
“Small Wins” for those with Lyme Disease in Canada: Patients in an Embodied Health Movement

1
School of Rehabilitation Therapy, Queen’s University, Louise D Acton Building, 31 George Street, Kingston, ON K7L 3N6, Canada
2
Department of Politics and International Relations, Mount Allison University, 144 Main Street, Sackville, NB E4L 1A7, Canada
*
Author to whom correspondence should be addressed.
Zoonotic Dis. 2024, 4(1), 22-36; https://doi.org/10.3390/zoonoticdis4010004
Submission received: 10 December 2023
/
Revised: 14 January 2024
/
Accepted: 17 January 2024
/
Published: 22 January 2024
Abstract
:Simple Summary
Many Lyme disease patients are struggling to navigate a healthcare system that increasingly dismisses their condition. Patient organizations have arisen to contest a healthcare system that dismisses patient conditions and to help bridge the divide between patients, researchers, healthcare systems, and policymakers. This study documents this experience to reveal the marginal progress made to date and the complexity of the challenges that remain.
Abstract
Lyme disease patient organizations have formed to challenge a health system that is failing Canadians who suffer from a disease that is ambiguous in its symptomology and trajectory. The framework of an embodied health movement illustrates the importance of the illness experience in mobilizing patients to oppose a system that is reliant on restrictive guidelines that deny testing and treatment and to seek alliances with researchers, physicians, and politicians who are sympathetic to their goals. The strategies of Lyme disease patient organizations, the importance of experiential knowledge, and the roles of both adversaries and allies are examined through a “small wins” approach to gauge successes and setbacks within a Canadian context.
{kind=link}
1. Introduction
People suffering from Lyme disease (LD) have united to support one another and advocate for prevention, testing, diagnosis, treatment, and, above all, recognition of both acute and chronic manifestations of the disease. Evidence has been mounting since the disease was identified in the 1970s in Lyme, Connecticut, USA. By 2018, the US Centers for Disease Control and Prevention reported that approximately 476,000 Americans were diagnosed and treated for Lyme disease every year [1,2]. In Canada, Lyme disease first surfaced in western Nova Scotia, southern Ontario, southern Manitoba, and southern British Columbia. Birds have been a primary vector for the spread of the deer tick (Ixodes scapularis), after which other mammals, large (deer) and small (mice, pets such as dogs), ensured its establishment and continued spread [1,3,4]. In 2021, Health Canada reported 3,147 confirmed cases of Lyme disease [5]. However, recent work by Lloyd and Hawkins found a 10.2- to 28-fold under detection of Lyme disease, suggesting that its prevalence in Canada is much greater [4]. Overall, LD cases are increasing across North America, and the outcomes for patients can be debilitating and sometimes fatal [4,6]. Yet, those who suffer from LD continue to be marginalized within Canada’s healthcare system. People become infected when they are bitten by a black-legged tick carrying a bacteria (Borrelia), and treatment delays put patients at risk of severe complications, including Bell’s palsy, Lyme carditis, and Lyme meningitis [7]. The issue is that the illness experience of patients, particularly those with chronic conditions, differs from the rhetoric of scientists that LD is straightforward to diagnose and curable with a short course of antibiotics, with persistent infection being non-existent [8,9,10]. The divergence between the lived patient experience and clinical evidence defended by influential scientists threatens the health and well-being of patients whose symptomology does not conform to guidelines sanctioned by health authorities.
This threat has resulted in the formation of LD patient organizations across Canada that offer peer support, provide information, and serve as patient advocates by challenging and collaborating with stakeholders for improved prevention, diagnosis, and treatment. Using the framework of embodied health movements, we highlight the motivation and mobilization of LD patient organizations and a need for the mutual appreciation of scientific evidence, clinical judgement, and experiential knowledge. The emphasis is on evidence-informed medicine as a tenet of person-centred medicine with the understanding that scientific knowledge is a means to support rather than limit clinical judgement [11]. The substance of LD patient organizations is framed as an embodied health movement described by Brown et al. as a subset of health social movements that captures the “blurring of boundaries” between medical experts and patients with validation of the illness experience and patient expertise [12]. In this context, the goal of patient organizations is to partner with decision makers, allowing for greater transparency and accountability. The application of the framework reveals the impact of government policies and the influence of medical standards and guidelines on the lives of those who suffer from LD and the role of patient organizations in giving a voice to patients and caregivers.
Our investigation explores the crucial role that patients continue to play in the advancement of understanding LD, how they have influenced Canadian healthcare policy, and the challenges they encounter. The first section examines the embodied health movement framework and its utility in examining the actions and reactions of LD patient organizations regarding research and policy. A “small wins” approach put forth by Jason is employed as a means to gauge the movement’s success [13]. Second, a snapshot of one of the first LD patient advocates, Polly Murray, foreshadows the tensions between clinical experts and patients that have persisted for over forty years. Third, the influence and limitations of the controversial clinical practice guidelines for LD and the ongoing challenges presented to patients who do not meet the criteria for diagnosis and treatment are examined. This includes implications of efforts to disentangle chronic Lyme disease (CLD) and post-treatment Lyme disease syndrome (PTLDS) for patients. The small wins achieved by patient organizations are outlined from the inception of the first patient organization in Canada to the formation of the Canadian Lyme Consortium, with patients represented as equal partners with researchers and health professionals. We note the ongoing burden and financial costs incurred by patients and their caregivers as problematic and unresolved. Figures published in 2023 suggest the healthcare cost in Canada per case ranges from an average of CAD 47 for early localized LD to an average of CAD 443 for disseminated LD when cases are diagnosed [14]. Yet this masks the potentially significant costs associated with loss of income due to either reduced work hours or the inability to work, let alone associated travel and other ancillary costs. For those who go undiagnosed in Canada, costs for treatment and travel expenses can be much higher, with reports noting costs ranging from CAD 29,000 to CAD 150,000 [15,16]. Two challenges confronting patient organizations are then explored: attempts to discredit patient organizations and funding dilemmas. This article concludes with an assessment of LD patient organizations as an embodied health movement.
2. Research Approach
2.1. Embodied Health Movements Framework
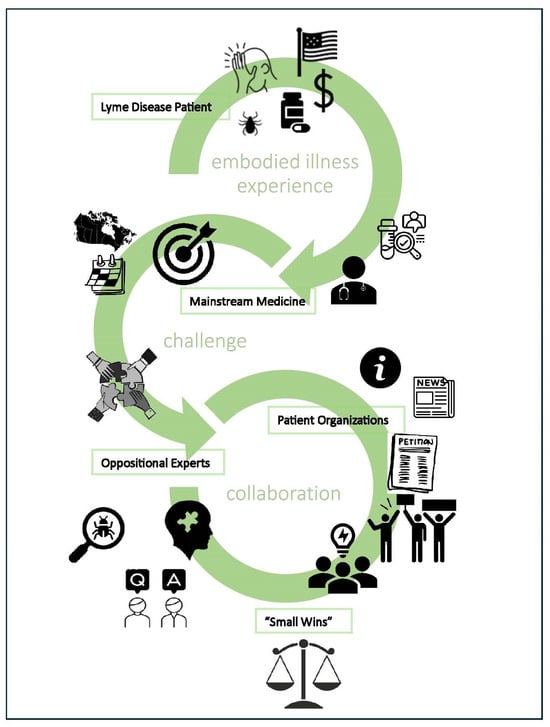
Embodied health movements, as outlined by Brown et al., “address disease, disability or illness experience by challenging science on etiology, diagnosis, treatment and prevention” [12] (p. 50). Central to these movements are the embodied experiences of LD patients, challenges to current practices and scientific knowledge, and the collaboration of patient advocates with oppositional experts. Oppositional experts are scientists, physicians, and other professionals who are able to support patients’ pursuits for validation, diagnosis, and treatment through evidence-informed practice [13]. Hinds and Sutcliffe count embodied health movements as “a product of the democratization of knowledge, seen in the health context as the incorporation of the patient experience into the management of health problems” [17] (p. 1662). This framework has been prominent in the study of unexplained and contested illnesses relative to diseases that have widespread acceptance in mainstream medicine [12,17,18]. The following sample of titles provide some insight into the challenges: “Illnesses You Have to Fight to Get…” [19]; “Living in Limbo…” [20]; “I just want permission to be ill…” [21]; and, “Keep complaining ‘til someone listens…” [22]. Although the existence of LD in the acute stage is questioned less, the variability of signs and symptoms and unreliable testing can lead to delayed/mis-/non-diagnosis [23]. The possibility of treatment failure and existence of persistent infections are more often disputed by scientists and physicians [24].
