Practical Judgment of Workload Based on Physical Activity, Work Conditions, and Worker’s Age in Construction Site

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
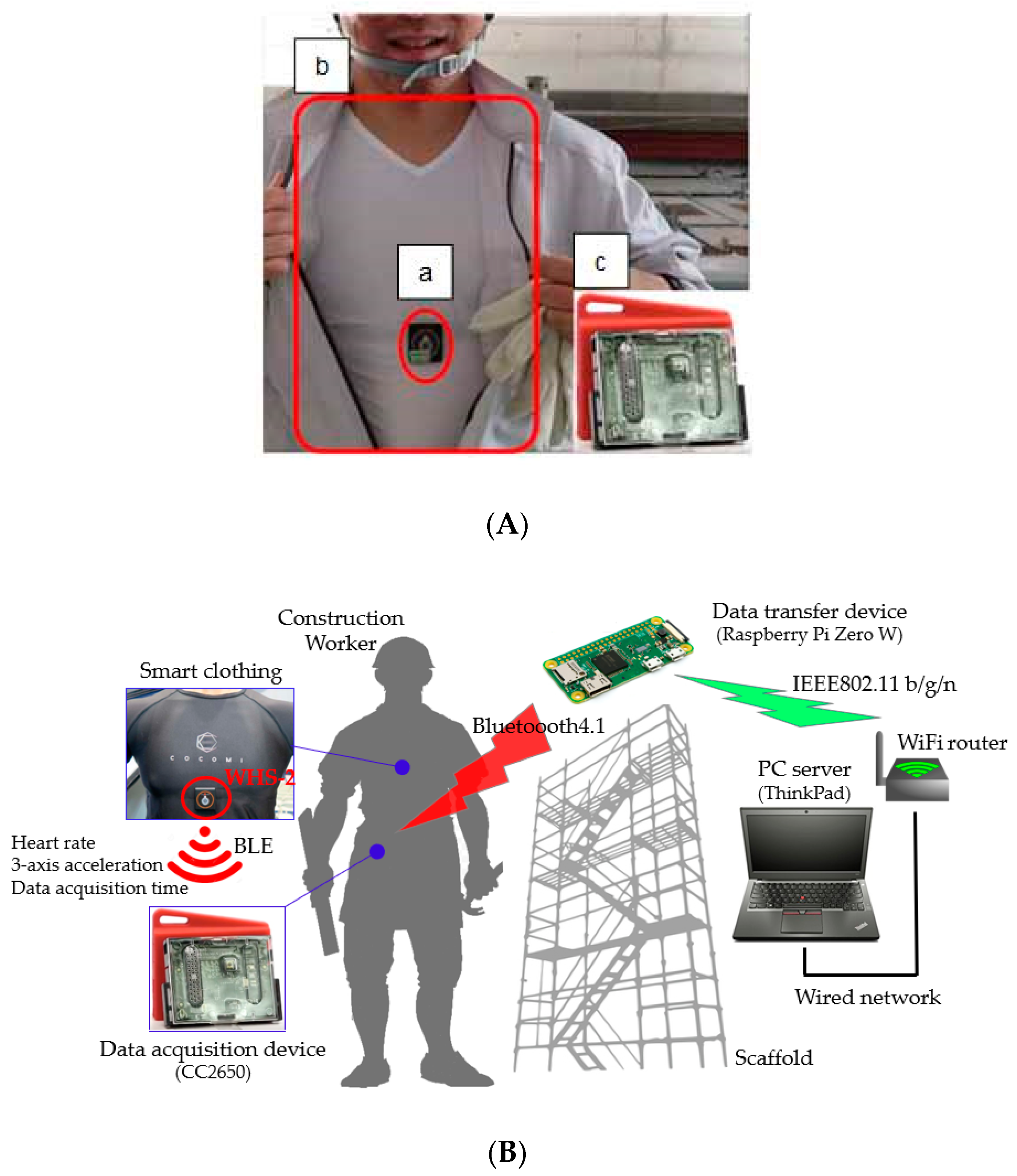
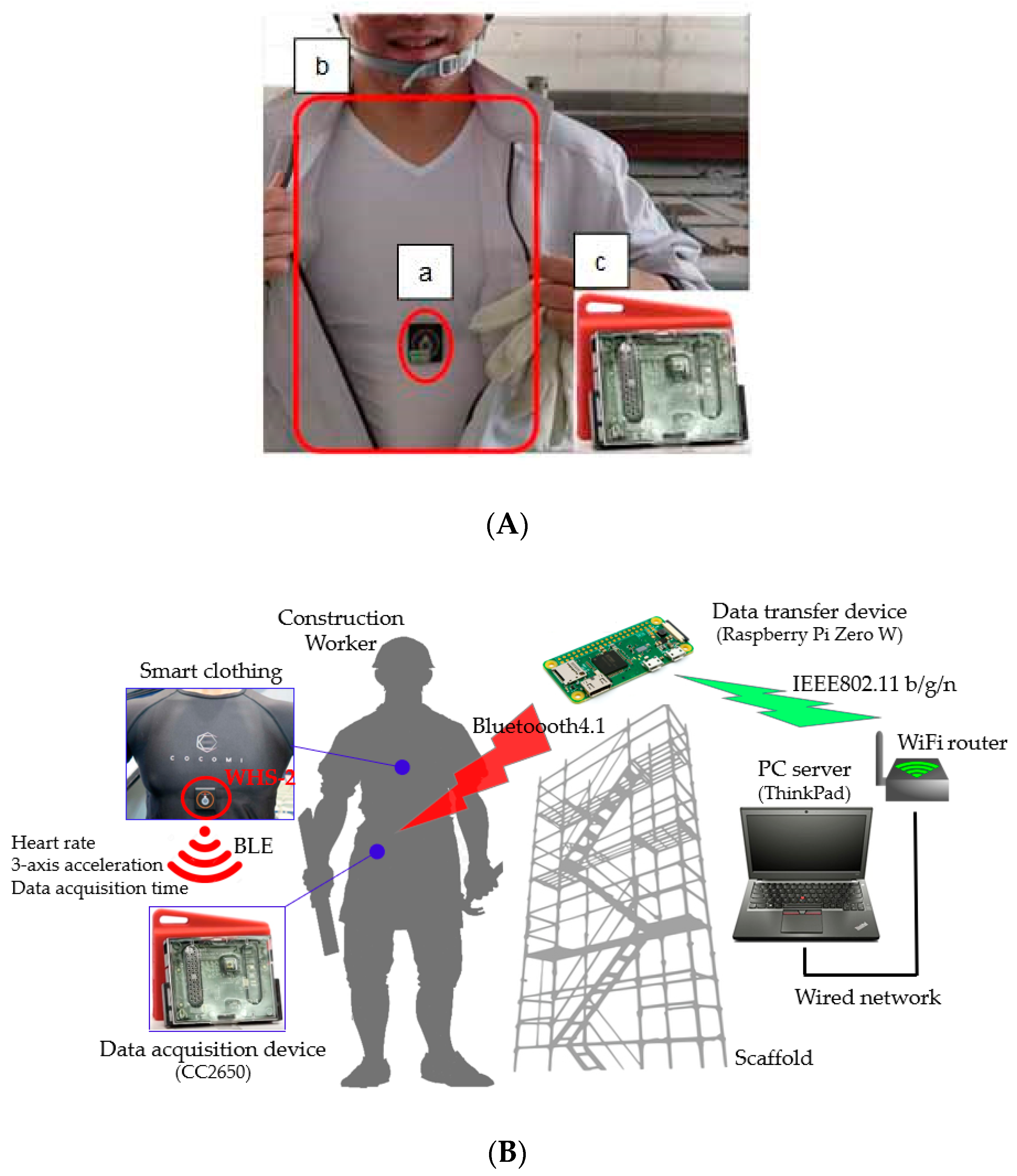
2.1. Measurement System
2.2. Measurement Method
2.3. Participants
2.4. Protocol
2.5. Data Collection
2.6. Model Development and Statistical Analysis
3. Results
3.1. Subject Characteristics and Measurements
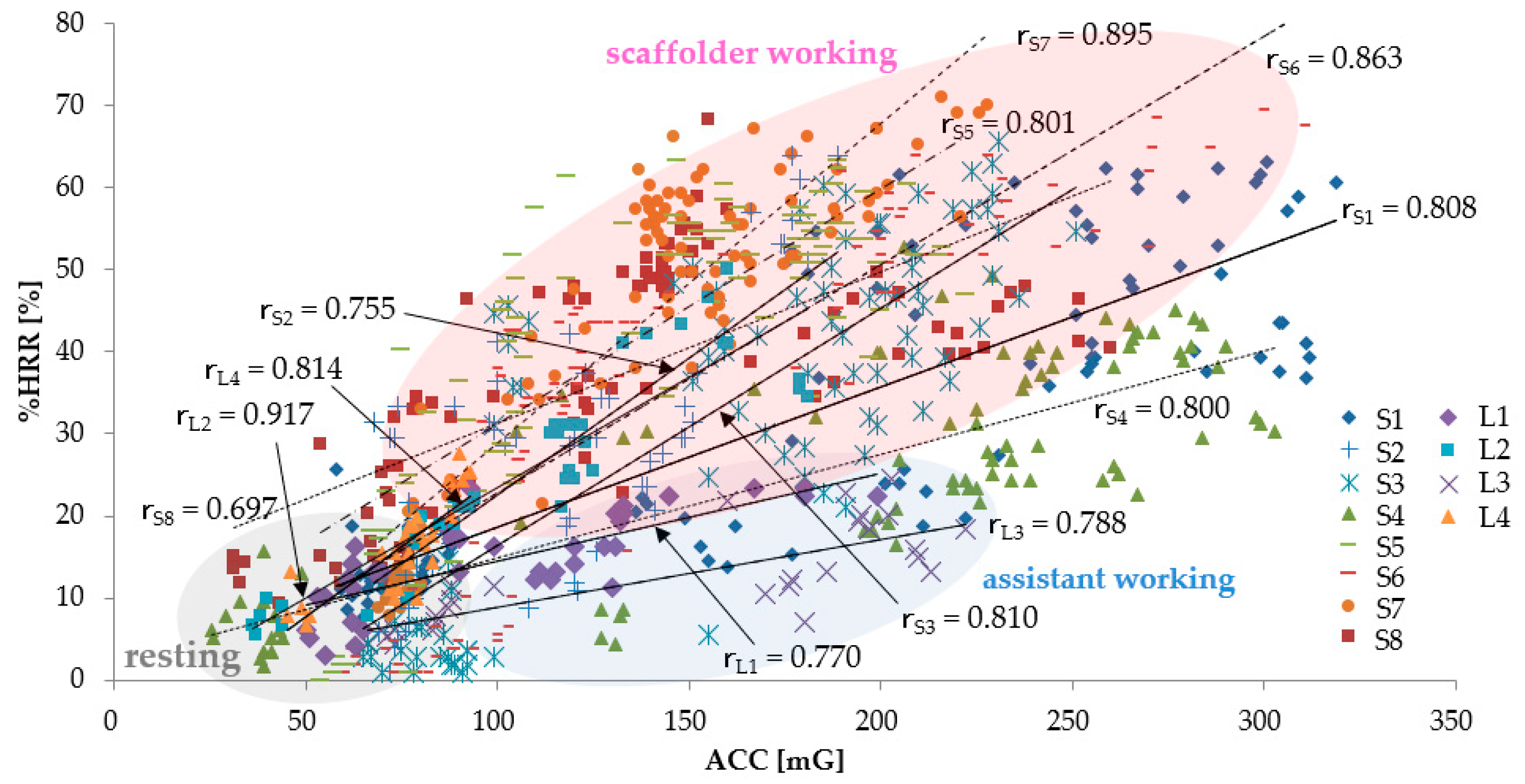
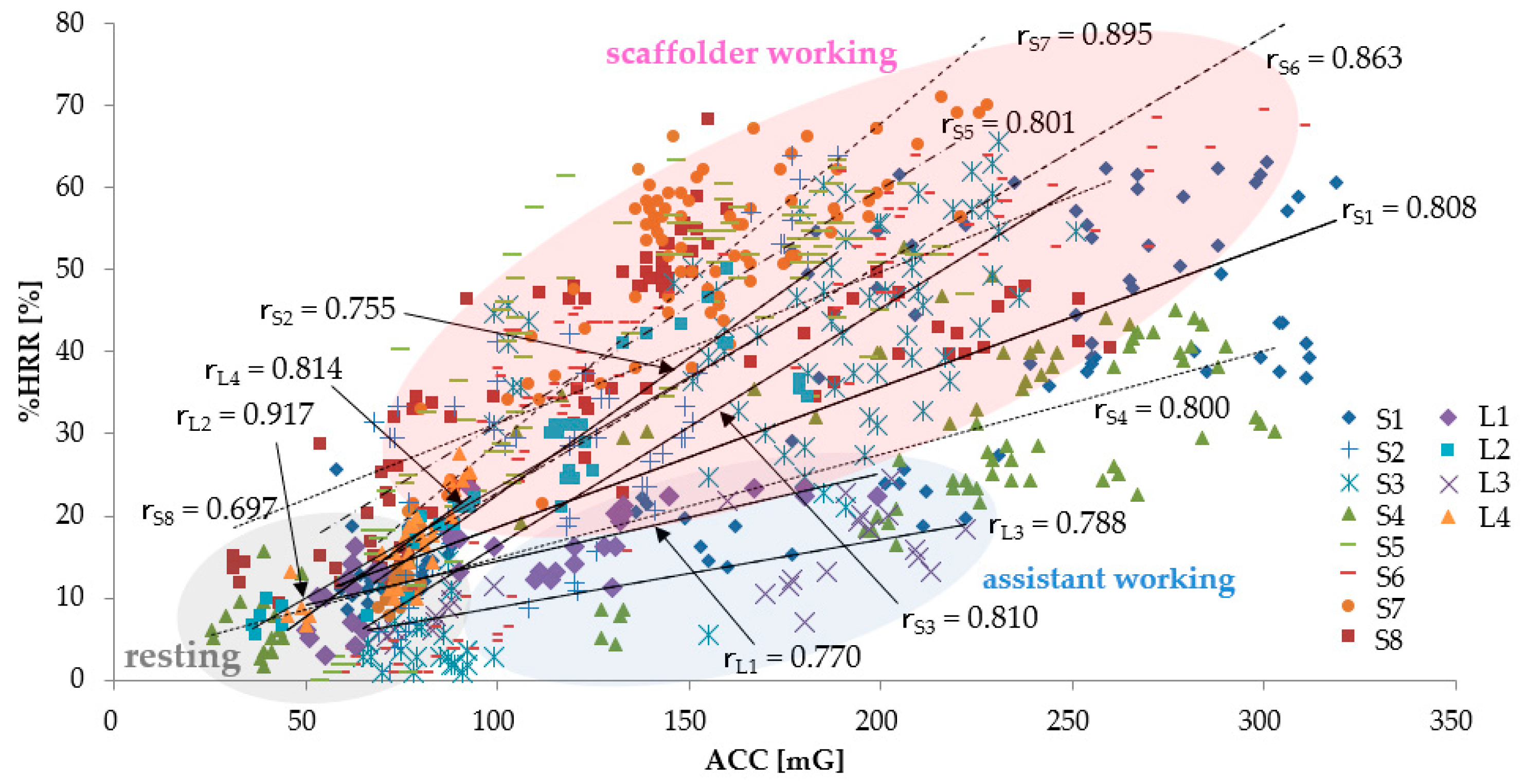
3.1.1. The Relationship between ACC and %HRR
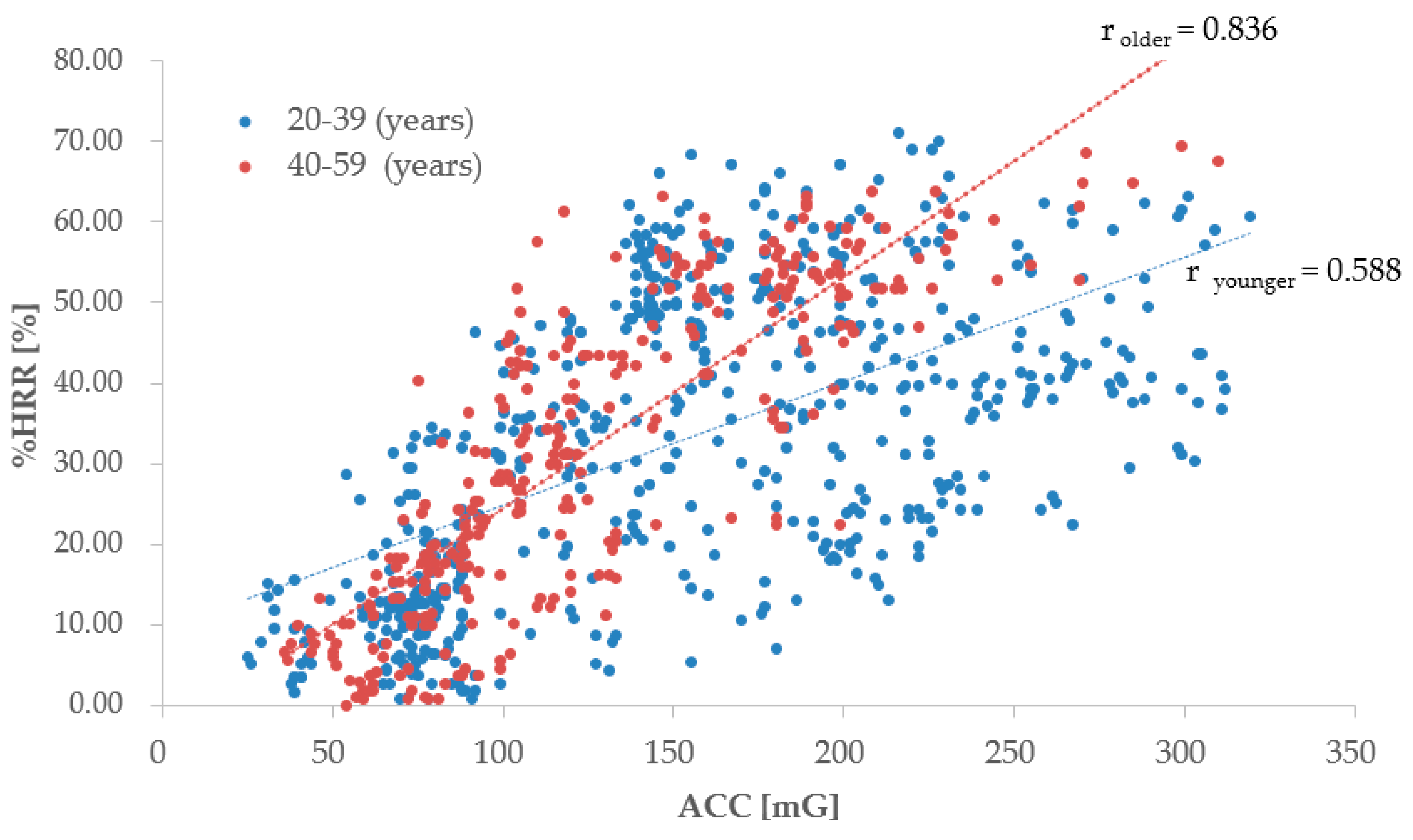
3.1.2. The Relationship between ACC and %HRR by Workers’ Age
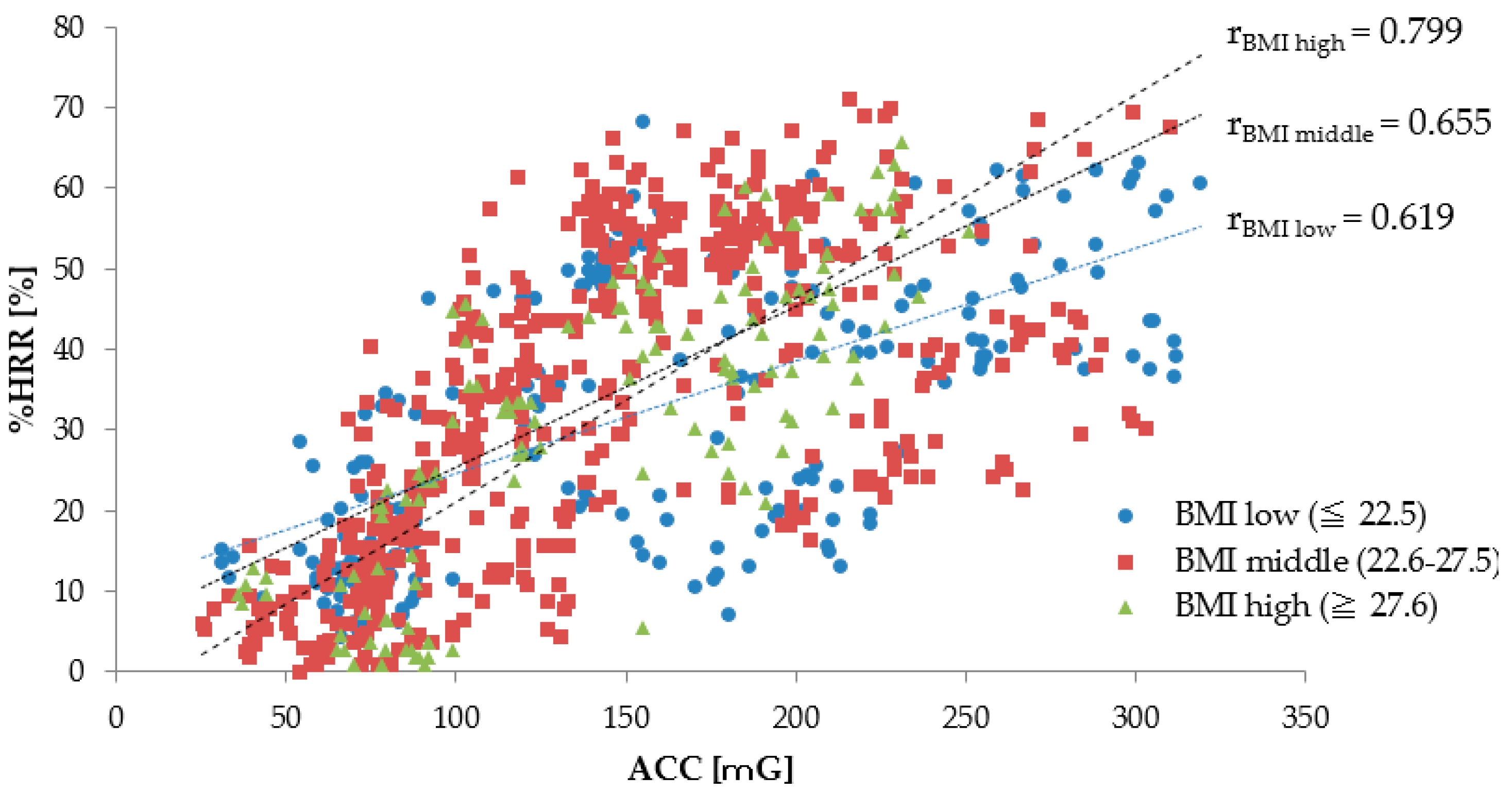
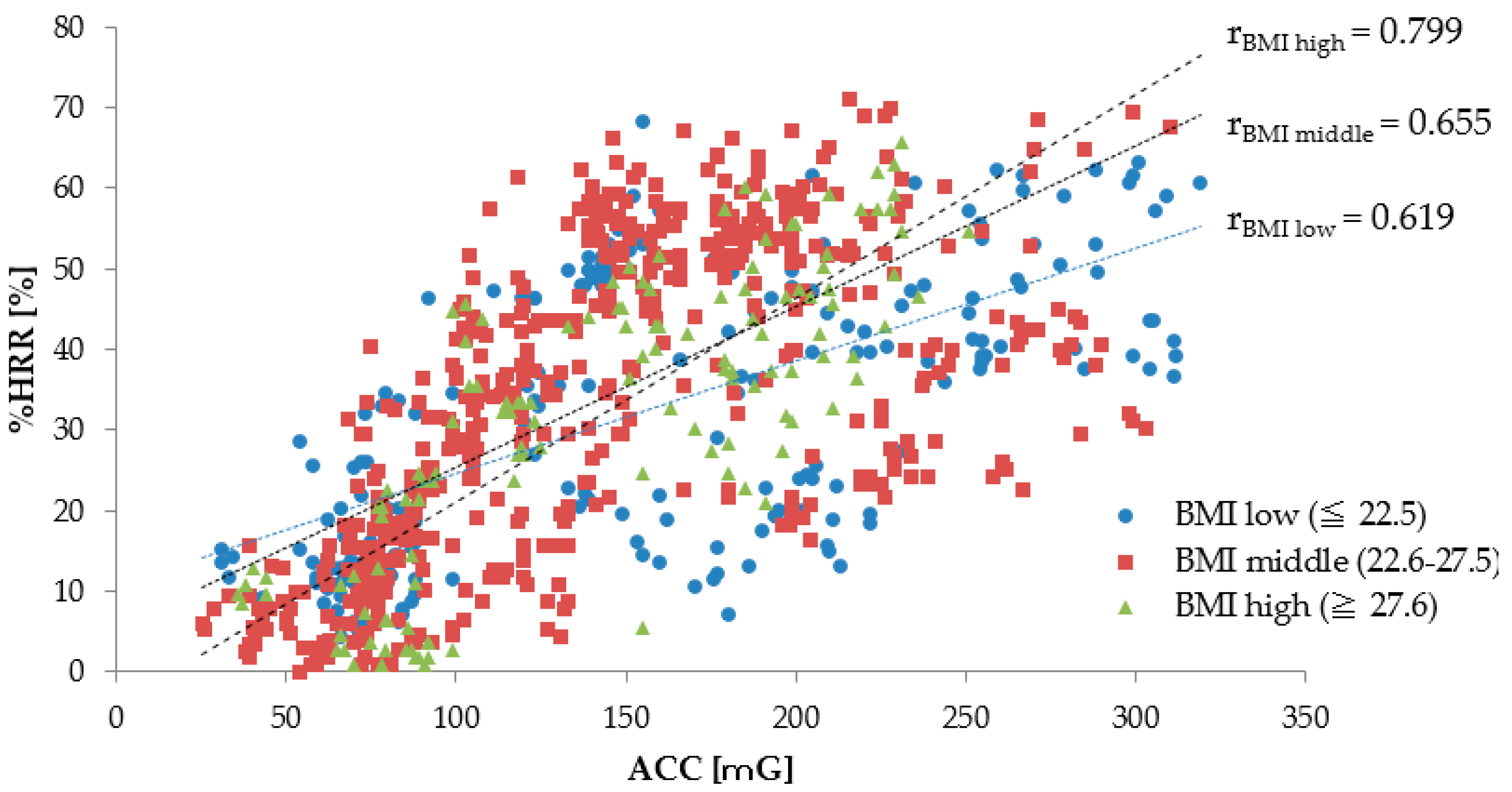
3.1.3. The Relationship between ACC and %HRR by Workers’ BMI
