Mental Health Disturbances and Related Problems in Italian University Medical Students from 2000 to 2020: An Integrative Review of Qualitative and Quantitative Studies


 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
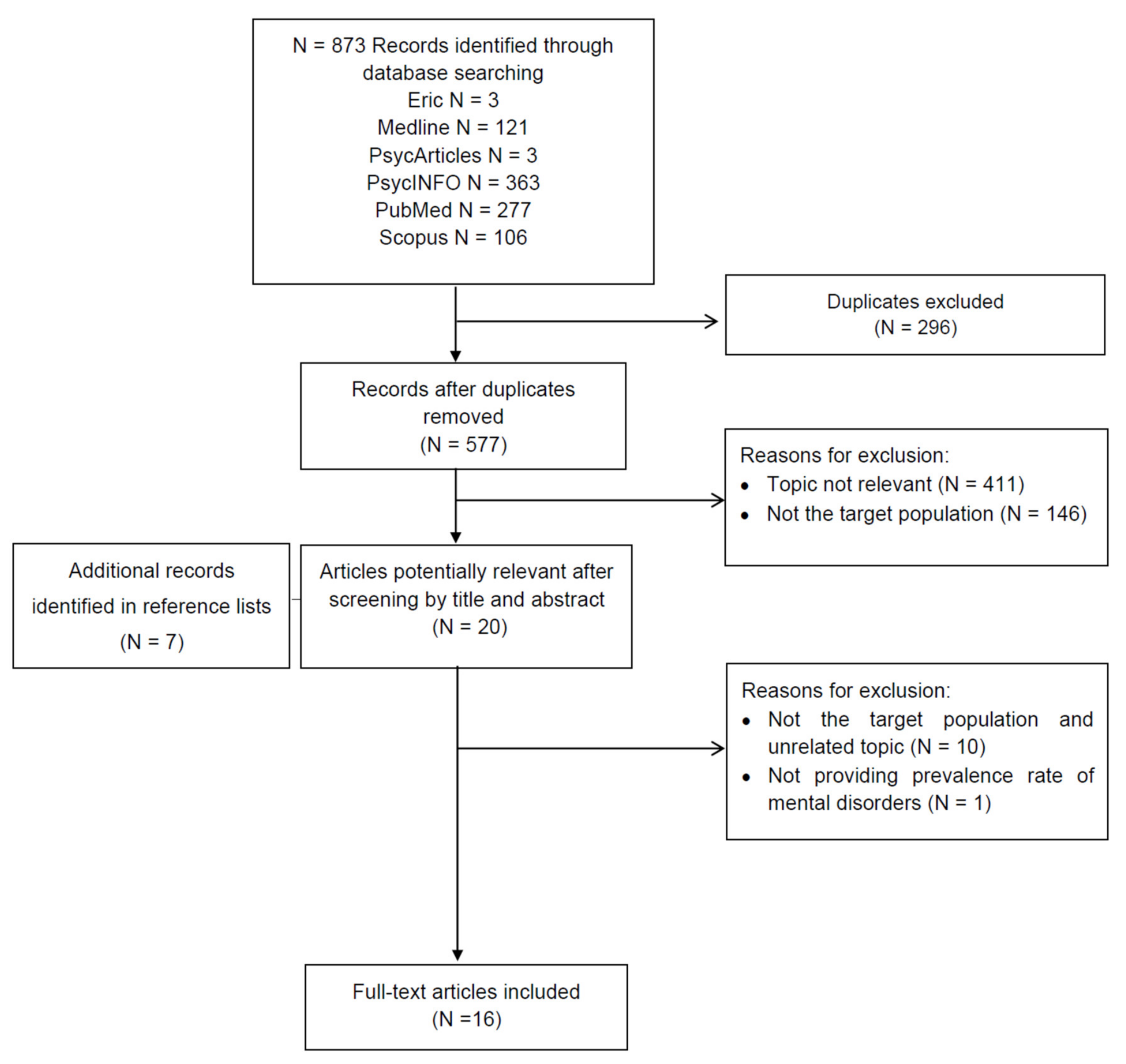
2.1. Selection of Study and Data Extraction
2.2. Quality Assessment According to the GRADE Criteria
3. Results
Summary of Design Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Auerbach, R.P.; Mortier, P.; Bruffaerts, R.; Alonso, J.; Benjet, C.; Cuijpers, P.; Demyttenaere, K.; Ebert, D.D.; Green, J.G.; Hasking, P.; et al. WHO World Mental Health Surveys International College Student Project: Prevalence and distribution of mental disorders. J. Abnorm. Psychol. 2018, 127, 623–638. [Google Scholar] [CrossRef] [PubMed]
- Taylor, Z.; Doane, L.; Eisenberg, N. Transitioning from high school to college: Relations of social support, ego-resiliency, and maladjustment during emerging adulthood. Emerg. Adulthood 2013, 2, 105–115. [Google Scholar] [CrossRef]
- Rotenstein, L.S.; Ramos, M.A.; Torre, M.; Bradley Segal, J.; Peluso, M.J.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students a systematic review and meta-analysis. JAMA J. Am. Med. Assoc. 2016, 316, 2214–2236. [Google Scholar] [CrossRef] [PubMed]
- Mousa, O.Y.; Dhamoon, M.S.; Lander, S.; Dhamoon, A.S. The MD Blues: Under-Recognized depression and anxiety in medical trainees. PLoS ONE 2016, 11, e0156554. [Google Scholar] [CrossRef] [PubMed]
- Moutinho, I.L.D.; Lucchetti, A.L.G.; da Ezequiel, O.S.; Lucchetti, G. Mental health and quality of life of Brazilian medical students: Incidence, prevalence, and associated factors within two years of follow-up. Psychiatry Res. 2019, 274, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Agnafors, S.; Barmark, M.; Sydsjö, G. Mental health and academic performance: A study on selection and causation effects from childhood to early adulthood. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 1–10. [Google Scholar] [CrossRef]
- Lemola, S.; Perkinson-Gloor, N.; Brand, S.; Dewald-Kaufmann, J.; Grob, A. Adolescents’ electronic media use at night, sleep disturbance, and depressive symptoms in the smartphone age. J. Youth Adolesc. 2015, 44, 405–418. [Google Scholar] [CrossRef]
- Mas, A.; Nerín, I.; Barrueco, M.; Cordero, J.; Guillén, D.; Jiménez-Ruiz, C.; Sobradillo, V. Smoking habits among sixth-year medical students in spain. Arch. Bronconeumol. Engl. Ed. 2004, 40, 403–408. [Google Scholar] [CrossRef]
- Fluharty, M.; Taylor, A.E.; Grabski, M.; Munafò, M. The Association of cigarette smoking with depression and anxiety: A systematic review. Nicotine Tob. Res. 2017, 19, 3–13. [Google Scholar] [CrossRef]
- Azagba, S.; Langille, D.; Asbridge, M. An emerging adolescent health risk: Caffeinated energy drink consumption patterns among high school students. Prev. Med. 2014, 62, 54–59. [Google Scholar] [CrossRef]
