


Discrepancies in Cephalometric Analysis Results between Orthodontists and Radiologists and Artificial Intelligence: A Systematic Review


 , , , , , ,
, , , , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Focused Question
2.2. Protocol
2.3. Eligibility Criteria
2.4. Information Sources, Search Strategy, and Study Selection
2.5. Data Collection and Data Items
2.6. Assessing Risk of Bias in Individual Studies
2.7. Quality Assessment
3. Results
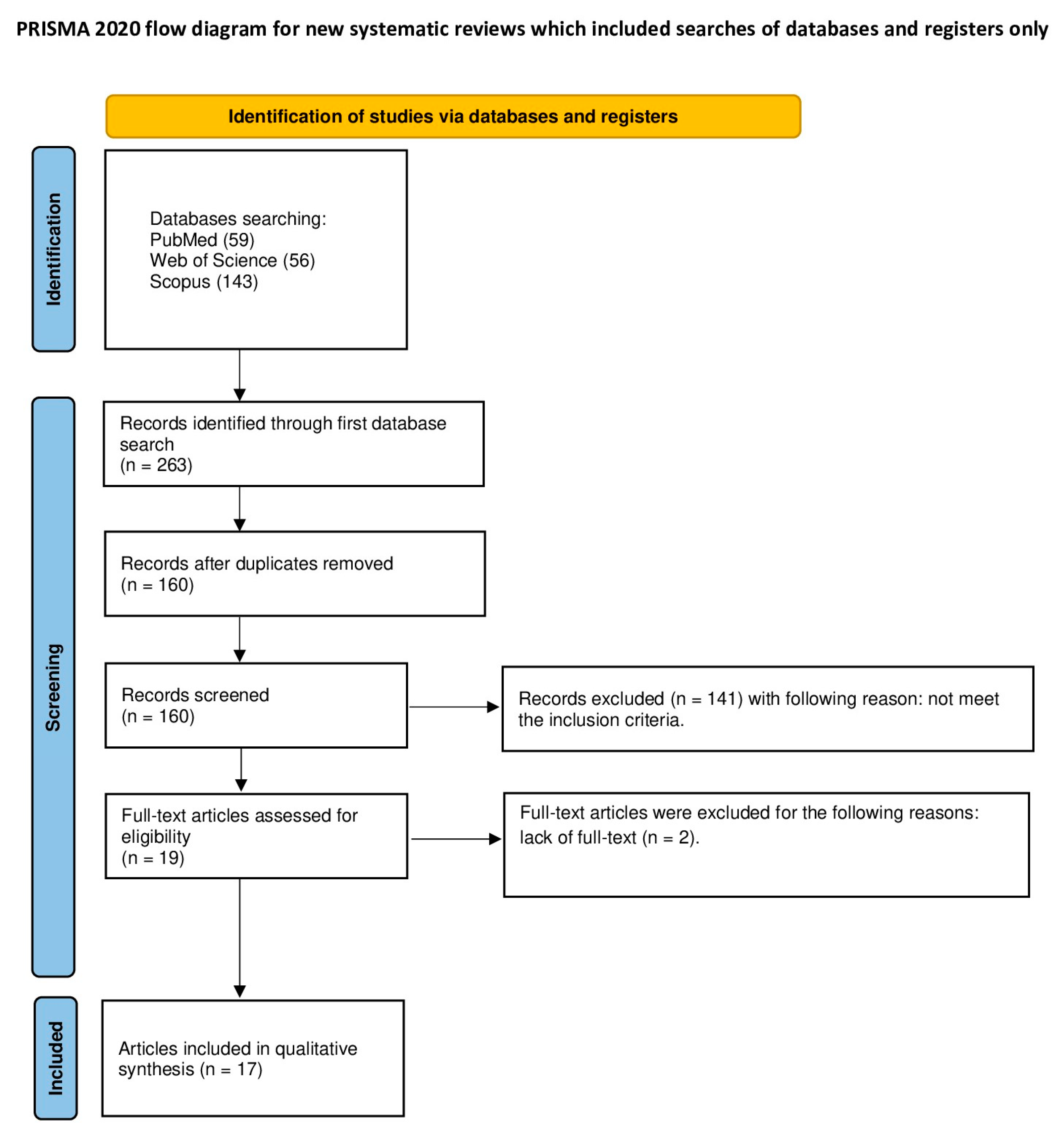
3.1. Study Selection
3.2. General Characteristics of the Included Studies
3.3. Main Study Outcomes
3.4. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Starch-Jensen, T.; Hernández-Alfaro, F.; Kesmez, Ö.; Gorgis, R.; Valls-Ontañón, A. Accuracy of Orthognathic Surgical Planning Using Three-Dimensional Virtual Techniques Compared with Conventional Two-Dimensional Techniques: A Systematic Review. J. Oral Maxillofac. Res. 2023, 14, 14101. [Google Scholar] [CrossRef] [PubMed]
- Alkhayer, A.; Piffkó, J.; Lippold, C.; Segatto, E. Accuracy of Virtual Planning in Orthognathic Surgery: A Systematic Review. Head Face Med. 2020, 16, 34. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Shanavas, M.; Sidappa, A.; Kiran, M. Cone Beam Computed Tomography—Know Its Secrets. J. Int. Oral Health 2015, 7, 64. [Google Scholar] [PubMed]
- Chien, P.C.; Parks, E.T.; Eraso, F.; Hartsfield, J.K.; Roberts, W.E.; Ofner, S. Comparison of Reliability in Anatomical Landmark Identification Using Two-Dimensional Digital Cephalometrics and Three-Dimensional Cone Beam Computed Tomography in Vivo. Dentomaxillofacial Radiol. 2014, 38, 262–273. [Google Scholar] [CrossRef] [PubMed]
- Hariharan, A.; Diwakar, N.R.; Jayanthi, K.; Hema, H.M.; Deepukrishna, S.; Ghaste, S.R. The Reliability of Cephalometric Measurements in Oral and Maxillofacial Imaging: Cone Beam Computed Tomography versus Two-Dimensional Digital Cephalograms. Indian J. Dent. Res. 2016, 27, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Teixeira, H.; Tanna, N.; Zheng, Z.; Chen, S.H.Y.; Zou, M.; Chung, C.H. The Reliability of Two- and Three-Dimensional Cephalometric Measurements: A CBCT Study. Diagnostics 2021, 11, 2292. [Google Scholar] [CrossRef] [PubMed]
- Gkantidis, N.; Opacic, J.; Kanavakis, G.; Katsaros, C.; Halazonetis, D. Facial Asymmetry and Midsagittal Plane Definition in 3D: A Bias-Free, Automated Method. PLoS ONE 2023, 18, e0294528. [Google Scholar] [CrossRef]
- Dobai, A.; Markella, Z.; Vízkelety, T.; Fouquet, C.; Rosta, A.; Barabás, J. Landmark-Based Midsagittal Plane Analysis in Patients with Facial Symmetry and Asymmetry Based on Cbct Analysis Tomography. J. Orofac. Orthop. 2018, 79, 371. [Google Scholar] [CrossRef] [PubMed]
- Damstra, J.; Fourie, Z.; De Wit, M.; Ren, Y. A Three-Dimensional Comparison of a Morphometric and Conventional Cephalometric Midsagittal Planes for Craniofacial Asymmetry. Clin. Oral Investig. 2012, 16, 285–294. [Google Scholar] [CrossRef]
- Wang, Y.; Wu, W.; Christelle, M.; Sun, M.; Wen, Z.; Lin, Y.; Zhang, H.; Xu, J. Automated Localization of Mandibular Landmarks in the Construction of Mandibular Median Sagittal Plane. Eur. J. Med. Res. 2024, 29, 84. [Google Scholar] [CrossRef]
- Lin, Y.H.; Yao, C.F.; Chen, Y.A.; Liao, Y.F.; Chen, Y.R. Three-Dimensional Positioning of the Maxilla Using Novel Intermediate Splints in Maxilla-First Orthognathic Surgery for Correction of Skeletal Class III Deformity. Clin. Oral Investig. 2024, 28, 141. [Google Scholar] [CrossRef]
- Lin, L.O.; Kalmar, C.L.; Vu, G.H.; Zimmerman, C.E.; Humphries, L.S.; Swanson, J.W.; Bartlett, S.P.; Taylor, J.A. Value-Based Analysis of Virtual Versus Traditional Surgical Planning for Orthognathic Surgery. J. Craniofacial Surg. 2020, 31, 1238–1242. [Google Scholar] [CrossRef] [PubMed]
- Antonini, F.; Borba, A.M.; Pagnoncelli, R.M.; Han, M.; Markiewicz, M.R.; Miloro, M. Does a Learning Curve Exist for Accuracy in Three-Dimensional Planning for Maxillary Positioning in Bimaxillary Orthognathic Surgery? Int. J. Oral Maxillofac. Surg. 2020, 49, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Frongia, G.; Piancino, M.G.; Bracco, A.A.; Crincoli, V.; Debernardi, C.L.; Bracco, P. Assessment of the Reliability and Repeatability of Landmarks Using 3-D Cephalometric Software. Cranio® 2012, 30, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Sam, A.; Currie, K.; Oh, H.; Flores-Mir, C.; Lagravére-Vich, M. Reliability of Different Three-Dimensional Cephalometric Landmarks in Cone-Beam Computed Tomography: A Systematic Review. Angle Orthod. 2019, 89, 317–332. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.K.; Alftaikhah, S.A.A.; Issrani, R.; Ronsivalle, V.; Lo Giudice, A.; Cicciù, M.; Minervini, G. Applications of Artificial Intelligence in the Utilisation of Imaging Modalities in Dentistry: A Systematic Review and Meta-Analysis of in-Vitro Studies. Heliyon 2024, 10, e24221. [Google Scholar] [CrossRef] [PubMed]
- Miryala, A.G.; Miryala, G.; Khan, Y.; Ramalingam, N.T.; Sevugaperumal, B.; Soman, M.; Padmanabhan, A. Revolutionizing Dental Imaging: A Comprehensive Study on the Integration of Artificial Intelligence in Dental and Maxillofacial Radiology. Cureus 2023, 15, e50292. [Google Scholar] [CrossRef] [PubMed]
- Tabatabaian, F.; Vora, S.R.; Mirabbasi, S. Applications, Functions, and Accuracy of Artificial Intelligence in Restorative Dentistry: A Literature Review. J. Esthet. Restor. Dent. 2023, 35, 842–859. [Google Scholar] [CrossRef] [PubMed]
- Akhare, P.J.; Dagab, A.M.; Alle, R.S.; Shenoyd, U.; Garla, V. Comparison of Landmark Identification and Linear and Angular Measurements in Conventional and Digital Cephalometry. Int. J. Comput. Dent. 2013, 16, 241–254. [Google Scholar]
- Giannopoulou, M.A.; Kondylidou-Sidira, A.C.; Papadopoulos, M.A.; Athanasiou, A.E. Are Orthodontic Landmarks and Variables in Digital Cephalometric Radiography Taken in Fixed and Natural Head Positions Reliable? Int. Orthod. 2020, 18, 54–68. [Google Scholar] [CrossRef]
- Wilkat, M.; Liu, S.; Schwerter, M.; Schrader, F.; Saigo, L.; Karnatz, N.; Kübler, N.R.; Rana, M. A New Approach to Virtual Occlusion in Orthognathic Surgery Planning Using Mixed Reality—A Technical Note and Review of the Literature. J. Pers. Med. 2023, 13, 1709. [Google Scholar] [CrossRef] [PubMed]