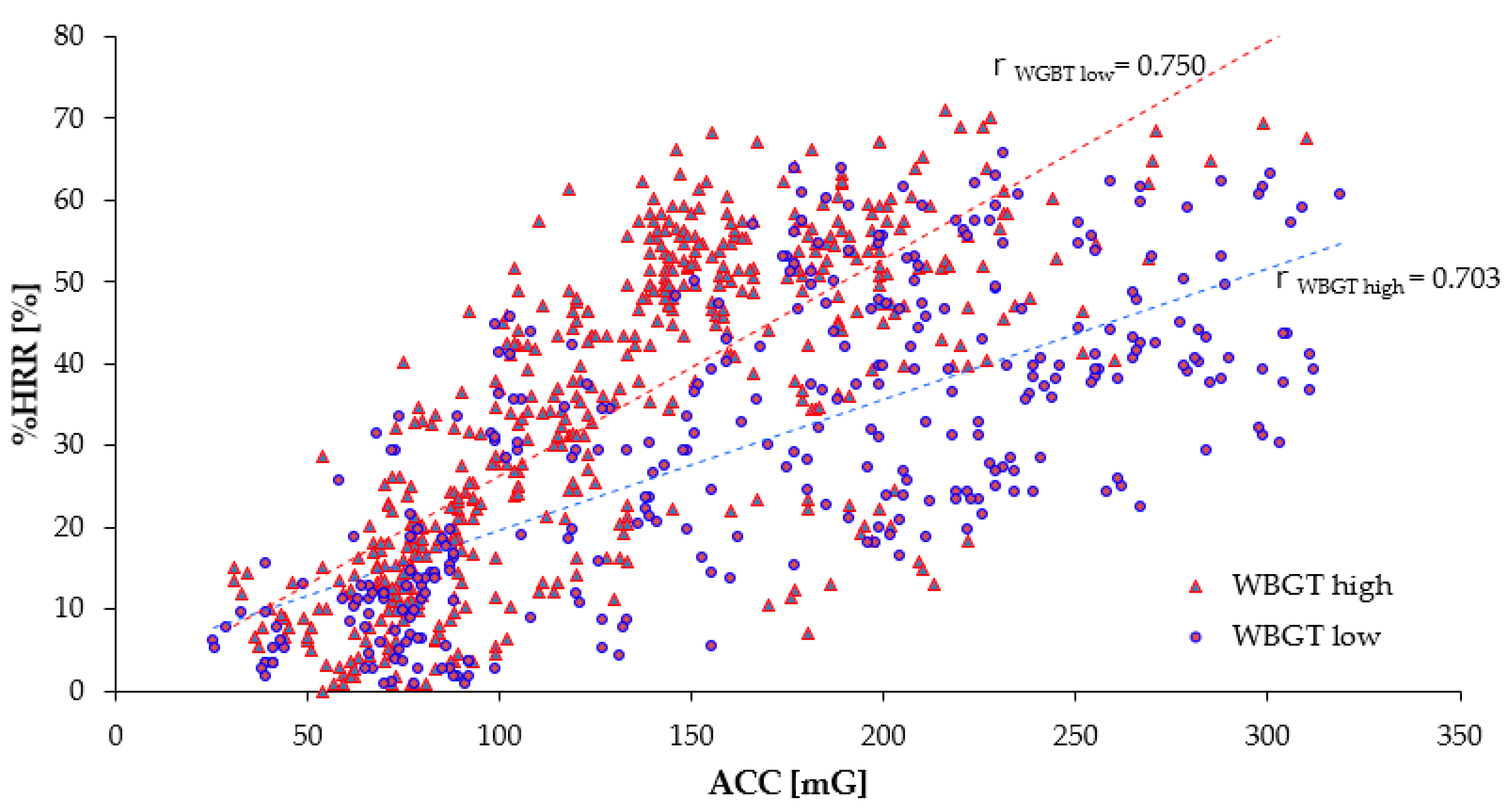
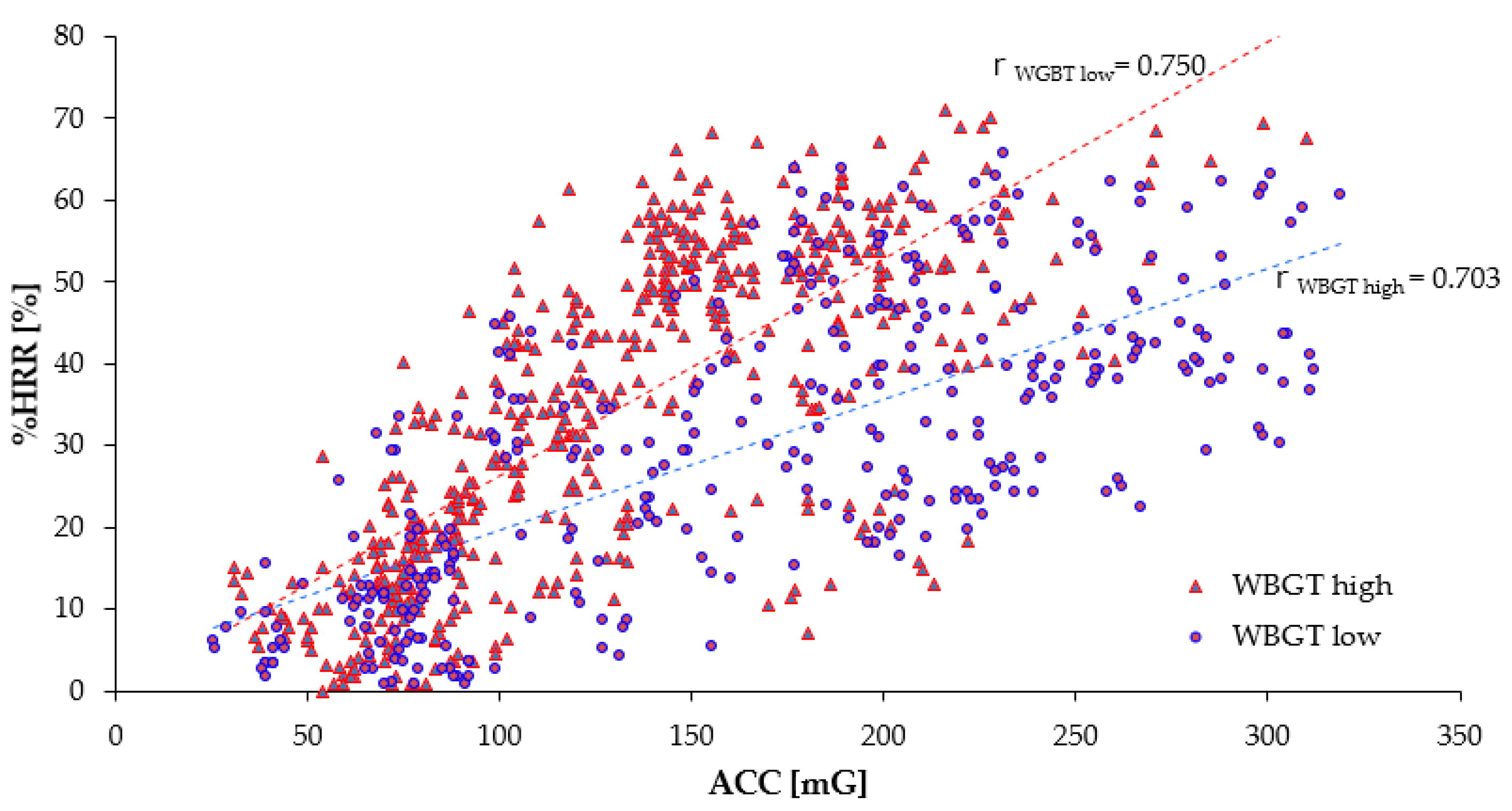
3.1.4. The Relationship between ACC and %HRR by Workers’ WBGT
3.2. Logistic Regression Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethical Statements
References
- Alkaissy, M.; Arashpour, M.; Ashuri, B.; Bai, Y.; Hosseini, R. Safety management in construction: 20 years of risk modeling. Saf. Sci. 2020, 129, 104805. [Google Scholar] [CrossRef]
- Hashiguchi, N.; Cao, J.; Lim, Y.; Kubota, Y.; Kitahara, S.; Ishida, S.; Kodama, K. The effects of psychological factors on perceptions of productivity in construction sites in Japan by worker age. Int. J. Environ. Res. Public Health 2020, 17, 3517. [Google Scholar] [CrossRef]
- Leung, M.Y.; Chan, I.Y.S.; Cooper, C.L. Stress Management in the Construction Industry; John Wiley & Sons: West Sussex, UK, 2014; pp. 1–27. [Google Scholar]
