Parental Optimism and Perceived Control over Children’s Initiation of Tobacco, Cannabis, and Opioid Use



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Procedure
2.4. Outcomes
2.4.1. Primary Outcome
2.4.2. Secondary Outcomes
2.5. Statistical Analyses
3. Results
3.1. Participant Characteristics
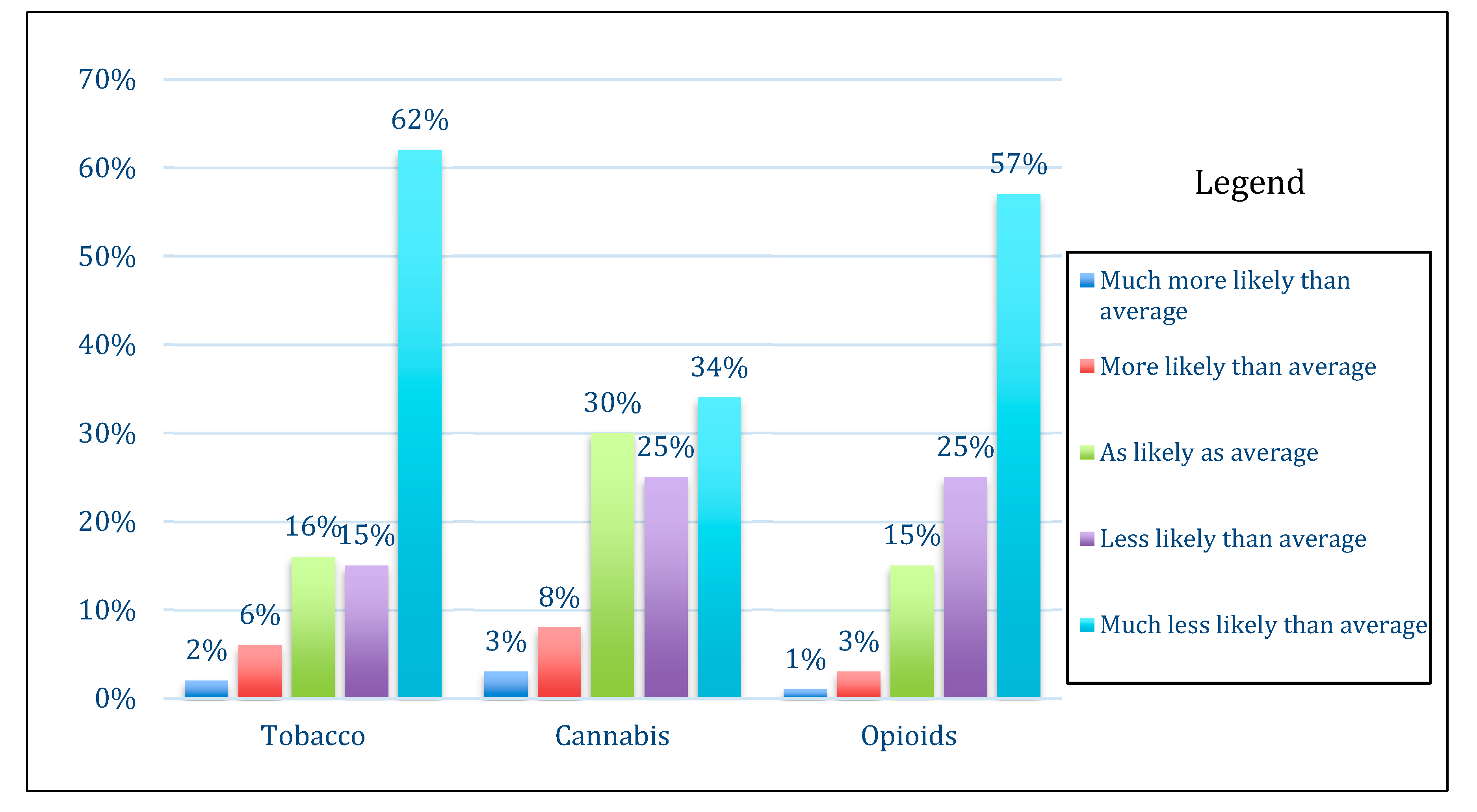
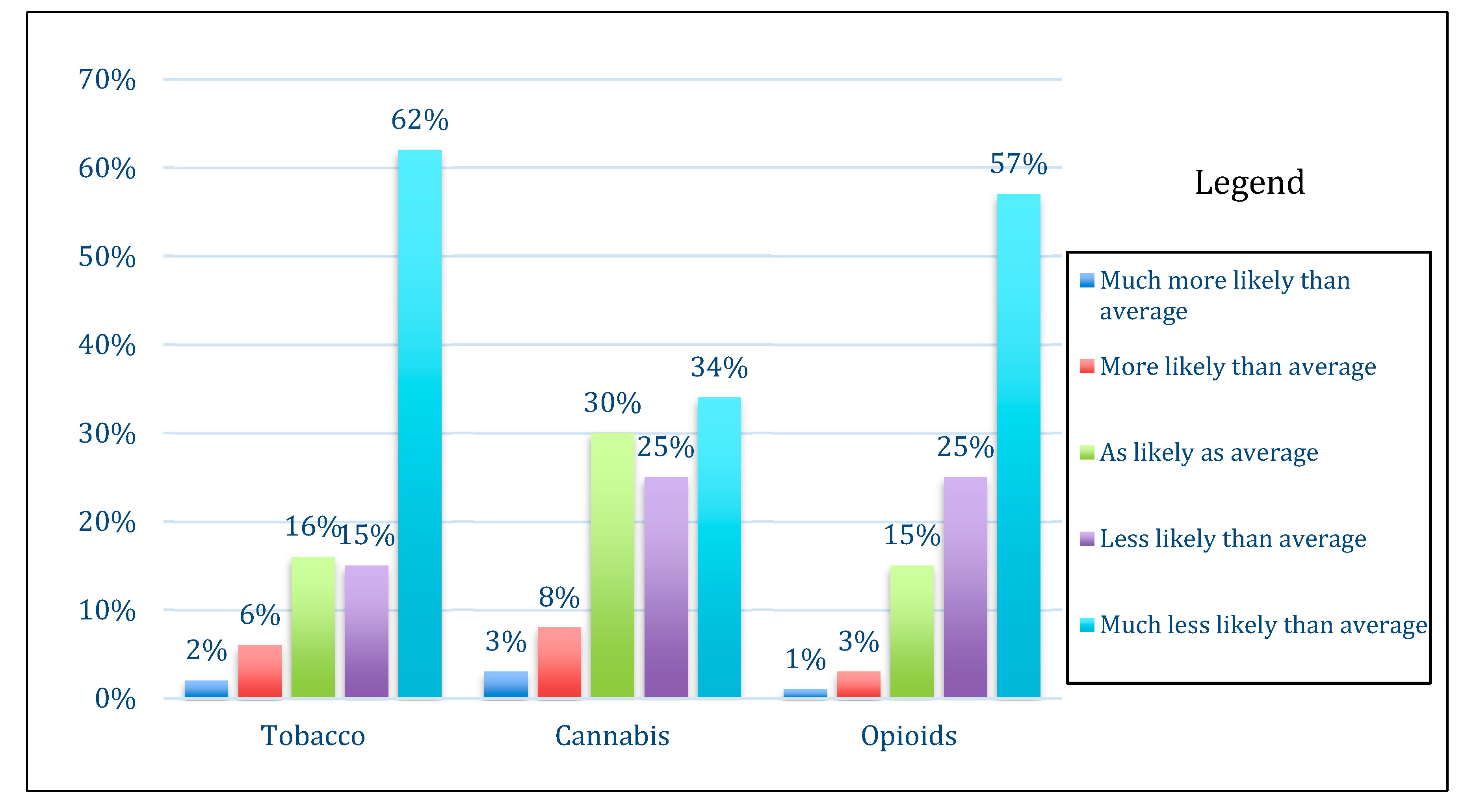
3.2. Parental Perceived Risk, Control, and Severity
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Johnston, L.D.; Miech, R.A.; O’malley, P.M.; Bachman, J.G.; Schulenberg, J.E.; Patrick, M.E. Key Findings on Adolescent Drug Use: Monitoring the Future Survey Results on Drug Use 1975–2019; Institute for Social Research, University of Michigan: Ann Arbor, MI, USA, 2020. [Google Scholar]
- Propel Center for Population Health Impact. Detailed Tables for the Canadian Student Tobacco, Alcohol and Drugs Survey 2016–17; University of Waterloo: Waterloo, ON, Canada, 2018. [Google Scholar]
- Ferkol, T.W.; Farber, H.J.; La Grutta, S.; Leone, F.T.; Marshall, H.M.; Neptune, E.; Pisinger, C.; Vanker, A.; Wisotzky, M.; Zabert, G.E.; et al. Electronic cigarette use in youths: A position statement of the Forum of International Respiratory Societies. Eur. Respir. J. 2018, 51, 1800278. [Google Scholar] [CrossRef] [PubMed]
- Lipari, R.N. Trends in Adolescent Substance Use and Perception of Risk from Substance Use; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2013. [Google Scholar]
- Okaneku, J.; Vearrier, D.; McKeever, R.G.; LaSala, G.S.; Greenberg, M.I. Change in perceived risk associated with marijuana use in the United States from 2002 to 2012. Clin. Toxicol. 2015, 53, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Trucco, E.M. A review of psychosocial factors linked to adolescent substance use. Pharmacol. Biochem. Behav. 2020, 196, 172969. [Google Scholar] [CrossRef] [PubMed]