- Zammit, D.; Ettinger, R.E.; Sanati-Mehrizy, P.; Susarla, S.M. Current Trends in Orthognathic Surgery. Medicina 2023, 59, 2100. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Mo, S.; Fan, X.; You, Y.; Ye, G.; Zhou, N. A Meta-Analysis and Systematic Review Comparing the Effectiveness of Traditional and Virtual Surgical Planning for Orthognathic Surgery: Based on Randomized Clinical Trials. J. Oral Maxillofac. Surg. 2021, 79, 471.e1–471.e19. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Singla, J.; Gera, G.; Gupta, M.; Kaur, G. Reliability of Natural Head Position in Orthodontic Diagnosis: A Cephalometric Study. Contemp. Clin. Dent. 2012, 3, 180–183. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira Lisboa, C.; Masterson, D.; da Motta, A.F.J.; Motta, A.T. Reliability and Reproducibility of Three-Dimensional Cephalometric Landmarks Using CBCT: A Systematic Review. J. Appl. Oral Sci. 2015, 23, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Lin, J.; Demner-Fushman, D. Evaluation of PICO as a Knowledge Representation for Clinical Questions. AMIA Annu. Symp. Proc. 2006, 2006, 359. [Google Scholar] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Homa, K.; Zakrzewski, W.; Dobrzyński, W.; Piszko, P.J.; Piszko, A.; Matys, J.; Wiglusz, R.J.; Dobrzyński, M. Surface Functionalization of Titanium-Based Implants with a Nanohydroxyapatite Layer and Its Impact on Osteoblasts: A Systematic Review. J. Funct. Biomater. 2024, 15, 45. [Google Scholar] [CrossRef]
- Piszko, P.J.; Piszko, A.; Kiryk, J.; Lubojański, A.; Dobrzyński, W.; Wiglusz, R.J.; Matys, J.; Dobrzyński, M. The Influence of Fluoride Gels on the Physicochemical Properties of Tooth Tissues and Dental Materials—A Systematic Review. Gels 2024, 10, 98. [Google Scholar] [CrossRef]
- Murias, I.; Grzech-Leśniak, K.; Murias, A.; Walicka-Cupryś, K.; Dominiak, M.; Deeb, J.G.; Matys, J. Efficacy of Various Laser Wavelengths in the Surgical Treatment of Ankyloglossia: A Systematic Review. Life 2022, 12, 558. [Google Scholar] [CrossRef]
- Kowalski, J.; Rygas, J.; Homa, K.; Dobrzyński, W.; Wiglusz, R.J.; Matys, J.; Dobrzyński, M. Antibacterial Activity of Endodontic Gutta-Percha—A Systematic Review. Appl. Sci. 2023, 14, 388. [Google Scholar] [CrossRef]
- Struzik, N.; Wiśniewska, K.; Piszko, P.J.; Piszko, A.; Kiryk, J.; Matys, J.; Dobrzyński, M. SEM Studies Assessing the Efficacy of Laser Treatment for Primary Teeth: A Systematic Review. Appl. Sci. 2024, 14, 1107. [Google Scholar] [CrossRef]
- Matys, J.; Kensy, J.; Gedrange, T.; Zawiślak, I.; Grzech-Leśniak, K.; Dobrzyński, M. A Molecular Approach for Detecting Bacteria and Fungi in Healthcare Environment Aerosols: A Systematic Review. Int. J. Mol. Sci. 2024, 25, 4154. [Google Scholar] [CrossRef] [PubMed]
- Kensy, J.; Dobrzyński, M.; Wiench, R.; Grzech-Leśniak, K.; Matys, J. Fibroblasts Adhesion to Laser-Modified Titanium Surfaces—A Systematic Review. Materials 2021, 14, 7305. [Google Scholar] [CrossRef] [PubMed]
- Rajewska, J.; Kowalski, J.; Matys, J.; Dobrzyński, M.; Wiglusz, R.J. The Use of Lactide Polymers in Bone Tissue Regeneration in Dentistry—A Systematic Review. J. Funct. Biomater. 2023, 14, 83. [Google Scholar] [CrossRef] [PubMed]
- Rygas, J.; Matys, J.; Wawrzyńska, M.; Szymonowicz, M.; Dobrzyński, M. The Use of Graphene Oxide in Orthodontics—A Systematic Review. J. Funct. Biomater. 2023, 14, 500. [Google Scholar] [CrossRef]
- Wiench, R.; Skaba, D.; Matys, J.; Grzech-Leśniak, K. Efficacy of Toluidine Blue—Mediated Antimicrobial Photodynamic Therapy on Candida Spp. A Systematic Review. Antibiotics 2021, 10, 349. [Google Scholar] [CrossRef]
- Woźniak, A.; Matys, J.; Grzech-Leśniak, K. Effectiveness of Lasers and APDT in Elimination of Intraoral Halitosis: A Systematic Review Based on Clinical Trials. Lasers Med. Sci. 2022, 37, 3403–3411. [Google Scholar] [CrossRef]
- Chen, S.-K.; Chen, Y.-J.; Yao, C.-C.J.; Chang, H.-F. Enhanced Speed and Precision of Measurement in a Computer-Assisted Digital Cephalometric Analysis System. Angle Orthod. 2004, 74, 501–507. [Google Scholar]
- Kuyl, M.H.; Verbeeck, R.M.H.; Dermaut, L.R. The Integumental Profile: A Reflection of the Underlying Skeletal Configuration? Am. J. Orthod. Dentofac. Orthop. 1994, 106, 597–604. [Google Scholar] [CrossRef]
- Chen, Y.-J.; Chen, S.-K.; Yao, C.-C.J.; Chang, H.-F. The Effects of Differences in Landmark Identification on the Cephalometric Measurements in Traditional Versus Digitized Cephalometry. Angle Orthod. 2004, 74, 155–161. [Google Scholar] [PubMed]
- Baker, S.B.; Goldstein, J.A.; Seruya, M. Outcomes in Computer-Assisted Surgical Simulation for Orthognathic Surgery. J. Craniofacial Surg. 2012, 23, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Mario, M.C.; Abe, J.M.; Ortega, N.R.S.; Del Santo, M. Paraconsistent Artificial Neural Network as Auxiliary in Cephalometric Diagnosis. Artif. Organs 2010, 34, E215–E221. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Davies, T.I. A Comparison of Cephalometric Measurements: A Picture Archiving and Communication System versus the Hand-Tracing Method-a Preliminary Study. Eur. J. Orthod. 2011, 33, 350–353. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.J.; Weerakone, S. An Evaluation of the Reproducibility of Landmark Identification Using Scanned Cephalometric Images. J. Orthod. 2001, 28, 221–230. [Google Scholar] [CrossRef]
- Mosleh, M.A.A.; Baba, M.S.; Malek, S.; Almaktari, R.A. Ceph-X: Development and Evaluation of 2D Cephalometric System. BMC Bioinform. 2016, 17, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Swennen, G.R.J.; Grimaldi, H.; Berten, J.-L.; Kramer, F.-J.; Dempf, R.; Schwestka-Polly, R.; Hausamen, J.-E. Reliability and Validity of a Modified Lateral Cephalometric Analysis for Evaluation of Craniofacial Morphology and Growth in Patients with Clefts. J. Craniofacial Surg. 2004, 15, 399–412. [Google Scholar] [CrossRef] [PubMed]
- Kılınç, D.D.; Kırcelli, B.H.; Sadry, S.; Karaman, A. Evaluation and Comparison of Smartphone Application Tracing, Web Based Artificial Intelligence Tracing and Conventional Hand Tracing Methods. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e906–e915. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Kumari, S.; Chandna, A.; Konark; Singh, A.; Kumar, H.; Punita. Comparative Evaluation of CephNinja for Android and NemoCeph for Computer for Cephalometric Analysis: A Study to Evaluate the Diagnostic Performance of CephNinja for Cephalometric Analysis. J. Int. Soc. Prev. Community Dent. 2020, 10, 286–291. [Google Scholar] [CrossRef]
- Tsorovas, G.; Linder-Aronson Karsten, A. A Comparison of Hand-Tracing and Cephalometric Analysis Computer Programs with and without Advanced Features—Accuracy and Time Demands. Eur. J. Orthod. 2010, 32, 721–728. [Google Scholar] [CrossRef]
- Bruntz, L.Q.; Palomo, J.M.; Baden, S.; Hans, M.G. A Comparison of Scanned Lateral Cephalograms with Corresponding Original Radiographs. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 340–348. [Google Scholar] [CrossRef]
- Zamrik, O.M.; Iseri, H. The Reliability and Reproducibility of an Android Cephalometric Smartphone Application in Comparison with the Conventional Method. Angle Orthod. 2021, 91, 236–242. [Google Scholar] [CrossRef]
- Dot, G.; Schouman, T.; Chang, S.; Rafflenbeul, F.; Kerbrat, A.; Rouch, P.; Gajny, L. Automatic Three-Dimensional Cephalometric Landmarking via Deep Learning. J. Dent. Res. 2022, 101, 1380–1387. [Google Scholar] [CrossRef]
