

The Association between Serum Vitamin D Levels and Urinary Tract Infection Risk in Children: A Systematic Review and Meta-Analysis

Highlights
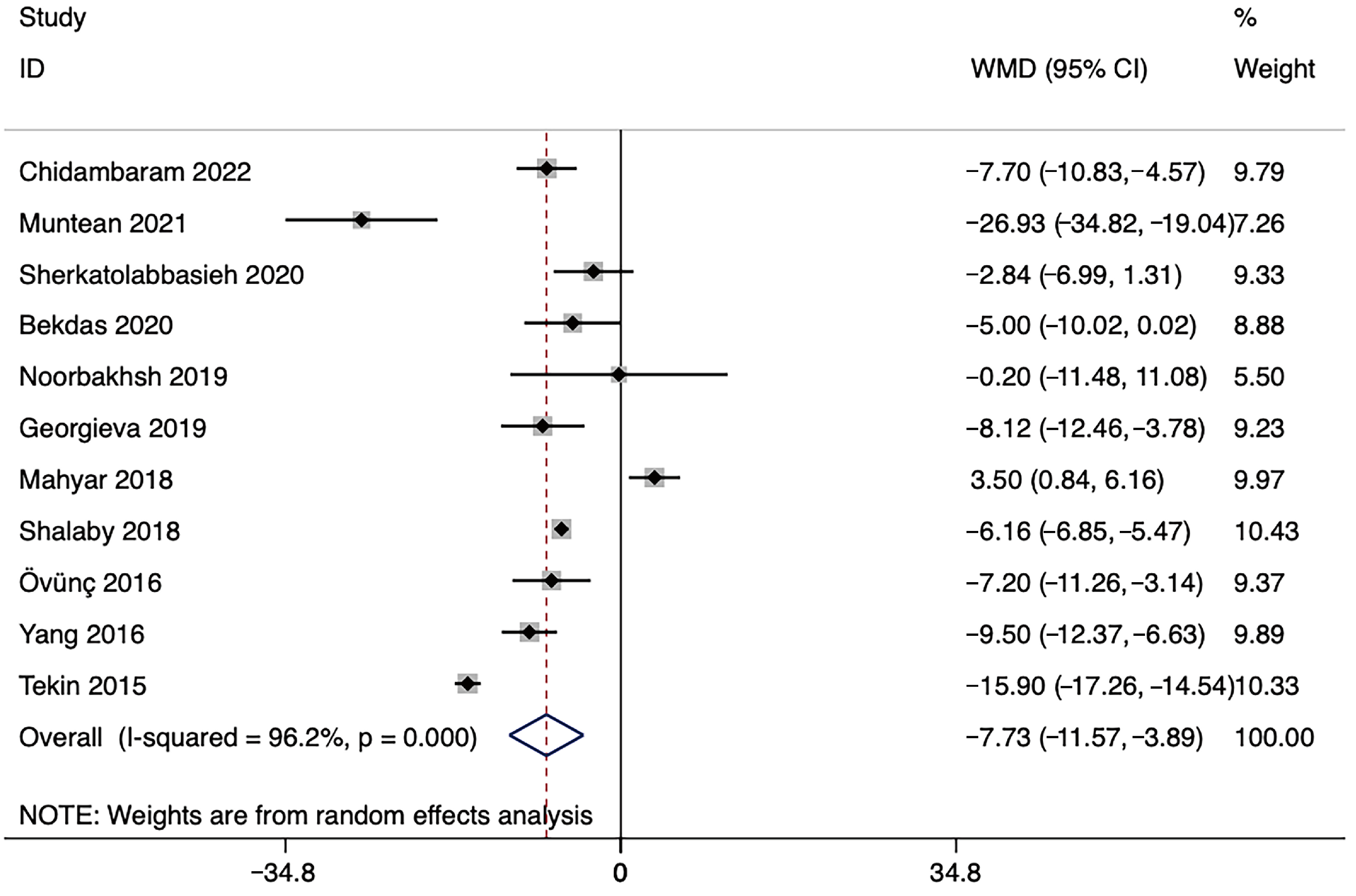
- Serum vitamin D levels were 7.730 ng/mL lower in children with urinary tract infections (UTIs) compared to the controls.