- Calafat, A.; Garcia, F.; Juan, M.; Becoña, E.; Fernández-Hermida, J.R. Which parenting style is more protective against adolescent substance use? Evidence within the European context. Drug Alcohol Depend. 2014, 138, 185–192. [Google Scholar] [CrossRef]
- Sargent, J.D.; Dalton, M. Does parental disapproval of smoking prevent adolescents from becoming established smokers? Pediatrics 2001, 108, 1256–1262. [Google Scholar] [CrossRef]
- Yule, A.; Wilens, T.E.; Martelon, M.K.; Simon, A.; Biederman, J. Does exposure to parental substance use disorders increase substance use disorder risk in offspring? A 5-year follow-up study. Am. J. Addict. 2013, 22, 460–465. [Google Scholar] [CrossRef]
- Sharmin, S.; Kypri, K.; Khanam, M.; Wadolowski, M.; Bruno, R.; Attia, J.; Holliday, E.G.; Palazzi, K.; Mattick, R.P. Effects of parental alcohol rules on risky drinking and related problems in adolescence: Systematic review and meta-analysis. Drug Alcohol Depend. 2017, 178, 243–256. [Google Scholar] [CrossRef]
- Grevenstein, D.; Nagy, E.; Jungaberle, H. Development of risk perception and substance use of tobacco, alcohol and cannabis among adolescents and emerging adults: Evidence of directional influences. Subst. Use Misuse 2014, 50, 376–386. [Google Scholar] [CrossRef]
- Chadi, N.; Levy, S.; Weitzman, E.R. Moving beyond perceived riskiness: Marijuana-related beliefs and marijuana use in adolescents. Subst. Abus. 2019, 1–4. [Google Scholar] [CrossRef]
- Drouin, O.; Winickoff, J.P.; Thorndike, A.N. Parental optimism about children’s risk of future tobacco use and excessive weight gain. Acad. Pediatr. 2019, 19, 90–96. [Google Scholar] [CrossRef]
- Wright, D.R.; Lozano, P.; Dawson-Hahn, E.; Christakis, D.A.; Haaland, W.L.; Basu, A. Parental optimism about childhood obesity-related disease risks. Int. J. Obes. 2017, 41, 1467–1472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lippold, M.A.; Glatz, T.; Fosco, G.M.; Feinberg, M.E. Parental perceived control and social support: Linkages to change in parenting behaviors during early adolescence. Fam. Process. 2017, 57, 432–447. [Google Scholar] [CrossRef] [PubMed]