- Wang, C.W.; Huang, C.T.; Hsieh, M.C.; Li, C.H.; Chang, S.W.; Li, W.C.; Vandaele, R.; Marée, R.; Jodogne, S.; Geurts, P.; et al. Evaluation and Comparison of Anatomical Landmark Detection Methods for Cephalometric X-ray Images: A Grand Challenge. IEEE Trans. Med. Imaging 2015, 34, 1890–1900. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Kharbanda, O.P.; Sardana, V.; Balachandran, R.; Sardana, H.K. Accuracy of 3D Cephalometric Measurements Based on an Automatic Knowledge-Based Landmark Detection Algorithm. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 1297–1309. [Google Scholar] [CrossRef]
- Mörch, C.M.; Atsu, S.; Cai, W.; Li, X.; Madathil, S.A.; Liu, X.; Mai, V.; Tamimi, F.; Dilhac, M.A.; Ducret, M. Artificial Intelligence and Ethics in Dentistry: A Scoping Review. J. Dent. Res. 2021, 100, 1452–1460. [Google Scholar] [CrossRef]
- Revilla-León, M.; Gómez-Polo, M.; Vyas, S.; Barmak, A.B.; Özcan, M.; Att, W.; Krishnamurthy, V.R. Artificial Intelligence Applications in Restorative Dentistry: A Systematic Review. J. Prosthet. Dent. 2022, 128, 867–875. [Google Scholar] [CrossRef]
- Shetty, S.; Gali, S.; Augustine, D.; Sowmya, S.V. Artificial Intelligence Systems in Dental Shade-Matching: A Systematic Review. J. Prosthodont. 2023, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Gómez-Polo, M.; Vyas, S.; Barmak, A.B.; Gallucci, G.O.; Att, W.; Özcan, M.; Krishnamurthy, V.R. Artificial Intelligence Models for Tooth-Supported Fixed and Removable Prosthodontics: A Systematic Review. J. Prosthet. Dent. 2023, 129, 276–292. [Google Scholar] [CrossRef]
- Ahmed, N.; Abbasi, M.S.; Zuberi, F.; Qamar, W.; Halim, M.S.B.; Maqsood, A.; Alam, M.K. Artificial Intelligence Techniques: Analysis, Application, and Outcome in Dentistry—A Systematic Review. Biomed. Res. Int. 2021, 2021, 9751564. [Google Scholar] [CrossRef]
- Prasad, S.; Arunachalam, S.; Boillat, T.; Ghoneima, A.; Gandedkar, N.; Diar-Bakirly, S. Wearable Orofacial Technology and Orthodontics. Dent. J. 2023, 11, 24. [Google Scholar] [CrossRef] [PubMed]
- Perrotti, G.; Baccaglione, G.; Clauser, T.; Testarelli, L.; Fabbro, M.D.; Testori, T. Total Face Approach (TFA): A Novel 3D Approach to Describe the Main Cephalometric Craniomaxillofacial Parameters. Methods Protoc. 2021, 4, 15. [Google Scholar] [CrossRef] [PubMed]
- Gateno, J.; Xia, J.J.; Teichgraeber, J.F. New 3-Dimensional Cephalometric Analysis for Orthognathic Surgery. J. Oral Maxillofac. Surg. 2011, 69, 606–622. [Google Scholar] [CrossRef] [PubMed]
- Thawri, S.R.; Paul, P.; Reche, A.; Rathi, H.P. 3D Technology Used for Precision in Orthodontics. Cureus 2023, 15, e47170. [Google Scholar] [CrossRef] [PubMed]
- Castillo, J.C.; Gianneschi, G.; Azer, D.; Manosudprasit, A.; Haghi, A.; Bansal, N.; Allareddy, V.; Masoud, M.I. The Relationship between 3D Dentofacial Photogrammetry Measurements and Traditional Cephalometric Measurements. Angle Orthod. 2019, 89, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Serafin, M.; Baldini, B.; Cabitza, F.; Carrafiello, G.; Baselli, G.; Del Fabbro, M.; Sforza, C.; Caprioglio, A.; Tartaglia, G.M. Accuracy of Automated 3D Cephalometric Landmarks by Deep Learning Algorithms: Systematic Review and Meta-Analysis. Radiol. Medica 2023, 128, 544–555. [Google Scholar] [CrossRef]
- Winkler-Schwartz, A.; Bissonnette, V.; Mirchi, N.; Ponnudurai, N.; Yilmaz, R.; Ledwos, N.; Siyar, S.; Azarnoush, H.; Karlik, B.; Del Maestro, R.F. Artificial Intelligence in Medical Education: Best Practices Using Machine Learning to Assess Surgical Expertise in Virtual Reality Simulation. J. Surg. Educ. 2019, 76, 1681–1690. [Google Scholar] [CrossRef] [PubMed]
- Malkoc, S.; Sari, Z.; Usumez, S.; Koyuturk, A.E. The Effect of Head Rotation on Cephalometric Radiographs. Eur. J. Orthod. 2005, 27, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Alkaabi, S.; Maningky, M.; Helder, M.N.; Alsabri, G. Virtual and Traditional Surgical Planning in Orthognathic Surgery—Systematic Review and Meta-Analysis. Br. J. Oral Maxillofac. Surg. 2022, 60, 1184–1191. [Google Scholar] [CrossRef]
- Weingart, J.V.; Schlager, S.; Metzger, M.C.; Brandenburg, L.S.; Hein, A.; Schmelzeisen, R.; Bamberg, F.; Kim, S.; Kellner, E.; Reisert, M.; et al. Automated Detection of Cephalometric Landmarks Using Deep Neural Patchworks. Dentomaxillofacial Radiol. 2023, 52, 7280319. [Google Scholar] [CrossRef]
- Pittayapat, P.; Bornstein, M.M.; Imada, T.S.N.; Coucke, W.; Lambrichts, I.; Jacobs, R. Accuracy of Linear Measurements Using Three Imaging Modalities: Two Lateral Cephalograms and One 3D Model from CBCT Data. Eur. J. Orthod. 2015, 37, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Pittayapat, P.; Limchaichana-Bolstad, N.; Willems, G.; Jacobs, R. Three-Dimensional Cephalometric Analysis in Orthodontics: A Systematic Review. Orthod. Craniofacial Res. 2014, 17, 69–91. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Study | Aim of the Study | Materials and Methods | Results | Conclusions |
|---|---|---|---|---|
| Chen et al. [39] | Evaluation of time needed by a clinician (expert and novice) and digital cephalometric analysis system (CADCAS) to perform a cephalometric analysis. | 6 clinicians (3 experts and 3 novices) were asked to perform the cephalometric analysis (tracing, 19 landmark identification and measurements). The same analysis was conducted using CADCAS. | The time spent on analysis in the novice group was longer than in the expert group in cases of tracing and landmarks identification. The time needed for measurements was similar. The CADCAS showed the measurements results straight after landmarks identification. | The experience of a clinician can speed up the process of tracing anatomical structures and landmark identification but not the measurements process. The computer system CADCAS can reduce the time needed for measurements, and it can also reduce the number of errors committed in manual analysis. |
| Baker et al. [42] | Using the computer-assisted surgical simulation (CASS) software programs to assist in the planning of orthognathic surgeries. | Eleven patients qualified to perform orthognathic surgery were evaluated with traditional cephalometry and CASS. | In all cases that were simulated by CASS software, the surgery was successful, and all fabricated splints fit well. However, the CASS system turned out to be better in establishing the midline. | The CASS software proved to be an effective instrument for orthognathic surgery planning. |
| Mario et al. [43] | The use of a paraconsistent artificial neural network (PANN) in cephalometric analysis. | In total, 120 orthodontic patients were subjected to cephalometric analysis by 3 orthodontic experts and PANN using 3 units: anteroposterior, vertical, and dental discrepancy. | The results provided by the experts differed from those of PANN, with inconsistent results. | Manual cephalometric analysis is a subjective analysis by diagnosis that can be made between specialists. PANN treatment methods are more precise and eliminate the disadvantages of traditional analyses |
