1. Introduction
Traumatic spinal cord injury (TMSI) is characterized by the abrupt interruption of nerve stimuli in the cone or cauda equina due to a blunt force, causing anatomical changes that may alter motor, autonomous, sensory, and psychoaffective functions in the patient [
1]. According to worldwide epidemiological data, 15 to 40 individuals suffer TSCI per million people. In the U.S., 12,000 new cases of TSCI are recorded per year, while in Brazil this number is between 6000 and 8000, of which 80% are male, and 60% are between 10 and 30 years of age [
2] and young adult males between the ages of 18 and 40 who are fully employed and contribute to the country’s gross domestic product (GDP) [
3].
The main causes of TSCI are motor accidents, gunshot and knife wounds, falls, sports, work accidents, and diving into shallow water [
2]. Most patients are young males and most of these cases lead to complications, especially involving fecal incontinence, sexual dysfunction, and reduced or absent sensory reflexes that negatively affect quality of life (QOL), way of life, and the capacity to live a healthy lifestyle [
2,
3,
4,
5].
People with LMT need to adapt to develop coping strategies for their new health condition [
2]. In this context, resilience stands out as an important factor in personal construction and strengthening in the face of the environmental and individual resources available at the time [
5].
In this regard, any changes resulting from the injury can be associated with low mood, depression, and suicidal ideation and behavior. Suicidal behavior is considered a worldwide social phenomenon and a serious public health problem. It mostly occurs within a continuum of events that includes suicidal ideation, suicide planning, failed suicide attempts, and death by suicide [
6,
7].
It is important to note that the World Health Organization (WHO) suicide prevention manual for primary healthcare professionals mentions neurological impairments resulting from SCI and head injuries as one of the risk factors for suicide, with the severity of injury being directly proportional to the increased risk of ending one’s own life [
8].
The term chosen to describe this complex phenomenon in this study was suicidal ideation. This is the term used by the Beck Scale for Suicide Ideation [
9], which is one of the most widely employed instruments worldwide to measure the severity of suicidal behavior, and which was also used in this study.
Research aimed at testing the association between LMT and the development of depression has shown that a large proportion of people belonging to this group develop depressive symptoms, with recurrent thoughts of death, suicide ideation, behavior, and suicide attempts [
10].
A cohort study conducted in two British rehabilitation centers that assessed the cause of death of 533 patients with TSCI identified suicide as the cause of death for 4.2% of individuals. Of these deaths, 91% occurred in the first ten years after trauma. Moreover, the findings revealed that overall mortality and death by suicide significantly increased in individuals who suffered TSCI due to a suicide attempt when compared with those in the remaining sample [
11].
Thus, considering the magnitude of the problem, the repercussions of sudden trauma, the emotional, physical, and social complications, and the lack of Brazilian studies on the subject, this study aims to evaluate factors associated with suicidal ideation in people with TSCI. It is hoped that this study will contribute to the development and improvement of strategies for the rehabilitation of people with TSCI.
2. Materials and Methods
2.1. Study Design
This is a descriptive, cross-sectional study conducted in a virtual environment after the participants signed an online informed consent form
2.2. Location, Population, and Sample
The study included 200 individuals with TSCI aged 18 years or older and living in Brazil. These individuals were selected after they voluntarily registered to participate in studies on TSCI at the Center for Research and Care in Neuropsychomotor Rehabilitation—Neurorehab of Ribeirao Preto School of Nursing, University of São Paulo. To announce the study, specific links for e-mail or messaging applications were sent to the 700 registered volunteers until a sample of 200 individuals was obtained.
2.3. Inclusion and Exclusion Criteria
Brazilian adults with SCI, registered as volunteers to participate in research on spinal cord injury from the Neurorehab research group and with access to the internet were included. Individuals who did not complete the questionnaire in full were excluded.
2.4. Data Collection
Data were collected from March to May 2018 via the SurveyMonkey® virtual platform, which made it possible to investigate participants from all regions of Brazil.
Data were collected using SurveyMonkey®, supported by two research tools previously approved in a pre-test by four judges, namely the Beck Scale for Suicide Ideation (BSI) and a form created using Core Dataset® and developed by the International Spinal Cord Society (ISCOS).
