
Socio-Economic and Environmental Factors Associated with Overweight and Obesity in Children Aged 6–8 Years Living in Five Italian Cities (the MAPEC_LIFE Cohort)

 , , , , , , , , , , , ,
, , , , , , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Monitoring Air Pollution Effects on Children for Supporting Public Health Policy (MAPEC_LIFE) Project
2.2. Recruitment of Children and Questionnaire Administration
2.3. Data Processing and Statistical Analysis
- Personal data: age, gender, child’s nation of birth (Italy or outside Italy), city of residence;
- Information on the parents: nation of birth (Italy or outside Italy), level of education (degree or high-school leaving certificate/lower qualification), employment status (employed or unemployed, including students and homemakers), level of employment (level I: businessman, manager, professional; level II: office worker; level III: manual worker, craftsman), smoking habits;
- Information on child’s physical activity: regular exercise (three or more times a week), outdoor sports;
- Outdoor pollution exposure factors: perceived level of traffic near the home and the school.
2.4. Ethical Aspects
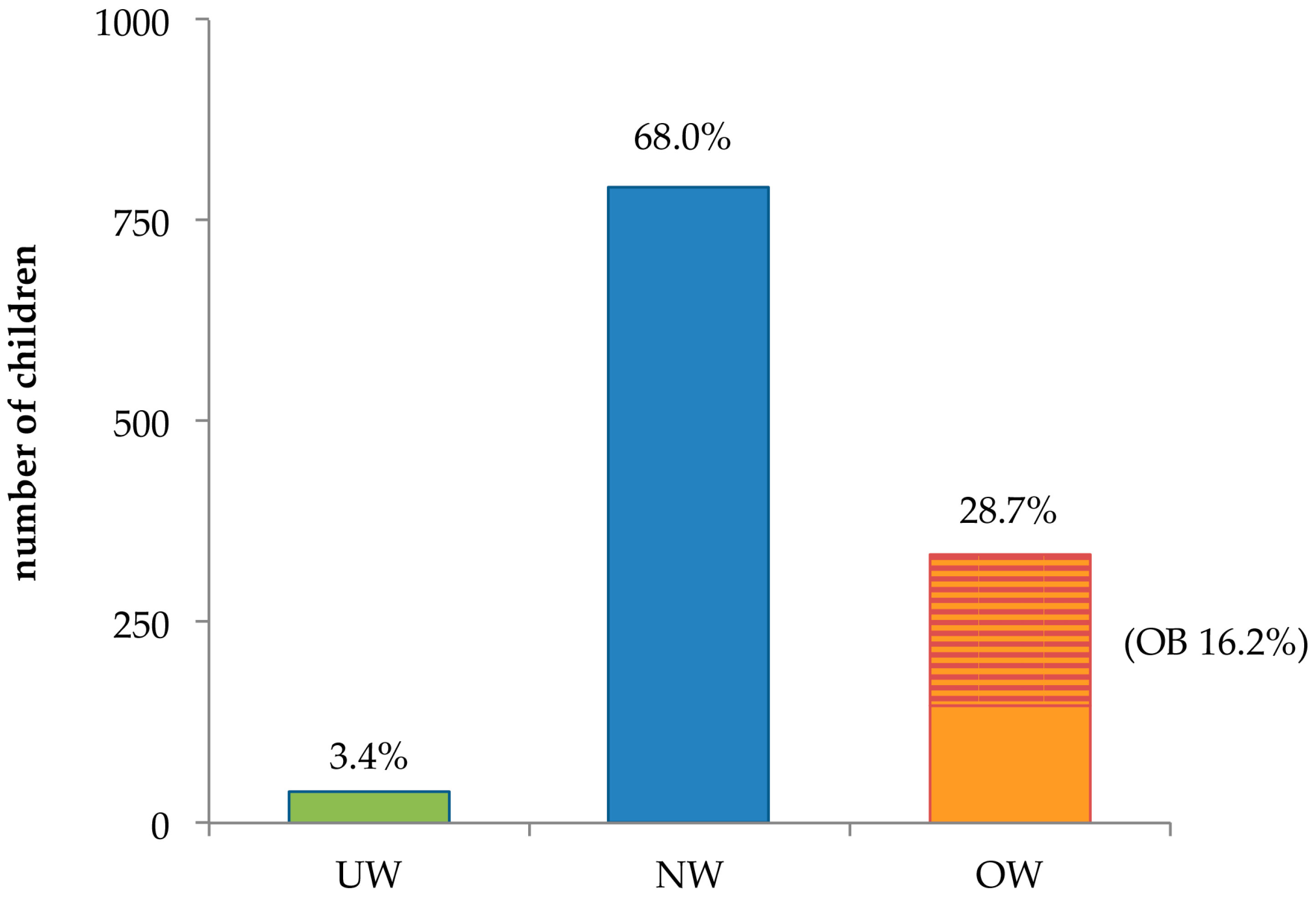
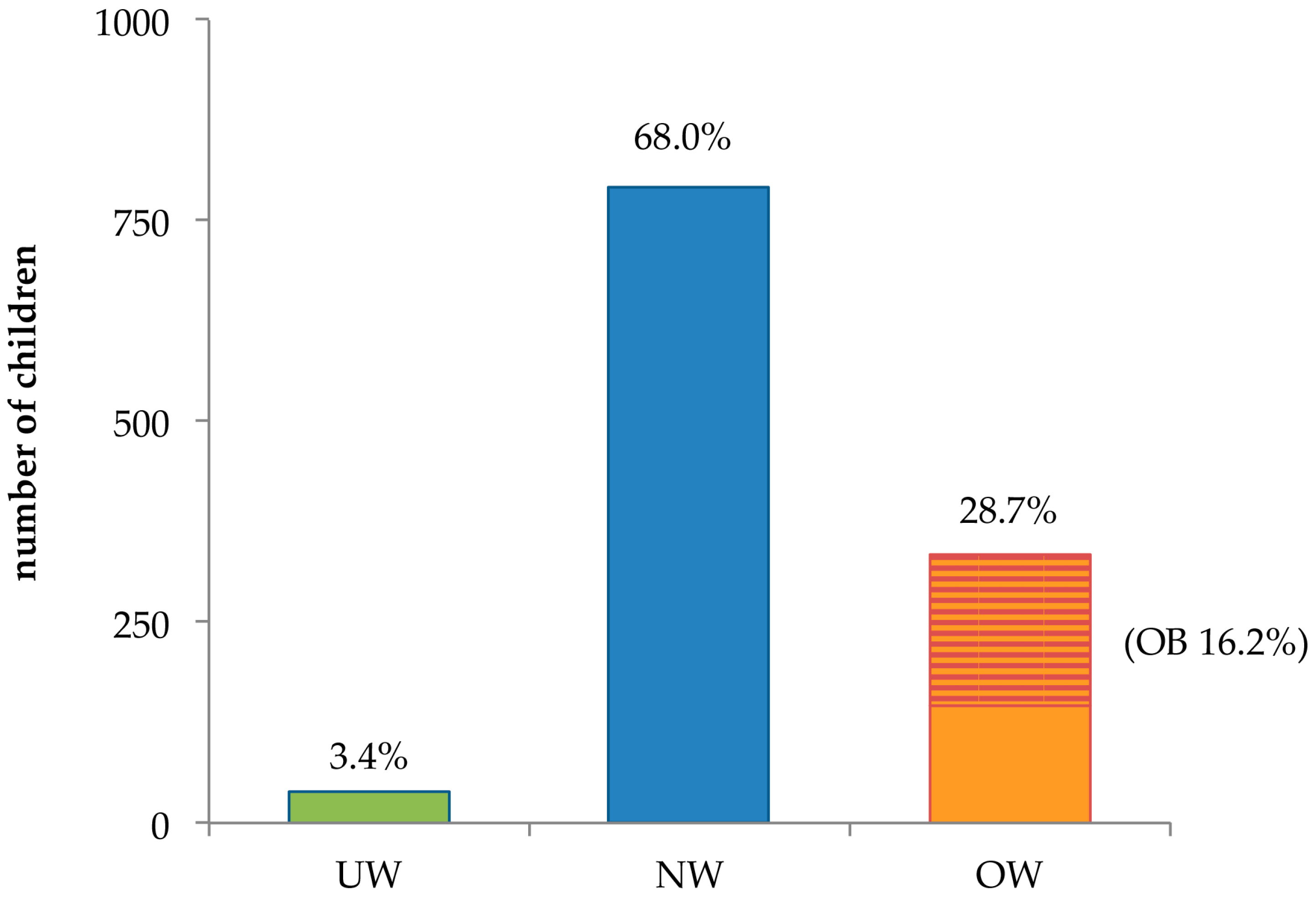
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; WHO Obesity Technical Report Series 894; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- James, P.T.; Leach, R.; Kalamara, E.; Shayeghi, M. The Worldwide obesity epidemic. Obes. Res. 2001, 9, 228S–233S. [Google Scholar] [CrossRef] [PubMed]
- Caballero, B. The global epidemic of obesity: An overview. Epidemiol. Rev. 2007, 29, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, Q.I.; Ahmad, C.B.; Ahmad, S.M. Childhood obesity. Indian J. Endocrinol. Metab. 2010, 14, 19–25. [Google Scholar] [PubMed]
- Lobstein, T.; Baur, L.; Uauy, R.; IASO International Obesity Task Force. Obesity in children and young people: A crisis in public health. Obes. Rev. 2004, 5, 4–104. [Google Scholar] [CrossRef] [PubMed]
- Branca, F.; Nikogosian, H.; Lobstein, T. The Challenge of Obesity in the WHO European Region and the Strategies for Response; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2007. [Google Scholar]
- Wijnhoven, T.M.; van Raaij, J.M.; Spinelli, A.; Starc, G.; Hassapidou, M.; Spiroski, I.; Rutter, H.; Martos, É.; Rito, A.I.; Hovengen, R.; et al. WHO European childhood obesity surveillance initiative: Body mass index and level of overweight among 6–9-year-old children from school year 2007/2008 to school year 2009/2010. BMC Public Health 2014, 14, 806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobstein, T. Prevalence and Trends across the World. Available online: http://ebook.ecog-obesity.eu/chapter-epidemiology-prevention-across-europe/prevalence-trends-across-world/ (accessed on 30 August 2016).
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Ferede Abera, S. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the global burden of disease study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Nardone, P.; Spinelli, A.; Lauria, L.; Buoncristiano, M.; Lauria, L.; Pizz, E.; Galeone, D. Il Sistema di Sorveglianza OKkio Alla SALUTE: Risultati 2014. Available online: http://www.iss.it/binary/publ/cont/ONLINE_Okkio.pdf (accessed on 27 July 2016).
