Association between Adverse Effects and Parental Beliefs about Antiepileptic Medicines



Abstract
1. Introduction
2. Methods
2.1. Patient’s Characteristics
2.2. LAEP
2.3. BMQ
2.4. Data Management and Statistical Analysis
3. Results
3.1. General Characteristics
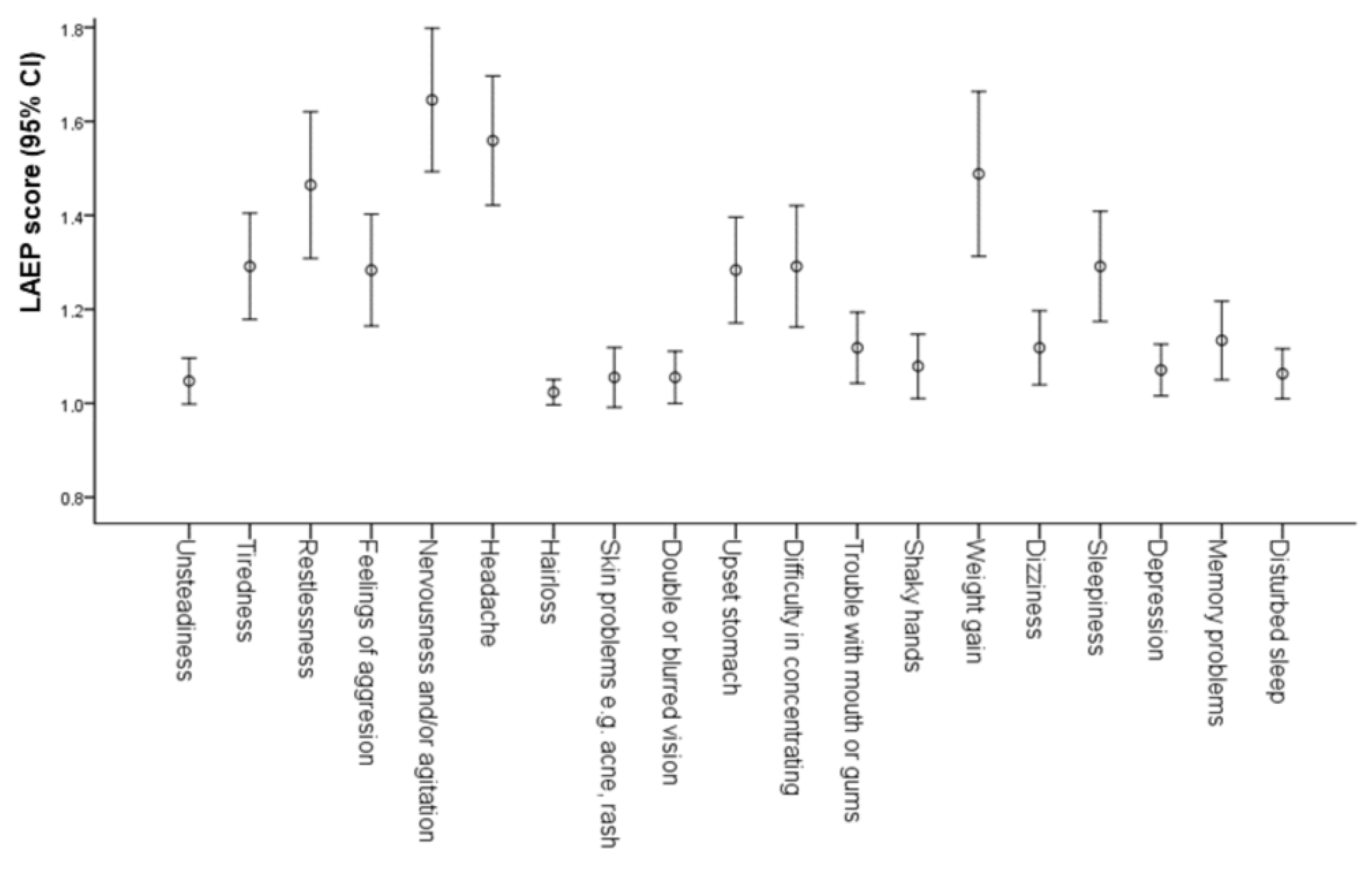
3.2. Adverse Effects
3.3. Parental Beliefs about Medications
3.4. Predictors for BMQ Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Harbord, M.G. Significant anticonvulsant side-effects in children and adolescents. J. Clin. Neurosci. 2000, 7, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Herranz, J.L.; Armijo, J.A.; Arteaga, R. Clinical side effects of phenobarbital, primidone, phenytoin, carbamazepine, and valproate during monotherapy in children. Epilepsia 1988, 29, 794–804. [Google Scholar] [CrossRef] [PubMed]
- Zeng, K.; Wang, X.; Xi, Z.; Yan, Y. Adverse effects of carbamazepine, phenytoin, valproate and lamotrigine monotherapy in epileptic adult Chinese patients. Clin. Neurol. Neurosurg. 2010, 112, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Devinsky, O.; Cramer, J. Safety and efficacy of standard and new antiepileptic drugs. Neurology 2000, 55, S5–S10. [Google Scholar] [PubMed]
- Panelli, R.J.; Kilpatrick, C.; Moore, S.M.; Matkovic, Z.; D’Souza, W.J.; O’Brien, T.J. The Liverpool adverse events profile Relation to AED use and mood. Epilepsia 2007, 48, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Abetz, L.; Jacoby, A.; Baker, G.A.; McNulty, P. Patient-based assessments of quality of life in newly diagnosed epilepsy patients: Validation of the NEWQOL. Epilepsia 2000, 41, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Baker, G.A.; Jacoby, A.; Francis, P.; Chadwick, D. The Liverpool adverse events drug profile. Epilepsia 1995, 36, 59. [Google Scholar]
- Baker, G.A. Initial development, reliability, and validity of a patient-based adverse event scale. Epilepsia 1994, 35, S20. [Google Scholar]
- Baker, G.A. Development of a patient-based symptom check list to quantify adverse events in persons receiving antiepileptic drugs. Epilepsia 1993, 34, 18. [Google Scholar]
- Kowski, A.B.; Weissinger, F.; Gaus, V.; Fidzinski, P.; Losch, F.; Holtkamp, M. Specific adverse effects of antiepileptic drugs—A true-to-life monotherapy study. Epilepsy Behav. 2016, 54, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Viteva, E. Relation of perceived stigma to adverse events of medications in patients with epilepsy. Epilepsy Res. Treat. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Elafros, M.A.; Bui, E.; Birbeck, G.L. Medication side effects among people with epilepsy taking phenobarbital in Zambia. Epilepsy Res. 2014, 108, 1680–1684. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Arias, B.; Crail-Melendez, D.; Lopez-Zapata, R.; Martinez-Juarez, I.E. Severity of anxiety and depression are related to a higher perception of adverse effects of antiepileptic drugs. Seizure 2012, 21, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Martins, H.H.; Alonso, N.B.; Vidal-Dourado, M.; Carbonel, T.D.; de Araújo Filho, G.M.; Caboclo, L.O.; Yacubian, E.M.; Guilhoto, L.M. Are adverse effects of antiepileptic drugs different in symptomatic partial and idiopathic generalized epilepsies? The Portuguese-Brazilian validation of the Liverpool Adverse Events Profile. Epilepsy Behav. 2011, 22, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Baker, G.A.; Jacoby, A.; Buck, D.; Stalgis, C.; Monnet, D. Quality of life of people with epilepsy: A European study. Epilepsia 1997, 38, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Miner, P.J.; Alexander, J.; Ewing, H.; Gerace, L. Caregivers’ beliefs associated with medication adherence among children and adolescents with epilepsy. J. Neurosci. Nurs. 2013, 45, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Nakhutina, L.; Gonzalez, J.S.; Margolis, S.A.; Spada, A.; Grant, A. Adherence to antiepileptic drugs and beliefs about medication among predominantly ethnic minority patients with epilepsy. Epilepsy Behav. 2011, 22, 584–586. [Google Scholar] [CrossRef] [PubMed]
- Bautista, R.E.D.; Jain, D. Detecting health disparities among Caucasians and African-Americans with epilepsy. Epilepsy Behav. 2011, 20, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Horne, R.; Weinman, J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J. Psychosom. Res. 1999, 47, 555–567. [Google Scholar] [CrossRef]
- Modi, A.C.; Rausch, J.R.; Glauser, T.A. Patterns of nonadherence to antiepileptic drug therapy in children with newly diagnosed epilepsy. J. Am. Med. Assoc. 2011, 305, 1669–1676. [Google Scholar] [CrossRef] [PubMed]
- Snodgrass, S.R.; Vedanarayanan, V.V.; Parker, C.C.; Parks, B.R. Pediatric patients with undetectable anticonvulsant blood levels: Comparison with compliant patients. J. Child Neurol. 2001, 16, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Gilliam, F.G.; Fessler, A.J.; Baker, G.; Vahle, V.; Carter, J.; Attarian, H. Systematic screening allows reduction of adverse antiepileptic drug effects: A randomized trial. Neurology 2004, 62, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Horne, R.; Weinman, J.; Hankins, M. The beliefs about medicines questionnaire: The development and evaluation of a new method for assessing the cognitive representation of medication. Psychol. Health 1999, 14, 1–24. [Google Scholar] [CrossRef]