| Turner et al. [45] | A method of cephalometric analysis is described in which cephalometric X-rays were scanned using a flat-bed scanner and transparency hood. Then, the image was displayed on a computer monitor for point identification and sub- sequent cephalometric analysis using dedicated software. The reproducibility of point identification using this method was compared with two other, commonly used, methods. | The study material comprised 25 lateral skull X-rays taken as part of routine orthodontic assessment. Repeat cephalometric point identification was carried out on each X-ray using 3 methods: 1. On-screen digitization of the scanned bitmap image (Screenceph method); 2. Tracing followed by digitization of the identified points; 3. Direct digitization. | For the 8 angular and 4 linear cephalometric measurements examined, the Screenceph method compared favorably with the two conventional methods. The median difference between methods was 0.5 degrees and 0.2 mm. Using constructed Cartesian axes to examine the x, y discrepancy between repeat measurements and comparing Screenceph to tracing followed by digitization, there were significant differences in 3 instances at the 5% level and 2 instances at the 1% level. These differences represented median scores of 0.14 to 0.32 mm greater for Screenceph. Comparing Screenceph to direct digitization, 15 significant differences out of the 28 measurements were noted: 6 at the 5% level and 9 at the 1% level. The actual difference in median scores ranged from 0.2 mm to 0.53 mm | The results demonstrated that Screenceph is sufficiently accurate to use in a clinical setting but is not yet sufficiently exact for use in research projects owing to hardware limitations. |
| Kuyl et al. [40] | The aim of this study was twofold: (1) to evaluate the importance of the level of training in orthodontics when estimating skeletal configuration by visual inspection of the soft tissue profile, and (2) to evaluate a possible discrepancy between integumental profile (IP) and skeletal class (SC). | 4 test groups comprising 10 orthodontists (0), 10 senior assistants (S), 10 junior assistants (J), and 10 dentists (0) assessed horizontal and vertical skeletal pattern from a series of slides of 100 patients. The assessments were repeated after a 1-month interval. Cephalometric analysis was also carried out by using a number of conventional analyses. | Analysis of the results with Levene’s test, two-factor mixed-design variance analysis, and Newman–Keuls’ multiple-range test showed that (1) orthodontists, independent of their level of training, are more consistent in assessing an IP than dentists; (2) assessments were more consistent for sagittal profile than for vertical profile; (3) sagittally, the Wits’ appraisal corresponds best with IP, and (4) vertically, the Steiner analysis corresponds best with IP. | 1. Duplo-score indicates that sagittal discrepancies were scored more reliably (75%) than the vertical discrepancies (63%). Both scores show a considerable error, indicating that the consistency in scoring an underlying skeletal discrepancy by evaluating the soft tissue profile is not high. 2. Dentists scored less consistently than orthodontists in the repetition test. The level of advanced training in orthodontics had no influence on the consistency of scoring. 3. The recognition of the underlying skeletal discrepancy by evaluating the soft tissue profile was found to be difficult. Dentists had more problems doing so than orthodontists and orthodontists under training. 4. The sagittal profile score was similar between Sassouni’s analysis and the Steiner analysis for all test groups. A small difference was noticed between the Wits’ appraisal and the Steiner standards. The best reference was the Wits’ appraisal reflecting in 65% agreement between the soft tissue profile and the underlying skeletal growth pattern for advanced orthodontists. A percentage of 57% was found for the group of dentists. 5. The highest reflection of the underlying vertical skeletal pattern, evaluated by the soft tissue profile, was found by using the Steiner analysis. The Sassouni standards and the y-axis scored equally. Vertical scores were much lower than the sagittal ones. Differences between the four different test groups were negligible, indicating that advanced training did not contribute to an improvement in the vertical score. 6. The soft tissue profile does not reflect the underlying skeletal growth pattern very well. This does not mean that cephalograms are more accurate in determining the final treatment plan. More significance should be attached to soft tissue profile evaluation than to cephalometric analysis in orthodontic diagnosis and treatment planning. |
| Wang et al. [54] | To explore and compare automatic landmark detection methods in application to cephalometric X-ray images. | Anatomical landmarks were manually marked on cephalograms of 300 patients aged from 6 to 60 years as ground truth data, generated by 2 experienced doctors. Quantitative evaluation was performed to compare the results of a representative selection of current methods submitted to the challenge. |
| Automated methods save time and manual costs and avoid problems caused by intra- and inter-observer variations or errors due to fatigue. |
| Kumar et al. [49] | To compare values of cephalometric analysis performed by CephNinja and NemoCeph for Downs’s analysis. | Diagnostic images were cropped, and scale image was placed on top. A laptop with a mouse-controlled cursor was used for NemoCeph, and an Android phone controlled with a finger touch screen was used for CephNinja. | The difference in mean values obtained using the two softwares showed no statistical significance for 70% of the variables. Y-axis, incisor occlusal plane angle, and the upper incisor to A-Pog showed a statistically significant difference. | CephNinja presented a satisfactory result with NemoCeph, and can be used interchangeably with confidence. |
| Gupta et al. [55] | To evaluate the accuracy of three-dimensional cephalometric measurements obtained through an automatic landmark detection algorithm compared to those obtained through manual identification. | A comparison of 51 cephalometric measurements (28 linear, 16 angles and 7 ratios) on 30 CBCT (cone-beam computed tomography) images. The analysis was performed to compare measurements based on 21 cephalometric landmarks detected automatically and those identified manually by 3 observers. | Inter-observer ICC for each landmark was found to be excellent ([Formula: see text]) among three observers. The unpaired t-test revealed that there was no statistically significant difference in the measurements based on automatically detected and manually identified landmarks. The difference between the manual and automatic observation for each measurement was reported as an error. The highest mean error in the linear and angular measurements was found to be 2.63 mm ([formula: see text] distance) and [formula: see text] ([formula: see text]-Me angle), respectively. The highest mean error in the group of distance ratios was 0.03 (for N-Me/N-ANS and [formula: see text]). | Cephalometric measurements computed from automatic detection of landmarks on 3D CBCT image were as accurate as those computed from manual identification. |
