
Radial Access for Coronary Angiography Carries Fewer Complications Compared with Femoral Access: A Meta-Analysis of Randomized Controlled Trials

 ,
,  , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Clinical Outcomes and Definitions
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
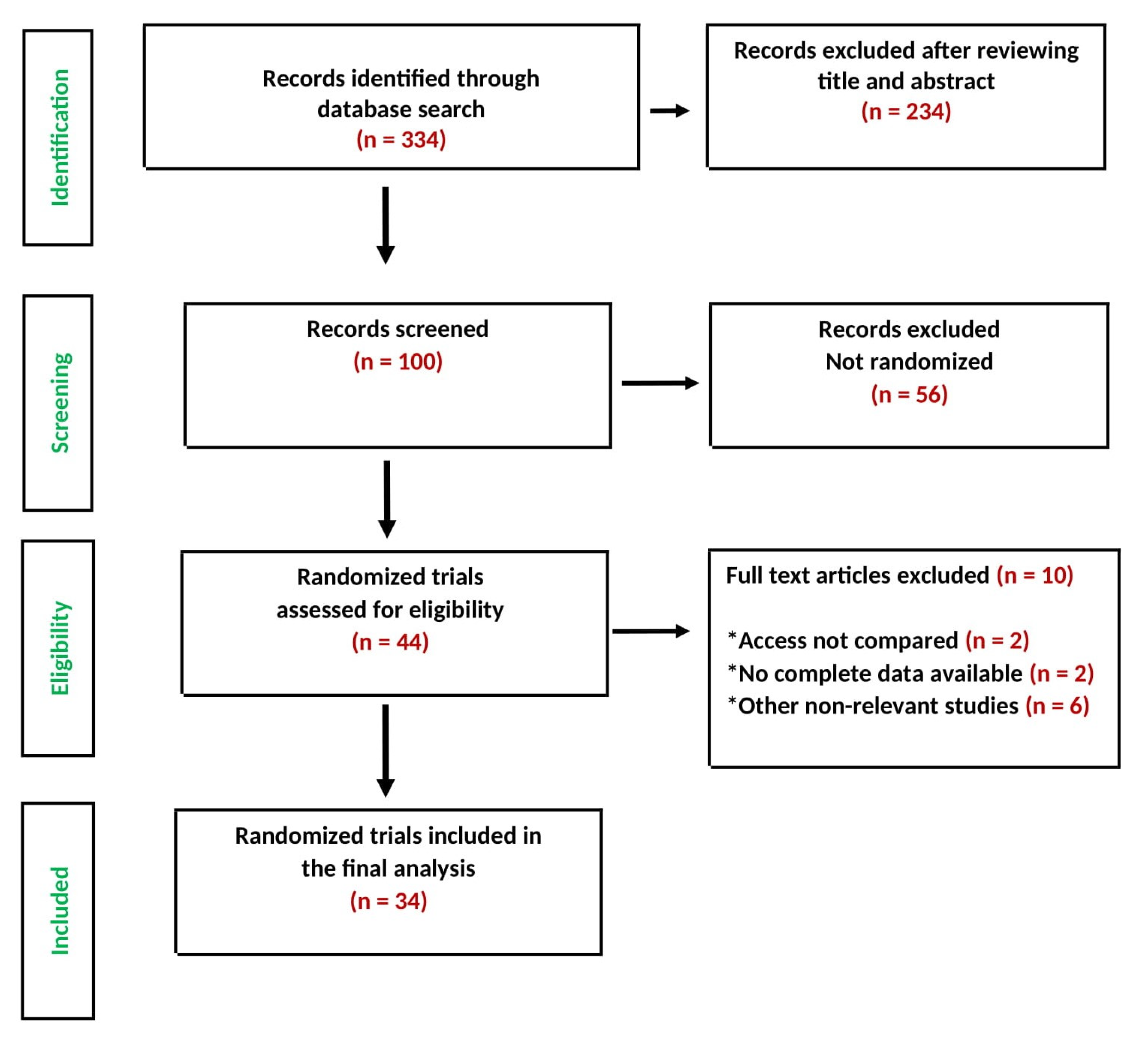
3.1. Search Results and Trial Flow
3.2. Characteristics of Included Patients
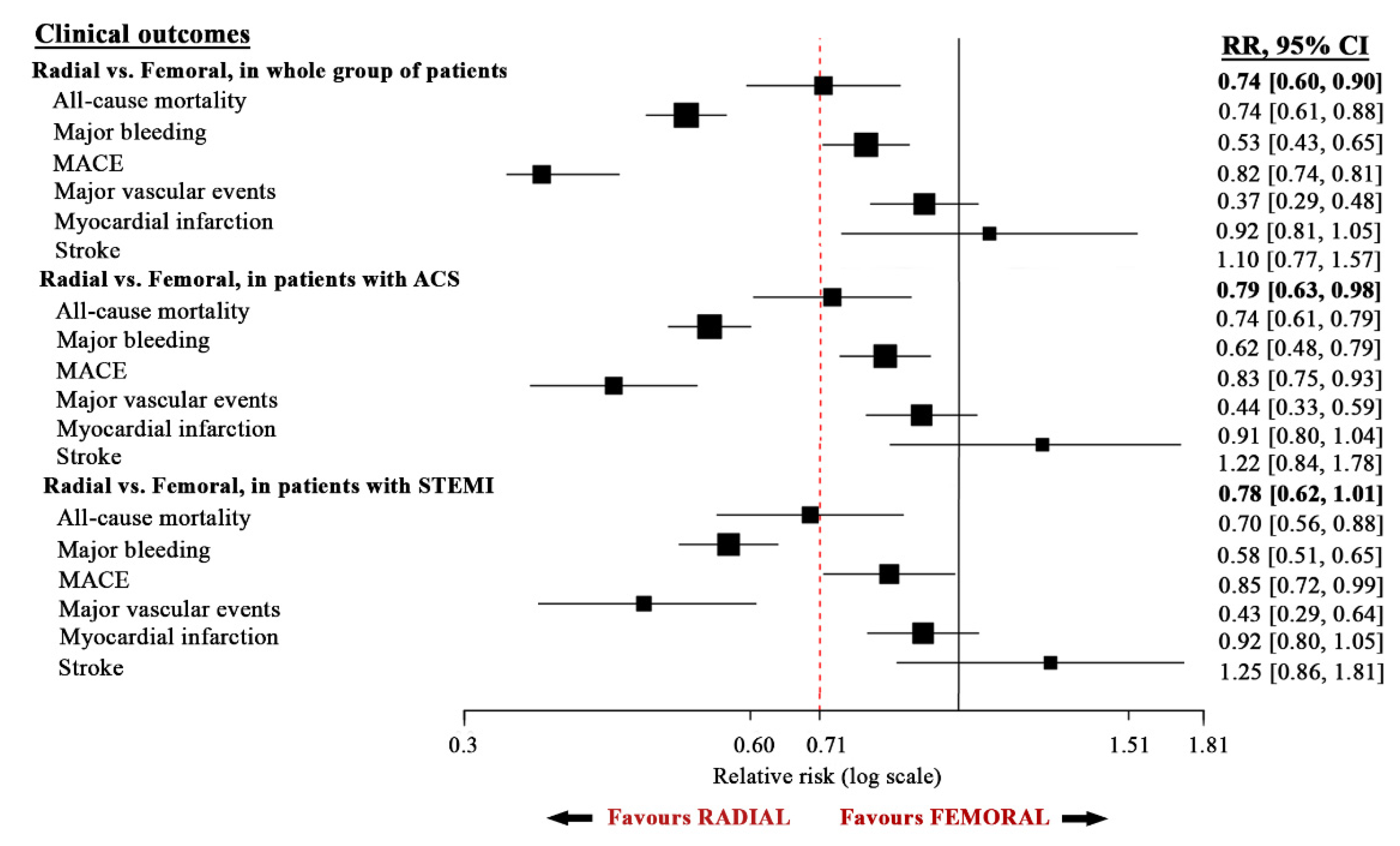
4. Outcomes of Patients in the Whole Group
4.1. Primary Clinical Outcomes
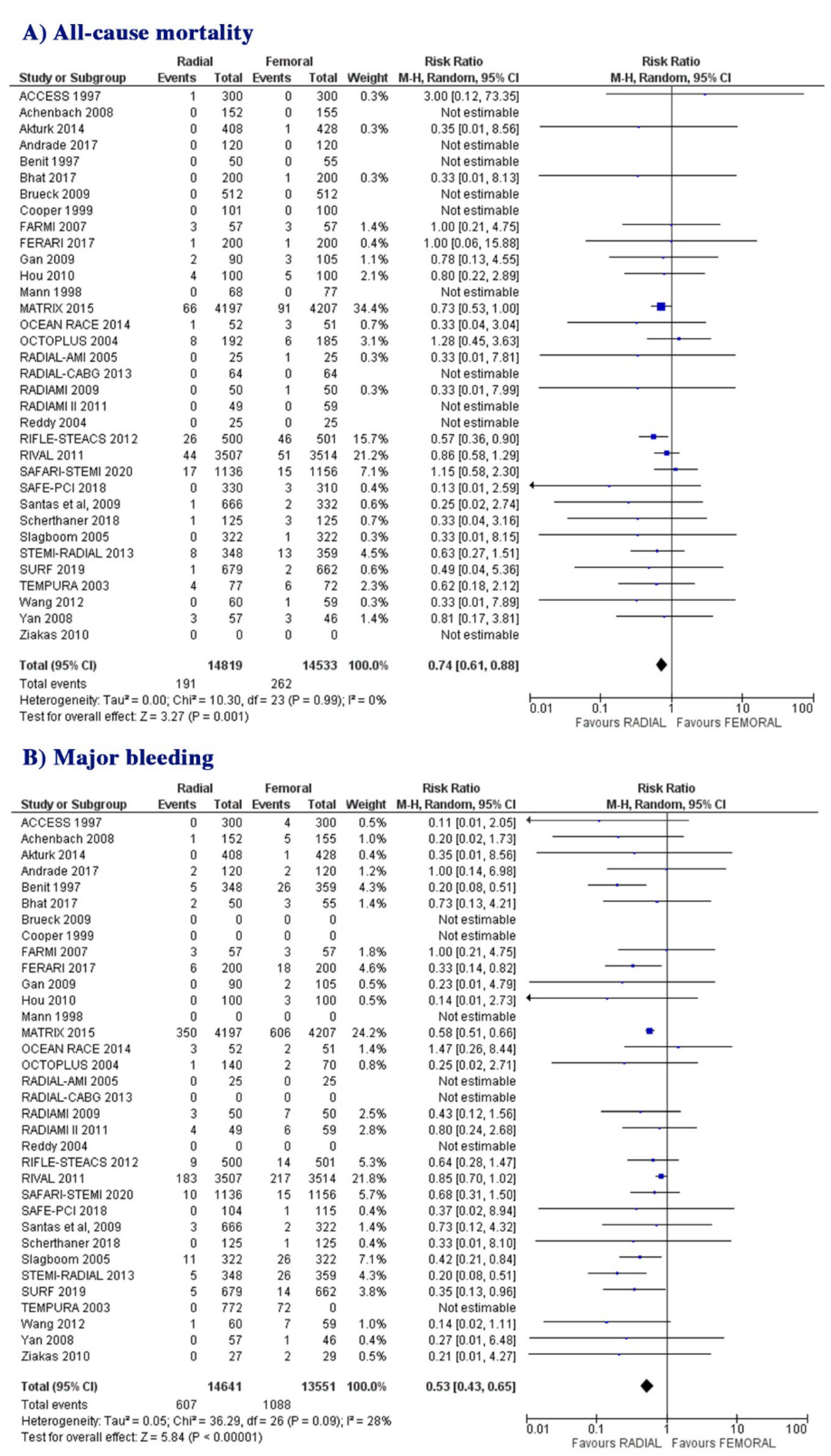
4.1.1. All-Cause Mortality
4.1.2. Major Bleeding
4.2. Secondary Clinical Outcomes
4.2.1. MACE
4.2.2. Major Vascular Complications
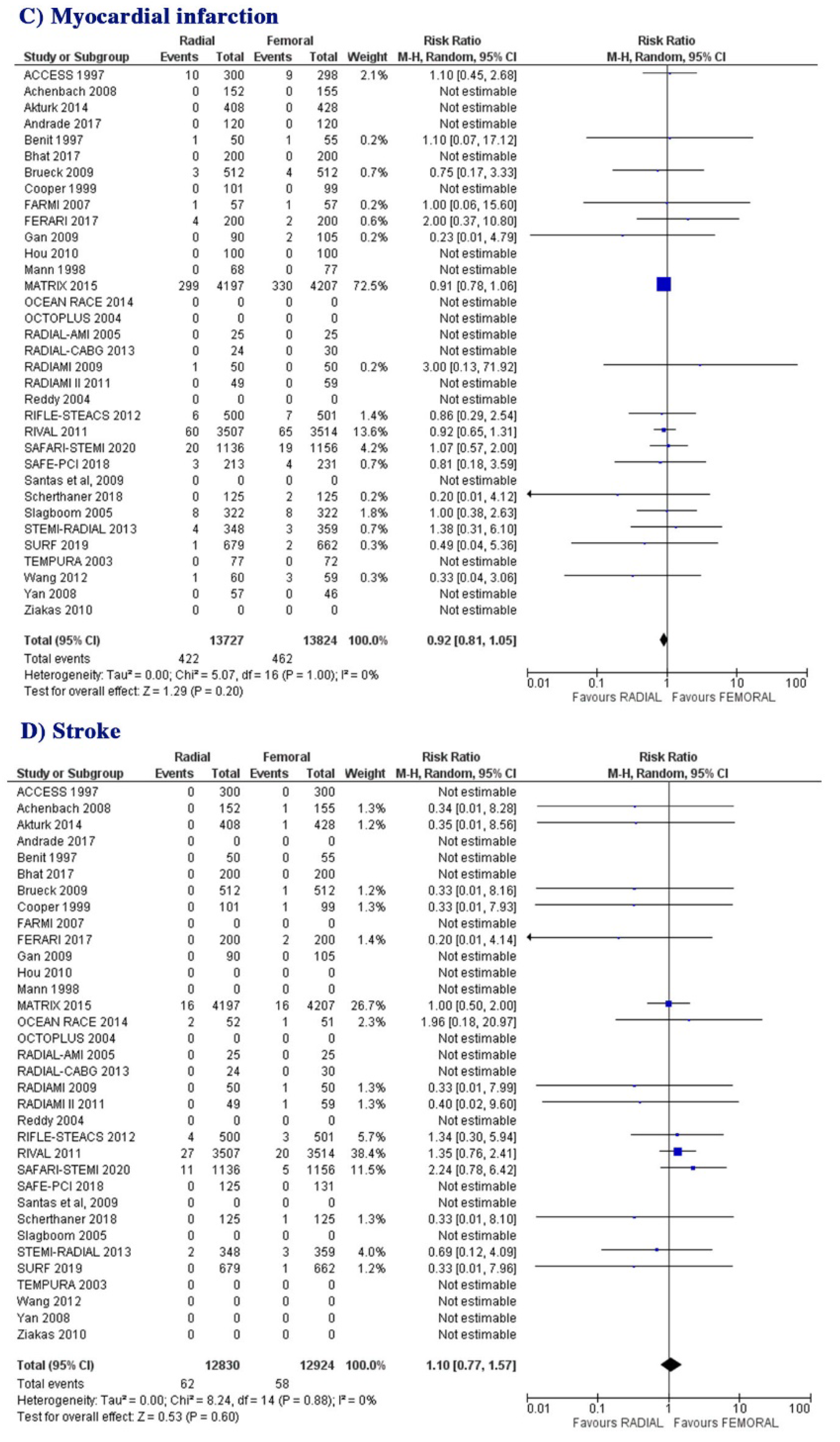
4.2.3. Myocardial Infarction
4.2.4. Stroke
5. Results
5.1. Outcomes of Patients with Acute Coronary Syndrome (ACS)
5.1.1. Primary Clinical Outcomes
All-Cause Mortality
Major Bleeding
5.1.2. Secondary Clinical Outcomes
MACE
Major Vascular Complications
Myocardial Infarction
Stroke
5.2. Outcomes of Patients with STEMI
5.2.1. Primary Clinical Outcomes
All-Cause Mortality
Major Bleeding
5.2.2. Secondary Clinical Outcomes
MACE
Major Vascular Complications
Myocardial Infarction
Stroke
5.2.3. Risk of Bias Assessment
6. Discussion
6.1. Findings
6.2. Data Interpretation
6.3. Clinical Implications
6.4. Limitations
6.5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Russ. J. Cardiol. 2019, 40, 87–165. [Google Scholar] [CrossRef] [Green Version]
- Habib, R.H.; Dimitrova, K.R.; Badour, S.A.; Yammine, M.B.; El-Hage-Sleiman, A.K.M.; Hoffman, D.M.; Geller, C.M.; Schwann, T.A.; Tranbaugh, R.F. CABG Versus PCI: Greater Benefit in Long-Term Outcomes with Multiple Arterial Bypass Grafting. J. Am. Coll. Cardiol. 2015, 66, 1417–1427. [Google Scholar] [CrossRef]
- Venkitachalam, L.; Kip, K.E.; Selzer, F.; Wilensky, R.L.; Slater, J.; Mulukutla, S.R.; Marroquin, O.C.; Block, P.C.; Williams, D.O.; Kelsey, S.F. Twenty-year evolution of percutaneous coronary intervention and its impact on clinical outcomes: A report from the National Heart, Lung, and Blood Institute-sponsored, multicenter 1985–1986 PTCA and 1997–2006 dynamic registries. Circ. Cardiovasc. Interv. 2009, 2, 6–13. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.V.; O’Grady, K.; Pieper, K.S.; Granger, C.B.; Newby, L.K.; Van de Werf, F.; Mahaffey, K.W.; Califf, R.M.; Harrington, R.A. Impact of Bleeding Severity on Clinical Outcomes Among Patients With Acute Coronary Syndromes. Am. J. Cardiol. 2005, 96, 1200–1206. [Google Scholar] [CrossRef]