Brown et al. maintain that embodied health movements are characterized by three interconnected elements [12]. First, the embodied experience, a personal awareness of the illness experience, is what drives patient involvement in advocacy work and activism. LD patients and their caregivers who are marginalized and denied a voice in their medical encounters often seek peer support from patient organizations to learn about the disease, the debates surrounding testing and treatment, and, most importantly, how to get well. The second element of an embodied health movement is enacted when patients and caregivers become leaders and advocates for change and directly challenge mainstream science and health practice. A principal issue for LD patient organizations is the recognition and validation of experiential knowledge during medical encounters and in research and policy decisions. This stance challenges a more orthodox viewpoint whereby patients submit to medical authority and, as Hinds and Sutcliffe add, “the privileged status of biomedical explanations” [17] (p. 1665). LD patient organizations argue that biomedical explanations by influential scientists are often selective and do not account for the illness experience of many patients [25]. There is heterogeneity in the LD patient population expressed in the variability of symptoms not always corroborated through laboratory testing [26]. The methods employed by leaders and advocates to counter medical authority are captured in the third element of the embodied health movement framework, which is that patient organizations engaging in advocacy “must simultaneously challenge and collaborate with science” [12] (p. 56). Alliances with scientists, health practitioners, politicians, and other professionals who are sympathetic to the goals of patient organizations are crucial to establishing credibility. These oppositional experts can ensure that information disseminated to the public and the challenges launched by patient organizations are supported by evidence.
Within the embodied health framework, the aim of LD patient organizations is to have a voice in setting research priorities that are evidence-informed, merging science with the illness experience. They seek experts to partner with to increase awareness of the disease, advance testing and treatment options, and lobby governments for changes in health policy. LD patient organizations featured in media reports display that they are well-positioned to develop alliances with oppositional experts and leverage the experiential knowledge of their membership to challenge biomedical models that do not adequately serve their interests [27,28].
2.2. A Small Wins Approach
We adopt Jason’s small wins approach to gauge the outcomes of LD patient organizations within the framework of an embodied health movement [13]. Jason illustrates the success of this approach in the legitimization and destigmatization of chronic fatigue syndrome, a disease which has also been strongly contested by the healthcare system [13]. The advancement of LD research and policy change involves many stakeholders, and progress can be challenged and muted by gatekeepers within the health system. The small wins approach offers insight into the utility of coalition building and the value of oppositional experts. To disrupt the status quo, patient organizations identify allies and manage opportunities to educate and mobilize those with expertise and authority to challenge the practices and politics of their adversaries. However, as Jason notes, social change requires “a long-term time commitment, and the process is often unpredictable as alliances emerge and crumble, and even adversaries become allies” [13] (p. 313). Despite numerous and noteworthy small wins resulting in increased public awareness and recognition through legislation, research commentary and patient narratives show that LD remains steeped in controversy related to restrictive clinical practice guidelines and physicians unfamiliar with the disease [23]. Nonetheless, LD patient organizations persevere, and meaningful alliances with oppositional experts continue to be forged as more Canadians are impacted. As we demonstrate, Jason’s small wins approach has utility in assessing the sometimes-muted gains of LD patient organizations and their capacity to manage both opportunities and setbacks [13].
3. Results
3.1. Polly Murray—The First Lyme Disease Patient Advocate
Progress in LD research has been hampered by setbacks and tensions since it was discovered in Lyme, Connecticut, in the 1970s. Researchers who collected information from LD patients anticipating a cure would later understate the illness experiences of those patients in their publications [29]. Dr. Allen Steere, a rheumatologist at Yale University in the 1970s, is credited with discovering LD; however, it was a patient, Polly Murray, who first recognized a health problem in her community in Connecticut and alerted the State Department of Health. Polly Murray provided Dr. Steere with detailed records of the nature and prevalence of symptoms and continued to pressure state officials to invest in research to understand the complexity of this disease [29]. She described her own debilitating symptoms and those of her family and neighbours so that their illness experiences could be validated, understood, and treated. Murray was thanked for her contribution yet was marginalized, as an editorial in the New England Journal of Medicine states: “The triumph belongs to the inquisitiveness and determination of clinical and laboratory investigators in medicine” [30] (pp. 774–775). Polly Murray’s lack of influence became apparent when Dr. Steere began publishing his findings and communicating information about this “new” disease. The information conveyed did not reflect the persistence and severity of the illness experienced by patients [29]. It was due to the dedication and cooperation of patients in the Lyme community in collaboration with scientists and state officials that this unexplained illness was identified. Though experiential knowledge was already being disputed, the naming of the disease validated the illness and led the way for a health movement that began to unite patients and caregivers across North America and eventually around the world.
3.2. Patients Challenged by LD Diagnosis and Treatment Protocols
Because symptoms of LD mimic other illnesses, misdiagnosis is possible; however, when tests for other diseases are negative and with no objective evidence for their complaints, patients who suspect LD are frequently dismissed and not tested [31,32]. Restrictive guidelines accompanied by investigations and sanctions by regulatory bodies discourage physicians from diagnosing suspected LD that falls outside the guidelines [25]. For example, the Nova Scotia Infectious Diseases Expert Group (IDEG) advises that physicians begin treatment for LD immediately when three criteria are met: (1) signs of a rash known as erythema migrans (EM), (2) it is the season when the black-legged tick vector is predicted to be active, and (3) exposure to a “risk area” where infected ticks have been identified. When a physician suspects LD in the absence of any of these factors, treatment is postponed pending confirmation by two-tiered serologic testing [33]. Patients in Nova Scotia who do not meet the criteria are confronted with delays or have treatment denied due to the lack of “objective” evidence despite their symptoms.
The fact that the illness experience of LD patients does not always conform to Nova Scotia’s IDEG guidelines is consistent with research. EM (e.g., a bulls-eye rash) appears in as few as 9 percent or as many as 80 percent of cases [33,34,35]. While useful for early identification, an over-dependence on this marker can rule out diagnoses when EM is atypical or absent [36]. Similarly, data on the seasonality and “risk areas” associated with the black-legged tick are constantly changing due to climate change [3]. Further uncertainty exists regarding estimates and prediction models with no consensus about the prevalence of infected ticks in targeted areas [4,37]. Combined, patients with presumed LD are potentially denied timely and appropriate care.
Delayed or misdiagnosis is problematic, given patients often experience slower recovery and more persistent symptoms. Cameron reported “that treatment delay is strongly associated with treatment failure for patients with Lyme disease” and, as such, is a precursor for chronic Lyme disease [38] (p. 471). The recommended serological tests are an impediment to timely diagnoses since they are inaccurate during the early stages of the disease, unreliable, and results can take several weeks to obtain [26]. Lloyd and Hawkins propose that accurate diagnosis from serological tests in Canada could be as low as 16.7 percent [4]. After receiving a report that 24 patients had received false-negative test results, Health Canada advised health professionals to use the tests only as an aid and not as the basis for diagnostic or treatment decisions [39]. Despite this caution, Nova Scotia’s IDEG (2020) instructs physicians to look for other causes of illness in the absence of EM and negative test results. The IDEG also advises “against” repeat serological testing, using alternate tests, using laboratories that do not subscribe to the Centers for Disease Control and Prevention (CDC) criteria, and the use of antibiotics beyond the 14–28 day guidelines. These are referenced as voluntary guidelines, but cases exist where physicians in Canada have been investigated for non-compliance [40].