- Murray, T.; Rodgers, W.M.; Fraser, S.N. Exploring the relationship between socioeconomic status, control beliefs and exercise behavior: A multiple mediator model. J. Behav. Med. 2011, 35, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.R. Sufficient Grounds for Optimism?: The relationship between perceived controllability and optimistic bias. J. Soc. Clin. Psychol. 1996, 15, 9–52. [Google Scholar] [CrossRef]
- Winickoff, J.P.; Nabi-Burza, E.; Chang, Y.; Regan, S.; Drehmer, J.; Finch, S.; Wasserman, R.; Ossip, D.; Hipple, B.; Woo, H.; et al. Sustainability of a parental tobacco control intervention in pediatric practice. Pediatrics 2014, 134, 933–941. [Google Scholar] [CrossRef] [Green Version]
- Buhrmester, M.; Kwang, T.; Gosling, S.D. Amazon’s mechanical turk. Perspect. Psychol. Sci. 2011, 6, 3–5. [Google Scholar] [CrossRef]
- Crump, M.J.C.; McDonnell, J.V.; Gureckis, T.M. Evaluating amazon’s mechanical turk as a tool for experimental behavioral research. PLoS ONE 2013, 8, e57410. [Google Scholar] [CrossRef] [Green Version]
- Weinstein, N.D. Unrealistic optimism about susceptibility to health problems: Conclusions from a community-wide sample. J. Behav. Med. 1987, 10, 481–500. [Google Scholar] [CrossRef]
- Schiavon, C.C.; Marchetti, E.; Gurgel, L.G.; Busnello, F.M.; Reppold, C.T. Optimism and hope in chronic disease: A systematic review. Front. Psychol. 2017, 7, 543. [Google Scholar] [CrossRef] [Green Version]
- Casey, B.; Jones, R.M. Neurobiology of the adolescent brain and behavior: Implications for substance use disorders. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 1189–1201. [Google Scholar] [CrossRef]
- Squeglia, L.M.; Gray, K.M. Alcohol and drug use and the developing brain. Curr. Psychiatry Rep. 2016, 18, 46. [Google Scholar] [CrossRef] [PubMed]