- Chhatriwalla, A.K.; Amin, A.P.; Kennedy, K.F.; House, J.A.; Cohen, D.J.; Rao, S.V.; Messenger, J.C.; Marso, S.P.; Registry, F.T.N.C.D. Association Between Bleeding Events and In-hospital Mortality After Percutaneous Coronary Intervention. JAMA 2013, 309, 1022–1029. [Google Scholar] [CrossRef] [Green Version]
- Campeau, L. Percutaneous radial artery approach for coronary angiography. Catheter. Cardiovasc. Diagn. 1989, 16, 3–7. [Google Scholar] [CrossRef]
- Hildick-Smith, D.J.; Lowe, M.D.; Walsh, J.T.; Ludman, P.F.; Stephens, N.G.; Schofield, P.M.; Stone, D.L.; Shapiro, L.M.; Petch, M.C. Coronary angiography from the radial artery—Experience, complications and limitations. Int. J. Cardiol. 1998, 64, 231–239. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; for the PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Bovill, E.G.; Terrin, M.L.; Stump, D.C.; Berke, A.D.; Frederick, M.; Collen, D.; Feit, F.; Gore, J.M.; Hillis, L.D.; Lambrew, C.T.; et al. Hemorrhagicevents during therapy with recombinant tissue-type plasminogen activator, heparin, and aspirin for acute myocardial infarction. Results of the Thrombolysis in Myocardial Infarction (TIMI), phase II trial. Ann. Intern. Med. 1991, 115, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [Green Version]
- Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Cooper, H.M.; Hedges, L.V. The Handbook of Research Synthesis; Russell Sage Foundation: New York, NY, USA, 1994. [Google Scholar]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiemeneij, F.; Laarman, G.J.; Odekerken, D.; Slagboom, T.; van der Wieken, R. A Randomized Comparison of Percutaneous Transluminal Coronary Angioplasty by the Radial, Brachial and Femoral Approaches: The Access Study. J. Am. Coll. Cardiol. 1997, 29, 1269–1275. [Google Scholar] [CrossRef]
- Benit, E.; Missault, L.; Eeman, T.; Carlier, M.; Muyldermans, L.; Materne, P.; Lafontaine, P.; De Keyser, J.; DeCoster, O.; Pourbaix, S.; et al. Brachial, radial, or femoral approach for elective Palmaz-Schatz stent implantation: A randomized comparison. Catheter. Cardiovasc. Diagn. 1997, 41, 124–130. [Google Scholar] [CrossRef]
- Mann, T.; Cubeddu, G.; Bowen, J.; Schneider, J.E.; Arrowood, M.; Newman, W.N.; Zellinger, M.J.; Rose, G.C. Stenting in acute coronary syndromes: A comparison of radial versus femoral access sites. J. Am. Coll. Cardiol. 1998, 32, 572–576. [Google Scholar] [CrossRef] [Green Version]
- Cooper, C.J.; El-Shiekh, R.A.; Cohen, D.J.; Blaesing, L.; Burket, M.W.; Basu, A.; Moore, J.A. Effect of transradial access on quality of life and cost of cardiac catheterization: A randomized comparison. Am Heart J. 1999, 138 Pt 1, 430–436. [Google Scholar] [CrossRef]