The BSI is capable of measuring the extent of motivation and planning of suicidal be-havior, as well as detecting the presence of suicidal ideation. The BSI was translated into Portuguese and adapted for use in Brazil by Jurema Alcides Cunha. It is used to measure the level of motivation and planning of suicidal behavior and to detect suicidal ideation through 21 groups of statements, answered on a scale of 0 to 3 [
9]. The first 19 items grade the severity of suicidal wishes, attitudes, and plans, as follows: (I) wish to live; (II) wish to die; (III) reasons for living or dying; (IV) active suicide attempt; (V) passive suicide attempt; (VI) duration of suicide ideation; (VII) frequency of ideation; VIII) attitude toward ideation; (IX) control over suicidal action; (X) deterrents to attempt; (XI) reason for attempt; (XII) specificity of planning; (XIII) availability or opportunity of method; (XIV) capability to carry out attempt; (XV) expectancy of actual attempt; (XVI) extent of actual preparation; (XVII) suicide note; (XVIII) final acts; (XIX) deception and concealment [
9]. Although the last two items are not counted in the final score, they are informative and specify the number of previous suicide attempts and the intention to die in the latest attempt.
These last two items are (XX) tiredness or fatigue and (XXI) loss of interest in sex. The final BSI value can vary between 0 and 38, where the higher the value, the greater the risk of suicide. The authors Beck and Steer neither differentiate between different degrees of suicide risk, nor do they determine cut-off values.
It was necessary to reorganize the logic of the groups of statements that made up the scale when transposing the instrument onto the digital platform used.
A form based on Core Dataset
® developed by the International Spinal Cord Society (ISCOS) [
12] was used to characterize the study participants. This questionnaire assessed sociodemographic data such as date of birth, rehabilitation service attended, level of spinal cord injury, city and state, level of education, occupation, and family income. In-formation regarding the severity of the spinal cord injury, details of hospitalization and the use of ventilatory support (e.g., mechanical ventilation) were not investigated because the ISCOS form was self-administered, and participants were unable to answer more in-depth questions about their clinical condition.
2.5. Data Analysis
For data analysis, descriptive data analysis was performed using absolute frequencies. The presence of suicidal ideation was based on any positive score given by the participant.
Statistically, the authors used bilateral tests for categorical variables and Fisher’s exact test. To compare the numerical variables, the Kruskal–Wallis non-parametric test was used. The p-value of 0.05 was the limit for statistical significance.
2.6. Ethical Considerations
In accordance with Resolution 510/16 of the Brazilian Ministry of Health’s National Commission for Research Ethics, on research involving human subjects, this study was approved by the Ethics Committee for Research with Human Subjects of the Ribeirão Preto School of Nursing, University of São Paulo, after being submitted to Plataforma Brazil under protocol number CAAE: 79532717.7.0000.5393.
3. Results
Based on the questionnaire administered, it was possible to ascertain the profile of the participants and the characteristics of their injury, according to gender; region of origin; level of education; occupation; family income; cause of injury; and the consequence of injury. Based on this data,
Table 1 was produced, which characterizes the sociodemographic and epidemiological profile of the participants in this study.
The sample consisted of 200 participants, aged between 18 and 60 years, with a mean of 36.22 and a standard deviation of 9.17. The mean time of injury occurrence was 134.4 months (approximately 11 years), with a standard deviation of 128.40.
