

Dietary Isorhamnetin Intake Is Inversely Associated with Coronary Artery Disease Occurrence in Polish Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of the Food Frequency Questionnaire
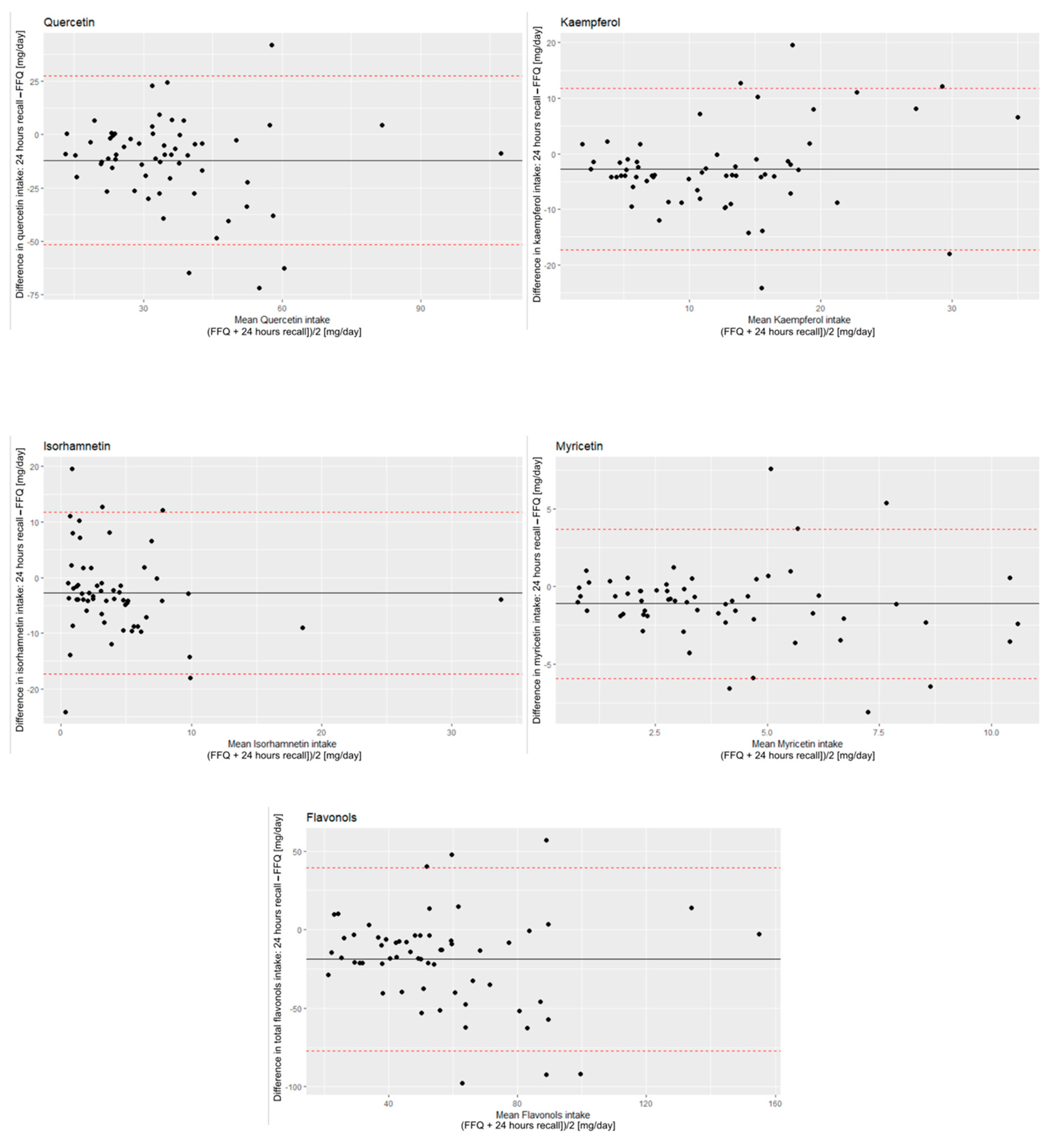
2.2. Validation Procedure
2.3. Reproducibility
2.4. Flavonol Intake Assessment in CAD Patients
2.5. Ethical Standards
3. Results
4. Discussion
5. Limitations of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Czapla, M.; Juárez-Vela, R.; Łokieć, K.; Wleklik, M.; Karniej, P.; Smereka, J. The Association between Nutritional Status and Length of Hospital Stay among Patients with Hypertension. Int. J. Environ. Res. Public Health 2022, 19, 5827. [Google Scholar] [CrossRef] [PubMed]
- Czapla, M.; Karniej, P.; Juárez-Vela, R.; Łokieć, K. The association between nutritional status and in-hospital mortality among patients with acute coronary syndrome—a result of the retrospective nutritional status heart study (Nshs). Nutrients 2020, 12, 3091. [Google Scholar] [CrossRef] [PubMed]
- Yue, Y.; Petimar, J.; Willett, W.C.; Smith-Warner, S.A.; Yuan, C.; Rosato, S.; Sampson, L.; Rosner, B.; Cassidy, A.; Rimm, E.B.; et al. Dietary flavonoids and flavonoid-rich foods: Validity and reproducibility of FFQ-derived intake estimates. Public Health Nutr. 2020, 23, 3295–3303. [Google Scholar] [CrossRef] [PubMed]
- Galván-Portillo, M.; Vázquez-Salas, R.A.; Hernández-Pérez, J.G.; Blanco-Muñoz, J.; López-Carrillo, L.; Torres-Sánchez, L. Dietary flavonoid patterns and prostate cancer: Evidence from a Mexican population-based case-control study. Br. J. Nutr. 2022, 127, 1695–1703. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, V.; Zanolin, M.E.; Cazzoletti, L.; Bono, R.; Cerveri, I.; Ferrari, M.; Pirina, P.; Garcia-Larsen, V. Dietary flavonoids and respiratory diseases: A population-based multi-case-control study in Italian adults. Public Health Nutr. 2020, 23, 2548–2556. [Google Scholar] [CrossRef]
- Chekalina, N.; Burmak, Y.; Petrov, Y.; Borisova, Z.; Manusha, Y.; Kazakov, Y.; Kaidashev, I. Quercetin reduces the transcriptional activity of NF-kB in stable coronary artery disease. Indian Heart J. 2018, 70, 593–597. [Google Scholar] [CrossRef]
- Suri, S.; Liu, X.H.; Rayment, S.; Hughes, D.A.; Kroon, P.A.; Needs, P.W.; Taylor, M.A.; Tribolo, S.; Wilson, V.G. Quercetin and its major metabolites selectively modulate cyclic GMP-dependent relaxations and associated tolerance in pig isolated coronary artery. Br. J. Pharmacol. 2010, 159, 566–575. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Zhang, X.; Li, D.; Hao, W.; Meng, F.; Wang, B.; Han, J.; Zheng, Q. Kaempferide Protects against Myocardial Ischemia/Reperfusion Injury through Activation of the PI3K/Akt/GSK-3 β Pathway. Mediat. Inflamm. 2017, 2017, 5278218. [Google Scholar] [CrossRef] [Green Version]