- Saito, S.; Tanaka, S.; Hiroe, Y.; Miyashita, Y.; Takahashi, S.; Tanaka, K.; Satake, S. Comparative study on transradial approach vs. transfemoral approach in primary stent implantation for patients with acute myocardial infarction: Results of the test for myocardial infarction by prospective unicenter randomization for access sites (TEMPURA) trial. Catheter. Cardiovasc. Interv. 2003, 59, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Reddy, B.K.; Brewster, P.S.; Walsh, T.; Burket, M.W.; Thomas, W.J.; Cooper, C.J. Randomized comparison of rapid ambulation using radial, 4 French femoral access, or femoral access with AngioSeal closure. Catheter. Cardiovasc. Interv. 2004, 62, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Louvard, Y.; Benamer, H.; Garot, P.; Hildick-Smith, D.; Loubeyre, C.; Rigattieri, S.; Monchi, M.; Lefèvre, T.; Hamon, M. Comparison of transradial and transfemoral approaches for coronary angiography and angioplasty in octogenarians (the OCTOPLUS study). Am. J. Cardiol. 2004, 94, 1177–1180. [Google Scholar] [CrossRef] [PubMed]
- Slagboom, T.; Kiemeneij, F.; Laarman, G.J.; Van Der Wieken, R. Outpatient coronary angioplasty: Feasible and safe. Catheter. Cardiovasc. Interv. 2005, 64, 421–427. [Google Scholar] [CrossRef]
- Cantor, W.J.; Puley, G.; Natarajan, M.K.; Dzavik, V.; Madan, M.; Fry, A.; Kim, H.H.; Velianou, J.L.; Pirani, N.; Strauss, B.H.; et al. Radial versus femoral access for emergent percutaneous coronary intervention with adjunct glycoprotein IIb/IIIa inhibition in acute myocardial infarction—the RADIAL-AMI pilot randomized trial. Am. Heart J. 2005, 150, 543–549. [Google Scholar] [CrossRef]
- Brasselet, C.; Tassan, S.; Nazeyrollas, P.; Hamon, M.; Metz, D. Randomised comparison of femoral versus radial approach for percutaneous coronary intervention using abciximab in acute myocardial infarction: Results of the FARMI Trial. Heart 2006, 93, 1556–1561. [Google Scholar] [CrossRef] [Green Version]
- Yan, Z.-X.; Zhou, Y.-J.; Zhao, Y.-X.; Liu, Y.-Y.; Shi, D.-M.; Guo, Y.-H.; Cheng, W.-J. Safety and feasibility of transradial approach for primary percutaneous coronary intervention in elderly patients with acute myocardial infarction. Chin. Med. J. 2008, 121, 782–786. [Google Scholar] [CrossRef]
- Achenbach, S.; Ropers, D.; Kallert, L.; Turan, N.; Krähner, R.; Wolf, T.; Garlichs, C.; Flachskampf, F.; Daniel, W.G.; Ludwig, J. Transradial versus transfemoral approach for coronary angiography and intervention in patients above 75 years of age. Catheter. Cardiovasc. Interv. 2008, 72, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Santas, E.; Bodí, V.; Sanchis, J.; Núñez, J.; Mainar, L.; Miñana, G.; Chorro, F.J.; Llácer, A. The left radial approach in daily practice. A randomized study comparing femoral and right and left radial approaches. Rev. Española Cardiol. 2009, 62, 482–490. [Google Scholar] [CrossRef]