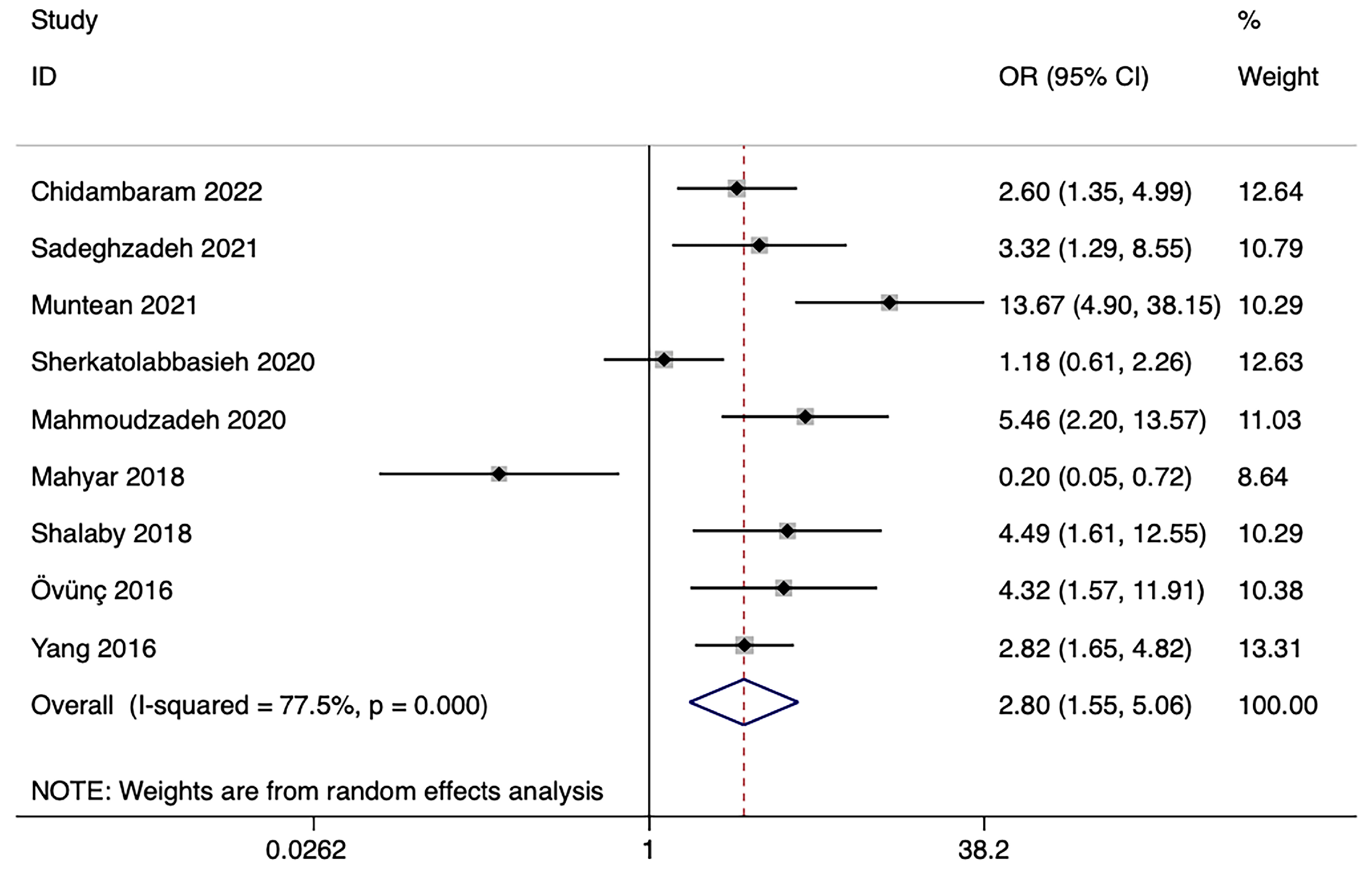
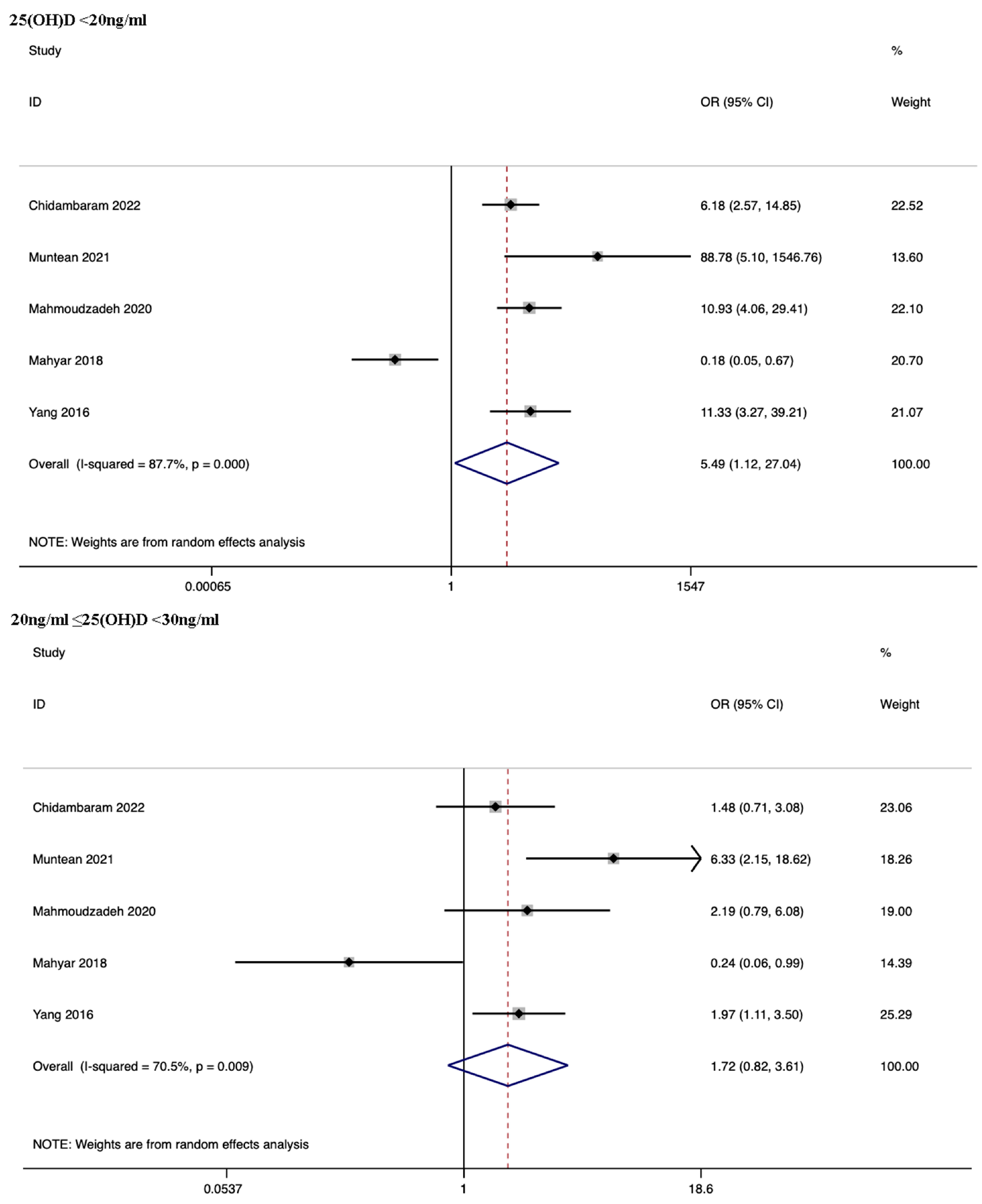
- Children with serum vitamin D levels below 20 ng/mL were significantly more likely to develop UTIs.
- Lower serum vitamin D levels were associated with a higher risk of UTI in children.
- This highlights the potential importance of vitamin D supplementation as a preventive measure for reducing UTI risk in children.
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
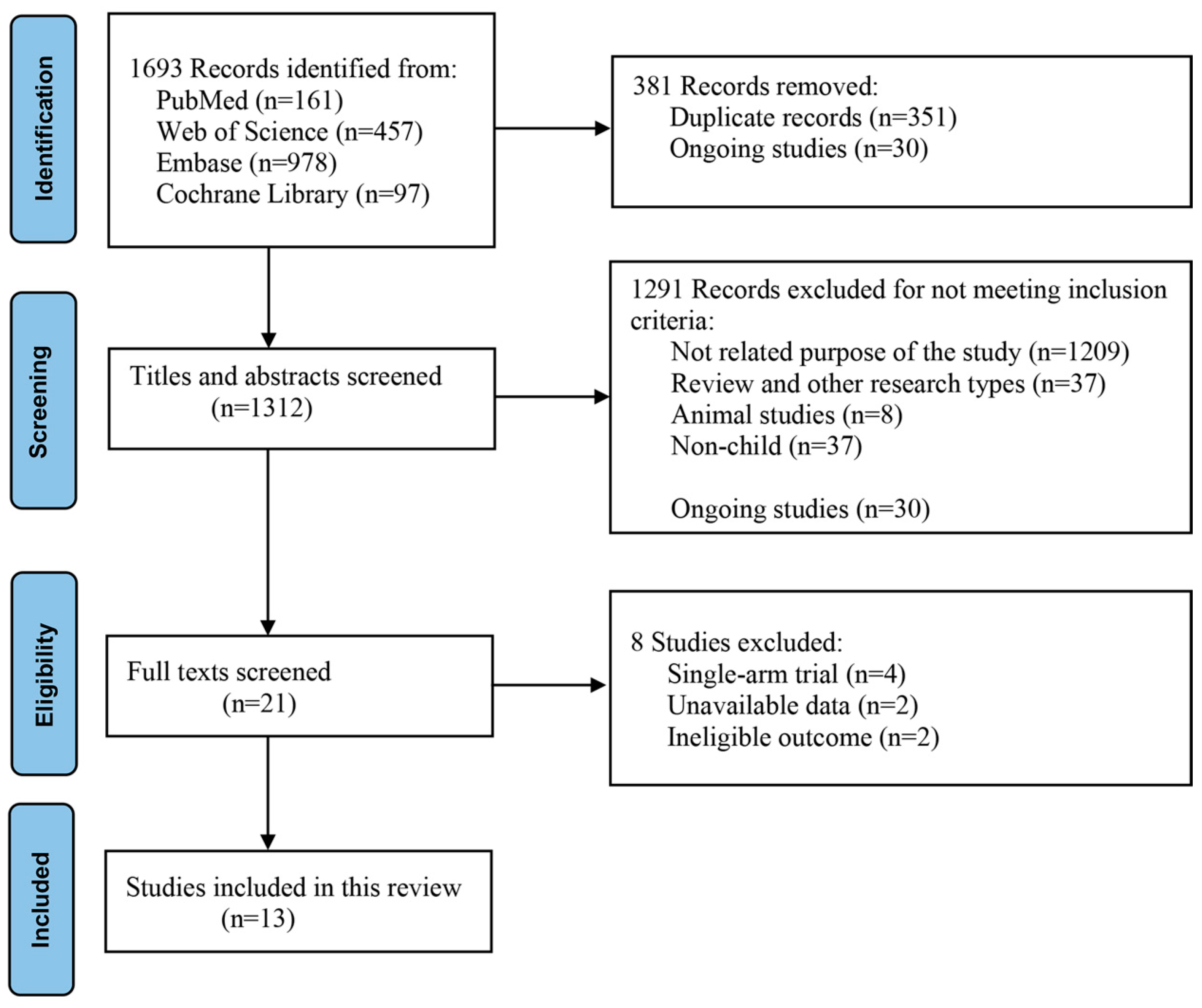
3.1. Literature Search
3.2. Characteristics and Quality Assessment of the Included Studies
3.3. Meta-Analyses
3.3.1. Meta-Analysis of Serum Vitamin D Levels
3.3.2. Meta-Analysis of ORs
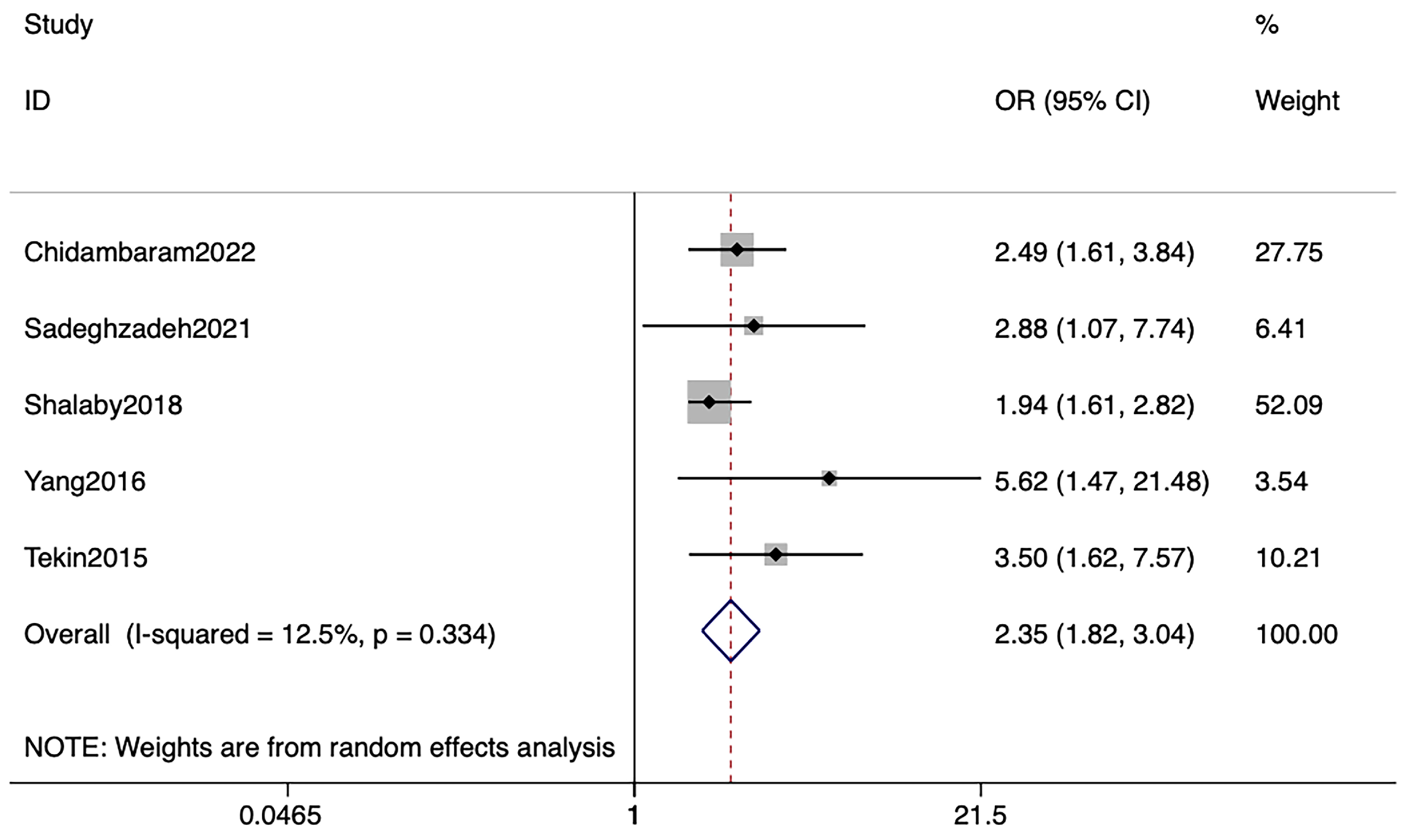
3.3.3. Meta-Analysis of Adjusted ORs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zorc, J.J.; Levine, D.A.; Platt, S.L.; Dayan, P.S.; Macias, C.G.; Krief, W.; Schor, J.; Bank, D.; Shaw, K.N.; Kuppermann, N. Clinical and demographic factors associated with urinary tract infection in young febrile infants. Pediatrics 2005, 116, 644–648. [Google Scholar] [CrossRef]
- Mattoo, T.K.; Shaikh, N.; Nelson, C.P. Contemporary Management of Urinary Tract Infection in Children. Pediatrics 2021, 147, e2020012138. [Google Scholar] [CrossRef]
- Schlager, T.A. Urinary Tract Infections in Infants and Children. Microbiol. Spectr. 2016, 4, 4–5. [Google Scholar] [CrossRef]
- Shaikh, N.; Morone, N.E.; Lopez, J.; Chianese, J.; Sangvai, S.; D’Amico, F.; Hoberman, A.; Wald, E.R. Does this child have a urinary tract infection? JAMA 2007, 298, 2895–2904. [Google Scholar] [CrossRef]
- Stein, R.; Dogan, H.S.; Hoebeke, P.; Kočvara, R.; Nijman, R.J.; Radmayr, C.; Tekgül, S. Urinary tract infections in children: EAU/ESPU guidelines. Eur. Urol. 2015, 67, 546–558. [Google Scholar] [CrossRef]
- White, J.H. Vitamin D signaling, infectious diseases, and regulation of innate immunity. Infect. Immun. 2008, 76, 3837–3843. [Google Scholar] [CrossRef]
- Mangin, M.; Sinha, R.; Fincher, K. Inflammation and vitamin D: The infection connection. Inflamm. Res. 2014, 63, 803–819. [Google Scholar] [CrossRef]
