
COVID-19 Phenotypes and Comorbidity: A Data-Driven, Pattern Recognition Approach Using National Representative Data from the United States

 ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
- The use of reported symptoms to identify latent structures via categorical PCA and dimension reduction approaches, using data from the COVID-19 Delphi Facebook study.
- To scrutinize the previously created latent structures as potential COVID-19 phenotypes or phenotyping parameters via TSC and artificial intelligence-based classification.
2. Materials and Methods
2.1. Study Population
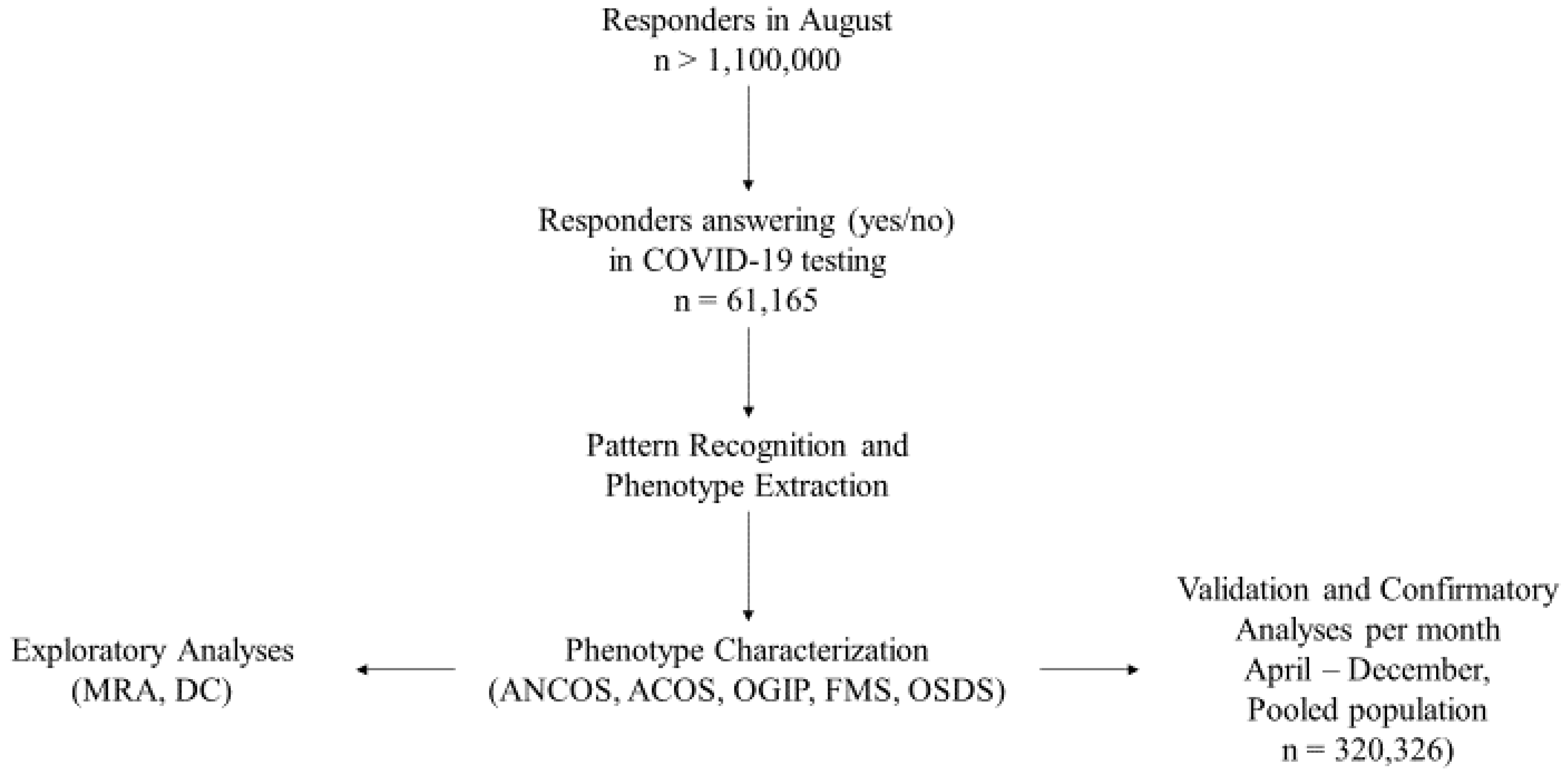
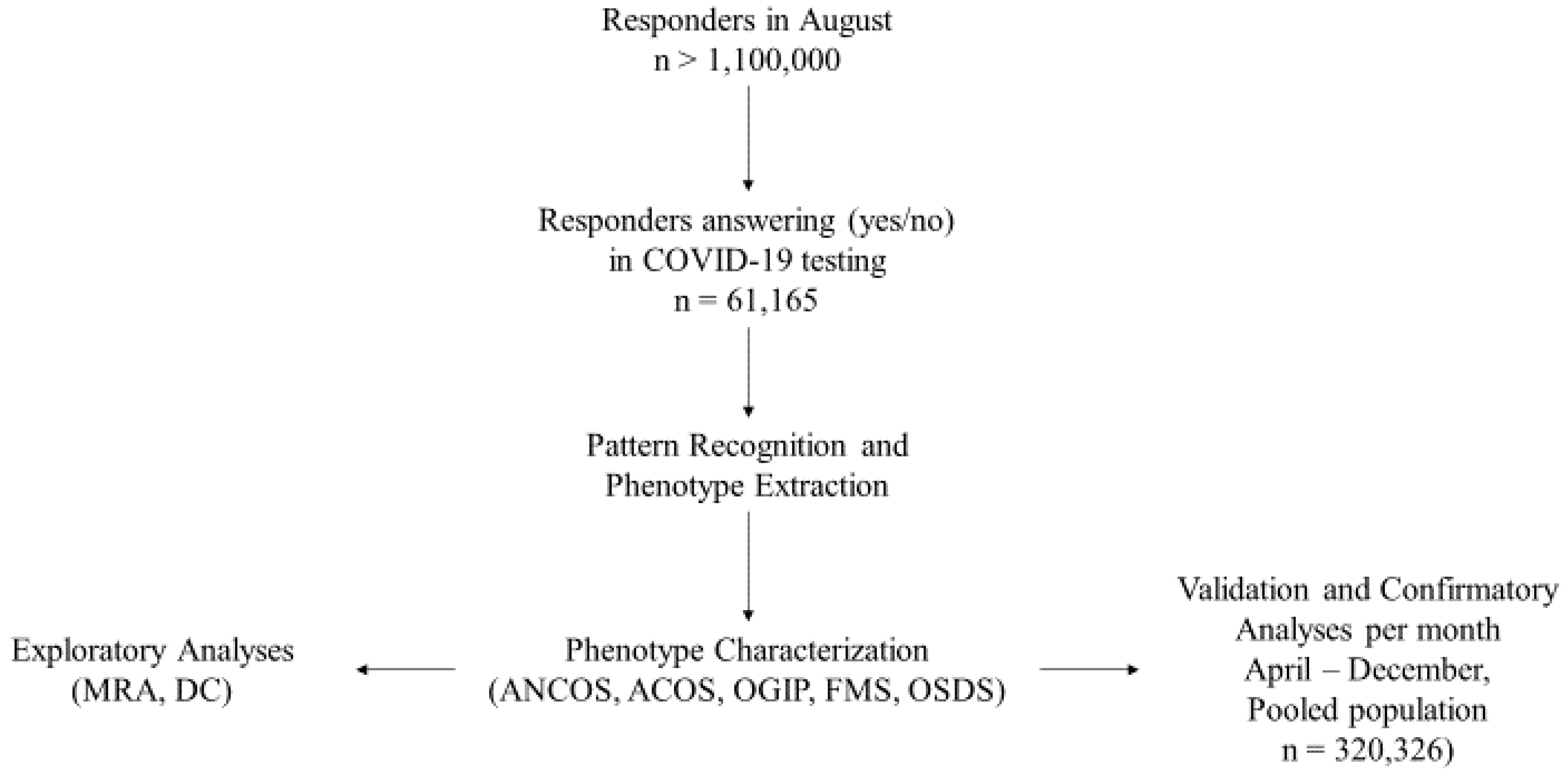
2.2. Study Design
2.3. Statistical Analysis
Pattern Recognition via Multiple Correspondence Analysis
2.4. Two-Step Clustering and Phenotype Extraction
2.5. Phenotype Validation: Cross-Sectional and Longitudinal Aspects
- (a)
- The weights extracted from August’s responders were applied to an MCA based on symptom data recorded for each subsequent and preceding month’s responders.