The issue is that such restrictive guidelines are enforced as mandatory and discourage physicians from exercising clinical judgement based on a range of non-specific symptoms [41]. Yet, “it is through diagnosis that an illness gains legitimacy and entry into the medical system” [17] (p. 1667). For patients, this poses an additional burden. The exclusive focus of physicians on objective evidence discounts the subjective illness experience of the patient, particularly when there is divergence, and the patient is sidelined given that physicians remain gatekeepers to treatment [19]. It is the precipitous exclusion of an LD diagnosis prompted by sanctions that discourage clinical judgement, which denies patients validation and timely and appropriate treatment.
Due to the debilitating symptoms associated with LD, some Canadians challenge their family physicians, consult multiple physicians, or travel to the United States for testing and treatment, while those with fewer resources go undiagnosed and untreated [23]. Even with early diagnosis and the recommended course of antibiotics, patients may be at risk if their symptoms persist since the probability of chronic infection is disputed in Canada (discussed below).
At the heart of this issue are the 2006 guidelines developed by the Infectious Diseases Society of America (IDSA), widely endorsed across Canada, which recognize that some LD patients experience persistent symptoms but maintain that there is no evidence of infection post-antibiotic treatment. Physicians are thus advised to manage the symptoms (e.g., prescribe anti-inflammatory medications) or look for other causes [10]. The International Lyme and Associated Diseases Society contested this position by compiling a list of over 700 peer-reviewed articles that support the persistence of LD [42]. Suppression of this evidence not only discounts the probability but also the possibility of persistent infection, thus depriving patients of treatment options.
Canadian physicians, governed by licensing bodies, are advised to follow the guidelines set out by their provincial authorities, which reflect the outdated 2006 IDSA guidelines. This is controversial because panellists who developed the IDSA guidelines in the United States were found to have conflicts of interest associated with patents and diagnostic tests, received compensation from insurance companies to substantiate the denial of coverage for CLD, and were guilty of suppressing evidence [43]. The 2006 guidelines were delisted in the United States in 2016 because they were outdated and did not meet the National Academy of Medicine (NAM) standards yet continue to be cited by authorities in Canada [44,45].
This is problematic because ILADS published medical guidelines for LD in 2015 (that meet NAM standards) acknowledging the prevalence and variability of LD as informed by an array of laboratory tests and patients’ illness experiences [24]. In 2018, the Public Health Agency of Canada added these guidelines to their website [46]; however, many provinces lag behind (e.g., Ontario, Nova Scotia). This may be due to the influence of the Association of Medical Microbiology and Infectious Disease Canada (AMMI), which partners with IDSA and endorses the outdated 2006 guidelines [47]. Note that members of AMMI have prominent positions in public health authorities (e.g., Government of Canada; IDEG; Public Health Ontario).
In 2019, IDSA drafted revised guidelines to replace the outdated 2006 version, but it was rejected by a coalition of over 35 Canadian and American patient organizations collaborating with researchers and practitioners [41]. They stated that the proposed revisions were more restrictive than the 2006 version, the panel membership excluded “representative” patients and their treating physicians, and no allowance was made for clinical judgement. Final revised IDSA guidelines remain unresolved.
Other factors exacerbate obtaining an LD diagnosis. This includes health professionals communicating a low risk of contracting LD despite acknowledging that tick populations are increasing in Canada [48] and the need to meet artificial thresholds of infected ticks in a given area to justify LD testing [10,49]. The possibility of adventitious ticks and the expansion of established populations yet to be surveyed is ignored. The risk of over-diagnosis, over-treatment, and the overuse of resources is also emphasized [49,50,51]. In contrast, patient organizations and their allies support more rigorous diagnostics to manage the complexity of LD and facilitate appropriate diagnosis and timely treatment [28,52]. These factors are amplified by Lloyd and Hawkins, whose study estimates that many cases of LD go “undetected, unreported, and hence potentially untreated” in Canada [4] (p. 16). The challenge for patient organizations is to inform the public of the risks of contracting LD and the associated toll of a misdiagnosis or non-diagnosis.
In addition, the subjective complaints of patients who go undiagnosed are sometimes regarded as psychosomatic rather than biological [53,54]. Persistent symptoms of patients who were previously treated for LD and remain ill may also be suspect [17]. Similarly, parents of children with LD have been accused of “fabricating their children’s symptoms” to get attention [55] (p. 440). When the legitimacy of an illness is contested or labelled “unexplained”, patients are marginalized by physicians and also by family and friends [56]. A lack of medical attention and social support further compromises their health and well-being.
The Canadian healthcare system fails patients whose LD is not diagnosed. Physicians are pressured to conform to guidelines that limit clinical judgement and do not adequately address LD cases. Surveys in Canada have also shown high variability among family physicians regarding knowledge of LD and serological tests [34,49]. Patients who suspect that they have LD but whose symptoms do not conform to the criteria in the outdated IDSA guidelines often seek the opinion of Lyme-literate Medical Doctors, LD specialists who are few in number in Canada [25]. Other patients who have the financial resources travel abroad for diagnosis and treatment [23]. Those with fewer resources may be reluctant to challenge family physicians on whom they are dependent for medical attention. These circumstances mobilize an embodied health movement. As Barker observed, patients not adequately served by the health system seek outpatient organizations, “drawing on their shared embodied expertise”, to validate the illness experience and connect with oppositional experts who will partner with them to identify treatment options and advocate for change [57] (p. 23).
Embodied health movements form when the illness experiences of patients are inconsistent with medical authority accounts [12]. Ecological probability, the appearance of rashes, and serological testing are undisputed aids in the diagnosis of LD, but they are insufficient, leaving LD undetected in many patients who are symptomatic. Debate exists regarding how many patients with LD go undiagnosed and untreated [4,37], but the number of petitions and personal accounts shared on social media and forwarded to politicians (see [58]) is an indication that this is a concern for many Canadians. Not all involved have LD. Some LD advocates may live in “at risk” regions and feel vulnerable themselves, and others know a family member or friend who is living with chronic Lyme. Oppositional experts also participate—scientists provide evidence to challenge the prevailing dogma, and physicians, educated about the complexity of LD, challenge restrictive guidelines when warranted. Patients find allies in those whose evidence-informed research or medical practice includes the illness experience and whose understanding of LD aligns with their own to counter a group who disproportionately downplays their subjective accounts of LD.
3.3. Chronic Lyme Disease
3.3.1. Chronic Lyme Disease versus Post-Treatment Lyme Disease Syndrome
Central in this conflict is the persistence of LD following treatment. Long-term and debilitating symptoms associated with LD are acknowledged by most researchers, but debate exists regarding the clinical term for this condition, which results in confusion for patients and physicians and validates patients’ illness experience. Both chronic Lyme disease (CLD) and post-treatment Lyme disease syndrome (PTLDS) describe symptoms that persist for more than six months [59,60]. However, PTLDS, a term used by IDSA, describes symptoms that follow treatment but are of unknown origin [10], with no treatment protocol and symptoms merged as “medically unexplained”. In contrast, CLD is defined by ILADS as an ongoing infection, including intermittent and previously treated or untreated symptoms [60], warranting further testing and treatment. This distinction is significant.