- Conn, K.M.; Halterman, J.S.; Lynch, K.; Cabana, M.D. The impact of parents’ medication beliefs on asthma management. Pediatrics 2007, 120, e521–e526. [Google Scholar] [CrossRef] [PubMed]
- Conn, K.M.; Halterman, J.S.; Fisher, S.G.; Yoos, H.L.; Chin, N.P.; Szilagyi, P.G. Parental beliefs about medications and medication adherence among urban children with asthma. Ambul. Pediatr. 2005, 5, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, O.; Eroglu, N.; Ozalp, D.; Yuksel, H. Beliefs about medications in asthmatic children presenting to emergency department and their parents. J. Asthma 2012, 49, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Andrew, T.; Milinis, K.; Baker, G.; Wieshmann, U. Self reported adverse effects of mono and polytherapy for epilepsy. Seizure 2012, 21, 610–613. [Google Scholar] [CrossRef] [PubMed]
- Wieshmann, U.C.; Tan, G.M.; Baker, G. Self-reported symptoms in patients on antiepileptic drugs in monotherapy. Acta Neurol. Scand. 2011, 124, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.W.K.; DeBruyne, J.A. Parental concern towards the use of inhaled therapy in children with chronic asthma. Pediatr. Int. 2000, 42, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Loiselle, K.; Rausch, J.R.; Modi, A.C. Behavioral predictors of medication adherence trajectories among youth with newly diagnosed epilepsy. Epilepsy Behav. 2015, 50, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.C.E.; Horne, R.; Chater, A.; Hukins, D.; Smithson, W.H. Patients’ perspectives on antiepileptic medication: Relationships between beliefs about medicines and adherence among patients with epilepsy in UK primary care. Epilepsy Behav. 2014, 31, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Gazibara, T.; Nikolovski, J.; Lakic, A.; Pekmezovic, T.; Kisic-Tepavcevic, D. Parental knowledge, attitudes, and behaviors towards children with epilepsy in Belgrade (Serbia). Epilepsy Behav. 2014, 41, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Paschal, A.M.; Mitchell, Q.P.; Wilroy, J.D.; Hawley, S.R.; Mitchell, J.B. Parent health literacy and adherence-related outcomes in children with epilepsy. Epilepsy Behav. 2016, 56, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Castillo, A.; Vılchez-Lara, M. Anxiety and parent’s beliefs about medication in primary pediatric health care. Clínica y Salud 2014, 25, 117–122. [Google Scholar] [CrossRef]


{kind=link}
| Patient Characteristics | Total (N = 127) |
|---|---|