- Lian, T.W.; Wang, L.; Lo, Y.H.; Huang, I.J.; Wu, M.J. Fisetin, morin and myricetin attenuate CD36 expression and oxLDL uptake in U937-derived macrophages. Biochim. Biophys. Acta—Mol. Cell Biol. Lipids 2008, 1781, 601–609. [Google Scholar] [CrossRef]
- Panche, A.N.; Diwan, A.D.; Chandra, S.R. Flavonoids: An overview. J. Nutr. Sci. 2016, 5, e47. [Google Scholar] [CrossRef] [Green Version]
- Zamora-Ros, R.; Andres-Lacueva, C.; Lamuela-Raventós, R.M.; Berenguer, T.; Jakszyn, P.; Barricarte, A.; Ardanaz, E.; Amiano, P.; Dorronsoro, M.; Larrañaga, N. Estimation of Dietary Sources and Flavonoid Intake in a Spanish Adult Population (EPIC-Spain). J. Am. Diet. Assoc. 2010, 110, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Sampson, L.; Rimm, E.; Hollma, P.C.H.; de Vries, J.H.M.; Katan, M.B. Flavonol and Flavone Intakes in US Health Professionals. J. Am. Diet. Assoc. 2002, 102, 1414–1420. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Knaze, V.; Luján-Barroso, L.; Slimani, N.; Romieu, I.; Fedirko, V.; De Magistris, M.S.; Ericson, U.; Amiano, P.; Trichopoulou, A.; et al. Estimated dietary intakes of flavonols, flavanones and flavones in the European Prospective Investigation into Cancer and Nutrition (EPIC) 24 hour dietary recall cohort. Br. J. Nutr. 2011, 106, 1915–1925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassidy, A.; O’Reilly, É.J.; Kay, C.; Sampson, L.; Franz, M.; Forman, J.; Curhan, G.; Rimm, E.B. Habitual intake of flavonoid subclasses and incident hypertension in adults. Am. J. Clin. Nutr. 2011, 93, 338–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marniemi, J.; Alanen, E.; Impivaara, O.; Seppänen, R.; Hakala, P.; Rajala, T.; Rönnemaa, T. Dietary and serum vitamins and minerals as predictors of myocardial infarction and stroke in elderly subjects. Nutr. Metab. Cardiovasc. Dis. 2005, 15, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Marrero, A.D.; Quesada, A.R.; Martínez-Poveda, B.; Medina, M.Á. Antiangiogenic Phytochemicals Constituent of Diet as Promising Candidates for Chemoprevention of Cancer. Antioxidants 2022, 11, 302. [Google Scholar] [CrossRef]
- Popiolek-Kalisz, J.; Fornal, E. The Impact of Flavonols on Cardiovascular Risk. Nutrients 2022, 14, 1973. [Google Scholar] [CrossRef]
- Martin, M.A.; Goya, L.; Ramos, S. Protective effects of tea, red wine and cocoa in diabetes. Evidences from human studies. Food Chem. Toxicol. 2017, 109, 302–314. [Google Scholar] [CrossRef] [Green Version]
- Popiolek-Kalisz, J.; Fornal, E. The Effects of Quercetin Supplementation on Blood Pressure—Meta-Analysis. Curr. Probl. Cardiol. 2022, 47, 101350. [Google Scholar] [CrossRef]