Diagnosing LD at any stage is challenging since it mimics over 350 medical conditions and was deemed the new “great imitator” in the 1980s [50]. Many questions exist about what causes symptoms to arise and persist, but the fact that CLD “is not recognized by the majority of the medical community in Canada” [61] (p. 13) negates or delays testing and diagnosis and is costly for the healthcare system and patients [62]. Some argue that the fixation on Lyme disease deters patients from seeking proper medical advice and interferes with assessments that could lead to other causes that account for symptoms [50]. Alternatively, Noorani et al. found that patients are driven to seek information and support outside of the health system because their illness experience is challenged by mainstream medicine [63]. It is not the certainty of CLD but its possibility that physicians fail to address that puts patients at risk of inappropriate or no treatment. These types of medical encounters mobilize embodied health movements to transform the dominant epidemiological paradigm [12]. The desired outcome is a healthcare system that acknowledges and responds competently to the complex nature of LD, chronic symptoms, the possibility of persistent infection, and the heterogeneity of the illness experience.
3.3.2. The Burden of Untreated Chronic Lyme Disease
Patient care is largely dictated by parameters set by provinces and the interpretation and discretion exercised by physicians regarding sanctioned practice guidelines. Challenging conventional health care is costly for Canadians suffering from persistent LD symptoms who travel outside of the country in search of diagnosis and treatment. The exact number of how many patients are involved is unknown as a database that tracks individuals does not exist. Generally, patients are denied health insurance coverage for pharmaceuticals and tests when they return to Canada [23]. An inability to work and out-of-pocket expenses are significant burdens for many who suffer from CLD, their families, and caregivers [32,64,65]. The fact that costs are higher than with other infectious diseases warrants attention [66].
Despite claims that LD is over-diagnosed and over-treated and a misuse of resources [49,50,51], there is evidence that greater expense is incurred when LD goes undetected and untreated [62,67,68]. With delays in treatment a factor in persistent symptoms and CLD [38], the reluctance of physicians to diagnose LD and the waiting period for reliable test results undoubtedly come at a great personal cost for patients. Patient organizations challenge public health systems that deny care to LD patients and burden them with the cost of alternative diagnosis and treatment, a direct consequence of having their illness experience discounted [69].
3.4. Small Wins for Patient Organizations—Reassurances Then Status Quo
The first LD group in Canada was the Lyme Borreliosis Society in British Columbia (BC) (1989), which involved researchers who were concerned that LD research was being suppressed [25]. Lyme Ontario (1990) was the first patient-led organization founded by John Scott, who developed debilitating LD symptoms that went undiagnosed for years [25]. Currently, multiple LD patient organizations and support groups exist across Canada. In 2003, CanLyme was established as a pan-Canadian patient organization and resource for information on LD [70]. CanLyme, along with other advocates and patient organizations, strengthened their alliances with oppositional experts by entering into an equal partnership with researchers and healthcare providers in 2017 to form the Canadian Lyme Consortium. The focus of this partnership was to advance patient-centred LD research [71]. The following chronology outlines the small wins and setbacks of LD patient organizations over the past decade.
In 2010, Dr. Brian Schmidt, a senior health executive in BC, completed a government-commissioned report substantiating the concerns of patients and oppositional experts [27]. The report indicated that LD was poorly recognized by BC physicians, tests were inadequate, CLD was a valid diagnosis, the treatment protocol was lacking, and doctors were unfairly targeted for exercising clinical judgement, which breached practice guidelines [72]. It was made public by LD advocate Gwen Barlee through a Freedom of Information request. As a result, the Schmidt Report became front-page news, and BC immediately announced CAD 2 million in funding for research to help patients with complex chronic illnesses, including LD [27]. This culminated in the Complex Chronic Disease Program (CCDP), which was cause for optimism for many LD patients and advocates. There was input from patient organizations with representation from CanLyme on the advisory committee. However, the new program did not adopt the recommendations of the Schmidt Report, and there were no changes in treatment practices. CanLyme thus withdrew its support for the new program in 2013 [73]. After filing another Freedom of Information request in 2014, Gwen Barlee confirmed that promises to improve testing and treatment options had been disregarded in favour of the status quo [74]. In 2015, several physicians with specialties dedicated to treating patients with chronic diseases such as LD resigned from the CCDP “in protest to the administrative restraints” [27]. The Schmidt Report and an investment by the BC government appeared to be significant wins for LD patients and healthcare providers; however, the program’s potential for improved testing and treatment was never realized. Small wins were nonetheless achieved through media attention captured by Barlee due to her determination to access key documents. At one point, she was burdened with a CAD 2160 fee to acquire information, which she raised in four hours through crowdfunding, which shows the solidarity of the LD movement [52].
The Schmidt Report’s eight recommendations were highlighted in a proposed federal framework on LD (Bill C-442) in 2014 [75], which was enacted unanimously by all parties and supported by the Canadian Medical Association [76]. A 2016 conference in Ottawa was organized by the Public Health Agency of Canada (PHAC) to develop the federal framework. Over five hundred patients, caregivers, health professionals, representatives from the federal government, PHAC, CanLyme, and AMMI were in attendance [77]. Many LD patients spoke at the conference, sharing personal experiences with misdiagnosis, a lack of awareness of LD, the failure to provide treatment options, and inaccurate testing and reporting. CanLyme president Jim Wilson stressed the need for patients to be equal partners in LD health policy. The Green Party leader, Elizabeth May, the Minister of Health, Jane Philpott, and the Chief Public Health Officer, Dr. Gregory Taylor, gave assurances that the concerns of the participants would be duly considered and lead to changes in awareness, diagnosis, and treatment [77].
In 2017, the federal Framework for Lyme Disease was released with widespread disappointment among patient organizations, given that their input had been discounted. Briefs were submitted to the House of Commons Standing Committee on Health (HESA) by patients, patient organizations, physicians, and academics in protest because the framework did not reflect the evidence and illness experiences presented at the 2016 conference [78]. When a draft of the framework was shared with stakeholders in February 2017, LymeHope, a patient organization in Ontario, launched “The Ticking Lyme Bomb Petition”, detailing multiple outstanding issues, which quickly garnered over 86,500 signatures [58]. The number of signatures on the petition shows that the momentum of the LD movement has not wavered. Oppositional experts validated the patient narratives and grounded their opposition in scientific evidence (see [78]). The objections of patient organizations to the federal framework achieved further small wins by garnering public attention and awareness.
Other initiatives include LymeHope’s 2017 “Lyme Letters Canada Campaign”, which encouraged Canadians to tell their personal stories and struggles to access treatment for LD. In less than six months, over 2700 letters were delivered in person to the Minister of Health and Chief Public Health Officer [79]. Media attention ensued, and the efforts of LD patient organizations were featured in two issues of MacLean’s magazine in 2017 [28,80]. This illustrates the conviction and capacity of patient organizations to keep LD on the agenda to increase awareness of the disease and of the problems confronted by LD patients in the Canadian health system.
Despite these small wins, Canada has not adopted better testing and treatment protocols. In July 2018, a 37-year-old man from Manitoba who was untreated for LD died of Lyme carditis while waiting for serological testing results [6]. A 42-year-old teacher in Ontario tested negative for LD in 2016. When symptoms persisted for nearly two years, testing in the United States confirmed LD, yet provincial health insurance did not accept the diagnosis because it was not acquired through a Canadian-approved testing facility. The patient has paid CAD 120,000 in medical bills as she continues to manage persistent infection and chronic pain [81]. Others suffer from a range of mental health problems with a Lyme infection that reduces quality of life and increases the risk of suicide [54,82]. Many patients have no means to obtain a second opinion, locate alternative physicians, or pay for testing and treatments in the United States.
4. Discussion and Conclusions
4.1. Ongoing Challenges: Discrediting Patient Organizations
As memberships in patient organizations grow and their alliances with oppositional experts strengthen, there has been backlash from researchers and medical professionals whose authority regarding LD is challenged, especially online. Recent research concluded information on patient organization websites was unreliable because it diverged from government websites and was deemed inaccurate by government employee “experts” [83]. The authors failed to appreciate that patient organizations have the capacity to retrieve and disseminate information more quickly than governments and can be the impetus for changes and updates on government websites. For example, it was the collaborative efforts of patient organizations and human rights activists who successfully appealed to the WHO to update the diagnostic codes for LD, which reflected over twenty-five years of peer-reviewed, evidence-informed research [69]. As Epstein points out, it is “the immediate threat of disease” that motivates patients to become advocates and develop expertise to advance research and change policy [84] (p. 248). It is the embodied experience of LD that prompts the urgency within patient organizations to appraise the legitimacy of both the content and source of new information and share it with peers. Granted, some Internet sources for LD may have good intentions but do not adequately update their websites. There are also Internet predators who exploit uncertainties associated with LD [85]. Such websites must be evaluated independently and fairly with a focus on addressing illicit businesses while supporting reputable sources that have the potential to demystify LD for patients by providing information and peer support.