- Fletcher, J.; Bishop, E.L.; Harrison, S.R.; Swift, A.; Cooper, S.C.; Dimeloe, S.K.; Raza, K.; Hewison, M. Autoimmune disease and interconnections with vitamin D. Endocr. Connect. 2022, 11, e210554. [Google Scholar] [CrossRef]
- Kamen, D.L.; Tangpricha, V. Vitamin D and molecular actions on the immune. system: Modulation of innate and autoimmunity. J. Mol. Med. 2010, 88, 441–450. [Google Scholar] [CrossRef]
- Deluca, H.F.; Cantorna, M.T. Vitamin D: Its role and uses in immunology. FASEB J. 2001, 15, 2579–2585. [Google Scholar] [CrossRef]
- Ganmaa, D.; Enkhmaa, D.; Nasantogtokh, E.; Sukhbaatar, S.; Tumur-Ochir, K.E.; Manson, J.E. Vitamin D, respiratory infections, and chronic disease: Review of meta-analyses and randomized clinical trials. J. Intern. Med. 2022, 291, 141–164. [Google Scholar] [CrossRef]
- Islam, M.A.; Khandker, S.S.; Alam, S.S.; Kotyla, P.; Hassan, R. Vitamin D status in patients with systemic lupus erythematosus (SLE): A systematic review and meta-analysis. Autoimmun. Rev. 2019, 18, 102392. [Google Scholar] [CrossRef]
- Székely, J.I.; Pataki, Á. Effects of vitamin D on immune disorders with special. regard to asthma, COPD and autoimmune diseases: A short review. Expert Rev. Respir. Med. 2012, 6, 683–704. [Google Scholar] [CrossRef]
- Adams, J.S.; Hewison, M. Update in vitamin D. J. Clin. Endocrinol. Metab. 2010, 95, 471–478. [Google Scholar] [CrossRef]
- Nnoaham, K.E.; Clarke, A. Low serum vitamin D levels and tuberculosis: A systematic review and meta-analysis. Int. J. Epidemiol. 2008, 37, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Laaksi, I.; Ruohola, J.P.; Tuohimaa, P.; Auvinen, A.; Haataja, R.; Pihlajamäki, H.; Ylikomi, T. An association of serum vitamin D concentrations < 40 nmol/L with acute respiratory tract infection in young Finnish men. Am. J. Clin. Nutr. 2007, 86, 714–717. [Google Scholar]
- Schwalfenberg, G.K. A review of the critical role of vitamin D in the functioning. of the immune system and the clinical implications of vitamin D deficiency. Mol. Nutr. Food Res. 2011, 55, 96–108. [Google Scholar] [CrossRef]