- Peeters, M.; Oldehinkel, T.; Vollebergh, W. Behavioral control and reward sensitivity in adolescents’ risk taking behavior: A longitudinal TRAILS study. Front. Psychol. 2017, 8. [Google Scholar] [CrossRef] [Green Version]
- Woodgate, R.L.; Kreklewetz, C.M. Youth’s narratives about family members smoking: Parenting the parent- it’s not fair! BMC Public Health 2012, 12, 965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, K.P.; Levy, S. Big marijuana—Lessons from big tobacco. N. Engl. J. Med. 2014, 371, 399–401. [Google Scholar] [CrossRef] [Green Version]
- Griffin, K.W.; Botvin, G.J. Evidence-based interventions for preventing substance use disorders in adolescents. Child Adolesc. Psychiatr. Clin. N. Am. 2010, 19, 505–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Characteristics | n (%) a or Mean (SD) b | Missing 2 |
|---|---|---|
| Total | n = 427 | |
| Parent’s characteristics | ||
| Age (years) b | 38.1 (8.4) | 20 |
| Female a | 274 (67.3) | 20 |
| Education a | 21 | |
| Elementary/Some high school/High school graduate | 35 (8.6) | |
| Some college | 117 (28.8) | |
| College graduate | 191 (47.0) | |
| Graduate degree | 63 (15.5) | |
| Smoking a | 12 | |
| Smoker in the house | 93 (22.4) | |
| Respondent smokes cigarettes everyday | 58 (14.0) | |
| Respondent smokes cigarettes some days | 18 (4.3) | |
| Respondent is a former smoker | 123 (29.6) | |
| Respondent has never smoked cigarettes | 216 (52.0) | |
| Child’s characteristics 3 | ||
| Child age (years) b | 9.3 (5.1) | 1 |
| Female a | 203 (50.0) | 21 |
| Teenager: 13–17 years old a | 140 (32.9) | 1 |
| Substance use a | ||
| Child has consumed cannabis (yes) | 8 (6.0) 4 | 6 |
| Child has used opioids (yes) | 2 (1.5) 4 | 5 |
| Child smokes cigarettes (yes) | 1 (0.7) 4 | 0 |
| Respondent Characteristics | Optimism 2: Tobacco | Optimism: Cannabis | Optimism: Opioids |
|---|---|---|---|
| AOR 3 (95% CI) | AOR (95% CI) | AOR (95% CI) | |