The discursive marginalization of patients with CLD is further motivation for the embodied health movement. As Epstein contends, through the “melding of credentialed and experiential expertise”, patient organizations can provide current and accurate information empowering patients to make informed decisions about treatment options [84] (p. 249). In a quest for legitimacy, patient organizations rely on evidence-informed research to challenge mainstream medicine. However, as Phillips notes, patient expertise is often dismissed as unscientific, “which makes them [patients] prone to misinterpreting data and can lead to unfounded fears” [18] (p. 263). Interestingly, Phillips discovered that the boundary work that mainstream medicine engages in to maintain authority and discredit patient organizations extends to patient groups. Patients within an embodied health movement maintain that experiential knowledge is necessarily bound with scientific knowledge and censure patients who promote pseudo-science.
4.2. Ongoing Challenges: The Funding Dilemma
A primary role of patient organizations is to lobby for funding for research and education to support better testing, treatment, and prevention. Governments have recently responded by directing tax dollars for this purpose. However, the BC example of the CAD 2 million in provincial funding to launch the CCDP illustrates how objectives can be thwarted. Similarly, the release of the 2017 federal framework on LD was accompanied by CAD 4 million for LD research [27]. Despite assurances given by health officials and politicians at the 2016 conference, patient organizations were denied a role with funds given entirely to the newly formed Canadian Lyme Disease Research Network (CLyDRN) [86]. CLyDRN has been criticized for being disproportionately represented by health professionals and encouraging patient engagement but not sanctioning patient direction by partnering with patient organizations [87]. The majority of the 2016 conference attendees were LD patients; however, their contribution was marginalized in a statement issued by AMMI: “While AMMI Canada recognizes and values the importance of the patient’s perspective in the clinical encounter, anecdotal experiences do not constitute evidence-based science” [88]. What AMMI failed to appreciate was that some LD patients who spoke at the conference were medical professionals and scientists, and many others had been informed by peer-reviewed scientific evidence and oppositional experts and were not as naïve as their statement implied.
Access to funding allows patient organizations to share authority over research priorities and projects, and multiple stakeholder involvement can facilitate transparency and accountability [89]. As Patrick points out, involving patients in research planning and decision-making is necessary for “patient-relevant” outcomes but concedes that “involving patients adds complexity and expense”, yet token involvement remains unacceptable [90] (p. 1063). Strategies are needed to ensure patients can contribute to the process in an equitable fashion. The model adopted by the Canadian Lyme Consortium with patients, researchers, and healthcare providers equally represented is a positive step. However, the Consortium has been criticized and had funding proposals denied by the Canadian Institute of Health Research (CIHR) “because patients were involved as partners” [91]. Such criticism suggests that patient organizations are unwanted and discourages patient-driven research.
In contrast, support exists for independent LD research from families who have experienced LD and were challenged by the Canadian health system. In 2009, an Ontario family who had two members suffering from LD and had to travel to the United States for diagnosis and treatment anonymously donated CAD 500,000 to CanLyme to help fund an independent research facility in Canada [25]. Also, in 2009, Gabe Magnotta, untreated for LD in Canada due to a negative serological test, travelled out of country for diagnosis and treatment and died of a heart attack [92]. His family established the Magnotta Foundation for Vector-Borne Diseases, which awarded CAD 1.4 million to the University of Guelph to establish an LD research laboratory in 2017 [93]. Patient-driven funding has the benefit of being focused not only on scientific evidence but also on the priorities of patients and patient advocates.
4.3. “Small Wins” and Patients in an Embodied Health Movement
Viewed through the framework of an embodied health movement, LD patient organizations in Canada are building momentum as increasing numbers of Canadian patients, caregivers, and citizens are impacted by the disease. Researchers admit that there is much that remains unknown about LD. However, disregard and occasional contempt for the illness experience have contributed to an over-reliance on scientific evidence, which has hampered the advancement of LD research. It is the embodied experience of LD, the first element of the framework, that provides insight to aid diagnosis and treatment, particularly in the absence of objective evidence. Patients are reliant on physicians who have studied and treated LD to exercise clinical judgement and to give LD and the possibility of persistent infection due consideration.
In accordance with the second element of the embodied health framework, LD patient organizations have challenged the dominant epidemiological paradigm, which does not adequately align with their lived experience. Symptoms that are contested, a disease trajectory that is not reflected in case definitions, and restrictive guidelines that deny testing and treatment have mobilized a movement. Progress has been too slow for those who are suffering from LD, and patient organizations remind authorities that there is urgency due to the debilitating symptoms and the increasing prevalence. Those who are impacted the most by LD pursue the authority to set research priorities and contribute to decision-making. Patient organizations are challenging the boundaries upheld by mainstream medicine and encouraging researchers and physicians to partner with patients and validate their experiential knowledge.
The strategy fostered by Canadian patient organizations is collaborative rather than hostile. This is consistent with the third element of the framework. LD patients are resigned to challenge adversaries who deny them care and challenge experiential knowledge but also rely on oppositional experts to achieve their goals. The desired outcome is evidence-informed research and practice. Patient organizations choose to collaborate with scientists to develop better testing and treatments and to collaborate with administrators and politicians to develop better policies. However, one must be wary of ambiguous terms like “patient engagement” that allow token participation but deny authority. The objective is an equal partnership with other stakeholders for transparency and accountability and to ensure that the lived experience of LD is fairly represented and heeded.
The small wins of patient organizations that have accumulated since the time of Polly Murray in Lyme, Connecticut, have had a substantial influence on the progress made on LD. It is the peer support, the dissemination of information, the petitions, the alliances with scientists and physicians, and government lobbying that have advanced research and increased awareness of LD. Many of the achievements of patient organizations have been diminished by setbacks; however, as Jason noted, patient advocacy is a “long-term commitment” [13] (p. 313). It is the persistence of LD patient organizations that ensures that conditions improve for those suffering from LD, albeit slowly.
Author Contributions
Conceptualization, M.C. and M.L.; Methodology, M.C.; Formal Analysis, M.C.; Investigation, M.C.; Writing—Original Draft Preparation, M.C.; Writing—Review and Editing, M.C. and M.L.; Supervision, M.L.; Funding Acquisition, M.C. and M.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by a research grant (CAD 7000) from the Canadian Lyme Disease Foundation’s Atlantic Canada Lyme Research Support Initiative.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article. The data presented in the manuscript are available on request from the first author/corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Vrbova, L.; Middleton, D. Descriptive Epidemiology of Lyme Disease in Ontario: 1999–2004. Can. Commun. Dis. Rep. 2006, 32, 247–257. [Google Scholar] [PubMed]
- US Centers for Disease Control and Prevention. How Many People Get Lyme Disease? Available online: https://www.cdc.gov/lyme/stats/humancases.html (accessed on 13 January 2024).
- Levesque, M.; Klohn, M. A Multiple Streams Approach to Understanding the Issues and Challenges of Lyme Disease Management in Canada’s Maritime Provinces. Int. J. Environ. Res. Public Health 2019, 16, 1531. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, V.; Hawkins, R. Under-detection of Lyme Disease in Canada. Healthcare 2018, 6, 125. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Lyme Disease: Surveillance. Available online: https://www.canada.ca/en/public-health/services/diseases/lyme-disease/surveillance-lyme-disease.html (accessed on 13 January 2024).