- Taguchi, C.; Kishimoto, Y.; Kondo, K. Validation of Food-Frequency Questionnaires for Polyphenol Intake in Japanese Adults. J. Nutr. Sci. Vitaminol. 2021, 67, 72–75. [Google Scholar] [CrossRef]
- Hercberg, S.; Galan, P.; Preziosi, P.; Bertrais, S.; Mennen, L.; Malvy, D.; Roussel, A.M.; Favier, A.; Briançon, S. The SU.VI.MAX study: A randomized, placebo-controlled trial of the health effects of antioxidant vitamins and minerals. Arch. Intern. Med. 2004, 164, 2335–2342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhagwat, S.; Haytowitz, D.B.; Holden, J.M. USDA Database for the Flavonoid Content of Selected Foods. Release 3; U.S. Department of Agriculture: Beltsville, MD, USA, 2011. [Google Scholar]
- Yu, A.D.; Mumme, K.D.; Conlon, C.A.; von Hurst, P.R.; Gillies, N.; Heath, A.L.; Coad, J.; Beck, K.L. Relative Validity and Reproducibility of a Semi-Quantitative Food Frequency Questionnaire for Determining Nutrient Intake in Older Adults in New Zealand: The REACH Study. Nutrients 2022, 14, 519. [Google Scholar] [CrossRef] [PubMed]
- Martin Bland, J.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Watson, J.F.; Collins, C.E.; Sibbritt, D.W.; Dibley, M.J.; Garg, M.L. Reproducibility and comparative validity of a food frequency questionnaire for Australian children and adolescents. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 62. [Google Scholar] [CrossRef] [Green Version]
- Palacios, C.; Trak, M.A.; Betancourt, J.; Joshipura, K.; Tucker, K.L. Validation and reproducibility of a semi-quantitative FFQ as a measure of dietary intake in adults from Puerto Rico. Public Health Nutr. 2015, 18, 2550–2558. [Google Scholar] [CrossRef]
- Sadeghi, S.; Montazeri, V.; Zamora-Ros, R.; Biparva, P.; Sabour, S.; Pirouzpanah, S. Food frequency questionnaire is a valid assessment tool of quercetin and kaempferol intake in Iranian breast cancer patients according to plasma biomarkers. Nutr. Res. 2021, 93, 1–14. [Google Scholar] [CrossRef]
- Somerset, S.; Papier, K. A Food Frequency Questionnaire Validated for Estimating Dietary Flavonoid Intake in an Australian Population. Nutr. Cancer 2014, 66, 1200–1210. [Google Scholar] [CrossRef]
- Block, G.; Hartman, A.M.; Dresser, C.M.; Carroll, M.D.; Gannon, J.; Gardner, L. A data-based approach to diet questionnaire design and testing. Am. J. Epidemiol. 1986, 124, 453–469. [Google Scholar] [CrossRef]
- Christensen, K.Y.; Naidu, A.; Parent, M.-É.; Pintos, J.; Abrahamowicz, M.; Siemiatycki, J.; Koushik, A. The Risk of Lung Cancer Related to Dietary Intake of Flavonoids. Nutr. Cancer 2012, 64, 964–974. [Google Scholar] [CrossRef] [Green Version]