- Miller, K.E. Energy drinks, race, and problem behaviors among college students. J. Adolesc. Health 2008, 43, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, J.P.G.; Humes, E.C. Personality traits, alcohol and cannabis use among medical students. Braz. J. Psychiatry 2020, 42, 121. [Google Scholar] [CrossRef] [PubMed]
- Gold, J.A.; Johnson, B.; Leydon, G.; Rohrbaugh, R.M.; Wilkins, K.M. Mental health self-care in medical students: A comprehensive look at help-seeking. Acad. Psychiatry 2015, 39, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.S.; Edwards, M.L. Suffering in silence: Mental health stigma and physicians’ licensing fears. Am. J. Psychiatry Resid. J. 2018, 1, 1–4. [Google Scholar] [CrossRef]
- Deb, T.; Lempp, H.; Bakolis, I.; Vince, T.; Waugh, W.; Henderson, C.; INDIGO READ Study Group. Responding to experienced and anticipated discrimination (READ): Anti-stigma training for medical students towards patients with mental illness -study protocol for an international multisite non-randomised controlled study. BMC Med. Educ. 2019, 19, 41. [Google Scholar] [CrossRef]
- Pingani, L.; Catellani, S.; Del Vecchio, V.; Sampogna, G.; Ellefson, S.E.; Rigatelli, M.; Fiorillo, A.; Evans-Lacko, S.; Corrigan, P.W. Stigma in the context of schools: Analysis of the phenomenon of stigma in a population of university students. BMC Psychiatry 2016, 9, 29. [Google Scholar] [CrossRef]
- Thornicroft, G.; Bakolis, I.; Evans-Lacko, S.; Gronholm, P.C.; Henderson, C.; Kohrt, B.A.; Koschorke, M.; Milenova, M.; Semrau, M.; Votruba, N.; et al. Key lessons learned from the INDIGO global network on mental health related stigma and discrimination. World Psychiatry 2019, 18, 229–230. [Google Scholar] [CrossRef]
- Munizza, C.; Argentero, P.; Coppo, A.; Tibaldi, G.; Di Giannantonio, M.; Picci, R.L.; Rucci, P. Public beliefs and attitudes towards depression in Italy: A national survey. PLoS ONE 2013, 8, e63806. [Google Scholar] [CrossRef]
- Volpe, U.; Luciano, M.; Palumbo, C.; Sampogna, G.; Del Vecchio, V.; Fiorillo, A. Risk of burnout among early career mental health professionals. J. Psychiatr. Ment. Health Nurs. 2014, 21, 774–781. [Google Scholar] [CrossRef]
- Sacchini, D.; Antico, L. The professional autonomy of the medical doctor in Italy. Theor. Med. Bioeth. 2000, 21, 441–456. [Google Scholar] [CrossRef]
- Volpe, U.; Ventriglio, A.; Bellomo, A.; Kadhum, M.; Lewis, T.; Molodynski, A.; Sampogna, G.; Fiorillo, A. Mental health and wellbeing among Italian medical students: A descriptive study. Int. Rev. Psychiatry 2019, 31, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 3, e123–e130. [Google Scholar]
- Ryan, R.; Hill, S. How to GRADE the Quality of the Evidence. Cochrane Consumers and Communication Group. Version 3.0. 2016. Available online: http://cccrg.cochrane.org/author-resources (accessed on 23 December 2020).