- Semproni, M.; Rusk, R.; Wuerz, T. Fatal Lyme Carditis Presenting as Fluctuating High-grade Atrioventricular Block. CMAJ 2020, 192, E574–E577. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, A.; Herman, R.; Rebman, A.; Moon, K.; Aucott, J.; Heaney, C.; Schwartz, B. Obstacles to Diagnosis and Treatment of Lyme Disease in the USA: A Qualitative Study. BMJ Open 2018, 8, e021367. [Google Scholar] [CrossRef]
- Feder, H.M.; Johnson, B.J.; O’Connell, S.; Shapiro, E.D.; Steere, A.; Wormser, G. A Critical Appraisal of “Chronic Lyme Disease”. N. Engl. J. Med. 2007, 357, 1422–1430. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, E.; Wormser, G. Lyme Disease in 2018 What is New (and What is Not). JAMA 2018, 320, 635–636. [Google Scholar] [CrossRef]
- Wormser, G.; Dattwyler, R.; Shapiro, E.; Halperin, J.; Steere, A.; Klempner, M.; Krause, P.; Bakken, J.; Strle, F.; Stanek, G.; et al. The Clinical Assessment, Treatment, and Prevention of Lyme Disease, Human Granulocytic Anaplasmosis, and Babesiosis: Clinical Practice Guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2006, 43, 1089–1134. [Google Scholar] [CrossRef]
- Miles, A.; Loughlin, M. Models in the Balance: Evidence-based Medicine Versus Evidence-informed Individualized Care. J. Eval. Clin. Pract. 2011, 17, 531–536. [Google Scholar] [CrossRef]
- Brown, P.; Zavestoski, S.; McCormick, S.; Mayer, B.; Morello-Frosch, R.; Gasior Altman, R. Embodied Health Movements: New Approaches to Social Movements in Health. Sociol. Health Illn. 2004, 26, 50–80. [Google Scholar] [CrossRef]
- Jason, L. Small Wins Matter in Advocacy Movements: Giving Voice to Patients. Am. J. Community Psychol. 2012, 49, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Ripoche, M.; Irace-Cima, A.; Adam-Poupart, A.; Baron, G.; Bouchard, C.; Carignan, A.; Milord, F.; Ouhoummane, N.; Pilon, P.A.; Thivierge, K.; et al. Current and future burden from Lyme disease in Québec as a result of climate change. Can. Commun. Dis. Rep. 2023, 49, 446–456. [Google Scholar] [CrossRef]
- Szulc, K. Canadians Are Travelling to Mexico for Lyme Disease Treatments. That Worries Health Experts. 9 October 2023. Available online: https://www.cbc.ca/news/health/lyme-disease-mexico-treatment-1.6982720 (accessed on 12 December 2023).
- Green, K. Calgary Family Shares Dire Tale to Raise Awareness of Lyme Disease. 24 April 2023. Available online: https://calgary.ctvnews.ca/calgary-family-shares-dire-tale-to-raise-awareness-of-lyme-disease-1.6369795 (accessed on 6 July 2023).
- Hinds, K.; Sutcliffe, K. Heterodox and Orthodox Discourses in the Case of Lyme Disease: A Synthesis of Arguments. Qual. Health Res. 2019, 29, 1661–1673. [Google Scholar] [CrossRef] [PubMed]
- Phillips, T. ‘Mostly Accurate with Occasional Piles of Bullshit’: Patient ‘Boundary-work’ in an Online Scientific Controversy. Health Sociol. Rev. 2019, 28, 261–276. [Google Scholar] [CrossRef]
- Dumit, J. Illnesses You Have to Fight to Get: Facts as Forces in Uncertain, Emergent Illnesses. Soc. Sci. Med. 2006, 62, 577–590. [Google Scholar] [CrossRef]
- Rebman, A.; Aucott, J.; Weinstein, E.; Bechtold, K.; Smith, K.; Leonard, L. Living in Limbo: Contested Narratives of Patients with Chronic Symptoms Following Lyme Disease. Qual. Health Res. 2017, 27, 534–546. [Google Scholar] [CrossRef]
- Nettleton, S. ‘I Just Want Permission to be Ill’: Towards a Sociology of Medically Unexplained Symptoms. Soc. Sci. Med. 2006, 62, 1167–1178. [Google Scholar] [CrossRef]
- Foster, D. ‘Keep Complaining til Someone Listens’: Exchanges of Tacit Healthcare Knowledge in Online Illness Communities. Soc. Sci. Med. 2016, 166, 25–32. [Google Scholar] [CrossRef]
- Boudreau, C.R.; Lloyd, V.; Gould, O. Motivations and Experiences of Canadians Seeking Treatment for Lyme Disease Outside of the Conventional Canadian Health-care System. J. Patient Exp. 2018, 5, 120–126. [Google Scholar] [CrossRef]
- Stricker, R.; Johnson, L. Chronic Lyme Disease and the “Axis of Evil”. Future Microbiol. 2008, 3, 621–624. [Google Scholar] [CrossRef]
- Ferrie, H. (Ed.) Ending Denial: The Lyme Disease Epidemic: A Canadian Public Health Disaster; Kos Publishing: Caledon, ON, Canada, 2013. [Google Scholar]
- Donta, S.T. Issues in the Diagnosis and Treatment of Lyme Disease. Open Neurol. J. 2012, 6, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Fumano, D. Chronology of Lyme Disease in B.C. and the Complex Chronic Disease Program. The Province. 23 April 2015. Available online: https://www.pressreader.com/canada/the-province/20150423/281599534041366 (accessed on 15 July 2023).
- Kingston, A. How the New Impatient Patient is Disrupting Medicine. MacLean’s. 21 October 2017. Available online: https://www.macleans.ca/society/health/how-the-new-impatient-patient-is-disrupting-medicine/ (accessed on 12 June 2023).
- Murray, P. The Widening Circle: A Lyme Disease Pioneer Tells Her Story; St. Martin’s Press: New York, NY, USA, 1996. [Google Scholar]
- Harris, E.D., Jr. Lyme Disease-Success for Academia and the Community. N. Eng. J. Med. 1983, 308, 773–775. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Vitulano, L.; Lee, R.; Weiss, T.; Colson, E. Experiences of Patients Identifying with Chronic Lyme Disease in the Healthcare System: A Qualitative Study. BMC Fam. Pract. 2014, 15, 79. [Google Scholar] [CrossRef] [PubMed]
- Dankyi, J. Stress, Despair, and Quality of Life: The Lived Experience of Families with Children below 26 Years of Age Diagnosed with Lyme Disease. Ph.D. Dissertation, Capella University, Minneapolis, MN, USA, 2016. [Google Scholar]
- Guidance for Primary Care and Emergency Medicine Providers in the Management of Lyme Disease in Nova Scotia. IDEG. Available online: https://novascotia.ca/dhw/CDPC/documents/statement_for_managing_LD.pdf (accessed on 23 July 2023).
