Exploration of Alcohol Consumption Behaviours and Health-Related Influencing Factors of Young Adults in the UK


Abstract
:1. Introduction
2. Methods
2.1. Ethical Consent
2.2. Study Criteria, Recruitment and Data Collection
2.3. Study Design
2.4. Statistical Analysis
3. Results
3.1. Sample Demographics and Lifestyle Behaviours
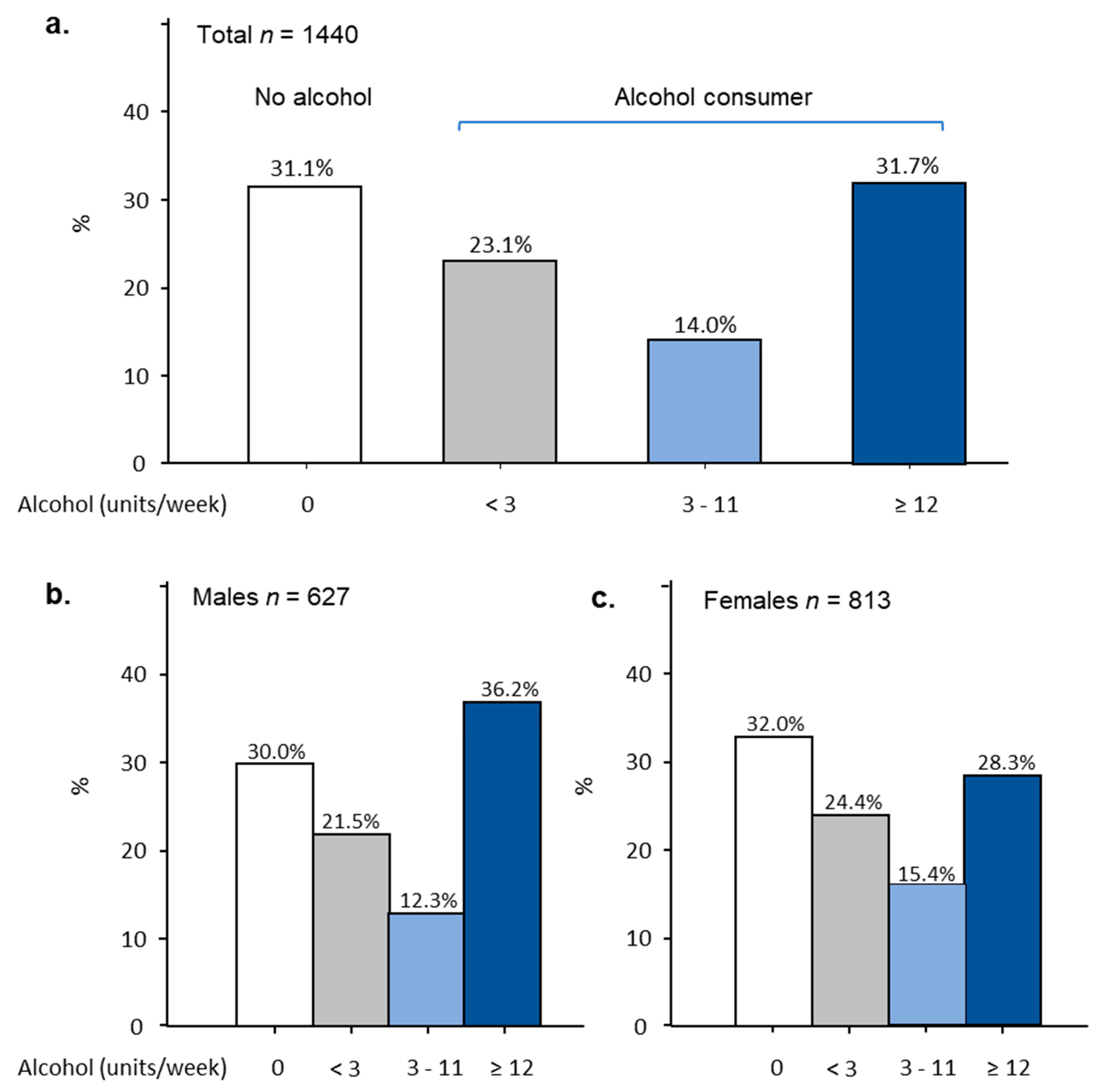
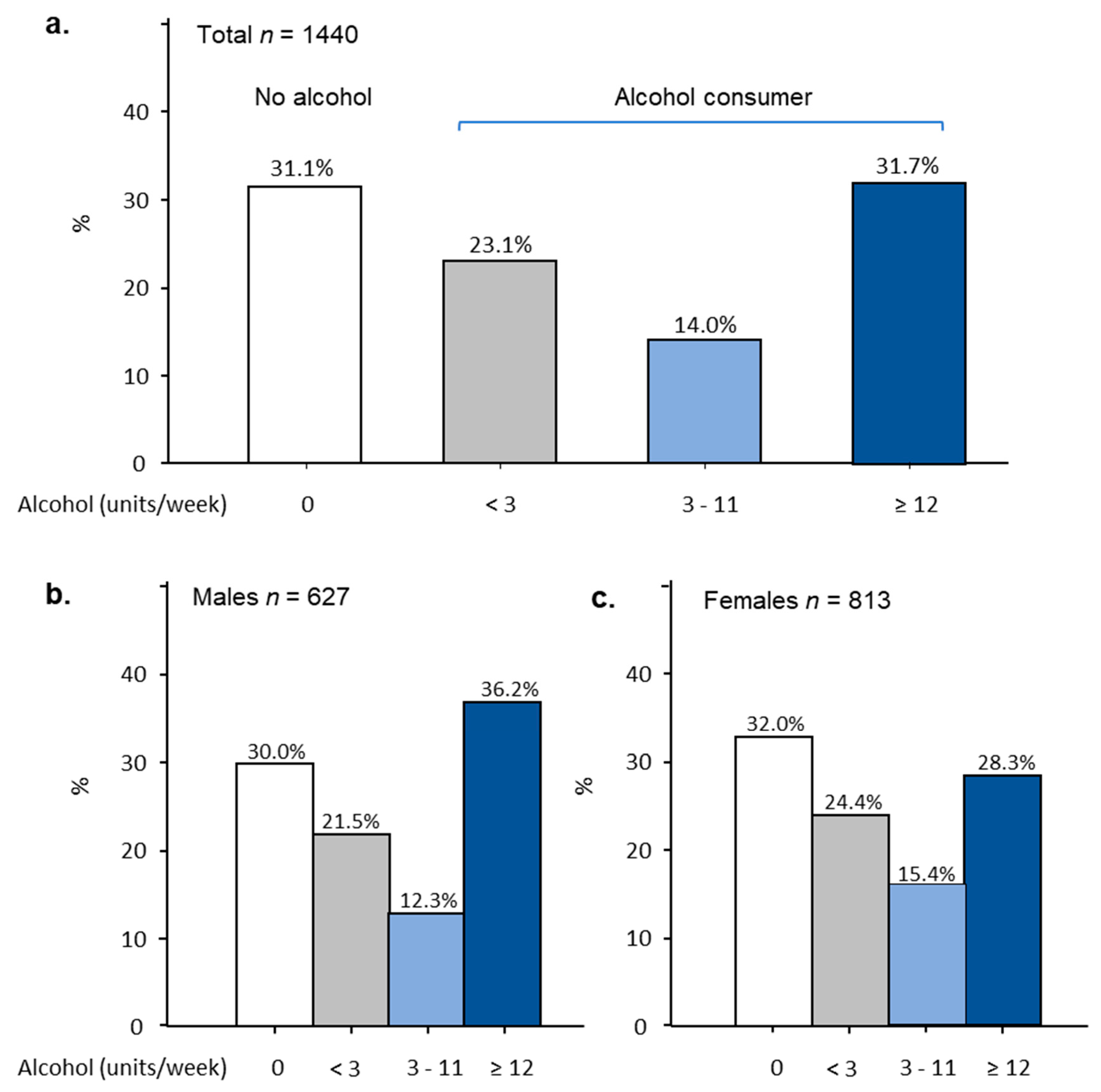
3.2. Alcohol Consumption
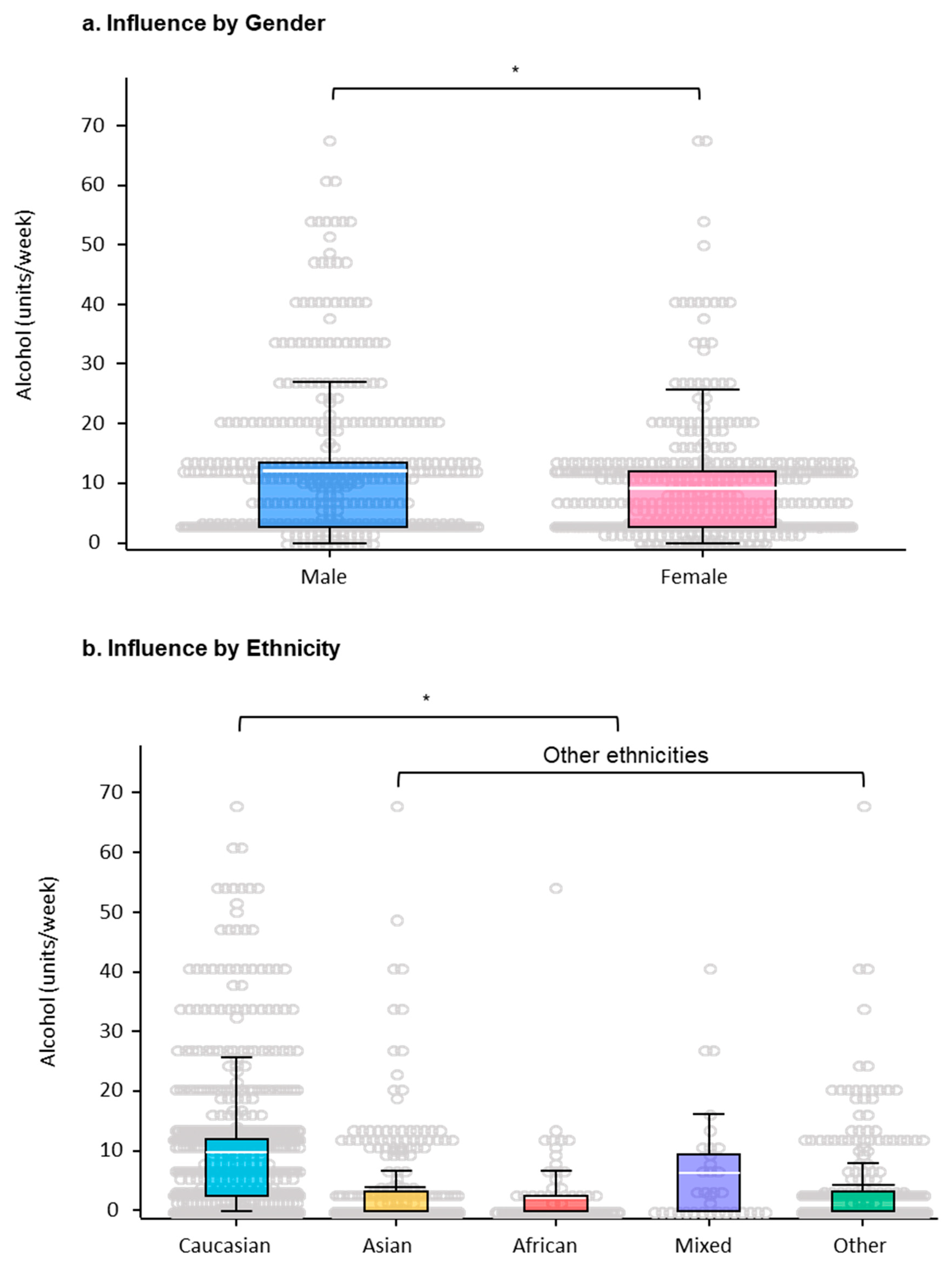
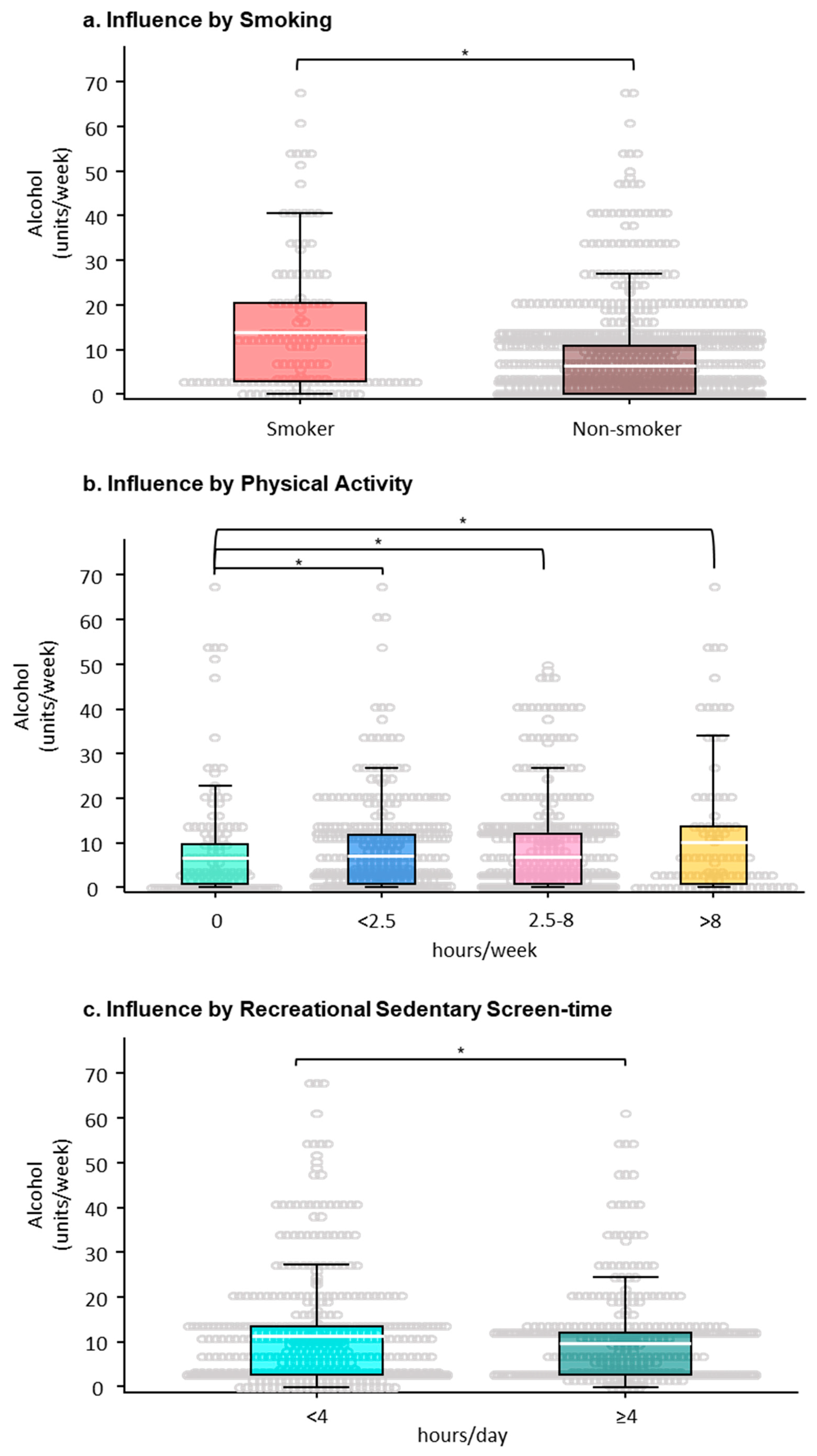
3.3. The Factors Correlated with Alcohol Consumption