| Dot et al. [53] | Aimed to train and evaluate a deep learning (DL) pipeline based on SpatialConfiguration-Net for automatic localization of 3D cephalometric landmarks on computed tomography (CT) scans. | A retrospective sample of consecutive presurgical CT scans was randomly distributed between a training/validation set (n = 160) and a test set (n = 38). The reference data consisted of 33 landmarks, manually localized once by 1 operator (n = 178) or twice by 3 operators (n = 20, test set only). After inference on the test set, 1 CT scan showed “very low” confidence level predictions; we excluded it from the overall analysis but still assessed and discussed the corresponding results. | The model performance was evaluated by comparing the predictions with the reference data; the outcome set included localization accuracy, cephalometric measurements, and comparison to manual landmarking reproducibility. On the hold-out test set, the mean localization error was 1.0 ± 1.3 mm, while success detection rates for 2.0, 2.5, and 3.0 mm were 90.4%, 93.6%, and 95.4%, respectively. Mean errors were −0.3 ± 1.3° and −0.1 ± 0.7 mm for angular and linear measurements, respectively. When compared to manual reproducibility, the measurements were within the Bland–Altman 95% limits of agreement for 91.9% and 71.8% of skeletal and dentoalveolar variables, respectively. | To conclude, while our DL method still requires improvement, it provided highly accurate 3D landmark localization on a challenging test set, with a reliability for skeletal evaluation on par with what clinicians obtain. |
| Mosleh et al. [46] | This study utilizes some techniques to evaluate reliability, performance, and usability metrics using SUS methods of the developed cephalometric system, which has not been reported in previous studies. | A new system named Ceph-X was developed to computerize the manual cephalometric measurements. The system was developed by using image processing techniques, such as an enhanced X-ray image model, locating landmark model, and computation model. Ceph-X was then evaluated by using X-ray images of 30 subjects (male and female) obtained from the University of Malaya hospital. Three orthodontics specialists were involved in the evaluation of accuracy to avoid intra examiner error, and performance for Ceph-X, and twenty orthodontics specialists were involved in the evaluation of the usability and user satisfaction for Ceph-X by using the SUS approach. | Statistical analysis for the comparison between the manual and automatic cephalometric approaches showed that Ceph-X achieved a great accuracy of approximately 96.6%, with an acceptable error variation approximately less than 0.5 mm and 1°. Results showed that Ceph-X increased the specialist performance and minimized the processing time to obtain cephalometric measurements of the human skull. Furthermore, SUS analysis approach showed that Ceph-X has excellent usability per users’ feedback. | Ceph-X has proved its reliability, performance, and usability and can be used by orthodontists for the analysis, diagnosis, and treatment of cephalometric issues. |
| Chen et al. [41] | Investigating the difference in the positioning of cephalometric points on digital and original cephalometric X-rays. | Cephalometric points were marked on 27 X-rays and, using a computer program, on their digitized counterparts. The absolute difference between measurements was assessed, and statistical analysis was performed | A statistically significant difference (greater than 2 mm or 2 degrees) was seen in 7 of 27 cephalograms. | The difference between measurements is statistically significant but clinically acceptable. |
| Bruntz et al. [51] | Assessment of lateral cephalometric distortions by scanning and printing them, and assessing the accuracy of digital images to perform analysis. | 8 measurement points were marked on 30 cephalometric X-rays, then they were scanned with an accuracy of 150 points per inch and printed with a laser printer. The difference in dot position on all 3 media was assessed. Statistical analysis was performed. | As a result of scanning, the images were enlarged by 0.8 mm vertically and reduced by 0.4 mm vertically. As a result of printing, vertical elongation of 1.1 mm and horizontal extension of 0.4 mm occurred. All differences are statistically significant. | The differences found are not clinically significant. |
| Zamrik et al. [52] | Assessment of the repeatability of cephalometric measurements performed using the traditional method and using the OnCeph Android application. | 22 measurement points were marked on 30 cephalometric photos, and 26 parameters were measured twice for each method. Statistical analysis was performed. | A statistically significant difference was observed in 5 measurements (SNB and nasolabial angles and linear measurements: N I to Pog, U1-A and upper lip to S-line). | The clinically significant difference concerned only one linear U1-A measurement and resulted from an incorrect measurement by the application. The remaining differences are clinically significant. |
| Singh et al. [44] | Evaluation of cephalometric measurements performed by the PACS (picture archiving and communication system) compared to the traditional method. | 6 measurements were made on 5 cephalometric X-rays. Statistical analysis was performed. | A statistically significant difference was demonstrated for 2 angles: SNB and lower incisors. | The differences demonstrated are not clinically significant. |
| Tsorovas et al. [50] | Evaluation of basic and advanced features of 5 different cephalometric analysis programs. Assessment of their compliance with the results obtained using the hand-tracking technique. | 30 digital lateral radiographs comprised the material. 23 measurements were calculated by a single operator, both manually and with the use of 5 different software programs for cephalometric analysis. | Of the 23 measurements tested for each procedure, only 1 (Ii to NB (mm)) showed better agreement with hand-tracing when the advanced features were used. For the remaining 20 measurements, good agreement with hand-tracing was observed for both basic and advanced features. Two measurements (AB on FOP and Ii to A/Pog) showed poor intra-user reproducibility. Hand-tracing required significantly more time compared to both basic and advanced features. The basic features took less time to complete than the advanced features. | A computerized tracing technique, whether basic or advanced, can be considered as equally reliable to hand-tracing for cephalometric measurements, while also being less time-consuming. |