- Henry, B.; Crabtree, A.; Roth, D.; Blackman, D.; Morshed, M. Lyme Disease: Knowledge, Beliefs, and Practices of Physicians in a Low-endemic Area. Can. Fam. Physician 2012, 58, e289–e295. Available online: https://www.cfp.ca/content/cfp/58/5/e289.full.pdf (accessed on 26 May 2020). [PubMed]
- Smith, R.; Schoen, R.; Rahn, D.; Sikand, V.; Nowakowski, J.; Parenti, D.; Holman, M.; Persing, D.; Steere, A. Clinical Characteristics and Treatment Outcome of Early Lyme Disease in Patients with Microbiologically Confirmed Erythema Migrans. Ann. Intern. Med. 2002, 136, 421–428. [Google Scholar] [CrossRef]
- Stonehouse, A.; Studdiford, J.; Henry, C.A. An Update on the Diagnosis and Treatment of Early Lyme Disease: “Focusing on the Bull’s Eye, You May Miss the Mark”. J. Emerg. Med. 2010, 39, e147–e151. [Google Scholar] [CrossRef]
- Ogden, N.; Bouchard, C.; Badcock, J.; Drebot, M.; Elias, S.; Hatchette, T.; Koffi, J.; Leighton, P.; Lindsay, L.R.; Lubelczyk, C.; et al. What is the Real Number of Lyme Disease Cases in Canada? BMC Public Health 2019, 19, 849. [Google Scholar] [CrossRef]
- Cameron, D.J. Consequences of Treatment Delay in Lyme Disease. J. Eval. Clin. Pract. 2007, 13, 470–472. [Google Scholar] [CrossRef]
- Health Canada. Lyme Disease Test Kits and Limitations. Can. Advers. React. Newsl. 2012, 22, 1–2. [Google Scholar]
- Teotonio, I. Lyme Disease is Steeped in Controversy. Now Some Doctors Are Too Afraid to Treat Patients. The Hamilton Spectator. 14 December 2018. Available online: https://www.thespec.com/life/health-wellness/2018/12/14/lyme-disease-is-steeped-in-controversy-now-some-doctors-are-too-afraid-to-treat-patients.html (accessed on 5 June 2020).
- Johnson, L.; Maloney, E. The Ad Hoc Patient and Physician Coalition Comments of the IDSA Proposed Lyme Guidelines 8 August 2019. 2019. Available online: https://www.lymedisease.org/wp-content/uploads/2019/08/Ad-Hoc-Patient-Physician-Coalition-Comments.pdf (accessed on 17 August 2023).
- ILADS. Peer-Reviewed Evidence of Persistence of Lyme Disease Spirochete Borrelia Burgdorferi and Tick-Borne Diseases. 2017. Available online: https://www.ilads.org/wp-content/uploads/2018/07/CLDList-ILADS.pdf (accessed on 16 August 2023).
- Ferguson, J. Cure Unwanted Exploring the Chronic Lyme Disease Controversy and Why Conflicts of Interest in Practice Guidelines May be Guiding us Down the Wrong Path. Am. J. Law Med. 2012, 38, 196–224. [Google Scholar]
- Bailey, J. Lyme Disease Guidelines. CMAJ 2016, 188, 754–755. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Clinical Practice Guidelines We Can Trust; National Academies Press: Washington, DC, USA, 2011; Available online: http://books.nap.edu/openbook.php?record_id=13058 (accessed on 16 August 2023).
- Government of Canada. For Health Professionals: Lyme Disease. 2020. Available online: https://www.canada.ca/en/public-health/services/diseases/lyme-disease/health-professionals-lyme-disease.html#a3 (accessed on 17 September 2023).
- AMMI. AMMI Canada Position Statement on the Diagnosis and Treatment of People with Persistent Symptoms That Have Been Attributed to Lyme Disease. 2020. Available online: https://www.ammi.ca/?ID=137 (accessed on 15 June 2023).
- Glauser, W. Combatting Lyme Disease Myths and the “Chronic Lyme Industry”. CMAJ 2019, 191, E1111–E1112. [Google Scholar] [CrossRef] [PubMed]
- Ferrouillet, C.; Milord, F.; Lambert, L.; Vibien, A.; Ravel, A. Lyme Disease: Knowledge and Practices of Family Practitioners in Southern Quebec. Can. J. Infect. Dis. Med. Microbiol. 2015, 26, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Baker, P.J. Is it Possible to Make a Correct Diagnosis of Lyme Disease on Symptoms Alone? Review of Key Issues and Public Health Implications. Am. J. Med. 2019, 132, 1148–1152. [Google Scholar] [CrossRef] [PubMed]
- Webber, B.; Burganowski, R.; Colton, L.; Escobar, J.; Pathak, S.; Gambino-Shirley, K. Lyme Disease Overdiagnosis in a Large Healthcare System: A Population-based, Retrospective Study. Clin. Microbiol. Infect. 2019, 25, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Fayerman, P. Crowdsourcing Used to Fund Lyme Disease FOI Request. Vancouver Sun. 9 September 2014. Available online: http://www.vancouversun.com/health/crowdsourcing+used+fund+lyme+disease+request/10186216/story.html (accessed on 23 June 2023).
- Csallner, G.; Hofmann, H.; Hausteiner-Wiehle, C. Patients with “Organically Unexplained Symptoms” Presenting to a Borreliosis Clinic: Clinical and Psychobehavioral Characteristics and Quality of Life. Psychosomatics 2013, 54, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Fallon, B.; Nields, J. Lyme Disease: A Neuropsychiatric Illness. Am. J. Psychiatry 1994, 151, 1571–1583. [Google Scholar]
- Sherr, V.T. Munchausen’s Syndrome by Proxy and Lyme Disease: Medical Misogyny or Diagnostic Mystery? Med. Hypotheses 2005, 65, 440–447. [Google Scholar] [CrossRef]
- Nettleton, S.; Watt, I.; O’Malley, L.; Duffey, P. Understanding the Narratives of People Who Live with Medically Unexplained Illness. Patient Educ. Couns. 2005, 56, 205–210. [Google Scholar] [CrossRef]
- Barker, K. Electronic Support Groups, Patient-consumers, and Medicalization: The Case of Contested Illness. J. Health Soc. Behav. 2008, 49, 20–36. [Google Scholar] [CrossRef]
- The Lyme Petition. 2020. Available online: https://www.lymehope.ca/lyme-petition.html (accessed on 21 June 2023).
- Aucott, J.; Rebman, A.; Crowder, L.; Kortte, K. Post-Treatment Lyme Disease Syndrome Symptomatology and the Impact on Life Functioning: Is There Something Here? Qual. Life Res. 2013, 22, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Shor, S.; Green, C.; Szantyr, B.; Phillips, S.; Liegner, K.; Burrascano, J., Jr.; Bransfield, R.; Maloney, E.L. Chronic Lyme Disease: An Evidence-Based Definition by the ILADS Working Group. Antibiotics 2019, 8, 269. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. Lyme Disease in Canada: A Federal Framework. Government of Canada. 2017. Available online: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/lyme-disease-canada-federal-framework.html (accessed on 13 September 2023).
- Adrion, E.; Aucott, J.; Lemke, K.; Weiner, J. Health Care Costs, Utilization and Patterns of Care Following Lyme Disease. PLoS ONE 2015, 10, e0116767. [Google Scholar] [CrossRef] [PubMed]
- Noorani, T.; Karlsson, M.; Borkman, T. Deep Experiential Knowledge: Reflections from Mutual Aid Groups for Evidence-based Practice. Evid. Policy 2019, 15, 217–234. [Google Scholar] [CrossRef]
- Drew, D.; Hewitt, H. A Qualitative Approach to Understanding Patients’ Diagnosis of Lyme Disease. Public Health Nurs. 2006, 23, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; Wilcox, S.; Mankoff, J.; Stricker, R. Severity of Chronic Lyme Disease Compared to Other Chronic Conditions: A Quality of Life Survey. PeerJ 2014, 2, e322. [Google Scholar] [CrossRef] [PubMed]
- van den Wijngaard, C.; Hofhuis, A.; Wong, A.; Harms, M.; de Wit, G.A.; Lugnér, A.; Suijkerbuijk, A.; Mangen, M.-J.; van Pelt, W. The cost of Lyme Borreliosis. Eur. J. Public Health 2017, 27, 538–547. [Google Scholar] [CrossRef]
- Henningsson, A.; Malmvall, B.; Ernerudh, J.; Matussek, A.; Forsberg, P. Neuroborreliosis—An Epidemiological, Clinical and Healthcare Cost Study from an Endemic Area in the South-east of Sweden. Clin. Microbiol. Infect. 2010, 16, 1245–1251. [Google Scholar] [CrossRef]
- Davidsson, M. The Financial Implications of a Well-hidden and Ignored Chronic Lyme Disease Pandemic. Healthcare 2018, 6, 16. [Google Scholar] [CrossRef]
- Luché-Thayer, J.; Ahern, H.; Bransfield, R.; Burrascano, J.; Fierlafijn, A.; Denham, T.; Kraaijeveld, H.; Kravis, J.; McManus, M.; Meseko, C.; et al. The Situation of Human Rights Defenders of Lyme and Relapsing Fever Borreliosis Patients; CreateSpace Independent Publishing Platform: Scotts Valley, CA, USA, 14 July 2018; Available online: http://www.canlyme.com/wp-content/uploads/2018/07/Defendersreport.pdf (accessed on 4 January 2023).