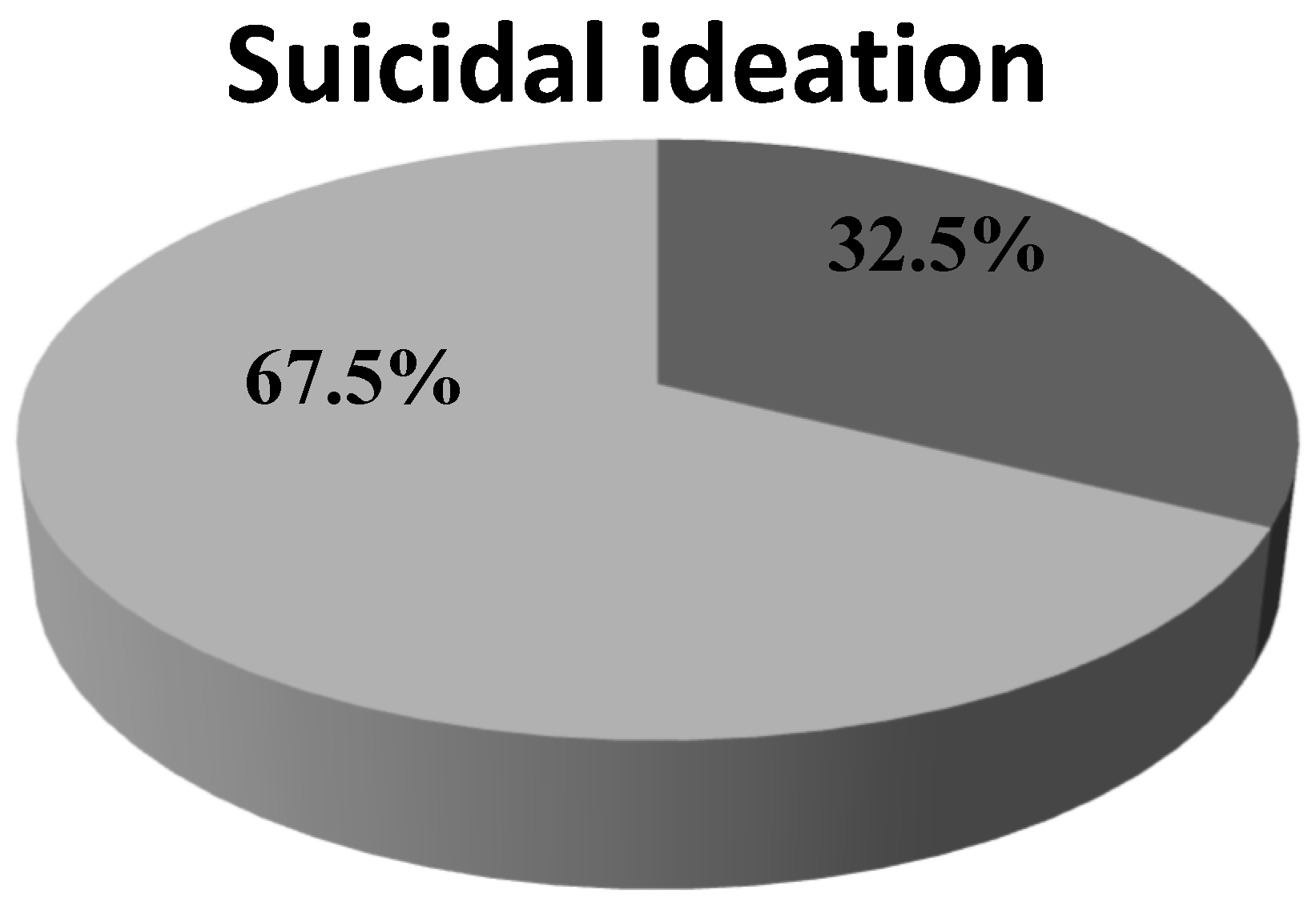
Regarding the presence of suicidal ideation in the sample studied, it was found that 65 participants showed suicidal ideation; this percentage can be seen in
Figure 1.
The gender variable and the prevalence of suicidal ideation in the population studied were cross-referenced. Among the interviewees, 149 were male and 51 were female. The presence of suicidal ideation was also verified in relation to the variables of schooling, rehabilitation, and the consequence of injury.
Table 2 shows the differences between the variables gender, type of injury, rehabilitation, and education in the presence of suicidal ideation. No statistically significant associations were found.
Table 3 shows the influence of the duration (in months) of spinal cord injury on the presence of suicidal ideation, along with the mean, median, and standard deviation. A statistically significant relationship was found between suicidal ideation and the duration of injury (
p ≤ 0.0085). It was observed that the shorter the duration of the spinal cord injury, the greater the likelihood of suicidal ideation.
4. Discussion
The results of this study corroborate the findings of the national and international literature by revealing a high prevalence of TSCI in young males, retired/on benefits, with a monthly income of one to three minimum wages, and with motor accidents being the main cause of TSCI [
13,
14,
15]. In addition to the individual impacts, TSCI directly impacts the socioeconomic structure of the country and becomes a public issue since the affected individuals are at a productive age. Therefore, the socioeconomic impact of TSCI directly involves a high cost per person to the country.