| Kılınç et al. [48] | Comparison and evaluation the reliability of five different cephalometric assessment methods: 1. Smartphone application 2. Tracing method CephNinja (SATM), 3. Web-based artificial intelligence (AI) 4. The conventional hand-tracing method (CHTM). 5. The driven tracing method with WebCeph (WATM). | The study enrolled 110 lateral cephalometric radiographs. One examiner measured 4 linear and 7 angular parameters using WebCeph, CephNinja, and conventional hand-tracing methods. | Statistically significant differences were found between the methods for SNA, SNB, SN-MP angle, U1-SN angle, L1-NB (mm), and E line–upper lip (mm) measurements. | Statistically and clinically significant differences were found among the groups in various measurements. |
| Swennen et al. [47] | Presentation of a modified hard and soft tissue lateral cephalometric cleft analysis to determine the accuracy, validity and reliability of this analysis for the future assessment of craniofacial morphology and growth in cleft patients. | Material comprised 40 conventional lateral cephalometric radiographs of non-cleft children, randomly selected. Lateral cephalometric radiographs were taken under standardized conditions. The study aimed to assess the accuracy, reliability, and validity of the modified cleft analysis. Linear and angular measurements of hard and soft tissues were recorded using 2 different methods: conventional and digital cephalometry. | Measurement error, as determined by the Bland and Altman method, was less than 1.00° and 1.00 mm. The squared correlation coefficients (r2), as determined by the Sackett et al. method, indicated high reliability. | The lateral cephalometric cleft analysis, which utilizes the Onyx Ceph software (version 2.5.6.), has been modified to analyze both hard and soft tissue. The results have demonstrated that this method is accurate, reliable, and suitable for future cleft research. |
| Authors | Comparison | Type of Analysis | Landmarks | Results |
|---|---|---|---|---|
| Chen et al. [39] | Clinicians vs. CADCAS | 19 landmarks and 26 linear and angular measurements were assessed by 6 dentists (experts and novices) and the CADCAS program | N, S, Po, Or, Ar, Go, Me, Gn, Pog, B, A, ANS, PNS, UIA, UIE, LIA, LIE, UM, and LM | Experienced clinician performed better than novice while identifying landmarks, but measurement times were similar; CADCAS resulted in a reduction in human errors and a reduction in analysis duration |
| Baker et al. [42] | CASS vs. traditional analysis | Treatments of 11 orthognathic surgery patients were planned both with CASS and traditional cephalometry | Euler angles | CASS—performed similarly or better than traditional analysis; transverse maxillary cants were observed on the CT cephalometric analyses that were not observed on posterior–anterior radiographic analyses, Spee and Wilson curves were fabricated by software with an averaged occlusal plane what led to accurately corrected occlusal cant, mindfulness of discrepancies between soft tissue midline and bony midline is strongly advised |
| Mario et al. [43] | PANN vs. orthodontists | 120 cases were examined by 3 orthodontists and PANN mathematical model | 1. Anterior cranial base 2. Palatal plane (PP) 3. Occlusal plane (OP) 4. Mandibular plane (MP) 5. Cranial base 6. Y-axis 7. Posterior facial feight 8. Anterior facial height–median third 9. Anterior facial height–lower third 10. Anterior facial height 11. SNA 12. SNB 13. Long axis–upper incisor 14. Long axis—lower incisor 15. A point—Pogonion line Wits: distance between the projections of the A and B points on the occlusal plane. | PANN eliminates problems of traditional analysis; the model points out contradictions presented in the data that were not noticed by the orthodontists, precision of the system increases when more cephalometric variables are added at PANN |
| Turner et al. [45] | Software vs. clinician | On 25 skull X-rays, 14 landmarks were traced in the Screenceph program by mouse cursor, on tracing paper, and then digitized on graphic tablet and directly on graphic tablet; afterwards, 8 angular and 4 linear measurements were taken | S, Ar, Go, PNS, UI Apex, LI Tip, LI Apex, ANS, A, B, UI, Tip, Po, and Me | Screenceph method compared favorably with the two conventional methods; direct digitization of X-rays is the most accurate method of measurement |
| Kuyl et al. [40] | Orthodontists vs. senior assistants vs. junior assistants vs. dentists | 100 cases assessed by 10 well-trained orthodontists, 10 senior postgraduate students, 10 junior postgraduate students, and 10 dentists using the analyses of Steiner, Wits, Sassouni, and Bjork | For the sagittal skeletal pattern, the analyses according to Steiner, Wits, and Sassouni were used, and for the vertical skeletal pattern, those of Steiner, Sassouni, and the y-axis of Bjork were used | Orthodontists perform better than dentists; sagittal profile was more consistently assessed than vertical |
| Wang et al. [54] | Orthodontists vs. AI | 5 automatic landmark detection methods were compared with ground truth data based on landmarks marked manually by orthodontists | Sella turcica, nasion, orbitale, porion, subspinale, supramentale, pogonion, menton, gnathion, gonion, lower incisal incision, upper incisal incision, upper lip, lower lip, subnasale, soft tissue pogonion, posterior nasal spine, anterior nasal spine, articulate | Automated methods save time, intra- and inter-observer variations are eliminated; 3 methods—detection rates greater than 80%, 4 mm precision range; 1 method—detection rate greater than 70%, 2 mm precision range |
| Kumar et al. [49] | Software vs. software | Down’s cephalometric analysis was performed in the programs NemoCeph (landmarks marked on laptop with a mouse cursor) and CephNinja (Android phone controlled with finger touch) | Facial angle Angle of convexity A–B plane angle Mandibular plane angle Y-axis Cant of occlusal plane Inter-incisal angle Incisor occlusal plane angle Incisor mandibular plane angle U1 to A-Pog (linear) | Android-based CephNinja can be an alternative to the computer program NemoCeph |