- Science, M.; Maguire, J.L.; Russell, M.L.; Smieja, M.; Walter, S.D.; Loeb, M. Low serum 25-hydroxyvitamin D level and risk of upper respiratory tract infection in children and adolescents. Clin. Infect. Dis. 2013, 57, 392–397. [Google Scholar] [CrossRef]
- Shah, K.; Varna, V.P.; Pandya, A.; Saxena, D. Low vitamin D levels and prognosis in a COVID-19 pediatric population: A systematic review. QJM 2021, 114, 447–453. [Google Scholar] [CrossRef]
- di Filippo, L.; Uygur, M.; Locatelli, M.; Nannipieri, F.; Frara, S.; Giustina, A. Low vitamin D levels predict outcomes of COVID-19 in patients with both severe and non-severe disease at hospitalization. Endocrine 2023, 80, 669–683. [Google Scholar] [CrossRef]
- Hertting, O.; Holm, Å.; Lüthje, P.; Brauner, H.; Dyrdak, R.; Jonasson, A.F.; Wiklund, P.; Chromek, M.; Brauner, A. Vitamin D induction of the human antimicrobial Peptide cathelicidin in the urinary bladder. PLoS ONE 2010, 5, e15580. [Google Scholar] [CrossRef]
- Övünç Hacıhamdioğlu, D.; Altun, D.; Hacıhamdioğlu, B.; Çekmez, F.; Aydemir, G.; Kul, M.; Müftüoğlu, T.; Süleymanoğlu, S.; Karademir, F. The Association between Serum 25-Hydroxy Vitamin D Level and Urine Cathelicidin in Children with a Urinary Tract Infection. J. Clin. Res. Pediatr. Endocrinol. 2016, 8, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Mahyar, A.; Ayazi, P.; Safari, S.; Dalirani, R.; Javadi, A.; Esmaeily, S. Association between vitamin D and urinary tract infection in children. Korean J. Pediatr. 2018, 61, 90–94. [Google Scholar] [CrossRef]
- Chidambaram, S.; Pasupathy, U.; Geminiganesan, S.; R, D. The Association Between Vitamin D and Urinary Tract Infection in Children: A Case-Control Study. Cureus 2022, 14, e25291. [Google Scholar] [CrossRef]
- Tekin, M.; Konca, C.; Celik, V.; Almis, H.; Kahramaner, Z.; Erdemir, A.; Gulyuz, A.; Uckardes, F.; Turgut, M. The Association between Vitamin D Levels and Urinary Tract Infection in Children. Horm. Res. Paediatr. 2015, 83, 198–203. [Google Scholar] [CrossRef]