- Melani, A.S.; Verponziani, W.; Boccoli, E.; Trianni, G.; Federici, A.; Amerini, R.; Vichi, M.; Sestini, P. Tobacco smoking habits, attitudes and beliefs among nurse and medical students in Tuscany. Eur. J. Epidemiol. 2000, 16, 607–611. [Google Scholar] [CrossRef]
- Oteri, A.; Salvo, F.; Caputi, A.P.; Calapai, G. Intake of energy drinks in association with alcoholic beverages in a cohort of students of the school of medicine of the university of Messina. Alcohol. Clin. Exp. Res. 2007, 31, 1677–1680. [Google Scholar] [CrossRef]
- Lucenteforte, E.; Vannacci, A.; Cipollini, F.; Gori, A.; Santini, L.; Franchi, G.; Terrone, R.; Ravaldi, C.; Mugelli, A.; Gensini, G.F.; et al. Smoking habits among university students in Florence: Is a medical degree course the right choice? Prev. Med. 2010, 51, 429–430. [Google Scholar] [CrossRef]
- Gualano, M.R.; Siliquini, R.; Manzoli, L.; Firenze, A.; Cattaruzza, M.S.; Bert, F.; Renzi, D.; Romano, N.; Ricciardi, W.; Boccia, A.; et al. Tobacco use prevalence, knowledge and attitudes, and tobacco cessation training among medical students: Results of a pilot study of Global Health Professions Students Survey (GHPSS) in Italy. J. Public Health 2012, 20, 89–94. [Google Scholar] [CrossRef]
- Saulle, R.; Bontempi, C.; Baldo, V.; Boccia, G.; Bonaccorsi, G.; Brusaferro, S.; Donato, F.; Firenze, A.; Gregorio, P.; Pelissero, G.; et al. GHPSS Multicenter Italian Survey: Smoking Prevalence, Knowledge and Attitudes, and Tobacco Cessation Training among Third-Year Medical Students. Tumori J. 2013, 99, 17–22. [Google Scholar] [CrossRef]
- Grassi, M.C.; Chiamulera, C.; Baraldo, M.; Culasso, F.; Ferketich, A.K.; Raupach, T.; Patrono, C.; Nencini, P. Cigarette smoking knowledge and perceptions among students in four Italian medical schools. Nicotine Tob. Res. 2012, 14, 1065–1072. [Google Scholar] [CrossRef]
- Lamberti, M.; Napolitano, F.; Napolitano, P.; Arnese, A.; Crispino, V.; Panariello, G.; Di Giuseppe, G. Prevalence of alcohol use disorders among under- and post-graduate healthcare students in Italy. PLoS ONE 2017, 12, e0175719. [Google Scholar] [CrossRef]
- Armstrong, G.W.; Veronese, G.; George, P.F.; Montroni, I.; Ugolini, G. Assessment of tobacco habits, attitudes, and education among medical students in the United States and Italy: A cross-sectional survey. J. Prev. Med. Public Health 2017, 50, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Casuccio, A.; Bonanno, V.; Catalano, R.; Cracchiolo, M.; Giugno, S.; Sciuto, V.; Immordino, P. Knowledge, attitudes, and practices on energy drink consumption and side effects in a cohort of medical students. J. Addict. Dis. 2015, 34, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Luca, M.; Ruta, S.; Signorelli, M.; Petralia, A.; Aguglia, E. Psychological variables and alcohol consumption in a sample of students of medicine: Gender differences. Riv. Psichiatr. 2015, 50, 38–42. [Google Scholar] [PubMed]
- La Torre, G.; Kirch, W.; Bes-Rastrollo, M.; Ramos, R.M.; Czaplicki, M.; Gualano, M.R.; Thümmler, K.; Ricciardi, W.; Boccia, A.; GHPSS Collaborative Group. Tobacco use among medical students in Europe: Results of a multicentre study using the Global Health Professions Student Survey. Public Health 2012, 126, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Rapinesi, C.; Kotzalidis, G.D.; Casale, A.; Del Ferrone, M.; Vento, A.; Callovini, G.; Curto, M.; Ferracuti, S.; Sani, G.; Epompili, M.; et al. Depressive symptoms, temperament/character, and attention deficit/hyperactivity disorder traits in medical students seeking counseling. Psychiatr. Danub. 2018, 30, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Solano, P.; Aguglia, A.; Caprino, M.; Conigliaro, C.; Giacomini, G.; Serafini, G.; Amore, M. The personal experience of severe suicidal behaviour leads to negative attitudes towards self- and other’s suicidal thoughts and behaviours: A study of temperaments, coping strategies, and attitudes towards suicide among medical students. Psychiatry Res. 2019, 272, 669–675. [Google Scholar] [CrossRef]
- Lia, C.; Lai, E.; Gallo, V.; Cavaggioni, G. Characteristics of a population of medical students reported to the university student counseling service “fatti vivo”. Riv. Psichiatr. 2013, 48, 162–168. [Google Scholar] [PubMed]
- Pighi, M.; Pontoni, G.; Sinisi, A.; Ferrari, S.; Mattei, G.; Pingani, L.; Simoni, E.; Galeazzi, G.M. Use and propensity to use substances as cognitive enhancers in Italian medical students. Brain Sci. 2018, 8, 197. [Google Scholar] [CrossRef]
- Cohen, K.A.; Graham, A.K.; Lattie, E.G. Aligning students and counseling centers on student mental health needs and treatment resources. J. Am. Coll. Health 2020. [Google Scholar] [CrossRef]
- Castaldelli-Maia, J.M.; Lewis, T.; Marques dos Santos, N.; Picon, F.; Kadhum, M.; Farrell, S.M.; Molodynski, A.; Ventriglio, A. Stressors, psychological distress, and mental health problems amongst Brazilian medical students. Int. Rev. Psychiatry 2019, 31, 603–607. [Google Scholar] [CrossRef]