- (b)
- Object scores were calculated for each responder.
- (c)
- Object scores and symptom duration per month were used in TSC.
2.6. Crossectional Validation: Phenotypes vs. Controls
2.7. Longitudinal Validation: Phenotype Re-Emergence and Symptom Invariance
2.8. Post-Hoc Analyses
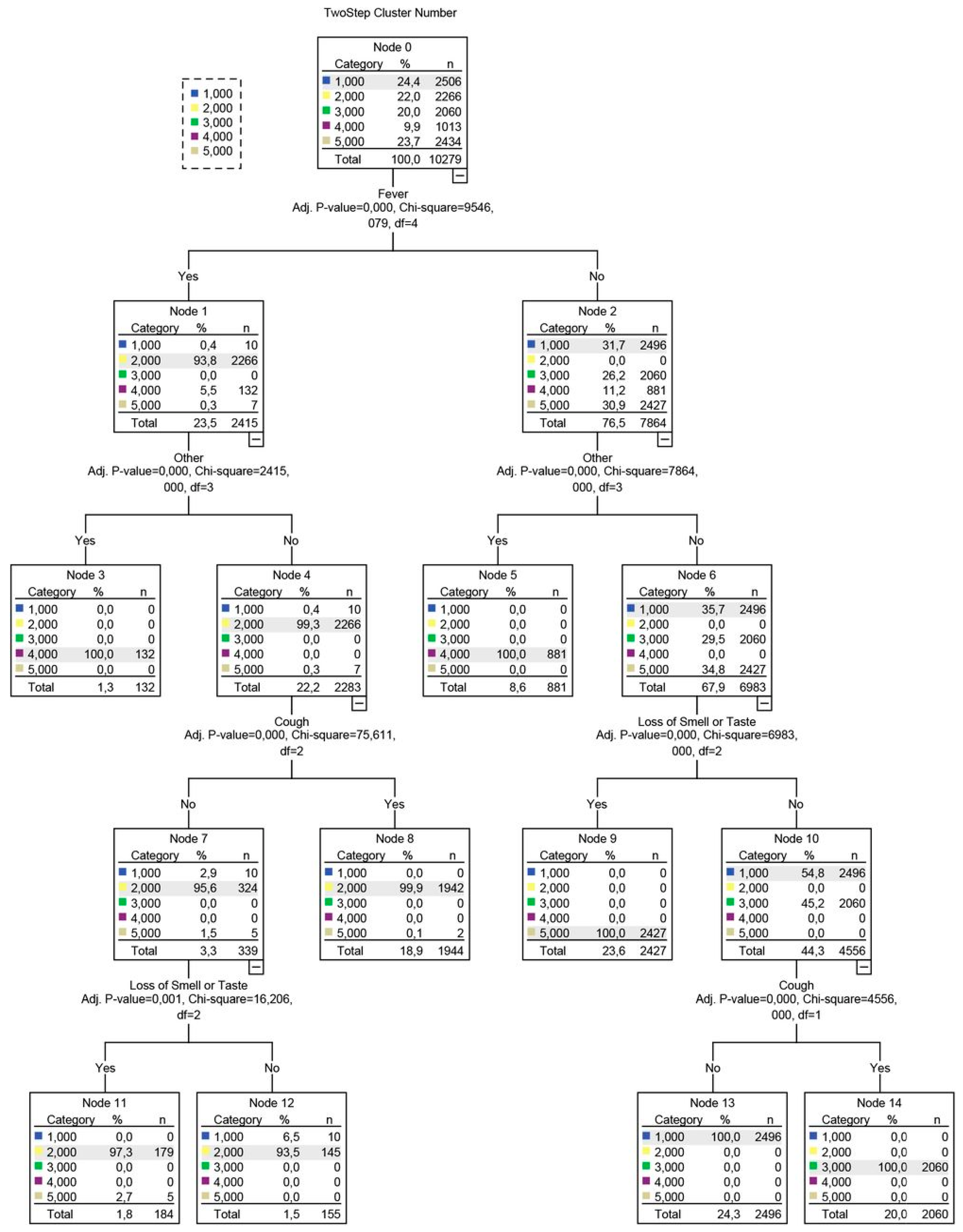
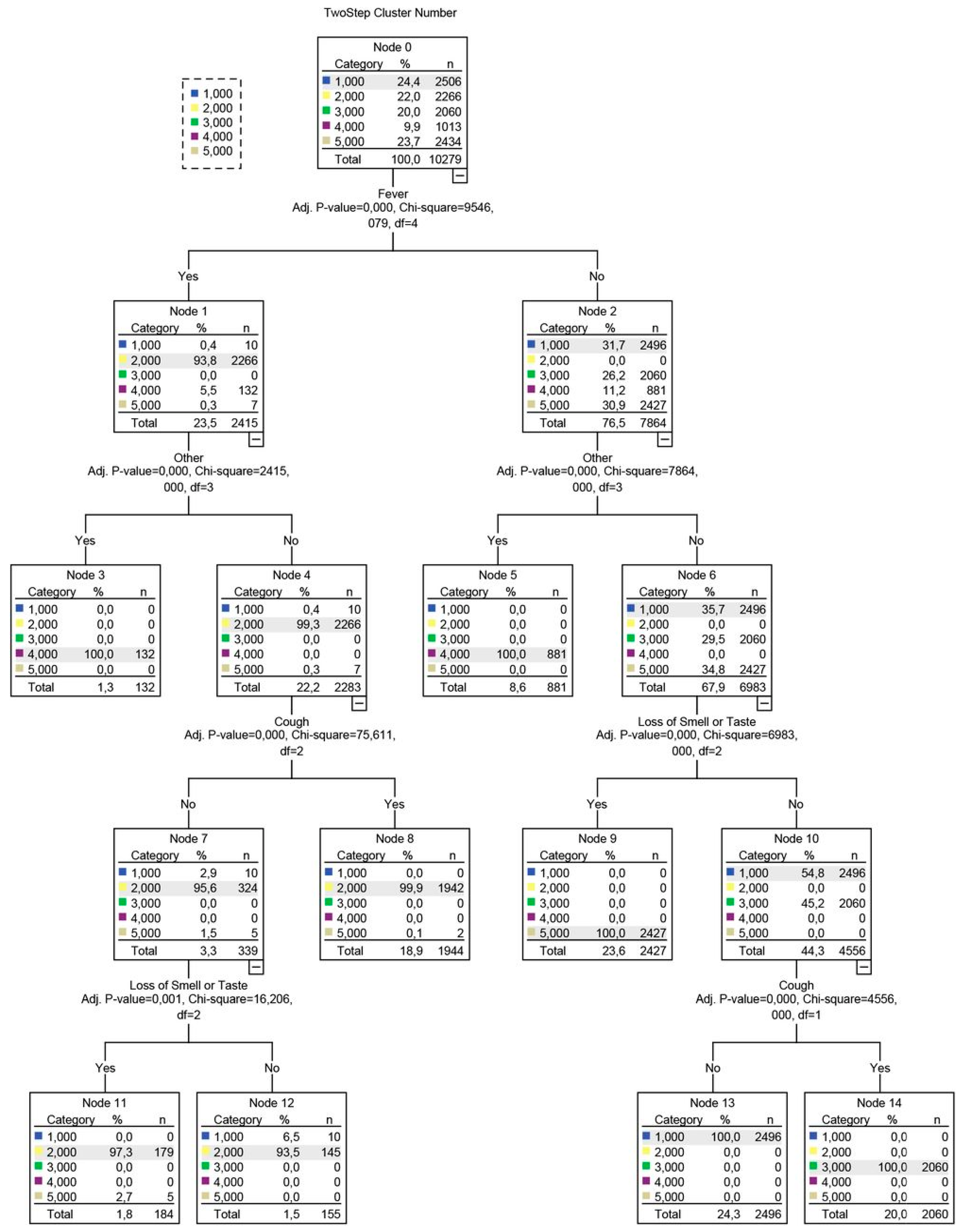
2.9. Determination of Data-Driven Diagnostic Rules via Decision Tree Analyses
3. Results
3.1. Study Population
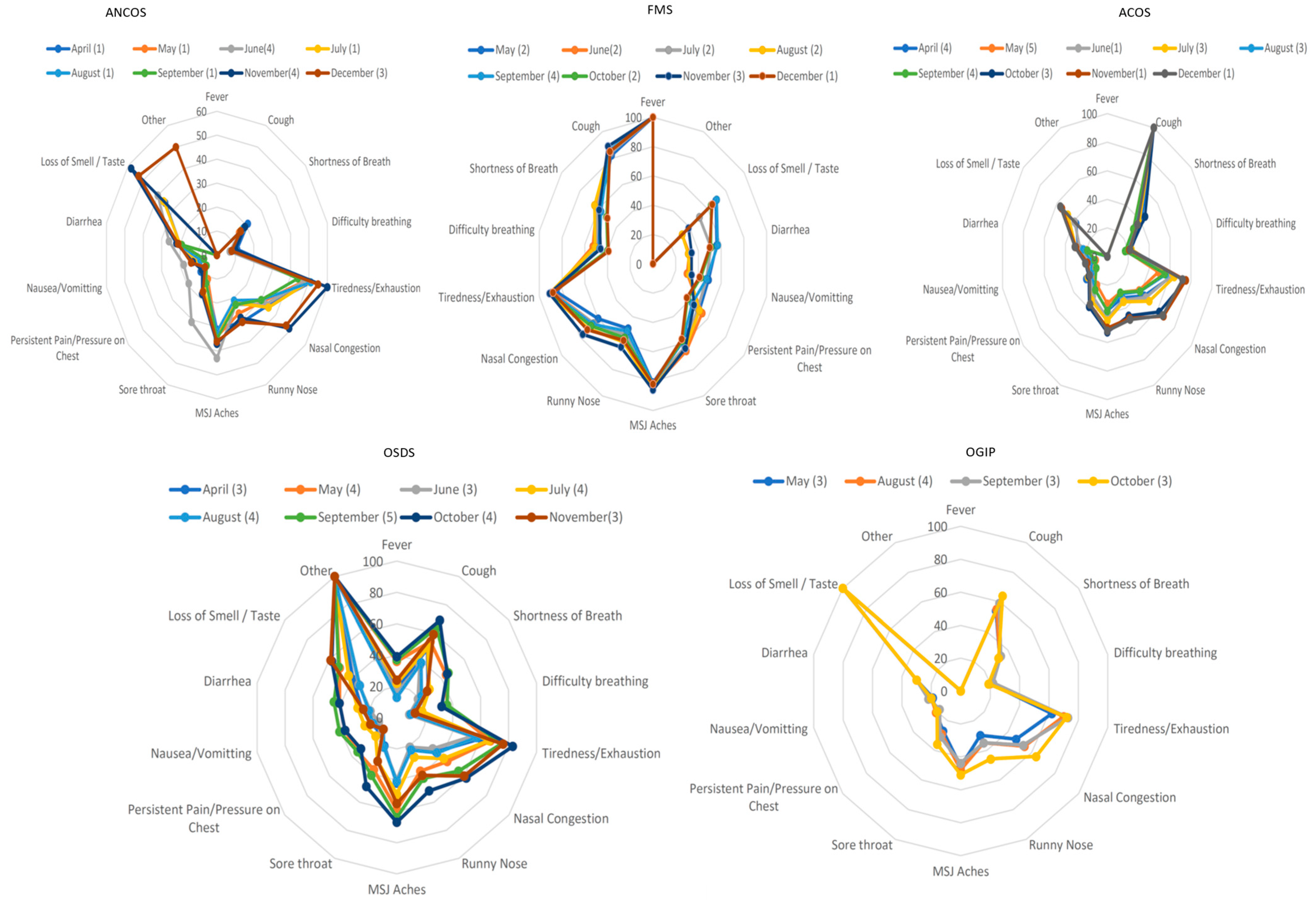