- Georgieva, V.; Kamolvit, W.; Herthelius, M.; Lüthje, P.; Brauner, A.; Chromek, M. Association between vitamin D, antimicrobial peptides and urinary tract infection in infants and young children. Acta Paediatr. 2019, 108, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudzadeh, H.; Nikibakhsh, A.A.; Pashapour, S.; Ghasemnejad-Berenji, M. Relationship between low serum vitamin D status and urinary tract infection in children: A case-control study. Paediatr. Int. Child Health 2020, 40, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Sadeghzadeh, M.; Khoshnevisasl, P.; Motamed, N.; Faghfouri, L. The serum vitamin D levels in children with urinary tract infection: A case-control study. New Microbes New Infect. 2021, 43, 100911. [Google Scholar] [CrossRef]
- Shalaby, S.A.; Handoka, N.M.; Amin, R.E. Vitamin D deficiency is associated with urinary tract infection in children. Arch. Med. Sci. 2018, 14, 115–121. [Google Scholar] [CrossRef]
- Muntean, C.; Săsăran, M. Vitamin D Status and Its Role in First-Time and Recurrent Urinary Tract Infections in Children: A Case-Control Study. Children 2021, 8, 419. [Google Scholar] [CrossRef]
- Raza, M.; Jabeen, N.; Najam, M.; Tareen, R.; Intekhab, A.; Uz Zaman Shahzad, Q.; Hamza, M. Determine the Mean Levels of Vitamin D in Children with First Episode of Urinary Tract Infection. Pak. J. Med. Health Sci. 2022, 16, 733–735. [Google Scholar] [CrossRef]
- Qadir, S.; Memon, S.; Chohan, M.N.; Memon, Y. Frequency of Vitamin-D deficiency in children with Urinary tract infection: A descriptive cross-sectional study. Pak. J. Med. Sci. 2021, 37, 1058–1062. [Google Scholar] [CrossRef]
- Yang, J.; Chen, G.; Wang, D.; Chen, M.; Xing, C.; Wang, B. Low serum. 25-hydroxyvitamin D level and risk of urinary tract infection in infants. Medicine 2016, 95, e4137. [Google Scholar] [CrossRef]
- Sherkatolabbasieh, H.; Firouzi, M.; Shafizadeh, S.; Nekohid, M. Evaluation of. the relationship between vitamin D levels and prevalence of urinary tract infections in children. New Microbes New Infect. 2020, 37, 100728. [Google Scholar] [CrossRef]