- Gross, J.J.; Uusberg, H.; Uusberg, A. Mental illness and well-being: An affect regulation perspective. World Psychiatry 2019, 18, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Puras, D.; Gooding, P. Mental health and human rights in the 21st century. World Psychiatry 2019, 18, 42–43. [Google Scholar] [CrossRef] [PubMed]
- Castaldelli-Maia, J.M.; Martins, S.S.; Bhugra, D.; Machado, M.P.; De Andrade, A.G.; Alexandrino-Silva, C.; Baldassin, S.; Alves, T.C.D.T.F. Does ragging play a role in medical student depression—Cause or effect? J. Affect. Disord. 2012, 139, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Torales, J.; Kadhum, M.; Zárate, G.; Barrios, I.; González, I.; Farrell, S.M.; Ventriglio, A.; Arce, A. Wellbeing and mental health among medical students in Paraguay. Int. Rev. Psychiatry 2019, 31, 598–602. [Google Scholar] [CrossRef]
- Cook, A.F.; Arora, V.M.; Rasinski, K.A.; Curlin, F.A.; Yoon, J.D. The prevalence of medical student mistreatment and its association with burnout. Acad. Med. 2014, 89, 749–754. [Google Scholar] [CrossRef]
- Milic, M.; Gazibara, T.; Pekmezovic, T.; Tepavcevic, D.K.; Maric, G.; Popovic, A.; Stevanovic, J.; Patil, K.H.; Levine, H. Tobacco smoking and health-related quality of life among university students: Mediating effect of depression. PLoS ONE 2020, 8, e0227042. [Google Scholar] [CrossRef]
- Oquendo, M.A.; Bernstein, C.A.; Mayer, L.E.S. A Key differential diagnosis for physicians—Major depression or burnout? JAMA Psychiatry 2019, 76, 1111–1112. [Google Scholar] [CrossRef]
- Pacheco, J.P.; Giacomin, H.T.; Tam, W.W.; Ribeiro, T.B.; Arab, C.; Bezerra, I.M.; Pinasco, G.C. Mental health problems among medical students in Brazil: A systematic review and meta-analysis. Braz. J. Psychiatry 2017, 39, 369–378. [Google Scholar] [CrossRef]
- Pedrelli, P.; Nyer, M.; Yeung, A.; Zulauf, C.; Wilens, T. College students: Mental health problems and treatment considerations. Acad. Psychiatry 2015, 39, 503–511. [Google Scholar] [CrossRef]
- McGorry, P.; Trethowan, J.; Rickwood, D. Creating headspace for integrated youth mental health care. World Psychiatry 2019, 18, 140–141. [Google Scholar] [CrossRef]
- Jackson, E.R.; Shanafelt, T.D.; Hasan, O.; Satele, D.V.; Dyrbye, L.N. Burnout and alcohol abuse/dependence among U.S. medical students. Acad. Med. 2016, 91, 1251–1256. [Google Scholar] [CrossRef] [PubMed]
- Panatto, D.; Amicizia, D.; Domnich, A.; Lai, P.L.; Cristina, M.L.; Signori, A.; Boccalini, S.; Sulaj, K.; Gasparini, R. Tobacco smoking among students in an urban area in northern Italy. J. Prev. Med. Hyg. 2013, 54, 97–103. [Google Scholar] [PubMed]
- Niu, L.; Liu, Y.; Luo, D.; Xiao, S. Current smoking behavior among medical students in Mainland China: A systematic review and meta-analysis. Asia Pac. J. Public Health 2018, 30, 610–623. [Google Scholar] [CrossRef] [PubMed]
- Lugo, A.; Zuccaro, P.; Pacifici, R.; Gorini, G.; Colombo, P.; La Vecchia, C.; Gallus, S. Smoking in Italy in 2015–2016: Prevalence, trends, roll-your-own cigarettes, and attitudes towards incoming regulations. Tumori 2017, 103, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Bassols, A.M.S.; Carneiro, B.B.; Guimarães, G.C.; Okabayashi, L.M.S.; Carvalho, F.G.; da Silva, A.B.; Cortes, G.N.; Rohde, L.A.P.; Eizirik, C.L. Stress and coping in a sample of medical students in Brazil. Rev. Psiquiatr. Clin. 2015, 42, 1–5. [Google Scholar] [CrossRef][Green Version]
- Lesiewska, N.; Borkowska, A.; Junik, R.; Kamińska, A.; Pulkowska-Ulfig, J.; Tretyn, A.; Bieliński, M. The association between affective temperament traits and dopamine genes in obese population. Int. J. Mol. Sci. 2019, 20, 1847. [Google Scholar] [CrossRef] [PubMed]
- Fico, G.; Luciano, M.; Sampogna, G.; Zinno, F.; Steardo, L., Jr.; Perugi, G.; Pompili, M.; Tortorella, A.; Volpe, U.; Fiorillo, A. Validation of the brief TEMPS-M temperament questionnaire in a clinical Italian sample of bipolar and cyclothymic patients. J. Affect. Disord. 2020, 260, 458–462. [Google Scholar] [CrossRef]
- Patel, V.; Burns, J.K.; Dhingra, M.; Tarver, L.; Kohrt, B.A.; Lund, C. Income inequality and depression: A systematic review and meta-analysis of the association and a scoping review of mechanisms. World Psychiatry 2018, 17, 76–89. [Google Scholar] [CrossRef]
- Erbuto, D.; Innamorati, M.; Lamis, D.A.; Berardelli, I.; Forte, A.; De Pisa, E.; Migliorati, M.; Serafini, G.; Gonda, X.; Rihmer, Z.; et al. Mediators in the association between affective temperaments and suicide risk among psychiatric inpatients. Psychiatry 2018, 81, 240–257. [Google Scholar] [CrossRef]
- Widiger, T.A.; Crego, C. The five factor model of personality structure: An update. World Psychiatry 2019, 18, 271–272. [Google Scholar] [CrossRef]