| Age, mean ± SD, years | 9.88 ± 4.16 |
| Gender, male n (%) | 64 (50.4) |
| Treatment n (%) | |
| Valproic acid | 102 (80.3) |
| Carbamazepine | 13 (10.2) |
| Lamotrigine | 12 (9.5) |
| Dose n (%) | |
| Valproic acid | |
| 20 mg/kg | 52 (51.0) |
| 25 mg/kg | 11 (10.8) |
| 30 mg/kg | 3 (2.9) |
| ≥45 kg | 36 (35.3) |
| Carbamazepine | |
| 10 mg/kg | 3 (23.1) |
| 20 mg/kg | 2 (15.4) |
| ≥45 kg | 8 (61.5) |
| Lamotrigine | |
| 3 mg/kg | 9 (75.0) |
| 4 mg/kg | 1 (8.3) |
| ≥45 kg | 2 (16.7) |
| Treatment duration, median (IQR), years | 3 (2-5) |
| Parental age, mean ± SD, years | 36 ± 12 |
| Gender, female n (%) | 106 (83.5) |
| Parental education level n (%) | |
| Primary school | 28 (22.0) |
| Secondary school | 83 (65.4) |
| University | 16 (12.6) |
| Dependent Value | Predictor | R2 | B (95% CI) | SE | p-Value |
|---|---|---|---|---|---|
| BMQ necessity | Parental education level | 0.273 | 1.13 (0.03–2.24) | 0.56 | 0.045 |
| Difficulty in concentrating | 0.273 | 1.08 (0.21–1.96) | 0.44 | 0.016 | |
| BMQ concerns | Difficulty in concentrating | 0.262 | 1.04 (0.36–1.72) | 0.34 | 0.003 |
| BMQ overuse | Headache | 0.193 | 0.70 (0.07–1.32) | 0.32 | 0.029 |
| BMQ-harm | not identified |
| Dependent Value | Predictor | R2 | B (95% CI) | SE | p-Value |
|---|---|---|---|---|---|
| BMQ necessity | Parental education level | 0.300 | 1.41 (0.20–2.63) | 0.61 | 0.023 |
| Difficulty in concentrating | 0.300 | 1.03 (0.07–1.99) | 0.49 | 0.036 | |
| BMQ concerns | Difficulty in concentrating | 0.231 | 0.86 (0.16–1.56) | 0.35 | 0.017 |
| BMQ overuse | Headache | 0.219 | 0.80 (0.11–1.51) | 0.35 | 0.024 |
| BMQ- harm | not identified |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilić, V.; Bogićević, D.; Miljković, B.; Vezmar-Kovačević, S. Association between Adverse Effects and Parental Beliefs about Antiepileptic Medicines. Medicina 2018, 54, 60. https://doi.org/10.3390/medicina54040060
Ilić V, Bogićević D, Miljković B, Vezmar-Kovačević S. Association between Adverse Effects and Parental Beliefs about Antiepileptic Medicines. Medicina. 2018; 54(4):60. https://doi.org/10.3390/medicina54040060
Chicago/Turabian StyleIlić, Violeta, Dragana Bogićević, Branislava Miljković, and Sandra Vezmar-Kovačević. 2018. "Association between Adverse Effects and Parental Beliefs about Antiepileptic Medicines" Medicina 54, no. 4: 60. https://doi.org/10.3390/medicina54040060
APA StyleIlić, V., Bogićević, D., Miljković, B., & Vezmar-Kovačević, S. (2018). Association between Adverse Effects and Parental Beliefs about Antiepileptic Medicines. Medicina, 54(4), 60. https://doi.org/10.3390/medicina54040060