The individual and social impacts are widely observed in this population. However, studies indicate the influence of TSCI on family construction, associated both with economic issues, as has been observed so far, and with ways of reorganizing the family nucleus, since family members take on new responsibilities to supplement their income and care for the person affected by TSCI [
16].
A cross-sectional study carried out in the municipality of Campina Grande-PB, in north-eastern Brazil, analyzed family functionality in relation to the coping strategies of people with TSCI. The results revealed family functionality in 72 per cent of cases. In addition, the logistic model showed relationships of probability (OR = 0.539—factor 2) and social support (OR = 1.997—factor 4) with emotion-focused family functionality and social support with family functionality [
17]. In addition, about the family situation, the literature indicates that the family is the first and main social support factor for individuals with TSCI. In this sense, the importance of including the family group in the rehabilitation process stands out, since everyone is affected by the occurrence of TSCI [
16].
About the presence of suicidal ideation, the findings of this study are consistent with those of previous studies that identified an association between the variables of depressive and anxious symptoms, and the recurrence of thoughts about death and suicidal ideation in people with TSCI [
5,
13,
15,
16,
17,
18]. Such results can be explained by the psychological reactions associated with insecurity, anxiety, social isolation, hopelessness, and difficulty in expressing deep emotional needs post-injury.
When analyzing sociodemographic variables with the presence of suicidal ideation, the results reinforced the prevalence of men over women, although this was not statistically significant. Globally, suicide is more frequent in men than in women, although women exhibit more non-fatal suicidal behavior, including the expression of suicidal ideation and suicide attempts [
18]. A possible hypothesis for these findings would consider the direct impact of TSCI on daily living activities, which results in dependence on others for basic needs such as feeding, locomotion, hygiene, and dressing.
About the consequence of injury variable, a higher incidence of suicidal ideation was identified in participants who stated that they were paraplegic. Although no significant association was found, this finding is concerning, as individuals with paraplegia who intend to commit suicide may have greater access to possible suicide methods due to upper limb function, especially in adapted and accessible environments. According to a literature review, physical sequelae are strongly associated with depression and lower satisfaction with life [
8].
Regarding rehabilitation, it was assumed that individuals with TSCI who had greater access to rehabilitation services would score lower for suicidal ideation. Surprisingly, the opposite was identified. A qualitative study conducted with 23 people with TSCI living in Maringá, state of Paraná, Brazil, identified that the participants view rehabilitation and health centers as support resources in their adaptation to living with the condition [
18]. The guidelines of the Care Network for People with Disabilities of the Unified Health System (UHS) stress the need to enhance rehabilitation and disability prevention through coordinated efforts between all healthcare services [
8].
Prior to the study, it was assumed that individuals with TSCI who had greater access to rehabilitation services would have lower rates of suicidal ideation. Research evaluating coping with TSCI characterizes social support as one of the main factors responsible for the development of successful coping strategies. Additionally, they show that the weakness or absence of social support is directly associated with high suicide rates in this population [
19].
However, the results of this study show the opposite. Individuals who attended rehabilitation services had higher percentages of suicidal ideation (28 per cent) compared to those who did not.
Considering that, in this study, any score other than zero on the Beck scale was classified as “with suicidal ideation”, this classification may also have included people who did not necessarily have active suicidal ideation, i.e., cases in which thoughts of death or fewer reasons to live were present. Thus, it is possible that individuals being monitored in a rehabilitation service were more symptomatic or that they found it easier to recognize and express feelings and needs related to mental health, aspects that can be taboo in many situations.
Authors define rehabilitation as a limited process carried out by a multi-professional team that jointly implements healthcare actions. These actions aim to achieve a high degree of physical, functional, mental, and social development, allowing the individual to set and achieve new goals [
4].
In the present study, every non-zero score on the Beck scale was classified as “suicidal ideation”, which may have included people who did not necessarily have active suicidal ideation, i.e., cases in which the participants thought about death or believed they had fewer reasons to live. Thus, the individuals in follow-up rehabilitation may have been more symptomatic or more easily recognized and may have expressed their feelings and mental health needs, which can be taboo in several situations.