- Statistics Bureau of Japan at Ministry of Internal Affairs and Communications Sites, Labour Force Survey. Available online: https://www.stat.go.jp/english/data/roudou/index.html (accessed on 7 April 2020).
- Al-Bouwarthan, M.; Quinn, M.M.; Kriebel, D.; Wegman, D.H. Assessment of Heat Stress Exposure among Construction Workers in the Hot Desert Climate of Saudi Arabia. Ann. Work Expo. Health 2019, 63, 505–520. [Google Scholar] [CrossRef] [PubMed]
- Japan Construction Occupational Safety and Health Association, Occupational Accident Statistics, Occurrence of Fatal Accidents in the Construction Industry by Month (In Japanese). Available online: https://www.kensaibou.or.jp/safe_tech/statistics/month/index.html (accessed on 7 April 2020).
- Rother, H.A.; John, J.; Caradee, Y.; Wright, C.Y.; Irlam, J.; Oosthuizen, R.; Garland, R.M. Perceptions of Occupational Heat, Sun Exposure, and Health Risk Prevention: A Qualitative Study of Forestry Workers in South Africa. Atmosphere 2020, 12, 37. [Google Scholar] [CrossRef] [Green Version]
- Sokas, R.K.; Dong, X.S.; Cain, C.T. Building a Sustainable Construction Workforce. Int. J. Environ. Res. Public Health 2019, 16, 4202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvo-Sotomayor, I.; Laka, J.P.; Aguado, R. Workforce Ageing and Labour Productivity in Europe. Sustainability 2019, 11, 5851. [Google Scholar] [CrossRef] [Green Version]
- Merkus, S.L.; Lunde, L.K.; Koch, M.; Wærsted, M.; Knardahl, S.; Veiersted, K.B. Physical capacity, occupational physical demands, and relative physical strain of older employees in construction and healthcare. Int. Arch. Occup. Environ. Health 2019, 92, 295–307. [Google Scholar] [CrossRef] [Green Version]
- Flower, D.J.C.; Tipton, M.J.; Milligan, G.S. Considerations for physical employment standards in the aging workforce. Work 2019, 63, 509–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pegula, S. An Analysis of Fatal Occupational Injuries at Road Construction Sites, 2003–2010. Available online: https://www.bls.gov/opub/mlr/2013 (accessed on 7 April 2020).
- Berhan, F.; Gebrehiwot, M.; Gizaw, Z. Workplace injury and associated factors among construction workers in Gondar town, Northwest Ethiopia. BMC Musculoskelet. Disord. 2019, 20, 523. [Google Scholar] [CrossRef]
- U.S. Department of Labor. The Revised Handbook for Analyzing Jobs; U.S. Department of Labor, Employment and Training Administration: Washington, DC, USA, 1991.