- Noorbakhsh, S.; Nia, S.J.; Movahedi, Z.; Ashouri, S. Does the trace element deficiency (vit A, D & zinc) have any role in vulnerability to urinary tract infection in children: A case-control study: Tehran, Iran. Open Urol. Nephrol. J. 2019, 12, 23–26. [Google Scholar]
- Katikaneni, R.; Ponnapakkam, T.; Ponnapakkam, A.; Gensure, R. Breastfeeding does not protect against urinary tract infection in the first 3 months of life, but vitamin D supplementation increases the risk by 76%. Clin. Pediatr. 2009, 48, 750–755. [Google Scholar] [CrossRef]
- Li, X.; Yu, Q.; Qin, F.; Zhang, B.; Lu, Y. Serum Vitamin D Level and the Risk of Urinary Tract Infection in Children: A Systematic Review and Meta-Analysis. Front. Public Health 2021, 9, 637529. [Google Scholar] [CrossRef]
- Lips, P.; Cashman, K.D.; Lamberg-Allardt, C.; Bischoff-Ferrari, H.A.; Obermayer-Pietsch, B.; Bianchi, M.L.; Stepan, J.; El-Hajj Fuleihan, G.; Bouillon, R. Current vitamin D status in European and Middle East countries and strategies to prevent vitamin D deficiency: A position statement of the European Calcified Tissue Society. Eur. J. Endocrinol. 2019, 180, 23–54. [Google Scholar] [CrossRef]
- Bekdas, M.; Caliskan, B.; Karabork, S.; Acar, S.; Kabakus, N. Do low vitamin D levels facilitae renal parenchymal injury? Paediatr. Indones. 2020, 60, 205–211. [Google Scholar] [CrossRef]
- van Schoor, N.M.; Lips, P. Worldwide vitamin D status. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 671–680. [Google Scholar] [CrossRef]
- Öhlund, I.; Silfverdal, S.A.; Hernell, O.; Lind, T. Serum 25-hydroxyvitamin D levels in preschool-age children in northern Sweden are inadequate after summer and diminish further during winter. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Lips, P. Worldwide status of vitamin D nutrition. J. Steroid. Biochem. Mol. Biol. 2010, 121, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Lips, P. Vitamin D status and nutrition in Europe and Asia. J. Steroid Biochem. Mol. Biol. 2007, 103, 620–625. [Google Scholar] [CrossRef]
- Bater, J.; Bromage, S.; Jambal, T.; Tsendjav, E.; Lkhagvasuren, E.; Jutmann, Y.; Martineau, A.R.; Ganmaa, D. Prevalence and Determinants of Vitamin D Deficiency in 9595 Mongolian Schoolchildren: A Cross-Sectional Study. Nutrients 2021, 13, 4175. [Google Scholar] [CrossRef]