- Woo, H.D.; Kim, J. Dietary Flavonoid Intake and Smoking-Related Cancer Risk: A Meta-Analysis. PLoS ONE 2013, 8, e75604. [Google Scholar] [CrossRef] [Green Version]
- Hafizah, Y.N.; Ang, L.C.; Yap, F.; Najwa, W.N.; Cheah, W.L.; Ruzita, A.T.; Jumuddin, F.A.; Koh, D.; Lee, J.A.C.; Essau, C.A.; et al. Validity and reliability of a food frequency questionnaire (FFQ) to assess dietary intake of preschool children. Int. J. Environ. Res. Public Health 2019, 16, 4722. [Google Scholar] [CrossRef] [Green Version]
- Jarvinen, R.; Seppanen, R.; Paul, K. Short-Term and Long-Term Reproducibility of Dietary History Interview Data. Int. J. Epidemiol. 1993, 22, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Graubard, B.; Ioannidis, J.P.A. Use and reporting of Bland–Altman analyses in studies of self-reported versus measured weight and height. Int. J. Obes. 2020, 44, 1311–1318. [Google Scholar] [CrossRef] [PubMed]
- Pursey, K.; Burrows, T.L.; Stanwell, P.; Collins, C.E. How accurate is web-based self-reported height, weight, and body mass index in young adults. J. Med. Internet Res. 2014, 16, e2909. [Google Scholar] [CrossRef] [PubMed]
- Powell-Young, Y.M. The validity of self-report weight and height as a surrogate method for direct measurement. Appl. Nurs. Res. 2012, 25, 25–30. [Google Scholar] [CrossRef] [Green Version]
- Yoong, S.L.; Carey, M.L.; D’Este, C.; Sanson-Fisher, R.W. Agreement between self-reported and measured weight and height collected in general practice patients: A prospective study. BMC Med. Res. Methodol. 2013, 13, 38. [Google Scholar] [CrossRef] [Green Version]
- Pasalich, M.; Lee, A.H.; Burke, L.; Jancey, J.; Howat, P. Accuracy of self-reported anthropometric measures in older Australian adults. Australas. J. Ageing 2014, 33, E27–E32. [Google Scholar] [CrossRef]
- Menezes, R.; Rodriguez-Mateos, A.; Kaltsatou, A.; González-Sarrías, A.; Greyling, A.; Giannaki, C.; Andres-Lacueva, C.; Milenkovic, D.; Gibney, E.R.; Dumont, J.; et al. Impact of flavonols on cardiometabolic biomarkers: A meta-analysis of randomized controlled human trials to explore the role of inter-individual variability. Nutrients 2017, 9, 117. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; He, H.; Liu, Z.; Liu, D.; Yin, D.; He, M. Protective Effects of Isorhamnetin on Cardiomyocytes Against Anoxia/Reoxygenation-induced Injury Is Mediated by SIRT1. J. Cardiovasc. Pharmacol. 2016, 67, 526–537. [Google Scholar] [CrossRef]
- Zhang, N.; Pei, F.; Wei, H.; Zhang, T.; Yang, C.; Ma, G.; Yang, C. Isorhamnetin protects rat ventricular myocytes from ischemia and reperfusion injury. Exp. Toxicol. Pathol. 2011, 63, 33–38. [Google Scholar] [CrossRef]