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Tavolacci, M.P.; Berthon, Q.; Cerasuolo, D.; Dechelotte, P.; Ladner, J.; Baguet, A. Does binge drinking between the age of 18 and 25 years predict alcohol dependence in adulthood? A retrospective case-control study in France. BMJ Open 2019, 9, e026375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollands, G.J.; Shemilt, I.; Marteau, T.M.; Jebb, S.A.; Kelly, M.P.; Nakamura, R.; Suhrcke, M.; Ogilvie, D. Altering micro-environments to change population health behaviour: Towards an evidence base for choice architecture interventions. BMC Public Health 2013, 13, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Davoren, M.P.; Shiely, F.; Byrne, M.; Perry, I.J. Hazardous alcohol consumption among university students in Ireland: A cross-sectional study. BMJ Open 2015, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatti, S.N.; Leidi, A.; Leake, D.; Li, J.-M. Studying biological science does not lead to adoption of a healthy lifestyle. Perspect. Public Health 2020, 140, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Morton, F.; Tighe, B. Prevalence of, and factors influencing, binge drinking in young adult university under-graduate students. J. Hum. Nutr. Diet. 2011, 24, 296–297. [Google Scholar] [CrossRef]
- Department of Health UK Chief Medical Officers’ Alcohol Guidelines Review 2016. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/489795/summary.pdf (accessed on 1 August 2020).
- Nutt, D.J.; King, L.A.; Phillips, L.D. Drug harms in the UK: A multicriteria decision analysis. Lancet 2010, 376, 1558–1565. [Google Scholar] [CrossRef]
- International Classification of Disease Mortality and Morbidity Statistics. Available online: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/766814084 (accessed on 1 August 2020).
- World Health Organization Global Status Report on Alcohol and Health 2018. Available online: https://www.who.int/substance_abuse/publications/global_alcohol_report/gsr_2018/en/ (accessed on 1 August 2020).
