (3.8) | ||
| Retired | 24 (29.6) | 22 (28.3) | ||
| Other | 12 (14.8) | 13 (16.6) | ||
| Psychiatric diagnosis, n (%) | ||||
| Depressive disorder | 19 (23.5) | 17 (21.8) | Χ2 = 0.06 | 0.802 |
| Anxiety disorder | 38 (46.9) | 34 (43.6) | Χ2 = 0.18 | 0.674 |
| Other | 9 (11.1) | 9 (11.5) | Χ2 = 0.01 | 0.932 |
| Symptom duration, n (%) | Χ2 = 3.07 | 0.547 | ||
| <1–3 months | 12 (14.8) | 6 (7.7) | ||
| 3 months–2 years | 36 (44.4) | 39 (50.0) | ||
| 2–10 years | 28 (34.6) | 28 (35.9) | ||
| >10 years | 5 (6.2) | 5 (6.4) | ||
| Previous psychotherapy, n (%) | 33 (40.7) | 16 (20.5) | Χ2 = 5.75 | 0.017 |
| Drop-out, n (%) | 23 (28.4) | 41 (52.6) | Χ2 = 9.65 | 0.002 |
| Phase | Sessions | Details |
|---|---|---|
| 1 | 1–4 |
|
| 2 | 5–13 |
|
| 3 | 14–16 |
|
| IPGT M (SD) | SHG M (SD) | Group Comparison at Baseline | Effect Sizes (Cohen’s d) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| t | p | IPGT vs. SHG | IPGT: T0–T1 | IPGT: T0–T2 | SHG: T0–T1 | SHG: T0–T2 | |||
| Vertigo-related handicap (VHQ sum score) | 1.10 | 1.06 | 0.86 | 1.29 | |||||
| Baseline | 57.34 (10.56) | 59.13 (12.04) | 0.99 | 0.32 | 0.16 | ||||
| End of treatment | 41.65 (17.16) | 45.54 (18.76) | 0.23 | ||||||
| 12-months follow-up | 39.95 (20.55) | 37.28 (20.77) | 0.13 | ||||||
| Restriction of activity (VHQ-ACT) | 0.95 | 0.97 | 0.83 | 1.24 | |||||
| Baseline | 2.21 (0.49) | 2.32 (0.47) | 1.48 | 0.14 | 0.24 | ||||
| End of treatment | 1.60 (0.75) | 1.78 (0.80) | 0.23 | ||||||
| 12-months follow-up | 1.53 (0.87) | 1.44 (0.89) | 0.11 | ||||||
| Vertigo-related anxiety (VHQ-ANX) | 0.81 | 0.77 | 0.45 | 0.86 | |||||
| Baseline | 2.61 (0.68) | 2.66 (0.78) | 0.45 | 0.66 | 0.07 | ||||
| End of treatment | 2.02 (0.78) | 2.28 (0.93) | 0.31 | ||||||
| 12-months follow-up | 1.93 (1.05) | 1.87 (1.04) | 0.06 | ||||||
| Vertigo severity (VSS-VER) | 0.20 | 0.72 | 0.05 | 0.44 | |||||
| Baseline | 1.30 (0.89) | 1.23 (0.69) | −0.47 | 0.64 | 0.09 | ||||
| End of treatment | 1.13 (0.84) | 1.19 (0.79) | 0.07 | ||||||
| 12-months follow-up | 0.75 (0.63) | 0.89 (0.82) | 0.19 | ||||||
| Autonomic Arousal (VSS-AA) | 0.15 | 0.35 | 0.15 | 0.38 | |||||
| Baseline | 1.52 (0.85) | 1.47 (0.77) | −0.34 | 0.73 | 0.06 | ||||
| End of treatment | 1.39 (0.81) | 1.35 (0.87) | 0.05 | ||||||
| 12-months follow-up | 1.23 (0.85) | 1.16 (0.85) | 0.08 | ||||||
| Somatization (PHQ-15) | 0.09 | 0.07 | 0.28 | 0.37 | |||||
| Baseline | 12.27 (5.31) | 12.38 (4.76) | −0.13 | 0.89 | 0.02 | ||||
| End of treatment | 11.0 (5.13) | 10.76 (6.04) | 0.04 | ||||||
| 12-months follow-up | 10.84 (5.67) | 9.95 (6.03) | 0.15 | ||||||
| Physical HRQoL (SF-12) | 0.20 | 0.01 | 0.20 | 0.58 | |||||
| Baseline | 40.08 (8.31) | 36.74 (9.58) | −1.83 | 0.07 | 0.37 | ||||
| End of treatment | 41.85 (9.55) | 38.75 (10.14) | 0.31 | ||||||