- Apovian, C.M. Obesity: Definition, comorbidities, causes, and burden. Am. J. Manag. Care 2016, 22, S176–S185. [Google Scholar] [CrossRef]
- Maffeis, C. Aetiology of overweight and obesity in children and adolescents. Eur. J. Pediatr. 2000, 159, S35–S44. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Armstrong, J.; Dorosty, A.R.; Emmett, P.M.; Ness, A.; Rogers, I.; Steer, C.; Sherriff, A. Early life risk factors for obesity in childhood: Cohort study. Br. Med. J. 2005, 330, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Wareham, N.J.; van Sluijs, E.M.F.; Ekelund, U. Physical activity and obesity prevention: A review of the current evidence. Proc. Nutr. Soc. 2005, 64, 229–247. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.W.; Grant, A.M.; Goulding, A.; Williams, S.M. Early adiposity rebound: Review of papers linking this to subsequent obesity in children and adults. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, P.O.A.; Victora, C.G. Rapid growth in infancy and childhood and obesity in later life—A systematic review. Obes. Rev. 2005, 6, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.K. Size at birth, postnatal growth and risk of obesity. Horm. Res. 2006, 65, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Moreno, L.A.; Rodríguez, G. Dietary risk factors for development of childhood obesity. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Kleiser, C.; Schaffrath Rosario, A.; Mensink, G.B.M.; Prinz-Langenohl, R.; Kurth, B.M. Potential determinants of obesity among children and adolescents in Germany: Results from the cross-sectional KIGGS study. BMC Public Health 2009, 9, 46. [Google Scholar] [CrossRef] [PubMed]
- Jerrett, M.; McConnell, R.; Wolch, J.; Chang, R.; Lam, C.; Dunton, G.; Gilliland, F.; Lurmann, F.; Islam, T.; Berhane, K. Traffic-related air pollution and obesity formation in children: A longitudinal, multilevel analysis. Environ. Health 2014, 13, 49. [Google Scholar] [CrossRef] [PubMed]
- Tchicaya, A.; Lorentz, N. Relationship between Children’s body mass index and parents’ obesity and socioeconomic status: A multilevel analysis applied with Luxembourg data. Health 2014, 6, 2322–2332. [Google Scholar] [CrossRef]
- Lamerz, A.; Kuepper-Nybelen, J.; Wehle, C.; Bruning, N.; Trost-Brinkhues, G.; Brenner, H.; Hebebrand, J.; Herpertz-Dahlmann, B. Social class, parental education, and obesity prevalence in a study of six-year-old children in Germany. Int. J. Obesity 2005, 29, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Methven, E.; McDowell, Z.C.; Hacking, B.; Alexander, D.; Steward, L.; Kelnar, C.J.H. Health consequences of obesity. Arch. Dis. Child. 2003, 88, 748–752. [Google Scholar] [CrossRef] [PubMed]
- Ebbeling, C.B.; Pawlak, D.B.; Ludwig, D.S. Childhood obesity: Public-health crisis, common sense cure. Lancet 2002, 360, 473–482. [Google Scholar] [CrossRef]
- Wang, G.; Dietz, W.H. Economic burden of obesity in youths aged 6 to 17 years: 1979–1999. Pediatrics 2002, 109, E81–E86. [Google Scholar] [CrossRef] [PubMed]
- Feretti, D.; Ceretti, E.; De Donno, A.; Moretti, M.; Carducci, A.; Bonetta, S.; Marrese, M.R.; Bonetti, A.; Covolo, L.; Bagordo, F.; et al. Monitoring air pollution effects on children for supporting public health policy: The protocol of the prospective cohort MAPEC study. BMJ Open 2014, 4, e006096. [Google Scholar] [CrossRef] [PubMed]