- Karwowski, W. International Encyclopedia of Ergonomics and Human Factors; CRC Press: Boca Raton, FL, USA, 2001; pp. 355–378. [Google Scholar]
- Astrand, P.O.; Rodahl, K.; Hans, A.D.; Sigmund, B.S. Textbook of Work Physiology: Physiological Bases of Exercise; Human Kinetics: Champaign, IL, USA, 2003. [Google Scholar]
- Gragnano, A.; Simbula, S.; Miglioretti, M. Work–Life Balance: Weighing the Importance of Work–Family andWork–Health Balance. Int. J. Environ. Res. Public Health 2020, 17, 907. [Google Scholar] [CrossRef] [Green Version]
- Choi, B.; Jebelli, H.; Lee, S.H. Feasibility analysis of electrodermal activity (EDA) acquired from wearable sensors to assess construction workers’ perceived risk. Saf. Sci. 2019, 115, 110–120. [Google Scholar] [CrossRef]
- Meina, M.; Ratajczak, E.; Sadowska, M.; Rykaczewski, K.; Dreszer, J.; Bałaj, B.; Biedugnis, S.; Węgrzyński, W.; Krasuski, A. Heart rate variability and accelerometry as classification tools for monitoring perceived stress levels—A pilot study on firefighters. Sensors 2020, 20, 2834. [Google Scholar] [CrossRef]
- Yang, L.; Lu, K.; Forsman, M.; Lindecrantz, K.; Seoane, F.; Ekblom, O.; Jörgen Eklund, J. Evaluation of physiological workload assessment methods using heart rate and accelerometry for a smart wearable system. Ergonomics 2019, 62, 694–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Małek, Ł.A.; Mróz, A.; Czajkowska, A.; Kosmol, A.; Ogonowska-Słodownik, A.; Molik, B.; Morgulec-Adamowicz, N. Accuracy of Impedance Cardiography for Hemodynamic Assessment During Rest and Exercise in Wheelchair Rugby Players. Res. Q. Exerc. Sport 2019, 90, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Adibi, S. Mobile Health: A Technology Road Map; Springer: Berlin, Germany, 2015; pp. 319–342. [Google Scholar]
- Wang, Y.; Cang, S.; Yu, H. A survey on wearable sensor modality centred human activity recognition in health care. Expert Syst. Appl. 2019, 137, 167–190. [Google Scholar] [CrossRef]
- Bambang, C.; Kuncoro, D.; Luo, W.J.; Kuan, Y.D. Wireless Photoplethysmography Sensor for Continuous Blood Pressure Biosignal Shape Acquisition. J. Sens. 2020, 2020, 7192015. [Google Scholar]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998; pp. 54–62. [Google Scholar]
- Scheidt, F.; Meier, S.; Krämer, J.; Apitz, A.; Siaplaouras, J.; Bride, P.; Kaestner, M.; Apitz, C. Heart Rate Response During Treadmill Exercise Test in Children and Adolescents With Congenital Heart Disease. Front. Pediatric 2019, 7, 65. [Google Scholar] [CrossRef]
- Matsuura, H.; Mukaino, M.; Otaka, Y.; Kagaya, H.; Aoshima, Y.; Suzuki, T.; Inukai, A.; Hattori, E.; Ogasawara, T.; Saito, E. Validity of simplified, calibration-less exercise intensity measurement using resting heart rate during sleep: A method-comparison study with respiratory gas analysis. BMC Sports Sci. Med. Rehabil. 2019, 11, 27. [Google Scholar] [CrossRef] [PubMed]
- Engelen, L.; Chau, J.; Young, S.; Mackey, M.; Jeyapalan, D.; Bauman, A. Is activity-based working impacting health, work performance and perceptions? A systematic review. Build. Res. Inf. 2019, 47, 468–479. [Google Scholar] [CrossRef]
- Jae, S.Y.; Bunsawat, K.; Kunutsor, S.K.; Yoon, E.S.; Kim, H.J.; Kang, M.; Choi, Y.H.; Franklin, B.A. Relation of Exercise Heart Rate Recovery to Predict Cardiometabolic Syndrome in Men. Am. J. Cardiol. 2019, 123, 582–587. [Google Scholar] [CrossRef] [Green Version]
- Lavie, C.J.; Hecht, H.F.; Wisloff, U. Extreme Physical Activity May Increase Coronary Calcification, But Fitness Still Prevails. Mayo Clin. Proc. Innov. Qual. Outcomes 2019, 3, 103–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.C.; Yang, C.Y.; Zhou, Z.; Wu, S. Intelligent health monitoring system based on smart clothing. Int. J. Distrib. Sens. Netw. 2018, 14. [Google Scholar] [CrossRef] [Green Version]
- Axisa, F.; Schmitt, P.M.; Gehin, C.; Deklhomme, G.; McAdams, E.; Dittmar, A. Flexible Technologies and Smart Clothing for Citizen Medicine, Home Healthcare, and Disease Prevention. IEEE Trans. Inf. Technol. Biomed. 2005, 9, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Ji, Y.G. Standardization for Smart Clothing Technology. In Proceedings of the 13th International Human-Computer Interaction: Ambient, Ubiquitous and Intelligent Interaction Conference (HCI Interaction 2009), San Diego, CA, USA, 19–24 July 2009; pp. 768–777. [Google Scholar]
- TOYOBO Co., ltd. Discover TOYOBO’s New Materials. Available online: https://www.toyobo-global.com/discover/materials/cocomi/index.html (accessed on 7 April 2020).
- Shiozawa, N.; Lee, J.; Okuno, A.; Makikawa, M. Novel Under Weare “Smart-Wear” with Stretchable and Flexible Electrodes Enables Insensible Monitoring Electrocardiograph. In Proceedings of the World Engineering conference and Convention, Kyoto, Japan, 29 November–2 December 2015; OS7-6-3. pp. 1–2. [Google Scholar]
- Zheng, W.; McLerran, D.F.; Rolland, B.; Zhang, X.; Inoue, M.; Matsuo, K.; He, J.; Gupta, P.C.; Ramadas, K.; Tsugane, S.; et al. Association between Body-Mass Index and Risk of Death in More Than 1 Million Asians. N. Engl. J. Med. Overseas Ed. 2011, 364, 719–729. [Google Scholar] [CrossRef] [Green Version]
- Porges, S.; Byrne, E. Research methods for measurement of heart rate and respiration. J. Biol. Phys. 1992, 34, 93–130. [Google Scholar] [CrossRef]
- Caballero, Y.; Ando, T.J.; Nakae, S.; Usui, C.; Aoyama, T.; Nakanishi, M.; Nagayoshi, S.; Fujiwara, Y.; Tanaka, S. Simple Prediction of Metabolic Equivalents of Daily Activities Using Heart Rate Monitor without Calibration of Individuals. IJERPH 2014, 11, 5333–5348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef] [Green Version]
- Bruin, E.D.; Najafi, B.; Murer, K.; Uebellhart, D.; Animian, K. Quantification of everyday motor function in a geriatric population. J. Rehabil. Res. Dev. 2007, 44, 417–428. [Google Scholar] [CrossRef]
- Menai, M.; Hees, V.T.; Elbaz, A.; Kivimaki, M.; Singh-manoux, A. Accelerometer assessed moderate-to-vigorous physical activity and successful ageing: Results from the Whitehall II study. Sci. Rep. 2017, 8, 45772. [Google Scholar] [CrossRef] [Green Version]
- Adair, J.G. The Hawthorne effect: A reconsideration of the methodological artifact. J. Appl. Psychol. 1984, 69, 334–345. [Google Scholar] [CrossRef]
- Agresti, A. An Introduction to Categorical Data Analysis; John Wiley and Sons: New Jersey, NJ, USA, 2007; pp. 99–136. [Google Scholar]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression; John Wiley and Sons: New York, NY, USA, 2000. [Google Scholar]
- IDAJ Co., LTD. modeFRONTIER®. Available online: https://www.idaj.co.jp/product/modefrontier/ (accessed on 2 May 2020).