- Winqvist, S.; Jokelainen, J.; Luukinen, H.; Hillbom, M. Adolescents’ Drinking Habits Predict Later Occurrence of Traumatic Brain Injury: 35-Year Follow-up of the Northern Finland 1966 Birth Cohort. J. Adolesc. Health 2006, 39, 275.e1. [Google Scholar] [CrossRef]
- Mewton, L.; Shaw, B.; Slade, T.; Birrell, L.; Newton, N.C.; Chapman, C.; Allsop, S.; Hides, L.; McBride, N.; Andrews, G.; et al. The comorbidity between alcohol use and internalising psychopathology in early adolescence. Ment. Health Prev. 2020, 17, 200176. [Google Scholar] [CrossRef]
- Squeglia, L.M.; Rinker, D.A.; Bartsch, H.; Castro, N.; Chung, Y.; Dale, A.M.; Jernigan, T.L.; Tapert, S.F. Brain volume reductions in adolescent heavy drinkers. Dev. Cogn. Neurosci. 2014, 9, 117–125. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Solà, J. Cardiovascular risks and benefits of moderate and heavy alcohol consumption. Nat. Rev. Cardiol. 2015, 12, 576–587. [Google Scholar] [CrossRef]
- Atwell, K.; Abraham, C.; Duka, T. A parsimonious, integrative model of key psychological correlates of UK university students’ alcohol consumption. Alcohol Alcohol. 2011, 46, 253–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Ansari, W.; Sebena, R.; Stock, C. Socio-demographic correlates of six indicators of alcohol consumption: Survey findings of students across seven universities in England, Wales and Northern Ireland. Arch. Public Health 2013, 71, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craigs, C.L.; Bewick, B.M.; Gill, J.; O’May, F.; Radley, D. UK student alcohol consumption: A cluster analysis of drinking behaviour typologies. Health Educ. J. 2012, 71, 516–526. [Google Scholar] [CrossRef]
- Carroll, H.A.; Rhew, I.; Larimer, M.E. Moderation of relation between psychological risk factors and alcohol use by sex. Women Health 2020, 60, 300–313. [Google Scholar] [CrossRef] [PubMed]
- Center for Substance Abuse Treatment. Substance Abuse Treatment: Addressing the Specific Needs of Women; Treatment Improvement Protocol (TIP) Series 51. HHS Publication No. (SMA) 09-4426; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2009.
- Gardner, S.K.; Robertson, A.A.; Tatch, A.; Walker, C.S. Racial differences in college-student drinking. J. Ethn. Subst. Abus. 2020, 19, 28–43. [Google Scholar] [CrossRef]
- Iwamoto, D.K.; Grivel, M.M.; Cheng, A.W.; Zamboanga, B.L. Asian American and White College Students’ Heavy Episodic Drinking Behaviors and Alcohol-Related Problems. Subst. Use Misuse 2016, 51, 1384–1392. [Google Scholar] [CrossRef]
- Perreault, K.; Bauman, A.; Johnson, N.; Britton, A.; Rangul, V.; Stamatakis, E. Does physical activity moderate the association between alcohol drinking and all-cause, cancer and cardiovascular diseases mortality? A pooled analysis of eight British population cohorts. Br. J. Sports Med. 2017, 51, 651–657. [Google Scholar] [CrossRef]
- Graupensperger, S.; Wilson, O.; Bopp, M.; Blair Evans, M. Longitudinal association between alcohol use and physical activity in US college students: Evidence for directionality. J. Am. Coll. Health 2018, 68, 155–162. [Google Scholar] [CrossRef]
- Pengpid, S.; Peltzer, K. Leisure-time sedentary behavior is associated with psychological distress and substance use among school-going adolescents in five southeast Asian countries: A cross-sectional study. Int. J. Environ. Res. Public Health 2019, 16, 2091. [Google Scholar] [CrossRef] [Green Version]
- Puolitaival, T.; Sieppi, M.; Pyky, R.; Enwald, H.; Korpelainen, R.; Nurkkala, M. Health behaviours associated with video gaming in adolescent men: A cross-sectional population-based MOPO study. BMC Public Health 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Spilková, J.; Chomynová, P.; Csémy, L. Predictors of excessive use of social media and excessive online gaming in Czech teenagers. J. Behav. Addict. 2017, 6, 611–619. [Google Scholar] [CrossRef]
- Office for National Statistics. Adult Drinking Habits in Great Britain: 2017. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/drugusealcoholandsmoking/bulletins/opinionsandlifestylesurveyadultdrinkinghabitsingreatbritain/2017#further-data-on-drinking-habits (accessed on 24 August 2020).
- National Health System (NHS). Statistics on Alcohol, England 2020—NHS Digital 2020. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/statistics-on-alcohol/2020/part-2 (accessed on 24 August 2020).
- Babor, T.F.; Robaina, K.; Noel, J.K.; Ritson, E.B. Vulnerability to alcohol-related problems: A policy brief with implications for the regulation of alcohol marketing. Addiction 2017, 112, 94–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Universities UK Patterns and Trends in UK Higher Education 2018. Available online: https://www.universitiesuk.ac.uk/facts-and-stats/data-and-analysis/Documents/patterns-and-trends-in-uk-higher-education-2018.pdf (accessed on 1 August 2020).
- Wu, W.Q.; Woodman, P.; Chandler-Wilde, S. University of Reading Annual Student Diversity & Inclusion Report 2016 to 2017 Academic Year 2018. Available online: https://www.reading.ac.uk/web/files/Diversity/Diversity_and_Inclusion_Annual_Report_Students_31_January_2018.pdf (accessed on 1 August 2020).
- Farnborough College of Technology Higher Education Application Statistics by Gender, Ethnicity and Index of Deprivation 2018/2019. Available online: https://www.farn-ct.ac.uk/applicationstatistics/ (accessed on 1 August 2020).