Another alarming finding concerns education, since the participants who had finished high school and had complete/incomplete higher education, representing most of the sample, exhibited suicidal ideation. Due to the association between years of education, greater access to the job market, and consequent financial stability, this could be considered a predictor of access to quality rehabilitation services [
8,
9,
10,
11,
12,
13,
14,
15,
16,
17]. Individual and social impacts are widely observed in this population and more years of education can in fact have a seriously harmful influence on suicide plans and attempts. In this sense, a support network with a unique therapeutic approach for each person with TSCI becomes critical.
Regarding the duration of injury, a significant difference was observed between this variable and suicidal ideation. These results corroborate a study conducted in the cities of Ribeirão Preto (SP) and Florianópolis (SC) with 81 people with TSCI that revealed the significant influence of the duration of injury on suicidal ideation in 86.4% of the sample [
15].
The suicidal ideation scores in this study, especially in the first five years of the inju-ry, reinforce the fact that spinal cord impairment causes physical, psychological, and so-cial transformations, which the affected individual will have to deal with through internal and external coping strategies [
16].
Jointly, these findings reinforce the hypothesis that, even after years of TSCI, these individuals still suffer from psychological reactions associated with insecurity, anxiety, social isolation, hopelessness, and difficulty in expressing deep emotional needs. This stresses the need for support that targets a high degree of physical, functional, mental, and social development and allows individuals with TSCI to establish and reach new goals.
Studies that have analyzed depressive and anxiety symptoms in people with PTL indicate the recurrent presence of thoughts about death and suicidal ideation in this population, including suicide plans and attempts. They also highlight the significant presence of psychological reactions associated with insecurity, anxiety, social isolation, hopelessness, and difficulty in expressing deep emotional needs [
15,
16,
17,
18,
20,
21].
No studies were found, primarily in the Brazilian literature, that evaluated the association between sociodemographic variables and suicidal ideation in people with TSCI and had a methodology like that of this study, which was based on the Beck Scale of Suicide Ideation (BSI). Therefore, it was not possible to compare the results found in the present study with those of prior studies. Further studies should be conducted in Brazil and internationally with the same methodology.
4.1. Implications for Practice
Spinal cord injury as a chronic condition [
22] must be managed, taking into account suicidal ideation, because as the years after injury increase, the presence of this increases. In this sense, it is necessary to recognize how individuals with TSCI live their experience regarding adjustment, coping, grief, and resilience [
23]. Also, to understanding the experience of people with spinal cord injury can help healthcare professionals to develop a better understanding of the needs of other people with chronic illnesses.
On the other hand, it is necessary to carry out early detection (i.e., screening assessments) and plan intervention strategies to reduce suicide risk among people living with TSCI [
24]. Improving TSCI patients’ access to healthcare and community resources may decrease the risk of suicide, as there will be increased contact with healthcare providers, mental health services, and peer support, which may alleviate the effect of physical comorbidities and psychological suffering. Furthermore, the use of mobile health technology and telehealth services could be an opportunity to improve access to health services and coordination of care for these patients [
25,
26].
4.2. Limitations
Limitations include the use of a cross-sectional model, which makes it impossible to identify cause and effect relationships between the variables explored. It is also pointed out that collecting data through a virtual platform may have limited and hindered the participation of a portion of the Brazilian population without internet access. In this sense, studies that include the collection of data from people without internet access could add other relevant data. Another limitation concerns the adaptation of the data collection tool, given the need to reorganize the logic of the groups of statements that made up the scale when the tool was transferred to the digital platform.
4.3. Future Indications
It is necessary to increase the number of studies, with more rigorous designs and with larger, representative samples of this population to draw informed conclusions about the risk of suicide. It is also necessary to carry out comparative studies including other countries. It is necessary to increase the number of studies, with more rigorous designs and with larger, representative samples of this population to draw informed conclusions about the risk of suicide. It is necessary to carry out comparative studies including other countries to explore the variable time of injury and design interventions to manage chronic conditions with the least psychological distress and reduce the presence of suicidal ideation and suicide.


 ,
, 




{kind=link}