- Brueck, M.; Bandorski, D.; Kramer, W.; Wieczorek, M.; Höltgen, R.; Tillmanns, H. A Randomized Comparison of Transradial Versus Transfemoral Approach for Coronary Angiography and Angioplasty. JACC Cardiovasc. Interv. 2009, 2, 1047–1054. [Google Scholar] [CrossRef] [Green Version]
- Gan, L.; Li, Q.; Liu, R.; Zhao, Y.; Qiu, J.; Liao, Y. Effectiveness and feasibility of transradial approaches for primary percutaneous coronary intervention in patients with acute myocardial infarction. J. Nanjing Med Univ. 2009, 23, 270–274. [Google Scholar] [CrossRef]
- Chodór, P.; Krupa, H.; Kurek, T.; Sokal, A.; Swierad, M.; Was, T.; Streb, W.; Duszańska, A.; Swiatkowski, A.; Honisz, G.; et al. RADIal versus femoral approach for percutaneous coronary interventions in patients with Acute Myocardial Infarction (RADIAMI): A prospective, randomized, single-center clinical trial. Cardiol. J. 2009, 16, 332–340. [Google Scholar] [PubMed]
- Hou, L.; Wei, Y.-D.; Li, W.-M.; Xu, Y.-W. Comparative study on transradial versus transfemoral approach for primary percutaneous coronary intervention in Chinese patients with acute myocardial infarction. Saudi Med. J. 2010, 31, 158–162. [Google Scholar] [PubMed]
- Ziakas, A.G.; Koskinas, K.C.; Gavrilidis, S.; Giannoglou, G.D.; Hadjimiltiades, S.; Gourassas, I.; Theofilogiannakos, E.; Economou, F.; Styliadis, I. Radial versus femoral access for orally anticoagulated patients. Catheter. Cardiovasc. Interv. 2010, 76, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Jolly, S.S.; Yusuf, S.; Cairns, J.; Niemelä, K.; Xavier, D.; Widimsky, P.; Budaj, A.; Niemelä, M.; Valentin, V.; Lewis, B.S.; et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): A randomised, parallel group, multicentre trial. Lancet 2011, 377, 1409–1420. [Google Scholar] [CrossRef]
- Chodór, P.; Kurek, T.; Kowalczuk, A.; Świerad, M.; Wąs, T.; Honisz, G.; Świątkowski, A.; Streb, W.; Kalarus, Z. Radial vs femoral approach with StarClose clip placement for primary percutaneous coronary intervention in patients with ST-elevation myocardial infarction. RADIAMI II: A prospective, randomised, single centre trial. Kardiol. Pol. 2011, 69, 763–771. [Google Scholar] [PubMed]