- Daoud, J. Multicollinearity and Regression Analysis. J. Phys. Conf. Ser. 2017, 949, 012009. [Google Scholar] [CrossRef]
- Parsons, K. Heat Stress Standard ISO 7243 and its Global Application. Ind. Health 2006, 44, 368–379. [Google Scholar] [CrossRef]
- Onder, S.; Mutle, M. Analyses of non-fatal accidents in an opencast mine by logistic regression model—A case study. Int. J. Inj. Control Saf. Promot. 2017, 24, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Onder, M.; Onder, S.; Adiguzel, E. Applying hierarchical loglinear models to nonfatal underground coal mine accidents for safety management. Int. J. Occup. Saf. Ergon. 2014, 20, 239–248. [Google Scholar] [CrossRef]
- Uh, H.W.; Mertens, B.J.; Wijk, J.H.; Houwelingen, H.C.; Houwing-Duistermaat, J. Model selection based on logistic regression in a highly correlated candidate gene region. BMC Proc. 2007, 1, S114. [Google Scholar] [CrossRef] [Green Version]
- Hastie, T.; Tibshirani, R.; Friedman, J. The Elements of Statistical Learning: Data Mining, Inference, and Prediction New York; Springer: Berlin, Germany, 2001. [Google Scholar]
- Smith, T.J.; Cornelius McKenna, C.M. A Comparison of Logistic Regression Pseudo R Indices. Mathematics 2013, 39, 17–26. [Google Scholar]
- Bewick, V.; Cheek, L.; Ball, J. Statistics review 14: Logistic regression. Crit. Care 2005, 9, 112–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mbachu, H.I.; Nduka, E.C.; Nja, M.E. Designing a Pseudo R-Squared Goodness-of-Fit Measure in Generalized Linear Models. J. Math. Res. 2012, 4, 148–154. [Google Scholar] [CrossRef] [Green Version]
- Hammert, G.A.J.; Schons, L.M.; Wieseke, J.; Schimmelpfennig, H. Log-likelihood-based Pseudo-R2 in Logistic Regression: Deriving Sample-sensitive Benchmarks. Sociol. Methods Res. 2016, 4, 507–531. [Google Scholar] [CrossRef]
- Guo, H.; Yu, Y.; Xiang, T.; Li, H.; Zhang, D. The availability of wearable-device-based physical data for the measurement of construction workers’ psychological status on site: From the perspective of safety management. Autom. Constr. 2017, 82, 207–217. [Google Scholar] [CrossRef]
- Nagelkerke, N.J.D. A note on a general definition of the coefficient of determination. Biometrika 1991, 78, 691–692. [Google Scholar] [CrossRef]
- Lee, W.; Lin, K.; Seto, E.; Migliaccio, G.C. Wearable sensors for monitoring on-duty and off-duty worker physiological status and activities in construction. Autom. Constr. 2017, 83, 341–353. [Google Scholar] [CrossRef]
- She, J.; Nakamura, H.; Makino, K.; Ohyama, Y.; Hashimoto, H. Selection of Suitable Maximum-heart-rate Formulas for Use with Karvonen Formula to Calculate Exercise Intensity. IJAC 2015, 12, 62–69. [Google Scholar] [CrossRef]
- Lounana, J.; Campion, F.; Noakes, T.D.; Medelli, J. Relationship between %HRmax,%HR Reserve, %VO2max, and %VO2 reserve in elite cyclists. Med. Sci. Sports Exerc. 2007, 39, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Garet, M.; Boudet, G.; Montaurier, C.; Vermorel, M.; Coudert, J.; Chamoux, A. Estimating relative physical workload using heart rate monitoring: A validation by whole-body indirect calorimetry. Eur. J. Appl 2005, 94, 46–53. [Google Scholar] [CrossRef]
- Buller, M.J.; Latzka, W.A.; Yokota, M.; Tharion, W.J.; Moran, D.S. A real-time heat strain risk classifier using heart rate and skin temperature. Physiol. Meas. 2008, 29, 79–85. [Google Scholar] [CrossRef]
- Miller, V.S.; Bates, G.P. The Thermal Work Limit Is a Simple Reliable Heat Index for the Protection of Workers in Thermally Stressful Environments. Ann. Occup. Hyg. 2007, 51, 553–561. [Google Scholar] [PubMed]
- Al-Bouwarthan, M.; Quinn, M.M.; Kriebel, D.; Wegman, D.H. A Field Evaluation of Construction Workers’ Activity, Hydration Status, and Heat Strain in the Extreme Summer Heat of Saudi Arabia. Ann. Work Expo. Health 2019, 63, 505–520. [Google Scholar] [CrossRef]
- Shirowzhan, S.; Tan, W.; Sepasgoza, S.M.E. Digital Twin and CyberGIS for Improving Connectivity and Measuring the Impact of Infrastructure Construction Planning in Smart Citiesices. Int. J. Geo-Inf. 2020, 9, 240. [Google Scholar] [CrossRef]
- Nakanishi, M.; Izumi, S.; Nagayoshi1, S.; Kawaguchi, H.; Yoshimoto, M.; Shiga, T.; Ando, T.; Nakae, S.; Usui, C.; Aoyama, T.; et al. Estimating metabolic equivalents for activities in daily life using acceleration and heart rate in wearable devices. Biomed. Eng. Online 2018, 17, 100. [Google Scholar] [CrossRef] [Green Version]
- Brandenburg, S.G.; Haas, C.T.; Byrom, K. Strategic Management of Human Resources in Construction. IJPM 2009, 27, 471–480. [Google Scholar] [CrossRef] [Green Version]
- Tabassi, A.A.; Baker, A.H.A. Training, motivation, and performance: The case of human resource management in construction projects in Mashhad, Iran. IJPM 2009, 27, 471–480. [Google Scholar] [CrossRef]
- Siew, R. Human Resource Management in the Construction -Industry Sustainability Competencies. AJCEB 2014, 14, 87–103. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurements | Equipment Model (Name of the Manufacturer) | Accuracy | Resolution | Interval | Note |
|---|---|---|---|---|---|
| Working environment | |||||
| Air temperature | AD-5696(A&D Co., Ltd.) | ±1 °C | 0.1 °C | 10 min. | Thermister |
| Relative humidity | ±5% Rh | 0.1% Rh | 10 min. | Capacitance | |
| WBGT | -- | 0.1 °C | 10 min. | -- | |
| Physical workload | |||||
| ECG(Smart clothing) | COCOMI *1 (TOYOBO Co., Ltd.) | 1 Ω/sq*2 | 0.3 mm *3 | -- | Stretchable conductive film |
| Heart rate sensor | WHS-2 *4 (Union Tool Co., Ltd.) | -- | 1 kHz *5 | Per beat | Analysis of R-R interval |
| 3-axis acceleration | -- | 31.25 Hz *5 | Per beat | Capacitive sense | |
| Infrastructure | |||||
| Data acquisition time | CC2650 *6 and ThinkPad (Texas Instruments and Lenovo co., Ltd.) | -- | 1 ms | Per beat | Synchronized time with server |
| Data transfer | Raspberry Pi Zero W (Raspberry Pi Foundation) | -- | -- | -- | IEEE802.11 b/g/n (Wireless LAN) Bluetooth 4.1 |
| Measurement Parameter [Unit] | Method | Unit |
|---|---|---|
| BMI | weight/(height)2 | kg/m2 |
| HRworking | average heart rate in 5 min during working hours | bpm |