- University of Surrey Student key facts 2018–2019. 2019. Available online: https://www.surrey.ac.uk/sites/default/files/2019-01/student-key-facts-2018-19.pdf (accessed on 1 August 2020).
- UK Chief Medical Officers’ Physical Activity Guidelines. 7 September 2019. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/832868/uk-chief-medical-officers-physical-activity-guidelines.pdf (accessed on 1 August 2020).
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Adams Hillard, P.J.; Katz, E.S.; et al. National Sleep Foundation’s updated sleep duration recommendations: Final report. Sleep Health 2015, 1, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Sisson, S.B.; Camhi, S.M.; Church, T.S.; Martin, C.K.; Tudor-Locke, C.; Bouchard, C.; Earnest, C.P.; Smith, S.R.; Newton, R.L.; Rankinen, T.; et al. Leisure time sedentary behavior, occupational/domestic physical activity, and metabolic syndrome in U.S. men and women. Metab. Syndr. Relat. Disord. 2009, 7, 529–536. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Health (NIH). Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. Arch. Intern. Med. 1998. [Google Scholar] [CrossRef] [Green Version]
- O’Connell, A. Logistic Regression Models for Ordinal Response Variables; Sage: Thousand Oaks, CA, USA, 2011. [Google Scholar] [CrossRef]
- Hackshaw, A.; Morris, J.K.; Boniface, S.; Tang, J.L.; Milenkovi, D. Low cigarette consumption and risk of coronary heart disease and stroke: Meta-analysis of 141 cohort studies in 55 study reports. BMJ 2018, 360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolla, N.J.; Wang, C.C. Alcohol and Violence in Psychopathy and Antisocial Personality Disorder: Neural Mechanisms. In Neuroscience of Alcohol: Mechanisms and Treatment; Academic Press: Cambridge, MA, USA, 2019; pp. 277–285. ISBN 9780128131251. [Google Scholar]
- Szinay, D.; Tombor, I.; Garnett, C.; Boyt, N.; West, R. Associations between self-esteem and smoking and excessive alcohol consumption in the UK: A cross-sectional study using the BBC UK Lab database. Addict. Behav. Rep. 2019, 10, 100229. [Google Scholar] [CrossRef]
- Parackal, S.; Smith, C.; Skidmore, P. Diet quality, nutrient intakes and biochemical status of New Zealand women of childbearing age according to alcohol consumption patterns. Public Health Nutr. 2020, 1–11. [Google Scholar] [CrossRef]
- National Union of Students. Students and Alcohol. Research into Students’ Relationship with Alcohol. April 2016. Available online: http://s3-eu-west-1.amazonaws.com/nusdigital/document/documents/27249/9c439fd3a22644fee56ed771c584303a/NUS_Alcohol_Impact_Students_and_alcohol_2016.pdf (accessed on 1 August 2020).
- Allen, J.P.; Loeb, E.L.; Kansky, J.; Davis, A.A. Beyond susceptibility: Openness to peer influence is predicted by adaptive social relationships. Int. J. Behav. Dev. 2020. [Google Scholar] [CrossRef]
- LaBrie, J.W.; Atkins, D.C.; Neighbors, C.; Mirza, T.; Larimer, M.E. Ethnicity specific norms and alcohol consumption among Hispanic/Latino/a and Caucasian students. Addict. Behav. 2012, 37, 573–576. [Google Scholar] [CrossRef] [Green Version]
- Münzel, T.; Hahad, O.; Daiber, A. Double hazard of smoking and alcohol on vascular function in adolescents. Eur. Heart J. 2019, 40, 354. [Google Scholar] [CrossRef] [Green Version]
- Htet, H.; Saw, Y.M.; Saw, T.N.; Htun, N.M.M.; Mon, K.L.; Cho, S.M.; Thike, T.; Khine, A.T.; Kariya, T.; Yamamoto, E.; et al. Prevalence of alcohol consumption and its risk factors among university students: A cross-sectional study across six universities in Myanmar. PLoS ONE 2020, 15, e0229329. [Google Scholar] [CrossRef] [Green Version]