| Gupta et al. [55] | Orthodontists vs. AI | 3 orthodontists marked 21 landmarks on 30 CBCT images in the MIMICS software (Materialise, Belgium) and those same landmarks were marked in an automatic landmark detection program; afterwards, 51 cephalometric measurements were taken in both methods | Nasion Orbitale left Orbitale right A-point Anterior nasal spine Posterior nasal spine B-point Poronion Menton Gnathion Gonion left Gonion right Condylion left Condylion right #yeomatic point left #yeomatic point right Frontozyzomiatic left Frontozyzomatic right Sella Jugal point left Jugal point right | Both methods equally accurate |
| Dot et al. [53] | Clinicians vs. AI | 33 landmarks were located by 1 orthodontist with 5 years of clinical experience or twice by 3 operators (2 trained orthodontists with 5 years of clinical experience, 1 final-year postgraduate maxillofacial surgeon) to create reference data; then, a deep learning-based landmarking model was created | 11 Apex 11 Edge 16 Occlusal #1 Apex 21 Edge 26 Occlusal 31 Apex 31 Edge 36 Occlusal Ail apex Ai edge A6 Occlusal A point Anterior nasal spine B point Gnathion Gonion L Gonion R Infraorbital foramen L Infraorbital foramen R Internal acoustic foramen L Internal acoustic foramen R Mental foramen L Mental foramen R Menton Nasion Orbitale L Orbitale R Pogonion Porion L Porion R Posterior nasal spine Sella | Deep learning method provides highly accurate 3D landmark detection but still requires improvement |
| Mosleh et al. [46] | Orthodontists vs. software | Manual tracing of 30 cases was performed by an orthodontist, then digitalized radiograph samples were evaluated by 3 orthodontists by marking 12 landmarks both manually and on screen with the CephX system; the system automatically measures 6 angles and 12 lines | N: Nasion S: Sella Po: Porion Or: Orbitale Ar articulare Go: gonion Me: menton ANS: anterior nasal spine PNS: posterior nasal spine Point A: sub-spinal Point B: supramental | CephX reduces the time and effort of manual analysis, and it proved reliable |
| Chen et al. [41] | Orthodontists vs. software | 7 orthodontic residents marked 19 landmarks both manually and on screen, and then 27 measurements were obtained and compared | SNA SNB ANB A-Nv Pog-Nv NAPog VVIts ab SN-FH SN-OP SN-MP UFA/LFA Ar-A Ar-Gn A-Gn Ar-A/Ar-Gn AArGn AGNAr ArAGn UI-SN UI-NPog U-L LI-OP LI-MP au DI u | Inter-observer errors in the manual method were comparable to the ones in digitized images; differences between data in both methods were statistically significant but clinically acceptable |
| Bruntz et al. [51] | Clinician vs. software vs. hard-copy | 30 cases were manually traced using acetate tracing paper then digitalized (both initial and final cephalograms); digitalized versions were traced with 42 landmarks in Dolphin Imaging with the mouse cursor, and hard-copies made from digitalized X-ray photos were also traced manually; this study uses Downs, Steiner, Tweed and Riedel analyses | FP, facial plane; CON, angle of convexity; AB, A point–B point plane to Naison–Pogonion plane; Y, y-axis; OP, occlusal plane; INT, interncisal angle; L1OP, lower incisor to occlusal plane; L1MP, lower incisor to mandibular plane; U1AP, upper incisor to A point–Pogonion plane; U1FH, upper incisor to Frankfort horizontal plane; FH/NA, Frankfort horizontal plane to Nasion–A point plane; U1NA, upper incisor to Naison–A point plane; L1NB, lower incisor to Naison–B point plane; PONB, Pogonion to Naison B point plane; POL1NB, Pogonion–lower incisor plane to Naison–B point plane. | There is a difficulty in identifying certain landmarks (porion and orbitale) in computerized program and printed hard-copy; otherwise, all cephalometric analyses showed comparable accuracies |
| Zamrik et al. [52] | Clinician vs. smartphone software | 30 cases were traced manually (22 landmarks, 7 planes, 26 linear and angular parameters) and digital versions were traced in the OneCeph program twice by the same investigator | Sella (S), nasion (N), anterior nasal spine (ANS), posterior nasal spine (PNS), A point (A), incisor superius (Is), incisor inferius (Ii), B point (B), pogonion (Pog), gnathion (Gn), menton (Me), gonion (Go), condylon (Cd), articulare (Ar), orbitale (Or), porion (Po), mid-point between molar superioris (Ms) and molar inferioris (Mi), (18) subnasal (Sn), (19) S point (Steiner analysis), (20) labial superius (LS), (21) labial inferius (LI), (22) soft tissue pogonion (Pog’). (A) SN plane, (B) Frankfort plane (Po-Or), (C) maxillary plane (ANS-PNS), (D) bisecting occlusal plane (BOP), (E) mandibular plane (Go-Gn), (F) mandibular plane (Go-Me), (G) mandibular plane (tangent to lower border of mandible) | Differences between the tracing methods were clinically insignificant except for the U1-A point measurement—the app incorrectly calculated the distance from the A line to the incisal edge of the upper central incisor rather than the facial surface of the upper incisor |
| Singh et al. [44] | Clinician vs. software | 5 cases were traced digitally and manually, and 7 angular and 4 linear parameters were measured by 2 operators with 4 years of experience in the hand-tracing method and 1 year of experience in the digital method | SNA: angle between points S, N, and A; SNB: angle between points S, N, and B; ANB: angle between points A, N, and B; MMPA: angle between the maxillary plane (ANS to PNS) and the mandibular plane (Go to Me) | The PACS system could be an acceptable method for cephalometric analysis—no significant difference between the manual and digitalized methods |
| Tsorovas et al. [50] | Clinician vs. software | 30 cases were traced manually by 1 observer (27 landmarks, 23 measurements) and afterwards were traced digitally in all 5 pieces of software with their basic and advanced features; the total time needed to trace the images was measured and compared | 1: Sella (S), the midpoint of sella turcica; 2: nasion (N), junction of the frontal and nasal bones at the naso-frontal suture; 3: glabella (G′), the most anterior point on the forehead, in the region of the supra-orbital ridges; 4: pronasale (Pr′), the most anterior point on the nasal tip; 5: subnasale (Sn′), the junction of the columella of the nose with the philtrum of the upper lip; 6: Labrare Superios. (Ls), the muco-cutaneous junction of the upper lip and philtrum; 7: Labrare Inferios. (Li), the muco-cutaneous junction of the lower lip and philtrum; 8: soft Pogonion (Pg′), the most anterior point on the soft tissue chin; 9:mMenton (Me), the most inferior point on the bony chin; 10: Pogonion (Pg), the most anterior point on the bony chin; 11: point B, the deepest point in the concavity of the anterior mandible between the alveolar crest and pogonion; 12: lower incisor apex, the root apex of the lower central incisor; 13: lower incisor tip, the tip of the crown of the lower central incisor; 14: upper incisor tip, the tip of the crown of the upper central incisor; 15: upper incisor apex, the root apex of the upper central incisor; 16: point A, the deepest point in the concavity of the anterior maxilla between anterior nasal