- Xu, Y.; Tang, C.; Tan, S.; Duan, J.; Tian, H.; Yang, Y. Cardioprotective effect of isorhamnetin against myocardial ischemia reperfusion (I/R) injury in isolated rat heart through attenuation of apoptosis. J. Cell. Mol. Med. 2020, 24, 6253–6262. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Mean Daily Intake [mg/Day] | Mean from 24 h Recall | SD | Mean from FFQ | SD | 95% CI | R | p | Paired t-Test |
|---|---|---|---|---|---|---|---|---|
| Total flavonols | 46.86 | ±38.36 | 65.72 | ±31.38 | 0.285–0.671 | 0.50 | <0.001 | <0.001 |
| Quercetin | 29.72 | ±17.77 | 41.82 | ±20.39 | 0.224–0.633 | 0.45 | <0.001 | <0.001 |
| Kaempferol | 10.82 | ±8.74 | 13.59 | ±7.37 | 0.388–0.730 | 0.58 | <0.001 | 0.01 |
| Isorhamnetin | 2.83 | ±3.64 | 5.72 | ±7.65 | 0.292–0.675 | 0.51 | <0.001 | 0.001 |
| Myricetin | 3.45 | ±2.59 | 4.58 | ±2.96 | 0.428–0.751 | 0.61 | <0.001 | 0.001 |
| Mean Daily Intake (24 h vs. FFQ) | Percentage in the Same Quartile | Percent in the Opposite Quartile | κ |
|---|---|---|---|
| Total flavonols | 46.67% | 5.00% | 0.41 |
| Quercetin | 43.33% | 6.67% | 0.33 |
| Kaempferol | 50.00% | 1.67% | 0.55 |
| Isorhamnetin | 43.33% | 5.00% | 0.31 |
| Myricetin | 48.33% | 3.33% | 0.49 |
| Mean Daily Intake | FFQ1 | SD | FFQ2 | SD | 95 CI | R | p | Paired t-Test |
|---|---|---|---|---|---|---|---|---|
| Total flavonols [mg/day] | 72.65 | ±38.36 | 58.78 | ±28.67 | 0.610–0.842 | 0.75 | <0.001 | <0.001 |
| Quercetin [mg/day] | 46.16 | ±24.54 | 37.48 | ±18.53 | 0.668–0.868 | 0.79 | <0.001 | <0.001 |
| Kaempferol [mg/day] | 14.63 | ±8.04 | 12.55 | ±7.41 | 0.715–0.889 | 0.82 | <0.001 | 0.001 |
| Isorhamnetin [mg/day] | 6.80 | ±13.66 | 4.64 | ±4.06 | 0.029–0.500 | 0.28 | 0.03 | 0.21 |
| Myricetin [mg/day] | 5.06 | ±3.34 | 4.10 | ±2.80 | 0.763–0.909 | 0.85 | <0.001 | <0.001 |
| Fruits [portion/day] | 4.28 | ±3.86 | 3.37 | ±2.44 | 0.470–0.779 | 0.65 | <0.001 | 0.02 |
| Citrus fruits [portion/day] | 0.78 | ±0.88 | 0.57 | ±0.53 | 0.466–0.771 | 0.64 | <0.001 | 0.02 |
| Exotics fruits [portion/day] | 1.23 | ±1.77 | 0.88 | ±0.78 | 0.239–0.643 | 0.47 | <0.001 | 0.09 |
| Seed fruits [portion/day] | 0.52 | ±0.96 | 0.40 | ±0.71 | 0.818–0.932 | 0.89 | <0.001 | 0.05 |
| Local fruits [portion/day] | 0.58 | ±0.56 | 0.56 | ±0.50 | 0.658–0.864 | 0.78 | <0.001 | 0.54 |
| Berries [portion/day] | 1.07 | ±1.31 | 0.88 | ±1.05 | 0.759–0.907 | 0.85 | <0.001 | 0.04 |
| Dried fruits [portion/day] | 0.10 | ±0.18 | 0.09 | ±0.16 | 0.878–0.955 | 0.93 | <0.001 | 0.24 |
| Vegetables [portion/day] | 6.56 | ±3.54 | 5.20 | ±2.57 | 0.567–0.822 | 0.72 | <0.001 | <0.001 |
| Lettuce [portion/day] | 0.81 | ±1.30 | 0.66 | ±0.73 | 0.583–0.829 | 0.73 | <0.001 | 0.19 |
| Other leafy vegetables [portion/day] | 0.39 | ±0.86 | 0.25 | ±0.42 | 0.262–0.657 | 0.48 | <0.001 | 0.17 |