- Romagnoli, E.; Biondi-Zoccai, G.; Sciahbasi, A.; Politi, L.; Rigattieri, S.; Pendenza, G.; Summaria, F.; Patrizi, R.; Borghi, A.; Di Russo, C.; et al. Radial versus femoral randomized investigation in ST-segment elevation acute coronary syndrome: The RIFLE-STEACS (Radial Versus Femoral Randomized Investigation in ST-Elevation Acute Coronary Syndrome) study. J. Am. Coll Cardiol. 2012, 60, 2481–2489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.-B.; Fu, X.-H.; Wang, X.-C.; Gu, X.-S.; Zhao, Y.-J.; Hao, G.-Z.; Jiang, Y.-F.; Li, S.-Q.; Wu, W.-L.; Fan, W.-Z. Randomized comparison of radial versus femoral approach for patients with STEMI undergoing early PCI following intravenous thrombolysis. J. Invasive Cardiol. 2012, 24, 412–416. [Google Scholar] [PubMed]
- Michael, T.T.; Alomar, M.; Papayannis, A.; Mogabgab, O.; Patel, V.G.; Rangan, B.V.; Luna, M.; Hastings, J.L.; Grodin, J.; Abdullah, S.; et al. A randomized comparison of the transradial and transfemoral approaches for coronary artery bypass graft angiography and intervention: The RADIAL-CABG Trial (RADIAL Versus Femoral Access for Coronary Artery Bypass Graft Angiography and Intervention). JACC Cardiovasc. Interv. 2013, 6, 1138–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kołtowski, Ł.; Filipiak, K.J.; Kochman, J.; Pietrasik, A.; Rdzanek, A.; Huczek, Z.; Ścibisz, A.; Mazurek, T.; Opolski, G. Access for percutaneous coronary intervention in ST segment elevation myocardial infarction: Radial vs. femoral—A prospective, randomised clinical trial (OCEAN RACE). Kardiol. Pol. 2014, 72, 604–611. [Google Scholar] [CrossRef]
- Aktürk, E.; Kurtoğlu, E.; Ermiş, N.; Açıkgöz, N.; Yağmur, J.; Altuntaş, M.S.; Pekdemir, H.; Özdemir, R. Comparision of pain levels of transradial versus transfemoral coronary catheterization: A prospective and randomized study. Anadolu Kardiyol. Derg. 2014, 14, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Bernat, I.; Horak, D.; Stasek, J.; Mates, M.; Pesek, J.; Ostadal, P.; Hrabos, V.; Dusek, J.; Koza, J.; Sembera, Z.; et al. ST-segment elevation myocardial infarction treated by radial or femoral approach in a multicenter randomized clinical trial: The STEMI-RADIAL trial. J. Am. Coll Cardiol. 2014, 63, 964–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valgimigli, M.; Gagnor, A.; Calabró, P.; Frigoli, E.; Leonardi, S.; Zaro, T.; Rubartelli, P.; Briguori, C.; Andò, G.; Repetto, A.; et al. Radial versus femoral access in patients with acute coronary syndromes undergoing invasive management: A randomisedmulticentre trial. Lancet 2015, 385, 2465–2476. [Google Scholar] [CrossRef]