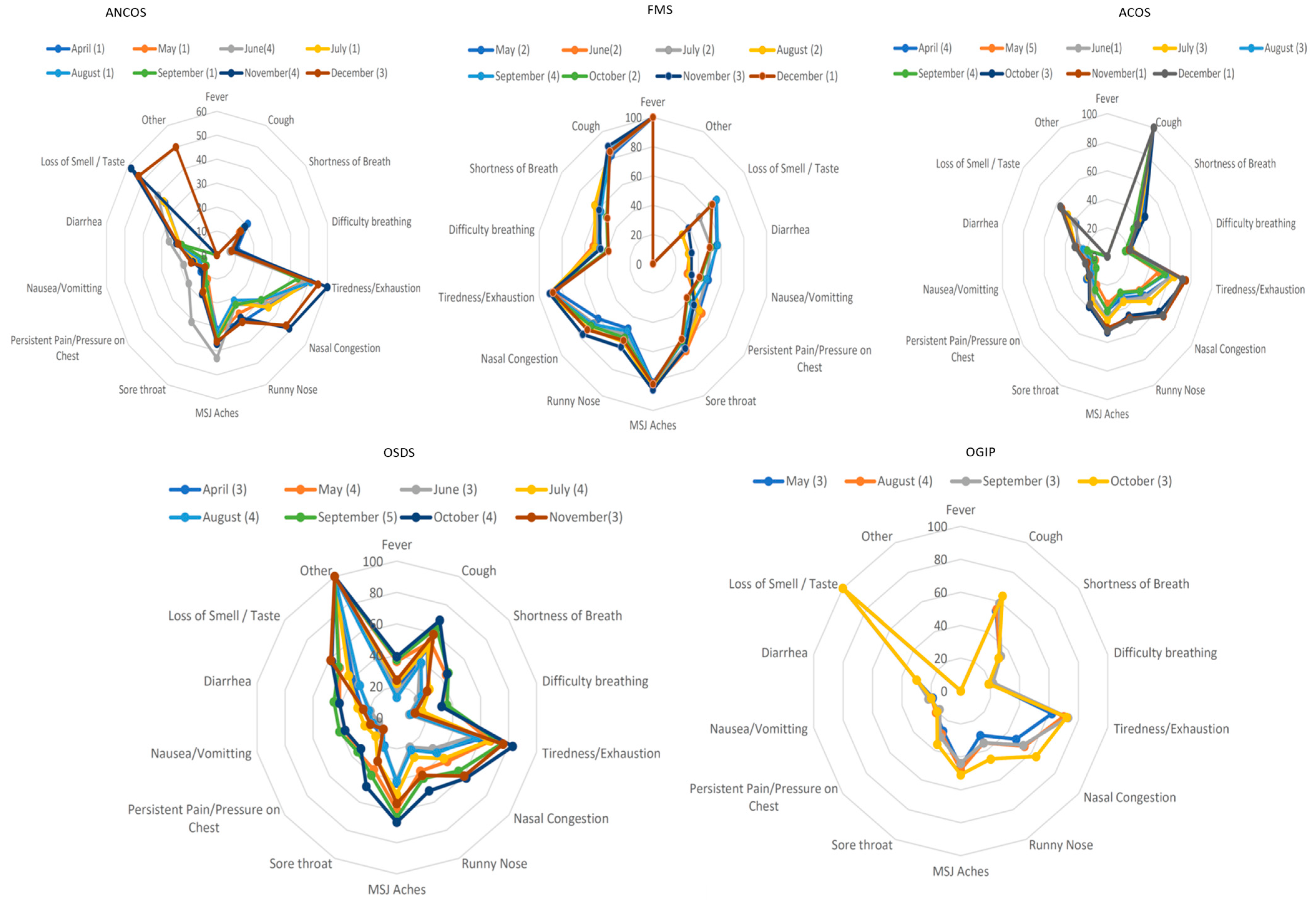
3.2. Phenotype Extraction
- Afebrile (0%), Non-Coughing (0%), Oligosymptomatic (ANCOS).
- Febrile (100%) Multisymptomatic (FMS).
- Afebrile (0%) Coughing (100%) Oligosymptomatic (ACOS).
- Oligosymptomatic with additional self-described symptoms (100%; OSDS).
- Olfaction/Gustatory Impairment Predominant (100%; OGIP).
- (a)
- ANCOS and OSDS emerged in 10/10 months
- (b)
- MFS and ACOS emerged in 9/10 months
- (c)
- OGIP emerged in 4/10 months.
- (a)
- ANCOS was characterized by general malaise in the absence of fever and upper respiratory tract symptoms.
- (b)
- ACOS was characterized as a mainly afebrile upper respiratory tract viral infection.
- (c)
- FMS was a more typical, febrile syndrome covering respiratory and gastrointestinal (GI) manifestations.
- (d)
- OGIP, the most invariant syndrome, was characterized by the absence of fever and diarrhea.
- (e)
- OSDS did not typically include symptoms of pain or pressure on the chest, nor difficulty in breathing.