| Solanaceous vegetables [portion/day] | 2.20 | ±1.36 | 1.75 | ±1.25 | 0.672–0.870 | 0.79 | <0.001 | 0.01 |
| Roots and tubers [portion/day] | 1.12 | ±0.83 | 0.93 | ±0.66 | 0.677–0.872 | 0.79 | <0.001 | <0.001 |
| Peppers [portion/day] | 0.70 | ±0.79 | 0.56 | ±0.63 | 0.822–0.933 | 0.89 | <0.001 | 0.004 |
| Cabbage [portion/day] | 0.21 | ±0.27 | 0.18 | ±0.25 | 0.697–0.881 | 0.81 | <0.001 | 0.18 |
| Onions [portion/day] | 0.99 | ±0.83 | 0.78 | ±0.63 | 0.670–0.870 | 0.79 | <0.001 | 0.002 |
| Sprouts [portion/day] | 0.13 | ±0.32 | 0.10 | ±0.27 | 0.408–0.741 | 0.60 | <0.001 | 0.39 |
| Legumes [portion/day] | 0.33 | ±0.40 | 0.28 | ±0.36 | 0.859–0.948 | 0.91 | <0.001 | 0.03 |
| Nuts and seeds [portion/day] | 0.36 | ±0.68 | 0.22 | ±0.41 | 0.332–0.698 | 0.54 | <0.001 | 0.07 |
| Herbs and spices [portion/day] | 1.61 | ±2.04 | 1.05 | ±0.99 | 0.400–0.736 | 0.59 | <0.001 | 0.01 |
| Sauces [portion/day] | 0.40 | ±0.42 | 0.37 | ±0.37 | 0.605–0.840 | 0.74 | <0.001 | 0.35 |
| Jam and honey [portion/day] | 0.35 | ±0.40 | 0.33 | ±0.41 | 0.796–0.923 | 0.87 | <0.001 | 0.57 |
| Jam [portion/day] | 0.17 | ±0.21 | 0.16 | ±0.23 | 0.542–0.810 | 0.70 | <0.001 | 0.70 |
| Honey [portion/day] | 0.17 | ±0.33 | 0.17 | ±0.33 | 0.939–0.978 | 0.96 | <0.001 | 0.60 |
| Wholegrain [portion/day] | 0.15 | ±0.21 | 0.14 | ±0.20 | 0.816–0.931 | 0.89 | <0.001 | 0.22 |
| Cocoa [portion/day] | 0.12 | ±0.17 | 0.10 | ±0.14 | 0.307–0.684 | 0.52 | <0.001 | 0.42 |
| Tea and coffee [portion/day] | 2.56 | ±1.92 | 2.22 | ±1.81 | 0.880–0.956 | 0.93 | <0.001 | <0.001 |
| Tea [portion/day] | 1.62 | ±1.48 | 1.40 | ±1.36 | 0.882–0.956 | 0.93 | <0.001 | 0.003 |
| Coffee [portion/day] | 0.94 | ±1.10 | 0.82 | ±1.00 | 0.800–0.924 | 0.88 | <0.001 | 0.09 |
| Other non-alcoholic beverages (juices) [portion/day] | 0.60 | ±0.52 | 0.56 | ±0.48 | 0.633–0.862 | 0.76 | <0.001 | 0.35 |
| Alcoholic beverages [portion/day] | 0.27 | ±0.44 | 0.25 | ±0.38 | 0.880–0.956 | 0.93 | <0.001 | 0.37 |
| Wine [portion/day] | 0.17 | ±0.35 | 0.16 | ±0.33 | 0.935–0.976 | 0.96 | <0.001 | 0.40 |
| Beer [portion/day] | 0.09 | ±0.14 | 0.08 | ±0.11 | 0.652–0.861 | 0.78 | <0.001 | 0.47 |
| Mean Daily Intake (FFQ) | Percentage in the Same Quartile [%] | Percent in the Opposite Quartile [%] | κ |
|---|---|---|---|
| Total flavonols [mg/day] | 63.33 | 1.67 | 0.65 |
| Quercetin [mg/day] | 58.33 | 6.67 | 0.60 |
| Kaempferol [mg/day] | 61.67 | 1.67 | 0.68 |
| Isorhamnetin [mg/day] | 68.33 | 8.33 | 0.68 |
| Myricetin [mg/day] | 70.00 | 3.33 | 0.73 |
| Fruits [portion/day] | 66.67 | 6.67 | 0.68 |
| Citrus fruits [portion/day] | 66.67 | 8.33 | 0.67 |
| Exotics fruits [portion/day] | 63.33 | 10.00 | 0.63 |
| Seed fruits [portion/day] | 58.33 | 1.67 | 0.64 |