- De Donno, A.; Grassi, T.; Ceretti, E.; Viola, G.C.V.; Levorato, S.; Vannini, S.; Salvatori, T.; Carducci, A.; Verani, M.; Bonetta, S.; et al. Air pollution biological effects in children living in Lecce (Italy) by buccal micronucleus cytome assay (the MAPEC_LIFE study). Int. J. Sus. Dev. Plan. 2016, 11, 500–510. [Google Scholar] [CrossRef]
- Zani, C.; Donato, F.; Grioni, S.; Viola, G.C.V.; Ceretti, E.; Feretti, D.; Festa, A.; Bonizzoni, S.; Bonetti, A.; Monarca, S.; et al. Feasibility and reliability of a questionnaire for evaluation of the exposure to indoor and outdoor air pollutants, diet and physical activity in 6–8-year-old children. Ann. Ig. 2015, 27, 646–656. [Google Scholar] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinnes in children and adolescents: International survey. BMJ 2007, 335, 194. [Google Scholar] [CrossRef] [PubMed]
- Wijnhoven, T.M.A.; van Raaij, J.M.A.; Spinelli, A.; Rito, A.I.; Hovengen, R.; Kunesova, M.; Starc, G.; Rutter, H.; Sjöberg, A.; Petrauskiene, A.; et al. WHO European Childhood Obesity Surveillance Initiative 2008: Weight, height and body mass index in 6–9-year-old children. Pediatr. Obes. 2013, 8, 79–97. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, W.; Pigeot, I.; Pohlabeln, H.; De Henauw, S.; Lissner, L.; Molnár, D.; Moreno, L.A.; Tornaritis, M.; Veidebaum, T.; Siani, A.; On behalf of the IDEFICS consortium. Prevalence of overweight and obesity in European children below the age of 10. Int. J. Obes. 2014, 38, S99–S107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maffeis, C.; Consolaro, A.; Cavarzere, P.; Chini, L.; Banzato, C.; Grezzani, A.; Silvagni, D.; Salzano, G.; De Luca, F.; Tatò, L. Prevalence of overweight and obesity in 2- to 6-year-old Italian children. Obesity 2006, 14, 765–769. [Google Scholar] [CrossRef] [PubMed]
- Censi, L.; D’Addesa, D.; Martone, D.; Galfo, M.; Bevilacqua, N.; Roccaldo, R.; Angelini, V.; Fabbri, I.; Catasta, G.; Toti, E.; et al. Articolazione dello studio ZOOM8. In Studio ZOOM8: l’alimentazione e l’attività Fisica dei Bambini della Scuola Primary; Censi, L., D’Addesa, D., Galeone, D., Andreozzi, S., Spinelli, A., Eds.; Rapporti ISTISAN 12/42; Istituto Superiore di Sanità: Roma, Italy, 2012; Volume 42, pp. 5–16. [Google Scholar]
- Turchetta, F.; Gatto, G.; Saulle, R.; Romano, F.; Boccia, A.; La Torre, G. Systematic review and meta-analysis of the prevalence of overweight and obesity among school-age children in Italy. Epidemiol. Prev. 2012, 36, 188–195. [Google Scholar] [PubMed]
- Celi, F.; Bini, V.; De Giorgi, G.; Molinari, D.; Faraoni, F.; Di Stefano, G.; Bacosi, M.L.; Berioli, M.G.; Contessa, G.; Florin, A. Epidemiology of overweight and obesity among school children and adolescents in three provinces of central Italy, 1993–2001: Study of potential influencing variables. Eur. J. Clin. Nutr. 2003, 57, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Harding, S.; Teyhan, A.; Maynard, M.J.; Cruickshank, J.K. Ethnic differences in overweight and obesity in early adolescence in the MRC DASH study: The role of adolescent and parental lifestyle. Int. J. Epidemiol. 2008, 37, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Huerta, M.; Bibi, H.; Haviv, J.; Scharf, S.; Gdalevich, M. Parental smoking and education as determinants of overweight in Israeli children. Prev. Chronic Dis. 2006, 3, 1–9. [Google Scholar]