- Batty, G.D.; Gale, C.R.; Tanji, F.; Gunnell, D.; Kivimäki, M.; Tsuji, I.; Jokela, M. Personality traits and risk of suicide mortality: Findings from a multi-cohort study in the general population. World Psychiatry 2018, 17, 371–372. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Karyotaki, E.; Reijnders, M.; Purgato, M.; Barbui, C. Psychotherapies for depression in low- and middle-income countries: A meta-analysis. World Psychiatry 2018, 17, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Min, J.A.; Lee, C.U.; Lee, C. Mental health promotion and illness prevention: A challenge for psychiatrists. Psychiatry Investig. 2013, 10, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J. Gender competence and mental health promotion. World Psychiatry 2020, 19, 34–35. [Google Scholar] [CrossRef] [PubMed]
- Ormel, J.; Cuijpers, P.; Jorm, A.F.; Schoevers, R. Prevention of depression will only succeed when it is structurally embedded and targets big determinants. World Psychiatry 2019, 18, 111–112. [Google Scholar] [CrossRef] [PubMed]
- Campos, R.C.; Holden, R.R.; Costa, F.; Oliveira, A.R.; Abreu, M.; Fresca, N. The moderating effect of gender on the relationship between coping and suicide risk in a Portuguese community sample of adults. J. Ment. Health 2017, 26, 66–73. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Blacker, C.J.; Lewis, C.P.; Swintak, C.C.; Bostwick, J.M.; Rackley, S.J. Medical Student Suicide Rates: A Systematic Review of the Historical and International Literature. Acad. Med. 2019, 94, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Masten, A.S. Resilience from a developmental systems perspective. World Psychiatry 2019, 18, 101–102. [Google Scholar] [CrossRef]
- Center, C.; Davis, M.; Detre, T.; Ford, D.E.; Hansbrough, W.; Hendin, H.; Laszlo, J.; Litts, D.A.; Mann, J.; Mansky, P.A. Confronting depression and suicide in physicians: A Consensus Statement. J. Am. Med. Assoc. 2003, 289, 3161–3166. [Google Scholar] [CrossRef]
- Rosenthal, J.M.; Okie, S. White coat, mood indigo—Depression in medical school. N. Engl. J. Med. 2005, 353, 1085–1088. [Google Scholar] [CrossRef]
- Dawson, K.S.; Watts, S.; Carswell, K.; Shehadeh, M.H.; Jordans, M.J.D.; Bryant, R.A.; Miller, K.E.; Malik, A.; Brown, F.L.; Servili, C.; et al. Improving access to evidence-based interventions for young adolescents: Early Adolescent Skills for Emotions (EASE). World Psychiatry 2019, 18, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Sinha, M.; Collins, P.; Herrman, H. Collective action for young people’s mental health: The cities RISE experience. World Psychiatry 2019, 18, 114–115. [Google Scholar] [CrossRef] [PubMed]
- Pinna, F.; Del Vecchio, V.; Luciano, M.; Sampogna, G.; De Rosa, C.; Ferrari, S.; Luca, P.; Ilaria, T.; Umberto, V.; Carrà, G.; et al. Shall psychiatry change its target? Reflections on the evolving role of psychiatry. Riv. Psichiatr. 2015, 50, 3–7. [Google Scholar] [PubMed]
- Fiorillo, A.; Malik, A.; Luciano, M.; Del Vecchio, V.; Sampogna, G.; Del Gaudio, L.; Kuzman, M.R.; Jovanovic, N.; Nawka, A.; Volpe, U. Challenges for trainees in psychiatry and early career psychiatrists. Int. Rev. Psychiatry 2013, 25, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, A.; Luciano, M.; Del Vecchio, V.; Sampogna, G.; Obradors-Tarragó, C.; Maj, M.; ROAMER Consortium. Priorities for mental health research in Europe: A survey among national stakeholders’ associations within the ROAMER project. World Psychiatry 2013, 12, 165–1670. [Google Scholar] [CrossRef] [PubMed]
- Pompili, M.; Fiorillo, A. Editorial: Unmet Needs in Modern Psychiatry. CNS Neurol. Disord. 2017, 16, 857. [Google Scholar] [CrossRef] [PubMed]
- Pinto da Costa, M.; Dima, K.; Ng, R.M.K. Undergraduate psychiatric education: A snapshot of medical students across the world. World Psychiatry 2019, 18, 243–244. [Google Scholar] [CrossRef]
- Whitley, R.; Shepherd, G.; Slade, M. Recovery colleges as a mental health innovation. World Psychiatry 2019, 18, 141–142. [Google Scholar] [CrossRef]
- Hanna, F.; Barbui, C.; Dua, T.; Lora, A.; van Regteren Altena, M.; Saxena, S. Global mental health: How are we doing? World Psychiatry 2018, 17, 367–368. [Google Scholar] [CrossRef]


{kind=link}
| Search Terms | Eric | Medline | Psyc Articles | Psyc INFO | PubMed | Scopus |
|---|---|---|---|---|---|---|
| Students, medical AND mental health AND Italy | 0 | 77 | 2 | 105 | 62 | 29 |
| Students, medical AND mental disorders AND Italy | 0 | 18 | 0 | 77 | 76 | 22 |
| Students, medical AND depression AND Italy | 1 | 5 | 0 | 50 | 30 | 12 |
| Students, medical AND anxiety AND Italy | 1 | 6 | 0 | 50 | 27 | 16 |
| Students, medical AND suicidal ideation AND Italy | 0 | 0 | 0 | 10 | 6 | 2 |
| Students, medical AND Suicide attempted AND Italy | 0 | 0 | 0 | 8 | 4 | 1 |
| Students, medical AND suicide AND Italy | 1 | 3 | 0 | 23 | 22 | 8 |
| Students, medical AND Alcoholism AND Italy | 0 | 1 | 1 | 6 | 2 | 6 |