| Men (vs. women) | 1.00 (0.59, 1.72) | 1.36 (0.86, 2.15) | 1.46 (0.81, 2.64) |
| College graduate (vs. not) | 1.10 (0.65, 1.86) | 1.31 (0.84, 2.04) | 0.90 (0.51, 1.58) |
| Parent of teenager (vs. parent of younger child) | 1.04 (0.61, 1.77) | 1.19 (0.75, 1.87) | 1.19 (0.67, 2.11) |
| Current smoker (vs. Never smoker) | 0.18 (0.10, 0.34) | 0.21 (0.12, 0.38) | 0.59 (0.30, 1.16) |
| Former smoker (vs. Never smoker) | 0.47 (0.26, 0.85) | 0.47 (0.29, 0.76) | 1.09 (0.58, 2.06) |
| Respondent Characteristics | Tobacco | Cannabis | Opioids |
|---|---|---|---|
| Delta 2 (95% CI) | Delta (95% CI) | Delta (95% CI) | |
| Men (vs. women) | 0.17 (−0.06, 0.40) | 0.09 (−0.14, 0.33) | 0.12 (−0.11, 0.36) |
| College graduate (vs. not) | −0.09 (−0.32, 0.13) | −0.08 (−0.32, 0.15) | −0.19 (−0.42, 0.04) |
| Parent of teenager (vs. parent of younger child) | −0.22 (−0.45, 0.01) | −0.19 (−0.43, 0.04) | −0.16 (−0.40, 0.07) |
| Current smoker (vs. Never smoker) | −0.34 (−0.63, −0.04) | −0.16 (−0.46, 0.15) | −0.16 (−0.46 0.14) |
| Former smoker (vs. Never smoker) | −0.32 (−0.56, −0.07) | −0.31 (−0.56, −0.05) | −0.26 (−0.52, −0.01) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chadi, N.; Winickoff, J.P.; Drouin, O. Parental Optimism and Perceived Control over Children’s Initiation of Tobacco, Cannabis, and Opioid Use. Int. J. Environ. Res. Public Health 2020, 17, 6181. https://doi.org/10.3390/ijerph17176181
Chadi N, Winickoff JP, Drouin O. Parental Optimism and Perceived Control over Children’s Initiation of Tobacco, Cannabis, and Opioid Use. International Journal of Environmental Research and Public Health. 2020; 17(17):6181. https://doi.org/10.3390/ijerph17176181
Chicago/Turabian StyleChadi, Nicholas, Jonathan P. Winickoff, and Olivier Drouin. 2020. "Parental Optimism and Perceived Control over Children’s Initiation of Tobacco, Cannabis, and Opioid Use" International Journal of Environmental Research and Public Health 17, no. 17: 6181. https://doi.org/10.3390/ijerph17176181