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lai, C.C.; Ko, W.C.; Lee, P.I.; Jean, S.S.; Hsueh, P.R. Extra-respiratory manifestations of COVID-19. Int. J. Antimicrob. Agents 2020, 56, 106024. [Google Scholar] [CrossRef] [PubMed]
- Cherian, R.; Chandra, B.; Tung, M.L.; Vuylsteke, A. COVID-19 conundrum: Clinical phenotyping based on pathophysiology as a promising approach to guide therapy in a novel illness. Eur. Respir. J. 2020, 56, 2002135. [Google Scholar] [CrossRef] [PubMed]
- Vavougios, G.D.; George, D.G.; Pastaka, C.; Zarogiannis, S.G.; Gourgoulianis, K.I. Phenotypes of comorbidity in OSAS patients: Combining categorical principal component analysis with cluster analysis. J. Sleep Res. 2016, 25, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Zinchuk, A.V.; Gentry, M.J.; Concato, J.; Yaggi, H.K. Phenotypes in obstructive sleep apnea: A definition, examples and evolution of approaches. Sleep Med. Rev. 2017, 35, 113–123. [Google Scholar] [CrossRef]
- Lim, D.C.; Sutherland, K.; Cistulli, P.A.; Pack, A.I. P4 medicine approach to obstructive sleep apnoea. Respirology 2017, 22, 849–860. [Google Scholar] [CrossRef] [Green Version]
- Mihaicuta, S.; Udrescu, M.; Topirceanu, A.; Udrescu, L. Network science meets respiratory medicine for OSAS phenotyping and severity prediction. PeerJ 2017, 5, e3289. [Google Scholar] [CrossRef] [Green Version]
- Crawford, M.R.; Chirinos, D.A.; Iurcotta, T.; Edinger, J.D.; Wyatt, J.K.; Manber, R.; Ong, J.C. Characterization of Patients Who Present with Insomnia: Is There Room for a Symptom Cluster-Based Approach? J. Clin. Sleep Med. 2017, 13, 911–921. [Google Scholar] [CrossRef] [Green Version]
- Scarlata, S.; Pennazza, G.; Santonico, M.; Santangelo, S.; Rossi Bartoli, I.; Rivera, C.; Vernile, C.; De Vincentis, A.; Antonelli Incalzi, R. Screening of Obstructive Sleep Apnea Syndrome by Electronic-Nose Analysis of Volatile Organic Compounds. Sci. Rep. 2017, 7, 11938. [Google Scholar] [CrossRef] [Green Version]
- Vavougios, G.D.; Doskas, T.; Kormas, C.; Krogfelt, K.A.; Zarogiannis, S.G.; Stefanis, L. Identification of a prospective early motor progression cluster of Parkinson’s disease: Data from the PPMI study. J. Neurol. Sci. 2018, 387, 103–108. [Google Scholar] [CrossRef]
- Reategui, R.; Ratte, S.; Bautista-Valarezo, E.; Duque, V. Cluster Analysis of Obesity Disease Based on Comorbidities Extracted from Clinical Notes. J. Med. Syst. 2019, 43, 52. [Google Scholar] [CrossRef]
- Zinchuk, A.; Yaggi, H.K. Phenotypic Subtypes of OSA: A Challenge and Opportunity for Precision Medicine. Chest 2020, 157, 403–420. [Google Scholar] [CrossRef]
- Martins, T.D.; Annichino-Bizzacchi, J.M.; Romano, A.V.C.; Filho, R.M. Principal Component Analysis on Recurrent Venous Thromboembolism. Clin. Appl. Thromb. Hemost. 2019, 25, 1076029619895323. [Google Scholar] [CrossRef]
- Shoji, T.; Sato, N.; Fukuda, H.; Muraki, Y.; Kawata, K.; Akazawa, M. Clinical Implication of the Relationship between Antimicrobial Resistance and Infection Control Activities in Japanese Hospitals: A Principal Component Analysis-Based Cluster Analysis. Antibiotics 2022, 11, 229. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Kim, S.S.; Lindsell, C.J.; Rose, E.B.; Shapiro, N.I.; Files, D.C.; Gibbs, K.W.; Erickson, H.L.; Steingrub, J.S.; Smithline, H.A.; et al. Symptom Duration and Risk Factors for Delayed Return to Usual Health Among Outpatients with COVID-19 in a Multistate Health Care Systems Network—United States, March–June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 993–998. [Google Scholar] [CrossRef]
- Costa, P.S.; Santos, N.C.; Cunha, P.; Cotter, J.; Sousa, N. The Use of Multiple Correspondence Analysis to Explore Associations between Categories of Qualitative Variables in Healthy Ageing. J. Aging Res. 2013, 2013, 302163. [Google Scholar] [CrossRef]
- Van Horn, A.; Weitz, C.A.; Olszowy, K.M.; Dancause, K.N.; Sun, C.; Pomer, A.; Silverman, H.; Lee, G.; Tarivonda, L.; Chan, C.W.; et al. Using multiple correspondence analysis to identify behaviour patterns associated with overweight and obesity in Vanuatu adults. Public Health Nutr. 2019, 22, 1533–1544. [Google Scholar] [CrossRef]