- Fastner, C.; Behnes, M.; Ünsal, M.; El-Battrawy, I.; Ansari, U.; Mashayekhi, K.; Hoffmann, U.; Lang, S.; Kuschyk, J.; Borggrefe, M.; et al. Clinical outcomes of femoral closure compared to radial compression devices following percutaneous coronary intervention: The FERARI study. Heart Vessel. 2016, 32, 520–530. [Google Scholar] [CrossRef]
- Andrade, P.B.; Mattos, L.A.; Rinaldi, F.S.; Bienert, I.C.; Barbosa, R.A.; Labrunie, A.; Tebet, M.; Esteves, V.; Abizaid, A.; Sousa, A.R. Comparison of a vascular closure device versus the radial approach to reduce access site complications in non-ST-segment elevation acute coronary syndrome patients: The angio-seal versus the radial approach in acute coronary syndrome trial. Catheter. Cardiovasc. Interv. 2016, 89, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Bhat, F.A.; Changal, K.H.; Raina, H.; Tramboo, N.A.; Rather, H.A. Transradial versus transfemoral approach for coronary angiography and angioplasty—A prospective, randomized comparison. BMC Cardiovasc. Disord. 2017, 17, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schernthaner, C.; Hammerer, M.; Harb, S.; Heigert, M.; Hoellinger, K.; Lassnig, E.; Maurer, E.; Schuler, J.; Siostrzonek, P.; Ulmer, H.; et al. Radial versus femoral access site for percutaneous coronary intervention in patients suffering acute myocardial infarction. Wien. Klin. Wochenschr. 2017, 130, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Koshy, L.M.; Aberle, L.H.; Krucoff, M.W.; Hess, C.N.; Mazzaferri, E., Jr.; Jolly, S.S.; Jacobs, A.; Gibson, C.M.; Mehran, R.; Gilchrist, I.C.; et al. Comparison of Radial Access, Guided Femoral Access, and Non-Guided Femoral Access Among Women Undergoing Percutaneous Coronary Intervention. J. Invasive Cardiol. 2018, 30, 18–22. [Google Scholar]
- Nguyen, P.; Makris, A.; Hennessy, A.; Jayanti, S.; Wang, A.; Park, K.; Chen, V.; Nguyen, T.; Lo, S.; Xuan, W.; et al. Standard versus ultrasound-guided radial and femoral access in coronary angiography and intervention (SURF): A randomised controlled trial. EuroIntervention 2019, 15, e522–e530. [Google Scholar] [CrossRef]
- May, M.L.; Wells, G.; So, D.; Chong, A.Y.; Dick, A.; Froeschl, M.; Glover, C.; Hibbert, B.; Marquis, J.F.; Blondeau, M.; et al. Safety and Efficacy of Femoral Access vs Radial Access in ST-Segment Elevation Myocardial Infarction: The SAFARI-STEMI Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Wensley, C.J.; Kent, B.; McAleer, M.B.; Savage, S.M.; Stewart, J.T. Pain relief for the removal of femoral sheath after percutaneous coronary intervention. Cochrane Database Syst. Rev. 2008, 2008, CD006043. [Google Scholar] [CrossRef]