spine and the alveolar crest; 17: anterior nasal spine (ANS), the anterior limit of the floor of the nose, at the tip of anterior nasal spine; 18: posterior nasal spine (PNS), the posterior limit of the floor of the nose, at the tip of posterior nasal spine; 19: lower molar crown, the tip of the mesial cusp of the lower first molar; 20: lower first premolar tip, the tip of the crown of the lower first premolar; 21: inferior gonion, a mid-planed point at a tangent to the inferior border of the mandible near the gonion; 22: posterior gonion, a mid-planed point at a tangent to the posterior border of the mandible near gonion; 23: Ad1, a landmark located at the intersection of the line between PNS and basion with the posterior nasopharyngeal wall; 24: basion (Ba), the most inferior point on the anterior margin of the foramen magnum; 25: articulare (Ar), a mid-planed point located at the intersection of the posterior border of the ramus with the inferior surface of the cranial base; 26: porion (Po), the most superior point of the bony external auditory meatus; 27: orbitale (Or), the most inferior point on the infra-orbital margin | The computerized tracing method (either with basis or advanced features) takes less time and is equally reliable when compared to the manual method |
| Kılınç et al. [48] | Clinician vs. software vs. AI | 110 cases were traced manually by 1 technician, on the smartphone application CephNinja and in WebCeph (an AI web-based orthodontic analysis platform) | SNA, SNB, SN-MP angle, U1-SN angle, L1-NB (mm), and E line–upper lip (mm) | Statistically and clinically significant differences were observed between three methods; however, the zoom function in applications gave much clearer images; AI software promises higher comfort, practicality, and speed |
| Swennen et al. [47] | Clinician vs. software | 40 cases were traced manually by 2 investigators and in Onyx Ceph | Ba = basion, anterior lip of the foramen magnum; S = sella, estimated center of the hypophyseal fossa; R = registration point, point of crossing of the greater wing of the sphenoid and planum sphenoidale; N = nasion, junction of the nasal and frontal bone; NB = lip of nasal bone; ANS = anterior nasal spine; A = point of greatest concavity of the alveolar process of the maxilla; UI = upper incisor; UI-apex = upper incisor apex; LI = lower incisor; Li-apex = lower incisor apex; B = point of greatest concavity of the mandibular alveolar process; Pog = pogonion, most prominent point on the chin; Gn = gnathion, point on the symphysis between pogonion and menton farthest from the condyle; Men = menton, most inferior point on the symphysis; Co = condylion, posterior superior point on the outline of the condyle; PTM = pterygomaxillary fissure, the inferior point in the fissure; PNS = posterior nasal spine. Hard tissue landmarks necessary to construct other cephalometric reference points: TgA = mandibular body tangent; TgP = mandibular ramus tangent; Ar = articulare, point at the intersection between the contour of the mandibular ramus and occipital bone; UM-cusp = upper molar mesial cuspides; LM-cusp = lower molar mesial cuspides. Constructed landmarks: Go = gonion, a constructed point on the outline of the mandible by bisecting the ramus plane (Ar-TgP) and body plane (TgA-Men); PMP = posterior maxillary point, a constructed point created by dropping perpendicular to the maxillary plane (PNS-ANS) from the PTM; OccA = anterior point of the occlusal plane, a constructed point at the midline between UI and LI; OccP = posterior point of the occlusal plane, a constructed point at the midline between UM-cusp and LM-cusp. References lines: Ba-N = reference line to scale all linear measurements; S-N = anterior cranial base, line from S through N; MxPl = maxillary plane, line from PNS through ANS; OccPl = occlusal plane, line from OccP through OccA; MdPl = mandibular plane, line from Go through Men | Onyx Ceph software is an accurate and reliable method for lateral cephalometric cleft analysis; both traditional and digitized method proved to be highly accurate and reliable techniques for measuring hard and soft tissues in patients with clefts |
| Group Size at Least 10 Subjects | Sample Size Calculation | Blind Study or Not | At Least 5 Landmarks Used | Triple Measurements | Experience of Researchers | Total Points | Risk of Bias | |
|---|---|---|---|---|---|---|---|---|
| Chen et al. [39] | 1 | 0 | 0 | 1 | 0 | 1 | 3 | moderate |
| Baker et al. [42] | 1 | 0 | 0 | 0 | 0 | 0 | 1 | high |
| Mario et al. [43] | 1 | 0 | 0 | 1 | 0 | 1 | 3 | moderate |
| Turner et al. [45] | 1 | 0 | 0 | 1 | 0 | 0 | 2 | high |
| Kuyl et al. [40] | 1 | 0 | 0 | 1 | 0 | 1 | 3 | moderate |
| Wang et al. [54] | 1 | 0 | 0 | 1 | 0 | 1 | 3 | moderate |
| Kumar et al. [49] | 1 | 1 | 1 | 1 | 0 | 1 | 5 | low |
| Gupta et al. [55] | 1 | 0 | 0 | 1 | 0 | 1 | 3 | moderate |
| Dot et al. [53] | 1 | 0 | 0 | 1 | 0 | 1 | 3 | moderate |
| Mosleh et al. [46] | 1 | 0 | 0 | 1 | 0 | 1 | 3 | moderate |
| Chen et al. [41] | 1 | 0 | 0 | 1 | 0 | 0 | 2 | high |
| Bruntz et al. [51] | 1 | 0 | 0 | 1 | 0 | 0 | 2 | high |
| Zamrik et al. [52] | 1 | 0 | 0 | 1 | 0 | 0 | 2 | high |
| Singh et al. [44] | 0 | 0 | 0 | 1 | 0 | 1 | 2 | high |
| Tsorovas et al. [50] | 1 | 0 | 0 | 1 | 0 | 1 | 3 | moderate |
| Kılınç et al. [48] | 1 | 0 | 0 | 1 | 0 | 1 | 3 | moderate |
| Swennen et al. [47] | 1 | 0 | 0 | 1 | 0 | 0 | 2 | high |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smołka, P.; Nelke, K.; Struzik, N.; Wiśniewska, K.; Kiryk, S.; Kensy, J.; Dobrzyński, W.; Kiryk, J.; Matys, J.; Dobrzyński, M. Discrepancies in Cephalometric Analysis Results between Orthodontists and Radiologists and Artificial Intelligence: A Systematic Review. Appl. Sci. 2024, 14, 4972. https://doi.org/10.3390/app14124972
Smołka P, Nelke K, Struzik N, Wiśniewska K, Kiryk S, Kensy J, Dobrzyński W, Kiryk J, Matys J, Dobrzyński M. Discrepancies in Cephalometric Analysis Results between Orthodontists and Radiologists and Artificial Intelligence: A Systematic Review. Applied Sciences. 2024; 14(12):4972. https://doi.org/10.3390/app14124972
Chicago/Turabian StyleSmołka, Piotr, Kamil Nelke, Natalia Struzik, Kamila Wiśniewska, Sylwia Kiryk, Julia Kensy, Wojciech Dobrzyński, Jan Kiryk, Jacek Matys, and Maciej Dobrzyński. 2024. "Discrepancies in Cephalometric Analysis Results between Orthodontists and Radiologists and Artificial Intelligence: A Systematic Review" Applied Sciences 14, no. 12: 4972. https://doi.org/10.3390/app14124972
APA StyleSmołka, P., Nelke, K., Struzik, N., Wiśniewska, K., Kiryk, S., Kensy, J., Dobrzyński, W., Kiryk, J., Matys, J., & Dobrzyński, M. (2024). Discrepancies in Cephalometric Analysis Results between Orthodontists and Radiologists and Artificial Intelligence: A Systematic Review. Applied Sciences, 14(12), 4972. https://doi.org/10.3390/app14124972