| HRresting | average heart rate in 5 min during the rest hours | bpm |
| HRmax | 208 − 0.7 × age | bpm |
| %HRR | % | |
| ACC | mG |
| ID# | Data Collection Dates | Age (Years) | Main Job Task | Height (cm) | Weight (kg) | Duration of Data Collection (min) | Scheduled Resting (min) | Number of Data * (Sets) |
|---|---|---|---|---|---|---|---|---|
| S1 | June-29-2018 | 20 | Scaffolder | 159.0 | 57.0 | 450 | 90 | 90 |
| S2 | June-29-2018 | 39 | Scaffolder | 179.0 | 74.0 | 300 | 90 | 60 |
| S3 | June-29-2018 | 32 | Scaffolder | 177.0 | 93.0 | 450 | 90 | 90 |
| S4 | June-29-2018 | 25 | Scaffolder | 182.0 | 82.0 | 450 | 90 | 90 |
| S5 | Nov-15-2018 | 41 | Scaffolder | 176.0 | 70.0 | 510 | 90 | 102 |
| S6 | Nov-15-2018 Nov-15-2018 | 40 | Scaffolder | 176.0 | 75.0 | 510 | 90 | 102 |
| S7 | 36 | Scaffolder | 170.0 | 68.0 | 510 | 90 | 102 | |
| S8 | Nov-15-2018 | 22 | Scaffolder | 165.0 | 55.0 | 510 | 90 | 102 |
| L1 | May-25-2018 | 43 | Worker | 168.0 | 70.0 | 210 | 60 | 42 |
| L2 | May-25-2018 | 50 | Worker | 174.5 | 87.5 | 210 | 60 | 42 |
| L3 | May-25-2018 | 27 | Worker | 170.5 | 62.5 | 150 | 60 | 30 |
| L4 | Nov-15-2018 | 59 | Worker | 169.0 | 76.0 | 150 | 60 | 30 |
| Variables | ACC | BMI | AGE | WBGT | VIF |
|---|---|---|---|---|---|
| ACC | 1.00 | 1.17 | |||
| BMI | 0.021 | 1.00 | 1.48 | ||
| AGE | −0.333 *** | 0.415 *** | 1.00 | 1.43 | |
| WBGT | −0.067 * | −0.387 *** | −0.048 * | 1.00 | 1.20 |
| ID# | Estimated HRmax (bpm) | Estimated HRresting (bpm) | HRworking Ave. ± SD (bpm) | %HRR Ave. ± SD (%) | ACC Ave. ± SD (mG) | rACC-%HRR |
|---|---|---|---|---|---|---|
| S1–S8 | 185.8 ± 5.6 | 75.8 ± 2.5 | 115.0 ± 20.2 | 35.8 ± 18.5 | 152.1 ± 67.0 | - |
| S1 *2 | 194.0 | 77 | 117.9 ± 21.4 | 35.0 ± 18.3 | 195.6 ± 86.3 | 0.808 |
| S2 *3 | 180.7 | 79 | 106.6 ± 16.0 | 27.2 ± 15.8 | 113.9 ± 35.7 | 0.755 |
| S3 *2 | 185.6 | 76 | 112.7 ± 21.9 | 33.4 ± 20.0 | 158.8 ± 55.7 | 0.810 |
| S4 | 190.5 | 75 | 105.0 ± 15.8 | 26.0 ± 13.7 | 188.0 ± 86.9 | 0.800 |
| S5 *1 | 179.3 | 75 | 119.1 ± 17.6 | 42.3 ± 16.9 | 138.6 ± 47.1 | 0.801 |
| S6 *2 | 180.0 | 72 | 111.5 ± 22.4 | 36.5 ± 20.7 | 149.2 ± 64.4 | 0.863 |
| S7 *1 | 182.8 | 80 | 125.7 ± 19.4 | 44.5 ± 18.9 | 139.9 ± 43.4 | 0.895 |
| S8 *2 | 192.6 | 74 | 117.2 ± 17.4 | 36.4 ± 14.7 | 127.4 ± 55.5 | 0.697 |
| L1–L4 | 176.5 ± 7.6 | 77.0 ± 2.0 | 95.0 ± 10.7 | 18.4 ± 10.2 | 106.7 ± 47.4 | - |
| L1 | 174.4 | 76 | 90.4 ± 5.4 | 14.2 ± 5.3 | 99.1 ± 39.5 | 0.770 |
| L2 | 173.0 | 80 | 106.4 ± 11.2 | 28.3 ± 11.9 | 108.2 ± 41.2 | 0.917 |
| L3 | 189.1 | 75 | 89.8 ± 6.9 | 13.0 ± 6.1 | 147.8 ± 57.6 | 0.788 |
| L4 | 166.7 | 76 | 90.4 ± 5.5 | 15.9 ± 6.1 | 74.2 ± 14.8 | 0.814 |
| Total Ave. ± SD | 182.4 ± 8.4 | 76.3 ± 2.4 | 111.7 ± 20.4 | 32.9 ± 18.6 | 144.7 ± 60.3 | - |
| Age Groups (Years) | Number of Data (Sets) | AGE Average ± SD (Years) | ACC Average ± SD (mG) | %HRR Average ± SD (bpm) | rACC-%HRR |
|---|---|---|---|---|---|
| AGEyounger | 562 | 28.7 ± 7.2 | 154.7 ± 69.8 | 33.3 ± 18.3 | 0.588 |
| AGEolder | 310 | 46.6 ± 8.0 | 127.1 ± 55.7 | 32.3 ± 19.1 | 0.836 |
| p-valueyounger-older * | <0.001 | 0.049 | - | ||
| BMI Groups (kg/m2) | Number of Data (Sets) | BMI Average ± SD (kg/m2) | %HRR Average ± SD (bpm) | ACC Average ± SD (mG) | rACC-%HRR |
|---|---|---|---|---|---|
| BMIlow | 222 | 21.3 ± 1.07 | 32.6 ± 17.3 | 157.8 ± 76.6 | 0.610 |
| BMImiddle | 528 | 23.9 ± 1.02 | 33.6 ± 19.3 | 139.7 ± 63.3 | 0.767 |
| BMIhigh | 132 | 29.4 ± 0.46 | 31.8 ± 17.9 | 142.8 ± 56.6 | 0.810 |
| p-value *low-middle | n.s. | 0.011 | |||
| p-value *middle-high | n.s. | 0.316 | |||
| p-value *low-high | n.s. | 0.334 | |||
| WBGT Groups (°C) | Number of Data (Sets) | WBGT Average ± SD (°C) | %HRR Average ± SD (bpm) | ACC Average ± SD (mG) (mG) | rACC-%HRR |
|---|---|---|---|---|---|
| WBGT low | 552 | 16.3 ± 2.75 | 30.7 ± 17.6 | 168.6 ± 77.4 | 0.703 |
| WBGT high | 330 | 27.6 ± 0.21 | 34.3 ± 19.1 | 130.5 ± 53.9 | 0.750 |
| p-value * low-high | 0.005 | <0.001 | |||
| Model | Independent Variables | Coefficient | Standard Error | Wald χ2 | p-Value | Odds Ratio | 95% CI for Odds |
|---|---|---|---|---|---|---|---|
| Model 1 | Constant | −25.6 | 3.40 | 61.3 | <0.001 | 0.000 | – |
| ACC | 0.041 | 0.003 | 183 | <0.001 | 1.042 | 1.036–1.048 | |
| AGE | 0.074 | 0.020 | 14.0 | <0.001 | 1.077 | 1.036–1.120 | |
| BMI | −0.035 | 0.058 | 0.361 | 0.548 | 0.966 | 0.862–1.082 | |
| WBGT | 0.705 | 0.095 | 54.6 | <0.001 | 2.023 | 1.678–2.438 | |
| Model 2 | Constant | −28.1 | 2.35 | 142 | <0.001 | 0.000 | – |
| ACC | 0.041 | 0.003 | 181 | <0.001 | 1.042 | 1.036–1.048 | |
| AGE | 0.066 | 0.014 | 23.1 | <0.001 | 1.068 | 1.040–1.097 | |
| WBGT | 0.742 | 0.074 | 101 | <0.001 | 2.100 | 1.817–2.427 |
| Model (Independent Variables) | Predicted Risk | Percentage | GoF | ||||
|---|---|---|---|---|---|---|---|
| Observed | 0 | 1 | (%) | AIC | Cox–Snell R2 | Nagelkerke R2 | |
| Model 1 (ACC, AGE, BMI, WBGT) | Risk 0 | 487 | 53 | 90.2 | 57.5 | 0.435 | 0.590 |
| 1 | 45 | 297 | 86.8 | ||||
| Overall | 88.5 | ||||||
| Model 2 (ACC, AGE, WBGT) | Risk 0 | 486 | 54 | 90.0 | 59.5 | 0.434 | 0.589 |
| 1 | 40 | 302 | 88.3 | ||||
| Overall | 89.2 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hashiguchi, N.; Kodama, K.; Lim, Y.; Che, C.; Kuroishi, S.; Miyazaki, Y.; Kobayashi, T.; Kitahara, S.; Tateyama, K. Practical Judgment of Workload Based on Physical Activity, Work Conditions, and Worker’s Age in Construction Site. Sensors 2020, 20, 3786. https://doi.org/10.3390/s20133786
Hashiguchi N, Kodama K, Lim Y, Che C, Kuroishi S, Miyazaki Y, Kobayashi T, Kitahara S, Tateyama K. Practical Judgment of Workload Based on Physical Activity, Work Conditions, and Worker’s Age in Construction Site. Sensors. 2020; 20(13):3786. https://doi.org/10.3390/s20133786
Chicago/Turabian StyleHashiguchi, Nobuki, Kota Kodama, Yeongjoo Lim, Chang Che, Shinichi Kuroishi, Yasuhiro Miyazaki, Taizo Kobayashi, Shigeo Kitahara, and Kazuyoshi Tateyama. 2020. "Practical Judgment of Workload Based on Physical Activity, Work Conditions, and Worker’s Age in Construction Site" Sensors 20, no. 13: 3786. https://doi.org/10.3390/s20133786