- Kolkailah, A.A.; Alreshq, R.S.; Muhammed, A.M.; Zahran, M.E.; El-Wegoud, M.A.; Nabhan, A.F. Transradial versus transfemoral approach for diagnostic coronary angiography and percutaneous coronary intervention in people with coronary artery disease. Cochrane Database Syst. Rev. 2018, 2018, CD012318. [Google Scholar] [CrossRef]
- Tavakol, M.; Ashraf, S.; Brener, S.J. Risks and Complications of Coronary Angiography: A Comprehensive Review. Glob. J. Health Sci. 2012, 4, 65–93. [Google Scholar] [CrossRef]
- Dal Molin, A.; Faggiano, F.; Bertoncini, F.; Buratti, G.; Busca, E.; Casarotto, R.; Gaboardi, S.; Allara, E. Bed rest for preventing complications after transfemoral cardiac catheterisation: A protocol of systematic review and network meta-analysis. Syst. Rev. 2015, 4, 47. [Google Scholar] [CrossRef] [Green Version]
- Kasapis, C.; Gurm, H.S. Current Approach to the Diagnosis and Treatment of Femoral-Popliteal Arterial Disease. A Systematic Review. Curr. Cardiol. Rev. 2009, 5, 296–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.-Y.; Yoon, J. Transradial Approach as a Default Route in Coronary Artery Interventions. Korean Circ. J. 2011, 41, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Brasselet, C.; Blanpain, T.; Tassan-Mangina, S.; Deschildre, A.; Duval, S.; Vitry, F.; Gaillot-Petit, N.; Clément, J.P.; Metz, D. Comparison of operator radiation exposure with optimized radiation protection devices during coronary angiograms and ad hoc percutaneous coronary interventions by radial and femoral routes. Eur. Heart J. 2007, 29, 63–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hess, C.N.; Peterson, E.D.; Neely, M.L.; Dai, D.; Hillegass, W.B.; Krucoff, M.W.; Kutcher, M.A.; Messenger, J.C.; Pancholy, S.; Piana, R.N.; et al. The Learning Curve for Transradial Percutaneous Coronary Intervention among Operators in the United States. Circulation 2014, 129, 2277–2286. [Google Scholar] [CrossRef] [Green Version]
- Hamon, M.; Pristipino, C.; Di Mario, C.; Nolan, J.; Ludwig, J.; Tubaro, M.; Sabaté, M.; Mauri-Ferré, J.; Huber, K.; Niemelä, K.; et al. Consensus document on the radial approach in percutaneous cardiovascular interventions: Position paper by the European Association of Percutaneous Cardiovascular Interventions and Working Groups on Acute Cardiac Care and Thrombosis of the European Society of Cardiology. EuroIntervention 2013, 8, 1242–1251. [Google Scholar] [CrossRef] [Green Version]
- Valgimigli, M.; Frigoli, E.; Leonardi, S.; Vranckx, P.; Rothenbühler, M.; Tebaldi, M.; Varbella, F.; Calabrò, P.; Garducci, S.; Rubartelli, P.; et al. Radial versus femoral access and bivalirudin versus unfractionated heparin in invasively managed patients with acute coronary syndrome (MATRIX): Final 1-year results of a multicentre, randomised controlled trial. Lancet 2018, 392, 835–848. [Google Scholar] [CrossRef]