| Students, medical AND street drugs AND Italy | 0 | 2 | 0 | 3 | 2 | 3 |
| Students, medical AND mental disorders AND Italy AND prevalence | 0 | 8 | 0 | 18 | 34 | 3 |
| Students, medical AND “mental disorders” AND Italy AND “risk factors” | 0 | 1 | 0 | 13 | 12 | 4 |
| Author(s), Year | Study Design | Sample Size, Site(s) | Mean Age | Gender | Assessment Tool(s) | Main Aim(s) | Data Collection and Response Rate | Prevalence | Main Findings | Main Conclusions | Study Limitations | GRADE Criteria |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Volpe et al. 2019 | Cross-sectional | N = 360, Ancona, Foggia | Not reported | F: 58.33% M: 41.67% | Oldenburgh Burnout Inventory (OLBI); General Health Questionnaire (GHQ); CAGE (Cutdown/Annoyed/Guilty/Eye Opener) | To evaluate the general health and the levels of burnout | Online survey, invitation through institutional email to all university’s students. Response rate: Ancona 88.6%; Foggia: 11.4% | 5%: anxiety disorder 2.5%: depression 0.28%: burnout syndrome 8.9%: alcohol related problems 33%: cognitive enhancers users | 8.6% of participants reported mental health issues whilst at medical school, ranking as follows: Anxiety Disorders > Major Depression > Eating Disorders > ADHD > Burnout Syndrome. | The finding show that a certain percentage of Italian Medical students present psychological conditions with alcohol misuse and use of drugs to cope with their condition | Online survey; self-reporter instruments | MODERATE |
| Solano et al. 2019 | Cross-sectional | N = 522, Genoa | 23.6 ± 1.1 years | F:59% M: 41% | Suicide Opinion Questionnaire (SOQ); Coping Orientation to Problem Experienced (COPE); Temperament Evaluation of the Memphis (TEMPS-A) | To evaluate the presence of suicidal thoughts/behaviors, coping strategies, temperament and attitude towards suicidality in medical students | Collection during classrooms activities from medical students Response rate: 82.3% | 17%: severe suicidal thought and behavior | The participants with poor coping strategies were more likely to be males, with poor academic achievement and less likely to have a parent working in medical or mental health fields. | The clinicians need to consider the complex interplay of clinical features present in medical students with severe suicidal behavior | Self-reported questionnaire; cross-sectional study | MODERATE |
| Pighi et al. 2018 | Cross-sectional | N = 433, Modena and Reggio Emilia | 22.4 years; Range: 18–48 years | F: 55.9% M: 44.1% | 36-item ad-hoc validated questionnaire | To evaluate the prevalence of use of energy drinks and students’ attitudes | Collection during classrooms activities from medical students Response rate: 83.8% | 74.7%: energy drinks users | Italian medical students used energy drinks and psychostimulant substances (coffee and caffeine) as cognitive enhancers very frequently | The use of psychostimulants is low and the majority of students are worried about academic performance. | Low generalizability of results; no use a standardized tool | MODERATE |
| Rapinesi et al. 2018 | Case-control | N = 98 (N = 49, help-seekers; N = 49 control group), Sapienza-Rome | 24.4 years (students seeking counseling); 21.7 years (non counseling controls) | Not reported | Beck Depression Inventory-II; Temperament and Character Inventory-Revised; Adult ADHD Self-Report Scale | To evaluate temperament, attention deficit/hyperactivity disorder traits and depressive symptomatology | Students attending 6-year of medical school and/or attending the counseling program Response rate: not available | 17.1%: depressive symptoms in help-seeking group 10.1%: depressive symptoms in control group (p < 0.001) ADHD total score: 3.7 (help-seeking group) vs. 2.5 (control group) (p < 0.001) | Help-seeking students were more likely to have attention deficit/hyperactivity symptoms, scored higher on the Beck Depression Inventory-II and on the Temperament and Character Inventory-Revised | Medical students attending counseling center need to be carefully assessed for mental disorders | Small sample size | LOW RATE |
| Lamberti et al. 2017 | Cross-sectional | N = 641, Naples | 26.2 ± 5.5 years | F:59.1% M: 40.9% | Alcohol Use Disorders Identification Test (AUDIT -C) | To assess the prevalence of alcohol drinking in a large sample of students and residents | Collection during medical examinations in medical course students Response rate: 100% | 85.5%: regular alcohol users 16.6%: regular smokers 91%: habitual coffee consumption | Over two-thirds of the students use alcohol regularly. Medical students use alcohol more frequently than residents. Over 90% of student use coffee regularly, one out five is active smoker and less than 60% perform physical activity | The results shown a need to assess alcohol use in healthcare professionals and to recognize risky behaviors in order to develop effective preventive interventions | Cross-sectional design, not representative sample | MODERATE |