- Partington, S.; Partington, E.; Heather, N.; Longstaff, F.; Allsop, S.; Jankowski, M.; Wareham, H.; Stephens, R.; Gibson, A.S.C. The relationship between membership of a university sports group and drinking behaviour among students at English Universities. Addict. Res. Theory 2013, 21, 339–347. [Google Scholar] [CrossRef]
- Tsunoda, K.; Kai, Y.; Uchida, K.; Kuchiki, T.; Nagamatsu, T. Physical activity and risk of fatty liver in people with different levels of alcohol consumption: A prospective cohort study. BMJ Open 2014, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albani, V.; Bradley, J.; Wrieden, W.L.; Scott, S.; Muir, C.; Power, C.; Fitzgerald, N.; Stead, M.; Kaner, E.; Adamson, A.J. Examining associations between body mass index in 18–25 year-olds and energy intake from alcohol: Findings from the health survey for England and the scottish health survey. Nutrients 2018, 10, 1477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macinnis, R.J.; Hodge, A.M.; Dixon, H.G.; Peeters, A.; Johnson, L.E.A.; English, D.R.; Giles, G.G. Predictors of increased body weight and waist circumference for middle-aged adults. Public Health Nutr. 2014, 17, 1087–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenney, S.R.; Paves, A.P.; Grimaldi, E.M.; LaBrie, J.W. Sleep quality and alcohol risk in college students: Examining the moderating effects of drinking motives. J. Am. Coll. Health 2014, 62, 301–308. [Google Scholar] [CrossRef] [Green Version]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. Int. J. Nurs. Stud. 2013, 50, 587–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epton, T.; Norman, P.; Harris, P.; Webb, T.; Snowsill, F.A.; Sheeran, P. Development of theory-based health messages: Three-phase programme of formative research. Health Promot. Int. 2015, 30, 756–768. [Google Scholar] [CrossRef]
- Sinadinovic, K.; Wennberg, P.; Johansson, M.; Berman, A.H. Targeting individuals with problematic alcohol use via web-based cognitive-behavioral self-help modules, personalized screening feedback or assessment only: A randomized controlled trial. Eur. Addict. Res. 2014. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M.; Al-Ahmadi, M. A Self-reported questionnaire for the assessment of physical activity in youth 15–25 years: Development, reliability and construct validity. Arab J. Food Nutr. 2003, 4, 279–291. [Google Scholar]
- Vadeboncoeur, C.; Foster, C.; Townsend, N. Freshman 15 in England: A longitudinal evaluation of first year university student’s weight change. BMC Obes. 2016, 3, 45. [Google Scholar] [CrossRef] [Green Version]
- Fincham, J.E. Response rates and responsiveness for surveys, standards, and the Journal. Am. J. Pharm. Educ. 2008, 72, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Variable | Males | Females | Total | p-Value | |||
|---|---|---|---|---|---|---|---|
| Gender | 627 | 813 | 1440 | <0.01 | |||
| Age (years), mean (SD) | 19.6 (2.17) | 20.2 (3.03) | 19.9 (2.73) | <0.01 | |||
| BMI (kg/m2), mean (SD) | 22.6 (4.95) | 21.2 (5.24) | 21.8 (5.16) | <0.01 | |||
| n | % | n | % | n | % | ||
| Underweight (<18.5) | 36 | 5.7 | 67 | 8.2 | 103 | 7.2 | 0.61 |
| Normal (18.5–24.9) | 437 | 69.7 | 636 | 78.2 | 1073 | 74.5 | <0.01 |
| Overweight/Obese (≥25/≥30) | 154 | 24.6 | 110 | 13.5 | 264 | 18.3 | 0.19 |
| Ethnicity | |||||||
| Caucasian | 328 | 52.3 | 455 | 56.0 | 783 | 54.4 | 0.17 |
| Asian | 113 | 18.0 | 158 | 19.4 | 271 | 18.8 | 0.49 |
| Black African | 47 | 7.5 | 41 | 5.0 | 88 | 6.1 | 0.05 |
| Mixed | 18 | 2.9 | 16 | 2.0 | 34 | 2.4 | 0.26 |
| Other ethnic group | 121 | 19.3 | 143 | 17.6 | 264 | 18.3 | 0.41 |
| Country of Residence | |||||||
| Europe | 527 | 84.1 | 703 | 86.5 | 1230 | 85.4 | 0.19 |
| Outside Europe | 77 | 12.3 | 85 | 10.5 | 162 | 11.3 | 0.28 |
| Not specified | 23 | 3.7 | 25 | 3.1 | 48 | 3.3 | |