- Chen, Z.; Lv, X.; Hu, W.; Qian, X.; Wu, T.; Zhu, Y. Vitamin D Status and. Its Influence on the Health of Preschool Children in Hangzhou. Front. Public Health 2021, 9, 675403. [Google Scholar] [CrossRef]
- Wang, L.L.; Wang, H.Y.; Wen, H.K.; Tao, H.Q.; Zhao, X.W. Vitamin D status among infants, children, and adolescents in southeastern China. J. Zhejiang Univ. Sci. B 2016, 17, 545–552. [Google Scholar] [CrossRef]
- Oktaria, V.; Putri, D.A.D.; Ihyauddin, Z.; Julia, M.; Sulistyoningrum, D.C.; Koon, P.B.; Danchin, M.; Murni, I.K. Vitamin D deficiency in South-East Asian children: A systematic review. Arch. Dis. Child 2022, 107, 980–987. [Google Scholar] [CrossRef]
- Płudowski, P.; Kos-Kudła, B.; Walczak, M.; Fal, A.; Zozulińska-Ziółkiewicz, D.; Sieroszewski, P.; Peregud-Pogorzelski, J.; Lauterbach, R.; Targowski, T.; Lewiński, A.; et al. Guidelines for Preventing and Treating Vitamin D Deficiency: A 2023 Update in Poland. Nutrients 2023, 15, 695. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Country | Total Number Cases/Controls | Age | Vitamin D (ng/mL) | Exposure Number Cases/ Controls | Estimated OR (95% CI) | Newcastle -Ottawa Score | |
|---|---|---|---|---|---|---|---|---|---|
| UTI | Control | ||||||||
| Chidambaram 2022 [24] | case–control | South India | 82/82 | UTI: 2.36 ± 1.42 y control: 2.57 ± 1.26 y | 24.27 ± 9.70 | 31.97 ± 10.7 | 60/42 | Adjusted OR: 2.486 (1.610, 3.838) | 8 |
| Sadeghzadeh 2021 [28] | case–control | Iran | 40/40 | 1–12 y | _ | _ | 30/19 | Adjusted OR: 2.884 (1.075, 7.738) | 7 |
| Muntean 2021 [30] | case–control | Romania | 59/42 | UTI: 3.95 ± 2.94 y control: 3.25 ± 3.03 y | 26.06 ± 14.25 | 52.99 ± 23.16 | 41/6 | _ | 7 |
| Sherkatolabbasieh 2020 [34] | case–control | Iran | 44/214 | UTI: 6.58 ± 1.57 y control: 6.7 ± 1.58 y | 29.2 ± 12.27 | 32.04 ± 15.04 | 25/113 | _ | 8 |
| Mahmoudzadeh 2020 [27] | case–control | Iran | 75/75 | UTI: 6.9 ± 4.2 y control: 7.9 ± 3.8 y | _ | _ | 68/48 | _ | 7 |