| Armstrong et al. 2017 | Multicenter cross-sectional | N = 527, Bologna | Not reported | M: 43.0% | International professional assessment of drinking and tobacco perceptions among young medical doctors | To evaluate the prevalence of medical students’ tobacco use, attitudes, clinical skills and tobacco-related curricula | Invitation through institutional email to all university’s students. Response rate: less than 40% | 29.5%: smoking habits | Italian students were less likely to receive smoking cessation training compared to American students. Students reported to want to receive smoking cessation training | There is the need to include training on smoking cessation in medical course in order to reduce smoking among medical students, physicians and patients | Recruitment bias | MODERATE |
| Casuccio et al. 2015 | Cross-sectional | N = 794, Palermo | 21.9 ± 2.7 years; Range: 19–41 | F: 52.5% M: 47.5% | Ad hoc questionnaire on consumption of energy drinks | To assess the levels of knowledge and attitudes related to energy drink consumption and the prevalence of side effects related to their use | Medical student of the 6- year course filling out the instruments during class time Response rate: 75% | 22%: energy drinks users | Female students present high levels of somatization, obsessive-compulsive, depressive and anxiety symptoms. Mental disorders are more common in students using energy drinks regularly | There is an association between specific psychopathological characteristics and alcohol consumption | Small sample, cross-sectional design | MODERATE |
| Luca et al. 2015 | Cross-sectional | N = 200, Catania | 21.8 ± 3.1 years | F: 52.5% M: 47.5% | Alcohol Use Disorders Identification Test (AUDIT-C); Self-Report Symptom Inventory-Revised (SCL-90-R); General Symptomatic Index (GSI) | To assess the levels of alcohol consumption in relation with socio-demographic and psychopathological variables in a sample of medical students | Students attending the 6-year of medical schoolAdministration of the survey during classroom activities Response rate: 75% | 27%: presence of mental health problems 13%: alcohol use disorder | Male students were most frequently regularly alcohol users 49% of participants consumed alcohol associated with energy drinks. | There is a great use of energy drinks among medical students, either alone or in combination with alcoholic beverages. | Cross-sectional design; self-reported questionnaires | LOW RATE |
| Lia et al. 2013 | Cross-sectional | N = 44, Sapienza University-Rome | Not reported | Not reported | SCID-I -CV (The Structured Clinical Interview for DSM-IV Axis I Disorders-Structured clinical Interview) | To assess the prevalence of mental disorders among medical students attending a university counseling service | Students attending 6-year of medical school and/or attending the counseling program Response rate: not available | 31.8%: axis I diagnosis 21.4%: depressive syndrome 35.7%: adaptation dis. 14.3%: psychotic dis. 7.1%: dysthymia 7.1%: anxiety 7.1%: panic attacks dis. 7.1%: bipolar dis. 7.1%: episode of mania | Services for psychological counseling targeting medical students should be present in Italian universities. | The prevalence of mental distress and mental disorder appears to be higher in medical students compared to the prevalence of the same problems in students attending other faculties | Small sample size, lack of comparison with other counseling services | VERY LOW RATE |
| Saulle et al. 2013 | Multicenter cross-sectional | N = 730, Turin, Padua, Florence, Brescia, Ferrara, Varese Udine, Palermo, Salerno | Range: 19–29 years | F: 19.1% M: 22.4% | The Global Health Professions Student Survey (GHPSS) | To evaluate smoking prevalence, knowledge and attitudes among Italian medical students | Students attending third year of medical school Survey performed during classroom activities Response rate: 100% | 20.4%: current smokers | 87.7% believed that health professionals need to receive specific training on smoking cessation. 65% believed that health professionals had a role in giving advice or information about smoking cessation. | There is a need to provide medical students with smoking cessation training | Cross-sectional study design, self-reported data, recruitment bias (only third-year students) | MODERATE |
| Grassi et al. 2012 | Cross-sectional | N = 439, Sapienza-Rome, Cattolica University-Rome, Udine, Verona | 23.3 ± 3.0 years; Range: 20–55 years | F:61% M:49% | 60-item ad-hoc validated questionnaire | To evaluate smoking behavior and to assess the levels of knowledge about smoking-related mortality, the harmful effects of cigarette smoking and the efficacy of counseling techniques | Self-administered questionnaires to students attending the course of pharmacology and toxicology Response rate: 40% | 15.3%: current smokers 9.6%: previous smoker | The levels of knowledge on epidemiological aspects of tobacco use was low. A great proportion of students did not know how to provide counselling to smokers | Italian medical students do not receive adequate training on tobacco dependence | Small sample size | MODERATE |