- CanLyme. About. Available online: https://canlyme.com/about/ (accessed on 4 December 2022).
- Canadian Lyme Consortium. Welcome. Available online: http://www.clymec.ca/ (accessed on 4 December 2022).
- Schmidt, B.T. Chronic Lyme Disease in British Columbia. BC: Provincial Health Services Authority. Available online: https://canlyme.com/uploads/Full_Schmidt.pdf (accessed on 24 November 2022).
- Fumano, D. ‘The Health-Care System Has Turned Its Back on Me’: Lyme Disease Sufferers Say Vancouver Clinic Has Been a Failure. The Province. 23 April 2015. Available online: https://www.pressreader.com/canada/the-province/20150423/281479274957078 (accessed on 17 August 2023).
- Hume, M. Crowdfunding Meets Goal to Procure Lyme Disease Program Files. The Globe and Mail. 9 September 2014. Available online: https://www.theglobeandmail.com/news/british-columbia/crowdfunding-for-files-on-treatment-of-lyme-disease-meets-goal/article20487550/ (accessed on 17 August 2023).
- HESA. House of Commons Canada Standing Committee on Health, Meeting No. 30, 2nd Session, 41st Parliament, 29 May 2014. Parliament of Canada. Available online: https://www.ourcommons.ca/DocumentViewer/en/41-2/HESA/meeting-30/evidence (accessed on 6 June 2023).
- Green Party of Canada. Senate Unanimously Passes Elizabeth May’s Federal Framework on Lyme Disease Act. 2014. Available online: https://www.greenparty.ca/en/media-release/2014-12-12/senate-unanimously-passes-elizabeth-may%E2%80%99s-federal-framework-lyme-disease (accessed on 14 May 2023).
- Public Health Agency of Canada. Conference to Develop a Federal Framework on Lyme Disease—15–17 May 2016—Conference Summary Report. 2016. Available online: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/conference-develop-federal-framework-lyme-disease-may-15-17-2016-conference-summary-report.html (accessed on 17 February 2023).
- HESA. Federal Framework on Lyme Disease. House of Commons Standing Committee on Health, 1st Session, 42nd Parliament, 8 June 2017. Parliament of Canada. Available online: https://www.ourcommons.ca/Committees/en/HESA/StudyActivity?studyActivityId=9527827 (accessed on 6 June 2023).
- LymeHope. Meeting with Federal Health Minister Jane Philpott: Delivery of Lyme Letters & Petition. 2017. Available online: https://www.lymehope.ca/advocacy-updates/meeting-with-federal-health-minister-jane-philpott-delivery-of-lyme-letters-petition (accessed on 10 February 2023).
- Kingston, A. The Rise of the Impatient Patient. Maclean’s. 1 December 2017. Available online: https://archive.macleans.ca/article/2017/12/1/the-rise-of-the-impatient-patient (accessed on 9 March 2023).
- Walter, K. Battle with Lyme Disease an Education for St. Catharines Grade 3 Teacher. The Standard. 13 November 2019. Available online: https://www.stcatharinesstandard.ca/news-story/9701837-battle-with-lyme-disease-an-education-for-st-catharines-grade-3-teacher/ (accessed on 9 March 2023).
- Bransfield, R.C. Suicide and Lyme and Associated Diseases. Neuropsychiatr. Dis. Treat. 2017, 13, 1575–1587. [Google Scholar] [CrossRef]
- Journault, A.-A.; Richard, L.; Aenishaenslin, C. Lyme Disease Prevention: A Content Analysis of Canadian Patient Group and Government Websites. Zoonoses Public Health 2020, 67, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Epstein, S. The Politics of Health Mobilization in the United States: The Promise and Pitfalls of “Disease Constituencies”. Soc. Sci. Med. 2016, 165, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Lantos, P.; Shapiro, E.; Auwaerter, P.; Baker, P.; Halperin, J.; McSweegan, E.; Wormser, G. Unorthodox Alternative Therapies Marketed to Treat Lyme Disease. Clin. Infect. Dis. 2015, 60, 1776–1782. [Google Scholar] [CrossRef]
- Rideout, D. Queen’s Receives $4M for New Lyme Disease Research Network. Queen’s Gazette. 15 October 2018. Available online: https://www.queensu.ca/gazette/stories/queen-s-receives-4m-new-lyme-disease-research-network (accessed on 7 November 2022).
- CanLyme. Latest Research Shows Canada’s Decision to Fund Only One Large National Lyme Research Conglomerate Goes against Creation of New Ideas. 2019. Available online: https://canlyme.com/2019/02/16/latest-research-shows-canadas-decision-to-fund-only-one-large-national-lyme-research-conglomerate-goes-against-creation-of-new-ideas/ (accessed on 19 January 2023).
- AMMI. AMMI Position Statement on the Federal Framework on Lyme Disease. 3 April 2017. Available online: https://ammi.ca/wp-content/uploads/2021/09/PositionStatement-PHACFederalFrameworkonLyme-En.pdf (accessed on 23 September 2022).
- Bucchi, M.; Neresini, F. Science and Public Participation. In The Handbook of Science and Technology Studies; Hackett, E.J., Amsterdamska, O., Lynch, M., Wajcman, J., Eds.; MIT Press: Cambridge, MA, USA, 2008; pp. 499–539. [Google Scholar]
- Patrick, K. Realizing the Vision of Patient-relevant Clinical Research. CMAJ 2016, 188, 1063. [Google Scholar] [CrossRef]
- Lloyd, V.; Wills, M.; Sperling, J.; Wilson, J.; Kravis, J.; Faber, S. An Update from the Canadian Lyme Consortium—5 March 2018. Available online: http://www.canlyme.com/wp-content/uploads/2018/03/CLC_moving%20forward.pdf (accessed on 15 December 2022).
- Kingston, A. The Truth about Lyme Disease-Lyme Disease Can Masquerade as MS, ALS, Even Dementia, and Its Numbers Are Growing. So Why is Canada Lagging Behind in Treating It? MacLean’s. 24 March 2014. Available online: https://www.macleans.ca/society/health/the-truth-about-lyme-disease/ (accessed on 5 January 2023).
- Ubelacker, S. University of Guelph Setting up Lab to Research Lyme Disease with $1.4M Donation; The Canadian Press: Toronto, ON, Canada, 14 June 2017; Available online: https://www.ctvnews.ca/health/university-of-guelph-setting-up-lab-to-research-lyme-disease-with-1-4m-donation-1.3458844 (accessed on 5 June 2020).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Cox, M.; Levesque, M. “Small Wins” for those with Lyme Disease in Canada: Patients in an Embodied Health Movement. Zoonotic Dis. 2024, 4, 22-36. https://doi.org/10.3390/zoonoticdis4010004
AMA Style
Cox M, Levesque M. “Small Wins” for those with Lyme Disease in Canada: Patients in an Embodied Health Movement. Zoonotic Diseases. 2024; 4(1):22-36. https://doi.org/10.3390/zoonoticdis4010004
Chicago/Turabian StyleCox, Marilyn, and Mario Levesque. 2024. "“Small Wins” for those with Lyme Disease in Canada: Patients in an Embodied Health Movement" Zoonotic Diseases 4, no. 1: 22-36. https://doi.org/10.3390/zoonoticdis4010004