| Bekdas 2020 [39] | case–control | Turkey | 43/24 | UTI: 6.9 ± 4.2 y control: 7.9 ± 3.8 y | 18 ± 9 | 23 ± 10.6 | _ | _ | 6 |
| Noorbakhsh 2019 [35] | case–control | Iran | 25/40 | mean: 2.7 y | 45.7 ± 21.05 | 45.9 ± 24.8 | _ | _ | 7 |
| Georgieva 2019 [26] | cross-section | Sweden | 76/44 | 4.5–33.5 m | 32.32 ± 8.48 | 40.44 ± 13.2 | _ | _ | 5 |
| Mahyar 2018 [23] | case–control | Iran | 70/70 | UTI: 53.2 ± 35.6 m control: 62.2 ± 36.1 m | 20.4 ± 8.6 | 16.9 ± 7.4 | 57/67 | _ | 8 |
| Shalaby 2018 [29] | case–control | Egypt | 50/50 | UTI: 0.98 ± 1.15 y control: 0.90 ± 1.23 y | 4.2 ± 1.08 | 10.36 ± 2.24 | 19/6 | Adjusted OR: 1.94 (1.61, 2.82) | 7 |
| Övünç 2016 [22] | case–control | Turkey | 36/38 | UTI: 6.8 ± 3.6 y control: 6.3 ± 2.8 y | 16.5 ± 6.3 | 23.7 ± 11 | 28/17 | _ | 7 |
| Yang 2016 [33] | case–control | China | 132/106 | UTI: 7.29 ± 3.06 m control: 7.09 ± 3.25 m | 29.09 ± 9.56 | 38.59 ± 12.41 | 74/33 | Adjusted OR: 5.619 (1.469, 21.484) | 7 |
| Tekin 2015 [25] | case–control | Turkey | 82/64 | UTI: 2.57 ± 2.56 y control: 2.10 ± 1.37 y | 11.7 ± 3.3 | 27.6 ± 4.7 | _ | Adjusted OR: 3.503 (1.621, 7.571) | 8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gan, Y.; You, S.; Ying, J.; Mu, D. The Association between Serum Vitamin D Levels and Urinary Tract Infection Risk in Children: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 2690. https://doi.org/10.3390/nu15122690
Gan Y, You S, Ying J, Mu D. The Association between Serum Vitamin D Levels and Urinary Tract Infection Risk in Children: A Systematic Review and Meta-Analysis. Nutrients. 2023; 15(12):2690. https://doi.org/10.3390/nu15122690
Chicago/Turabian StyleGan, Yan, Siyi You, Junjie Ying, and Dezhi Mu. 2023. "The Association between Serum Vitamin D Levels and Urinary Tract Infection Risk in Children: A Systematic Review and Meta-Analysis" Nutrients 15, no. 12: 2690. https://doi.org/10.3390/nu15122690
APA StyleGan, Y., You, S., Ying, J., & Mu, D. (2023). The Association between Serum Vitamin D Levels and Urinary Tract Infection Risk in Children: A Systematic Review and Meta-Analysis. Nutrients, 15(12), 2690. https://doi.org/10.3390/nu15122690