| Gualano et al. 2012 | Multicentre cross-sectional | N = 744, Rome, La Sapienza, Rome, Cattolica, Chieti, Turin, Palermo | Not reported | Not reported | The Global Health Professions Student Survey (GHPSS) questionnaire | To evaluate the prevalence of tobacco use, the levels of knowledge and attitudes about tobacco smoking cessation training | Self-administered questionnaires to all students interested Response rate: 98% | 31.4%: current smokers | The great majority considered health professionals as role models for patients as well as they have a role in giving advice or information about smoking cessation | It should be useful to include smoking cessation training in the Italian medical course | Cross-sectional study, self-reported data, recruitment bias (only third year students) | MODERATE |
| La Torre et al. 2012 | Multicenter cross-sectional | N = 655, Chieti, Palermo, Rome Sapienza, Rome Cattolica and Turin | 21.34 years; Range: 20–44 years | F: 50.4% M: 49,6% | Global Tobacco Surveillance System form | To assess smoking prevalence; the levels of knowledge and attitudes toward smoking; the availability of tobacco cessation training | Second semester of the third year of medical school Response rate: 92% | 29.3%: smoking habits | 57.2% of participants believe that health professionals are role models for patients. 89.8% of them are aware of smoking cessation interventions. | The prevalence of smoking was higher among medical students than the general population. The training in smoking cessation techniques need to be provided to medical students. | Cross-sectional design, lack of representativeness | MODERATE |
| Lucenteforte et al. 2010 | Cross-sectional | N = 194, Florence | Not reported | F: 65.8% M: 34.2% | Modified instrument of the World Health Organization about tobacco smoking for health caregivers | To assess the impact of university choice on smoking habits | First year students attending classroom lectures at the University of Florence Response rate: 100% | 20.1%: smoking habits | 32.5% of medical students had at least one parent who uses smoking | The medical students seem to be more conscious about the negative effects of smoking and tobacco-related diseases in comparison with other students. | Small sample size; not representative sample | LOW RATE |
| Oteri et al. 2007 | Cross-sectional | N = 450, Messina | 24.5 years; Range: 19–30 years | F: 58.7% M: 41.3% | Ad-hoc questionnaire about energy drink consumption | To evaluate the levels of knowledge related to the use of energy drinks (alone or in association with alcohol) | Anonymous survey Response rate: 90% | 56.9%: use of energy drink 48.4%: use of energy drink associated with alcohol | The use of energy drinks and alcohol is frequent. The usage combined is associated to a higher risk of developing alcohol dependence. | The consumption of alcohol and energy drinks is high in medical student population. | Not reported | LOW RATE |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sampogna, G.; Lovisi, G.M.; Zinno, F.; Del Vecchio, V.; Luciano, M.; Gonçalves Loureiro Sol, É.; Unger, R.J.G.; Ventriglio, A.; Fiorillo, A. Mental Health Disturbances and Related Problems in Italian University Medical Students from 2000 to 2020: An Integrative Review of Qualitative and Quantitative Studies. Medicina 2021, 57, 11. https://doi.org/10.3390/medicina57010011
Sampogna G, Lovisi GM, Zinno F, Del Vecchio V, Luciano M, Gonçalves Loureiro Sol É, Unger RJG, Ventriglio A, Fiorillo A. Mental Health Disturbances and Related Problems in Italian University Medical Students from 2000 to 2020: An Integrative Review of Qualitative and Quantitative Studies. Medicina. 2021; 57(1):11. https://doi.org/10.3390/medicina57010011
Chicago/Turabian StyleSampogna, Gaia, Giovanni Marcos Lovisi, Francesca Zinno, Valeria Del Vecchio, Mario Luciano, Érika Gonçalves Loureiro Sol, Roberto José Gervásio Unger, Antonio Ventriglio, and Andrea Fiorillo. 2021. "Mental Health Disturbances and Related Problems in Italian University Medical Students from 2000 to 2020: An Integrative Review of Qualitative and Quantitative Studies" Medicina 57, no. 1: 11. https://doi.org/10.3390/medicina57010011
APA StyleSampogna, G., Lovisi, G. M., Zinno, F., Del Vecchio, V., Luciano, M., Gonçalves Loureiro Sol, É., Unger, R. J. G., Ventriglio, A., & Fiorillo, A. (2021). Mental Health Disturbances and Related Problems in Italian University Medical Students from 2000 to 2020: An Integrative Review of Qualitative and Quantitative Studies. Medicina, 57(1), 11. https://doi.org/10.3390/medicina57010011