| Smoking Status | |||||||
| Non-smoker | 545 | 86.9 | 745 | 91.6 | 1290 | 89.6 | <0.01 |
| Smoker | 82 | 13.1 | 68 | 8.4 | 150 | 10.4 | |
| Physical Activity (h/week) | |||||||
| 0 | 75 | 12.0 | 123 | 15.1 | 198 | 13.8 | 0.08 |
| <2.5 | 212 | 33.8 | 301 | 37.0 | 513 | 35.6 | 0.21 |
| 2.5–8 | 277 | 44.2 | 346 | 42.6 | 623 | 43.3 | 0.54 |
| >8 | 63 | 10.0 | 43 | 5.3 | 106 | 7.4 | <0.01 |
| Sleeping (h/day) | |||||||
| <7 | 323 | 51.5 | 450 | 55.4 | 773 | 53.7 | 0.15 |
| ≥7 | 282 | 45.0 | 350 | 43.1 | 632 | 43.9 | |
| Not specified | 22 | 3.5 | 13 | 1.6 | 35 | 2.4 | |
| Recreational Sedentary Screen-Time (h/day) | |||||||
| <4 | 256 | 40.8 | 325 | 40.0 | 581 | 40.3 | 0.74 |
| ≥4 | 371 | 59.2 | 488 | 60.0 | 859 | 59.7 | |
| Perception of Physical Fitness | |||||||
| Unfit | 295 | 47.0 | 487 | 59.9 | 782 | 54.3 | <0.01 |
| Fit | 332 | 53.0 | 326 | 40.1 | 658 | 45.7 | |
| Assessments | Males (n = 627, 43.5%) | Females (n = 813, 56.5%) | ||||
|---|---|---|---|---|---|---|
| BMI (kg/m2) | n (%) | OR (CI) | p-value | n (%) | OR (CI) | p-value |
| Normal (18.5–24.9) * | 437 (69.7) | 636 (78.2) | ||||
| Underweight (<18.5) | 36 (5.7) | 1.49 (0.57–3.88) | 0.41 | 67 (8.2) | 0.86 (0.51–1.46) | 0.86 |
| Overweight/Obese (≥25/≥30) | 154 (24.6) | 1.10 (0.68–1.78) | 0.70 | 110 (13.5) | 1.3 (0.82–2.12) | 0.25 |
| Ethnicity | ||||||
| Caucasian | 328 (52.3) | 4.55 (2.63–7.69) | <0.01 | 455 (56.0) | 3.03 (2.04–4.48) | <0.01 |
| Other ethnic group * | 299 (47.7) | 358 (44.0) | ||||
| Smoking Status | ||||||
| Non-smoker * | 545 (86.9) | 3.5 (1.71–7.17) | <0.01 | 745 (91.6) | 2.76 (1.50–5.08) | <0.01 |
| Smoker | 82 (13.1) | 68 (8.4) | ||||
| Physical Activity Levels (h/week) | ||||||
| 0 * | 75 (12.0) | 123 (15.1) | ||||
| <2.5 | 212 (33.8) | 2.46 (1.13–5.32) | 0.02 | 301 (37.0) | 1.25 (0.75–2.07) | 0.04 |
| 2.5–8 | 277 (44.2) | 3.76 (1.71–8.28) | <0.01 | 346 (42.6) | 1.04 (0.62–1.74) | 0.88 |
| >8 | 63 (10.0) | 5.47 (2.12–10.11) | <0.01 | 43 (5.3) | 0.72 (0.33–1.58) | 0.41 |
| Sleep Duration (h/day) | ||||||
| <7 * | 323 (51.5) | 0.77 (0.52–1.14) | 0.19 | 450 (55.4) | 0.86 (0.64–1.17) | 0.33 |
| ≥7 | 282 (45.0) | 350 (43.1) | ||||
| Recreational Sedentary Screen-Time (h/day) | ||||||
| <4 * | 256 (40.8) | 0.31 (0.12–0.86) | 0.03 | 325 (40.0) | 0.63 (0.32–1.24) | 0.18 |
| ≥4 | 371 (59.2) | 488 (60.0) | ||||
| Perception of Physical Fitness | ||||||
| Unfit * | 295 (47.0) | 0.77 (0.50–1.19) | 0.24 | 487 (59.9) | 1.22 (0.88–1.69) | 0.24 |
| Fit | 332 (53.0) | 326 (40.1) | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhatti, S.N.; Fan, L.M.; Collins, A.; Li, J.-M. Exploration of Alcohol Consumption Behaviours and Health-Related Influencing Factors of Young Adults in the UK. Int. J. Environ. Res. Public Health 2020, 17, 6282. https://doi.org/10.3390/ijerph17176282
Bhatti SN, Fan LM, Collins A, Li J-M. Exploration of Alcohol Consumption Behaviours and Health-Related Influencing Factors of Young Adults in the UK. International Journal of Environmental Research and Public Health. 2020; 17(17):6282. https://doi.org/10.3390/ijerph17176282
Chicago/Turabian StyleBhatti, Sunbal Naureen, Lampson M. Fan, Adam Collins, and Jian-Mei Li. 2020. "Exploration of Alcohol Consumption Behaviours and Health-Related Influencing Factors of Young Adults in the UK" International Journal of Environmental Research and Public Health 17, no. 17: 6282. https://doi.org/10.3390/ijerph17176282
APA StyleBhatti, S. N., Fan, L. M., Collins, A., & Li, J.-M. (2020). Exploration of Alcohol Consumption Behaviours and Health-Related Influencing Factors of Young Adults in the UK. International Journal of Environmental Research and Public Health, 17(17), 6282. https://doi.org/10.3390/ijerph17176282