- Shrewsbury, V.; Wardle, J. Socioeconomic status and adiposity in childhood: A systematic review of cross-sectional studies 1990–2005. Obesity 2008, 16, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Johnson, F.; Pratt, M.; Wardle, W. Socio-economic status and obesity in childhood. In Epidemiology of Obesity in Children and Adolescents—Prevalence and Etiology; Moreno, L.A., Pigeot, I., Ahrens, W., Eds.; Springer: New York, NY, USA, 2011; Volume 2, pp. 377–390. [Google Scholar]
- Coll, J.L.; del Mar Bibiloni, M.; Salas, R.; Pons, A.; Tur, J.A. The prevalence of excessive weight in Balearic Islands’ young and middle-aged women and its association with social and socioeconomic factors: A ten-year trend (2000–2010). BMC Public Health 2015, 15, 837. [Google Scholar] [CrossRef] [PubMed]
- Lissner, L.; Wijnhoven, T.M.A.; Mehlig, K.; Sjöberg, A.; Kunesova, M.; Yngve, A.; Petrauskiene, A.; Duleva, V.; Rito, A.I.; Breda, J. Socioeconomic inequalities in childhood overweight: Heterogeneity across five countries in the WHO European Childhood Obesity Surveillance Initiative (COSI-2008). Int. J. Obes. 2016, 40, 796–802. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.H.; Huang, C.L.; French, S.A. Factors associated with women’s and children’s body mass indices by income status. Int. J. Obes. 2004, 28, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Hui, L.L.; Nelson, E.A.; Yu, L.M.; Li, A.M.; Fok, T.F. Risk factors for childhood overweight in 6- to 7-y-old Hong Kong children. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 1411–1418. [Google Scholar] [CrossRef] [PubMed]
- Danielsik, S.; Czerwinski-Mast, M.; Langnäse, K.; Dilba, B.; Müller, M.J. Parental overweight, socioeconomic status and high birth weight are the major determinants of overweight and obesity in 5–7 y-old children: Baseline data of the Kiel Obesity Prevention Study (KOPS). Int. J. Obes. Relat. Metab. Disord. 2004, 28, 1494–1502. [Google Scholar] [CrossRef] [PubMed]
- Carducci, A.; Casini, B.; Donzelli, G.; Verani, M.; Bruni, B.; Ceretti, E.; Zani, C.; Carraro, E.; Bonetta, S.; Bagordo, F.; et al. Improving awareness of health hazards associated with air pollution in primary school children: Design and test of didactic tools. Appl. Environ. Educ. Commun. 2016, 15, 247–260. [Google Scholar] [CrossRef]

{kind=link}
| Variable | (n) | OW (Including OB) | OB | |||
|---|---|---|---|---|---|---|
| % | OR (CI) | % | OR (CI) | |||
| Gender | Boys | (592) | 31.9 | 1.38 (1.07–1.78) | 20.1 | 1.83 (1.33–2.53) |
| Girls | (572) | 25.4 | - | 12.1 | ||
| Age | 6 years | (459) | 29.6 | 1.08 (0.83–1.40) | 17.0 | 1.11 (0.81–1.52) |
| 7 years | (401) | 26.9 | - | 15.2 | - | |
| 8 years | (304) | 29.6 | - | 16.1 | - | |
| Area of residence | North | (477) | 25.6 | 0.77 (0.59–1.00) | 14.5 | 0.81 (0.59–1.11) |
| Centre–South | (687) | 30.9 | - | 17.3 | - | |
| Variable | (n) | OW (Including OB) | OB | |||
|---|---|---|---|---|---|---|
| % | OR (CI) | % | OR (CI) | |||
| Mother’s Nation of Birth | Outside Italy | (180) | 38.9 | 1.74 (1.25–2.41) | 20.6 | 1.43 (0.96–2.13) |
| Italy | (984) | 26.8 | - | 15.3 | - | |
| Father’s Nation of Birth | Outside Italy | (138) | 35.5 | 1.43 (1.00–2.08) | 20.3 | 1.38 (0.88–2.15) |
| Italy | (1026) | 27.8 | - | 15.6 | - | |