- Benassi, M.; Garofalo, S.; Ambrosini, F.; Sant’Angelo, R.P.; Raggini, R.; De Paoli, G.; Ravani, C.; Giovagnoli, S.; Orsoni, M.; Piraccini, G. Using Two-Step Cluster Analysis and Latent Class Cluster Analysis to Classify the Cognitive Heterogeneity of Cross-Diagnostic Psychiatric Inpatients. Front. Psychol. 2020, 11, 1085. [Google Scholar] [CrossRef]
- Song, Y.Y.; Lu, Y. Decision tree methods: Applications for classification and prediction. Shanghai Arch. Psychiatry 2015, 27, 130–135. [Google Scholar]
- Girard, C.I.; Warren, C.E.; Romanchuk, N.J.; Del Bel, M.J.; Carsen, S.; Chan, A.D.; Benoit, D.L. Decision Tree Learning Algorithm for Classifying Knee Injury Status Using Return-to-Activity Criteria. In Proceedings of the 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society, Montreal, QC, Canada, 20–24 July 2020; Volume 2020, pp. 5494–5497. [Google Scholar]
- Ramezankhani, A.; Hadavandi, E.; Pournik, O.; Shahrabi, J.; Azizi, F.; Hadaegh, F. Decision tree-based modelling for identification of potential interactions between type 2 diabetes risk factors: A decade follow-up in a Middle East prospective cohort study. BMJ Open 2016, 6, e013336. [Google Scholar] [CrossRef]
- Venkatasubramaniam, A.; Wolfson, J.; Mitchell, N.; Barnes, T.; JaKa, M.; French, S. Decision trees in epidemiological research. Emerg. Themes Epidemiol. 2017, 14, 11. [Google Scholar] [CrossRef]
- Loh, W.; Shih, Y. Split selection methods for classification trees. Stat. Sin. 1997, 7, 815–840. [Google Scholar]
- Jain, A.; Doyle, D.J. Stages or phenotypes? A critical look at COVID-19 pathophysiology. Intensive Care Med. 2020, 46, 1494–1495. [Google Scholar] [CrossRef]
- Voutouri, C.; Nikmaneshi, M.R.; Hardin, C.C.; Patel, A.B.; Verma, A.; Khandekar, M.J.; Dutta, S.; Stylianopoulos, T.; Munn, L.L.; Jain, R.K. In silico dynamics of COVID-19 phenotypes for optimizing clinical management. Proc. Natl. Acad. Sci. USA 2021, 118, e2021642118. [Google Scholar] [CrossRef]
- Rello, J.; Storti, E.; Belliato, M.; Serrano, R. Clinical phenotypes of SARS-CoV-2: Implications for clinicians and researchers. Eur. Respir. J. 2020, 55, 2001028. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.S.; Richey, E.A.; Brunetto, W.L. A Symptom-Based Rule for Diagnosis of COVID-19. SN Compr. Clin. Med. 2020, 2, 1947–1954. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.T.; Wei, F.X. Primary stratification and identification of suspected Corona virus disease 2019 (COVID-19) from clinical perspective by a simple scoring proposal. Mil. Med. Res. 2020, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Bello-Chavolla, O.Y.; Antonio-Villa, N.E.; Vargas-Vazquez, A.; Fermin-Martinez, C.A.; Marquez-Salinas, A.; Bahena-Lopez, J.P. Profiling cases with non-respiratory symptoms and asymptomatic SARS-CoV-2 infections in Mexico City. Clin. Infect. Dis. 2020, 72, e655–e658. [Google Scholar] [CrossRef] [PubMed]
- Muniyappa, R.; Gubbi, S. COVID-19 pandemic, coronaviruses, and diabetes mellitus. Am. J. Physiol. Endocrinol. Metab. 2020, 318, E736–E741. [Google Scholar] [CrossRef] [Green Version]
- Bansal, M. Cardiovascular disease and COVID-19. Diabetes Metab. Syndr. 2020, 14, 247–250. [Google Scholar] [CrossRef]
- Hughes-Visentin, A.; Paul, A.B.M. Asthma and COVID-19: What do we know now. Clin. Med. Insights Circ. Respir. Pulm. Med. 2020, 14, 1179548420966242. [Google Scholar] [CrossRef]
- Higham, A.; Mathioudakis, A.; Vestbo, J.; Singh, D. COVID-19 and COPD: A narrative review of the basic science and clinical outcomes. Eur. Respir. Rev. 2020, 29, 200199. [Google Scholar] [CrossRef]
- Peters, M.C.; Sajuthi, S.; Deford, P.; Christenson, S.; Rios, C.L.; Montgomery, M.T.; Woodruff, P.G.; Mauger, D.T.; Erzurum, S.C.; Johansson, M.W.; et al. COVID-19-related Genes in Sputum Cells in Asthma. Relationship to Demographic Features and Corticosteroids. Am. J. Respir. Crit. Care Med. 2020, 202, 83–90. [Google Scholar] [CrossRef]
- Hosoki, K.; Chakraborty, A.; Sur, S. Molecular mechanisms and epidemiology of COVID-19 from an allergist’s perspective. J. Allergy Clin. Immunol. 2020, 146, 285–299. [Google Scholar] [CrossRef]
- Borcherding, N.; Jethava, Y.; Vikas, P. Repurposing Anti-Cancer Drugs for COVID-19 Treatment. Drug Des. Dev. Ther. 2020, 14, 5045–5058. [Google Scholar] [CrossRef]