| 12-months follow-up | 40.22 (10.35) | 42.83 (11.42) | 0.24 | ||||||
| Mental HRQoL (SF-12) | 0.34 | 0.43 | 0.11 | 0.34 | |||||
| Baseline | 40.16 (10.54) | 41.63 (13.46) | 0.60 | 0.55 | 0.12 | ||||
| End of treatment | 43.85 (10.96) | 43.05 (12.64) | 0.07 | ||||||
| 12-months follow-up | 44.67 (10.49) | 45.94 (11.57) | 0.12 | ||||||
| Depression (BDI-II) | 0.26 | 0.39 | 0.33 | 0.42 | |||||
| Baseline | 15.51 (8.75) | 16.97 (11.15) | 0.88 | 0.38 | 0.15 | ||||
| End of treatment | 13.25 (8.92) | 13.56 (9.80) | 0.03 | ||||||
| 12-months follow-up | 12.36 (7.20) | 12.26 (11.34) | 0.01 | ||||||
| Anxiety (BAI) | 0.21 | 0.26 | 0.19 | 0.41 | |||||
| Baseline | 19.27 (12.10) | 18.69 (11.79) | −0.29 | 0.77 | 0.05 | ||||
| End of treatment | 16.78 (11.53) | 16.40 (12.08) | 0.03 | ||||||
| 12-months follow-up | 16.14 (12.07) | 13.74 (12.24) | 0.20 | ||||||
| Outcome | Predictors | b | SE | t | Lower | Upper | p |
|---|---|---|---|---|---|---|---|
| Vertigo−related handicap (VHQ sum score) | Time: T0–T1 | −11.99 | 2.08 | −5.77 | −16.06 | −7.92 | <0.001 |
| Time: T0–T2 | −21.55 | 2.59 | −8.32 | −26.63 | −16.48 | <0.001 | |
| Group | −1.15 | 2.13 | −0.54 | −5.32 | 3.03 | 0.59 | |
| Time (T0–T1) x group | −4.00 | 2.81 | −1.43 | −9.51 | 1.50 | 0.16 | |
| Time (T0–T2) x group | 4.15 | 3.46 | 1.20 | −2.64 | 10.94 | 0.23 | |
| Symptom duration | 1.17 | 1.26 | 0.93 | −1.29 | 3.63 | 0.35 | |
| Depressive disorder | 5.74 | 2.30 | 2.50 | 1.24 | 10.25 | 0.01 | |
| Anxiety disorder | −0.05 | 2.16 | −0.02 | −4.28 | 4.18 | 0.98 | |
| Previous psychotherapy | 2.20 | 2.25 | 0.98 | −2.21 | 6.61 | 0.33 | |
| Restriction of activity (VHQ−ACT) | Time: T0–T1 | −0.49 | 0.09 | −5.61 | −0.67 | −0.32 | <0.001 |
| Time: T0–T2 | −0.86 | 0.11 | −8.16 | −1.07 | −0.65 | <0.001 | |
| Group | −0.08 | 0.09 | −0.89 | −0.26 | 0.10 | 0.38 | |
| Time (T0–T1) x group | −0.14 | 0.12 | −1.17 | −0.37 | 0.09 | 0.24 | |
| Time (T0–T2) x group | 0.19 | 0.14 | 1.36 | −.08 | 0.47 | 0.18 | |
| Symptom duration | 0.04 | 0.05 | 0.73 | −0.07 | 0.15 | 0.47 | |
| Depressive disorder | 0.17 | 0.10 | 1.71 | −0.02 | 0.36 | 0.09 | |
| Anxiety disorder | −0.09 | 0.09 | −0.94 | −0.27 | 0.09 | 0.35 | |
| Previous psychotherapy | 0.07 | 0.10 | 0.67 | −0.12 | 0.25 | 0.50 | |
| Vertigo−related anxiety (VHQ−ANX) | Time: T0–T1 | −0.33 | 0.11 | −3.03 | −0.54 | −0.11 | 0.003 |
| Time: T0–T2 | −0.81 | 0.14 | −5.93 | −1.08 | −0.54 | <0.001 | |
| Group | −0.05 | 0.13 | −0.36 | −0.30 | 0.21 | 0.72 | |
| Time (T0–T1) x group | −0.26 | 0.14 | −1.83 | −0.55 | 0.02 | 0.07 | |
| Time (T0–T2) x group | 0.11 | 0.18 | 0.63 | −0.24 | 0.47 | 0.53 | |
| Symptom duration | 0.08 | 0.07 | 1.12 | −0.06 | 0.22 | 0.26 | |
| Depressive disorder | 0.24 | 0.13 | 1.80 | −0.02 | 0.50 | 0.07 | |