| Local fruits [portion/day] | 63.33 | 5.00 | 0.66 |
| Berries [portion/day] | 60.00 | 11.67 | 0.59 |
| Dried fruits [portion/day] | 71.67 | 5.00 | 0.75 |
| Vegetables [portion/day] | 66.67 | 5.00 | 0.68 |
| Lettuce [portion/day] | 55.00 | 5.00 | 0.60 |
| Other leafy vegetables [portion/day] | 66.67 | 5.00 | 0.68 |
| Solanaceous vegetables [portion/day] | 53.33 | 6.67 | 0.55 |
| Roots and tubers [portion/day] | 55.00 | 6.67 | 0.57 |
| Peppers [portion/day] | 56.67 | 5.00 | 0.62 |
| Cabbage [portion/day] | 58.33 | 10.00 | 0.58 |
| Onions [portion/day] | 55.00 | 5.00 | 0.59 |
| Sprouts [portion/day] | 65.00 | 6.67 | 0.65 |
| Legumes [portion/day] | 70.00 | 1.67 | 0.76 |
| Nuts and seeds [portion/day] | 56.67 | 10.00 | 0.55 |
| Herbs and spices [portion/day] | 65.00 | 6.67 | 0.66 |
| Sauces [portion/day] | 66.67 | 10.00 | 0.65 |
| Jam and honey [portion/day] | 65.00 | 6.67 | 0.69 |
| Jam [portion/day] | 58.33 | 5.00 | 0.63 |
| Honey [portion/day] | 61.67 | 1.67 | 0.67 |
| Wholegrain [portion/day] | 63.33 | 8.33 | 0.64 |
| Cocoa [portion/day] | 66.67 | 13.33 | 0.64 |
| Tea and coffee [portion/day] | 70.00 | 3.33 | 0.74 |
| Tea [portion/day] | 71.67 | 1.67 | 0.76 |
| Coffee [portion/day] | 78.33 | 5.00 | 0.78 |
| Other non-alcoholic beverages (juices) [portion/day] | 73.33 | 5.00 | 0.73 |
| Alcoholic beverages [portion/day] | 76.67 | 0.00 | 0.82 |
| Wine [portion/day] | 75.00 | 8.33 | 0.74 |
| Beer [portion/day] | 81.67 | 5.00 | 0.82 |
| Mean Daily Intake [mg/Day] | CAD Patients (n = 43) | SD | Healthy Control (n = 60) | SD | p |
|---|---|---|---|---|---|
| Total flavonols | 63.40 | ±36.02 | 65.72 | ±31.38 | 0.54 |
| Quercetin | 40.84 | ±24.44 | 41.82 | ±20.39 | 0.53 |
| Kaempferol | 14.36 | ±8.55 | 13.59 | ±7.37 | 0.84 |
| Isorhamnetin | 2.70 | ±2.48 | 5.72 | ±7.65 | 0.002 |
| Myricetin | 5.51 | ±4.17 | 4.58 | ±2.96 | 0.26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popiolek-Kalisz, J.; Fornal, E. Dietary Isorhamnetin Intake Is Inversely Associated with Coronary Artery Disease Occurrence in Polish Adults. Int. J. Environ. Res. Public Health 2022, 19, 12546. https://doi.org/10.3390/ijerph191912546
Popiolek-Kalisz J, Fornal E. Dietary Isorhamnetin Intake Is Inversely Associated with Coronary Artery Disease Occurrence in Polish Adults. International Journal of Environmental Research and Public Health. 2022; 19(19):12546. https://doi.org/10.3390/ijerph191912546
Chicago/Turabian StylePopiolek-Kalisz, Joanna, and Emilia Fornal. 2022. "Dietary Isorhamnetin Intake Is Inversely Associated with Coronary Artery Disease Occurrence in Polish Adults" International Journal of Environmental Research and Public Health 19, no. 19: 12546. https://doi.org/10.3390/ijerph191912546