| Mother’s Level of Education | University Degree | (563) | 24.9 | 0.70 (0.54–0.90) | 13.9 | 0.72 (0.52–0.98) |
| High School or Lower | (600) | 32.1 | - | 18.3 | - | |
| Father’s Level of Education | University Degree | (457) | 24.5 | 0.72 (0.55–0.94) | 12.0 | 0.59 (0.42–0.83) |
| High School or Lower | (689) | 31.0 | - | 18.7 | - | |
| Mother Employed | Yes | (853) | 29.3 | 1.13 (0.85–1.52) | 16.3 | 1.04 (0.73–1.48) |
| No | (310) | 26.8 | - | 15.8 | - | |
| Father Employed | Yes | (1022) | 28.7 | 1.16 (0.76–1.77) | 16.2 | 1.14 (0.68–1.92) |
| No | (124) | 25.8 | - | 14.5 | - | |
| Mother’s Occupation | Level I 1 | (272) | 23.9 | 0.67 (0.48–0.93) | 9.9 | 0.46 (0.30–0.72) |
| Level II 2 | (389) | 30.1 | - | 18.5 | - | |
| Level III 3 | (192) | 35.4 | - | 20.8 | - | |
| Father’s Occupation | Level I 1 | (427) | 23.7 | 0.64 (0.49–0.85) | 12.2 | 0.58 (0.41–0.83) |
| Level II 2 | (279) | 32.3 | - | 19.0 | - | |
| Level III 3 | (315) | 32.7 | - | 19.4 | - | |
| Mother Smoker | Yes | (227) | 33.9 | 1.36 (1.00–1.86) | 24.2 | 1.93 (1.36–2.75) |
| No | (936) | 27.4 | - | 14.2 | - | |
| Father Smoker | Yes | (323) | 32.2 | 1.28 (0.97–1.70) | 21.7 | 1.72 (1.24–2.39) |
| No | (822) | 27.0 | - | 13.9 | - | |
| Variable | (n) | OW (Including OB) | OB | |||
|---|---|---|---|---|---|---|
| % | OR (CI) | % | OR (CI) | |||
| Level of Traffic near the Home | Heavy | (460) | 27.6 | 0.92 (0.71–1.19) | 15.7 | 0.94 (0.68–1.30) |
| Moderate or Light | (704) | 29.4 | - | 16.5 | - | |
| Level of Traffic near the School | Heavy | (603) | 29.5 | 1.09 (0.84–1.40) | 17.1 | 1.15 (0.84–1.58) |
| Moderate or Light | (561) | 27.8 | - | 15.2 | - | |
| Variable | (n) | OW (Including OB) | OB | |||
|---|---|---|---|---|---|---|
| % | OR (CI) | % | OR (CI) | |||
| Sport (≥3 Times/Week) | Yes | (522) | 31.0 | 1.23 (0.95–1.59) | 18.2 | 1.31 (0.96–1.79) |
| No | (642) | 26.8 | - | 14.5 | - | |
| Outdoor Sports | Yes | (329) | 28.3 | 0.97 (0.73–1.29) | 16.1 | 1.00 (0.70–1.41) |
| No | (835) | 28.9 | - | 16.2 | - | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grassi, T.; De Donno, A.; Bagordo, F.; Serio, F.; Piscitelli, P.; Ceretti, E.; Zani, C.; Viola, G.C.V.; Villarini, M.; Moretti, M.; et al. Socio-Economic and Environmental Factors Associated with Overweight and Obesity in Children Aged 6–8 Years Living in Five Italian Cities (the MAPEC_LIFE Cohort). Int. J. Environ. Res. Public Health 2016, 13, 1002. https://doi.org/10.3390/ijerph13101002
Grassi T, De Donno A, Bagordo F, Serio F, Piscitelli P, Ceretti E, Zani C, Viola GCV, Villarini M, Moretti M, et al. Socio-Economic and Environmental Factors Associated with Overweight and Obesity in Children Aged 6–8 Years Living in Five Italian Cities (the MAPEC_LIFE Cohort). International Journal of Environmental Research and Public Health. 2016; 13(10):1002. https://doi.org/10.3390/ijerph13101002
Chicago/Turabian StyleGrassi, Tiziana, Antonella De Donno, Francesco Bagordo, Francesca Serio, Prisco Piscitelli, Elisabetta Ceretti, Claudia Zani, Gaia C. V. Viola, Milena Villarini, Massimo Moretti, and et al. 2016. "Socio-Economic and Environmental Factors Associated with Overweight and Obesity in Children Aged 6–8 Years Living in Five Italian Cities (the MAPEC_LIFE Cohort)" International Journal of Environmental Research and Public Health 13, no. 10: 1002. https://doi.org/10.3390/ijerph13101002