- Cayla, G.; Silvain, J.; Barthelemy, O.; Connor, S.O.; Payot, L.; Bellemain-Appaix, A.; Beygui, F.; Aout, M.; Collet, J.-P.; Vicaut, E.; et al. Trans-radial approach for catheterisation in non-ST segment elevation acute coronary syndrome: An analysis of major bleeding complications in the ABOARD Study. Heart 2011, 97, 887–891. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, G.; Valgimigli, M.; Sunnåker, M.; Vranckx, P.; Frigoli, E.; Leonardi, S.; Spirito, A.; Gragnano, F.; Manavifar, N.; Galea, R.; et al. Choice of access site and type of anticoagulant in acute coronary syndromes with advanced Killip class or out-of-hospital cardiac arrest. Rev. Española Cardiol. 2020, 73, 893–901. [Google Scholar] [CrossRef]
- Alexopoulos, D.; Xanthopoulou, I.; Deftereos, S.; Sitafidis, G.; Kanakakis, I.; Hamilos, M.; Karayannis, G.; Angelidis, C.; Stavrou, K.; Vavuranakis, M.; et al. Bivalirudin Use and One-Month Outcome in the Context of Contemporary Antiplatelet Treatment: Insights from the Greek Antiplatelet Registry. Cardiovasc. Ther. 2014, 32, 120–126. [Google Scholar] [CrossRef] [Green Version]
- Vora, A.N.; Peterson, E.D.; McCoy, L.A.; Garratt, K.N.; Kutcher, M.A.; Marso, S.P.; Roe, M.T.; Messenger, J.C.; Rao, S.V. The Impact of Bleeding Avoidance Strategies on Hospital-Level Variation in Bleeding Rates Following Percutaneous Coronary Intervention: Insights from the National Cardiovascular Data Registry CathPCI Registry. JACC Cardiovasc. Interv. 2016, 9, 771–779. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bajraktari, G.; Rexhaj, Z.; Elezi, S.; Zhubi-Bakija, F.; Bajraktari, A.; Bytyçi, I.; Batalli, A.; Henein, M.Y. Radial Access for Coronary Angiography Carries Fewer Complications Compared with Femoral Access: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 2163. https://doi.org/10.3390/jcm10102163
Bajraktari G, Rexhaj Z, Elezi S, Zhubi-Bakija F, Bajraktari A, Bytyçi I, Batalli A, Henein MY. Radial Access for Coronary Angiography Carries Fewer Complications Compared with Femoral Access: A Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2021; 10(10):2163. https://doi.org/10.3390/jcm10102163
Chicago/Turabian StyleBajraktari, Gani, Zarife Rexhaj, Shpend Elezi, Fjolla Zhubi-Bakija, Artan Bajraktari, Ibadete Bytyçi, Arlind Batalli, and Michael Y. Henein. 2021. "Radial Access for Coronary Angiography Carries Fewer Complications Compared with Femoral Access: A Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 10, no. 10: 2163. https://doi.org/10.3390/jcm10102163