- Struyf, T.; Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Leeflang, M.M.; Spijker, R.; Hooft, L.; Emperador, D.; Domen, J.; et al. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19 disease. Cochrane Database Syst. Rev. 2020, 7, CD013665. [Google Scholar]
- Friedman, B.W.; Grosberg, B.M. Diagnosis and management of the primary headache disorders in the emergency department setting. Emerg. Med. Clin. N. Am. 2009, 27, 71–87. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| April (n = 22,320) | May (n = 38,043) | June (n = 51,582) | July (n = 78,951) | August (n = 66,155) | September (n = 12,801) | October (n = 19,137) | November (n = 22,698) | December (n = 48,629) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| COVID-19 | 4000 | 4955 | 6573 | 13,370 | 10,279 | 1773 | 5936 | 10,026 | 21,617 | |
| Age Group | 18–24 | 1783 | 2973 | 4202 | 7047 | 5965 | 1194 | 1211 | 1606 | 3312 |
| 25–34 | 4856 | 7423 | 9837 | 15,559 | 12,158 | 2204 | 3353 | 4805 | 9002 | |
| 35–44 | 4794 | 7249 | 8919 | 14,450 | 11,502 | 2116 | 3886 | 4856 | 9529 | |
| 45–54 | 4281 | 7030 | 8886 | 13,660 | 11,146 | 2119 | 3519 | 4095 | 8809 | |
| 55–64 | 3220 | 6235 | 8661 | 12,385 | 10,775 | 2173 | 3320 | 3227 | 7440 | |
| 65–74 | 1447 | 3597 | 5655 | 7791 | 7218 | 1483 | 1808 | 1539 | 3907 | |
| >75 | 312 | 907 | 1632 | 2317 | 2155 | 531 | 573 | 427 | 1181 | |
| NA | 1627 | 2629 | 3790 | 5742 | 5246 | 981 | 1467 | 2143 | 5449 | |
| Gender | M | 5001 | 9754 | 13,230 | 20,313 | 17,427 | 3434 | 4555 | 4752 | 10,684 |
| F | 15,459 | 24,985 | 33,672 | 51,556 | 42,364 | 8170 | 12,732 | 15,360 | 31,612 | |
| NB | 149 | 284 | 366 | 613 | 532 | 104 | 141 | 176 | 347 | |
| SD | 102 | 219 | 252 | 357 | 297 | 72 | 119 | 144 | 248 | |
| NA | 153 | 325 | 449 | 653 | 565 | 100 | 128 | 128 | 322 | |
| N/A | 1456 | 2486 | 3613 | 5459 | 4980 | 921 | 1462 | 2138 | 5416 | |
| Cancer | 1223 | 2338 | 3209 | 4353 | 3783 | 816 | 1082 | 1040 | 2289 | |
| HD | 6556 | 7768 | 8450 | 13,352 | 10,792 | 2036 | 4738 | 6213 | 12,229 | |
| HTN | 3952 | 4682 | 5129 | 8263 | 6486 | 1302 | 2979 | 3931 | 7785 | |
| Asthma | 12,222 | 19,035 | 24,962 | 38,645 | 32,205 | 6031 | 11,461 | 14,309 | 28,597 | |
| CLD | 9361 | 14,946 | 19,201 | 30,197 | 25,728 | 5141 | 9644 | 12,504 | 25,272 | |
| KD | 8035 | 12,264 | 14,668 | 22,830 | 19,393 | 3907 | 8203 | 10,029 | 20,615 | |
| AD | 8807 | 14,702 | 19,365 | 28,438 | 23,692 | 4587 | 8450 | 10,533 | 21,677 | |
| Diabetes | T1D | 4817 | 8313 | 9950 | 17,181 | 12,822 | 2627 | 5102 | 5565 | 12,807 |
| T2D | 4202 | 4397 | 4556 | 7698 | 5899 | 1110 | 2803 | 3933 | 7743 | |
| IC | 3091 | 5150 | 5847 | 10,235 | 7325 | 14755 | 3519 | 4087 | 9238 |
| N | AUC | p-Value | 95% CI | |
|---|---|---|---|---|
| ANCOS (1) | 2506 | <0.5 | NA | NA |
| FMS (2) | 2266 | 0.963 | <0.001 | 0.961–0.965 |
| ACOS (3) | 2060 | 0.737 | <0.001 | 0.729–0.746 |
| OSDS (4) | 1013 | 0.777 | <0.001 | 0.762–0.792 |
| OGIP (5) | 2434 | 0.983 | <0.001 | 0.982–0.984 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vavougios, G.D.; Stavrou, V.T.; Konstantatos, C.; Sinigalias, P.-C.; Zarogiannis, S.G.; Kolomvatsos, K.; Stamoulis, G.; Gourgoulianis, K.I. COVID-19 Phenotypes and Comorbidity: A Data-Driven, Pattern Recognition Approach Using National Representative Data from the United States. Int. J. Environ. Res. Public Health 2022, 19, 4630. https://doi.org/10.3390/ijerph19084630
Vavougios GD, Stavrou VT, Konstantatos C, Sinigalias P-C, Zarogiannis SG, Kolomvatsos K, Stamoulis G, Gourgoulianis KI. COVID-19 Phenotypes and Comorbidity: A Data-Driven, Pattern Recognition Approach Using National Representative Data from the United States. International Journal of Environmental Research and Public Health. 2022; 19(8):4630. https://doi.org/10.3390/ijerph19084630
Chicago/Turabian StyleVavougios, George D., Vasileios T. Stavrou, Christoforos Konstantatos, Pavlos-Christoforos Sinigalias, Sotirios G. Zarogiannis, Konstantinos Kolomvatsos, George Stamoulis, and Konstantinos I. Gourgoulianis. 2022. "COVID-19 Phenotypes and Comorbidity: A Data-Driven, Pattern Recognition Approach Using National Representative Data from the United States" International Journal of Environmental Research and Public Health 19, no. 8: 4630. https://doi.org/10.3390/ijerph19084630