| Anxiety disorder | 0.21 | 0.12 | 1.67 | −0.04 | 0.45 | 0.10 | |
| Previous psychotherapy | 0.17 | 0.13 | 1.28 | −0.09 | 0.42 | 0.20 | |
| Vertigo severity (VSS−VER) | Time: T0–T1 | 0.01 | 0.10 | 0.13 | −0.18 | 0.21 | 0.89 |
| Time: T0–T2 | −0.31 | 0.12 | −2.48 | −0.55 | −0.06 | 0.01 | |
| Group | 0.07 | 0.15 | 0.47 | −0.22 | 0.36 | 0.64 | |
| Time (T0–T1) x group | −0.13 | 0.13 | −0.97 | −0.39 | 0.13 | 0.33 | |
| Time (T0–T2) x group | −0.22 | 0.17 | −1.31 | −0.55 | 0.11 | 0.19 | |
| Symptom duration | 0.18 | 0.08 | 2.40 | 0.04 | 0.34 | 0.02 | |
| Depressive disorder | 0.10 | 0.14 | 0.70 | −0.18 | 0.37 | 0.49 | |
| Anxiety disorder | −0.14 | 0.13 | −1.04 | −0.39 | 0.11 | 0.30 | |
| Previous psychotherapy | 0.18 | 0.14 | 1.30 | −0.09 | 0.44 | 0.20 | |
| Autonomic Arousal (VSS−AA) | Time: T0–T1 | −0.07 | 0.08 | −0.87 | −0.23 | 0.09 | 0.38 |
| Time: T0–T2 | −0.29 | 0.09 | −3.05 | −0.47 | −0.10 | 0.003 | |
| Group | 0.02 | 0.13 | 0.13 | −0.25 | 0.28 | 0.90 | |
| Time (T0–T1) x group | −0.03 | 0.11 | −0.25 | −0.24 | 0.19 | 0.81 | |
| Time (T0–T2) x group | 0.03 | 0.13 | 0.26 | −0.21 | 0.28 | 0.80 | |
| Symptom duration | 0.05 | 0.08 | 0.60 | −0.11 | 0.20 | 0.55 | |
| Depressive disorder | 0.18 | 0.15 | 1.22 | −0.11 | 0.47 | 0.23 | |
| Anxiety disorder | 0.09 | 0.14 | 0.65 | −0.18 | 0.36 | 0.52 | |
| Previous psychotherapy | 0.33 | 0.14 | 2.92 | 0.05 | 0.61 | 0.02 | |
| Somatisation (PHQ−15) | Time: T0–T1 | −1.38 | 0.52 | −2.64 | −2.4 | −0.35 | 0.009 |
| Time: T0–T2 | −2.13 | 0.62 | −3.42 | −3.36 | −0.91 | 0.0008 | |
| Group | −.29 | 0.83 | −0.35 | −1.92 | 1.33 | 0.73 | |
| Time (T0–T1) x group | −0.02 | 0.71 | 0−.03 | −1.4 | 1.36 | 0.98 | |
| Time (T0–T2) x group | 0.88 | 0.83 | 1.06 | −0.75 | 2.5 | 0.29 | |
| Symptom duration | 0.41 | 0.50 | 0.81 | −0.58 | 1.39 | 0.42 | |
| Depressive disorder | 2.88 | 0.91 | 3.16 | 1.09 | 4.67 | 0.001 | |
| Anxiety disorder | 0.29 | 0.86 | 0.34 | −1.4 | 1.98 | 0.73 | |
| Previous psychotherapy | 1.64 | 0.90 | 1.82 | −0.13 | 3.41 | 0.07 | |
| Physical HRQoL (SF−12) | Time: T0–T1 | 2.10 | 1.13 | 1.86 | −0.12 | 4.32 | 0.07 |
| Time: T0–T2 | 6.03 | 1.54 | 3.92 | 3.01 | 9.04 | <0.001 | |
| Group | 3.31 | 1.77 | 1.87 | −0.15 | 6.77 | 0.06 | |
| Time (T0–T1) x group | −0.16 | 1.57 | −0.10 | −3.24 | 2.92 | 0.92 | |
| Time (T0–T2) x group | −5.75 | 2.11 | −2.73 | −9.88 | −1.62 | 0.01 | |
| Symptom duration | −0.93 | 0.92 | −1.02 | −2.73 | 0.87 | 0.31 | |
| Depressive disorder | −0.65 | 1.73 | −0.38 | −4.04 | 2.74 | 0.71 | |
| Anxiety disorder | 1.88 | 1.58 | 1.19 | −1.22 | 4.98 | 0.24 | |
| Previous psychotherapy | −0.86 | 1.74 | −0.49 | −4.28 | 2.56 | 0.62 | |
| Mental HRQoL (SF−12) | Time: T0–T1 | 0.66 | 1.55 | 0.42 | −2.38 | 3.69 | 0.67 |
| Time: T0–T2 | 2.95 | 1.80 | 1.64 | −0.59 | 6.48 | 0.10 | |
| Group | −0.45 | 2.14 | −0.21 | −4.64 | 3.75 | 0.83 | |
| Time (T0–T1) x group | 3.31 | 2.15 | 1.54 | −0.91 | 7.52 | 0.13 | |
| Time (T0–T2) x group | 2.06 | 2.48 | 0.83 | −2.79 | 6.91 | 0.41 | |
| Symptom duration | 0.07 | 1.08 | 0.07 | −2.04 | 2.18 | 0.95 | |
| Depressive disorder | −8.32 | 2.03 | −4.11 | −12.30 | −4.35 | <0.001 | |
| Anxiety disorder | −1.74 | 1.85 | −0.94 | −5.37 | 1.89 | 0.35 | |
| Previous psychotherapy | −6.61 | 2.04 | −3.24 | −10.60 | −2.61 | 0.002 | |
| Depression (BDI−II) | Time: T0–T1 | −1.75 | 0.95 | −1.84 | −3.61 | 0.11 | 0.07 |
| Time: T0–T2 | −2.85 | 1.04 | −2.73 | −4.90 | −0.80 | 0.01 | |
| Group | −1.86 | 1.44 | −1.29 | 4.69 | 0.96 | 0.20 | |
| Time (T0–T1) x group | −0.55 | 1.27 | −0.43 | −3.05 | 1.95 | 0.67 | |
| Time (T0–T2) x group | 0.07 | 1.39 | 0.05 | −2.67 | 2.80 | 0.96 | |
| Symptom duration | 0.79 | 0.83 | 0.95 | −0.84 | 2.42 | 0.34 | |
| Depressive disorder | 9.08 | 1.54 | 5.91 | 6.07 | 12.09 | <0.001 | |
| Anxiety disorder | 2.42 | 1.43 | 1.69 | −0.39 | 5.23 | 0.09 | |
| Previous psychotherapy | 3.85 | 1.50 | 2.58 | 0.92 | 6.79 | 0.01 | |
| Anxiety (BAI) | Time: T0–T1 | −1.66 | 1.20 | −1.39 | −4.01 | 0.69 | 0.17 |
| Time: T0–T2 | −5.00 | 1.33 | −3.76 | −7.60 | −2.39 | <0.001 | |
| Group | 0.18 | 1.91 | 0.10 | −3.56 | 3.93 | 0.92 | |
| Time (T0–T1) x group | −0.39 | 1.62 | −0.24 | −3.56 | 2.78 | 0.81 | |
| Time (T0–T2) x group | 2.49 | 1.77 | 1.40 | −0.99 | 5.96 | 0.16 | |
| Symptom duration | 1.01 | 1.12 | 0.90 | −1.18 | 3.19 | 0.37 | |
| Depressive disorder | 6.24 | 2.06 | 3.04 | 2.21 | 10.28 | 0.003 | |
| Anxiety disorder | 2.25 | 1.93 | 1.17 | −1.52 | 6.03 | 0.24 | |
| Previous psychotherapy | 5.10 | 2.01 | 2.54 | 1.16 | 9.03 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Limburg, K.; Radziej, K.; Sattel, H.; Henningsen, P.; Dieterich, M.; Probst, T.; Dale, R.; Lahmann, C. A Randomized Controlled Trial Evaluating Integrative Psychotherapeutic Group Treatment Compared to Self-Help Groups in Functional Vertigo/Dizziness. J. Clin. Med. 2021, 10, 2215. https://doi.org/10.3390/jcm10102215
Limburg K, Radziej K, Sattel H, Henningsen P, Dieterich M, Probst T, Dale R, Lahmann C. A Randomized Controlled Trial Evaluating Integrative Psychotherapeutic Group Treatment Compared to Self-Help Groups in Functional Vertigo/Dizziness. Journal of Clinical Medicine. 2021; 10(10):2215. https://doi.org/10.3390/jcm10102215
Chicago/Turabian StyleLimburg, Karina, Katharina Radziej, Heribert Sattel, Peter Henningsen, Marianne Dieterich, Thomas Probst, Rachel Dale, and Claas Lahmann. 2021. "A Randomized Controlled Trial Evaluating Integrative Psychotherapeutic Group Treatment Compared to Self-Help Groups in Functional Vertigo/Dizziness" Journal of Clinical Medicine 10, no. 10: 2215. https://doi.org/10.3390/jcm10102215