
Reliability and Repeatability of ACL Quick Check®: A Methodology for on Field Lower Limb Joint Kinematics and Kinetics Assessment in Sport Applications

 ,
,  ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
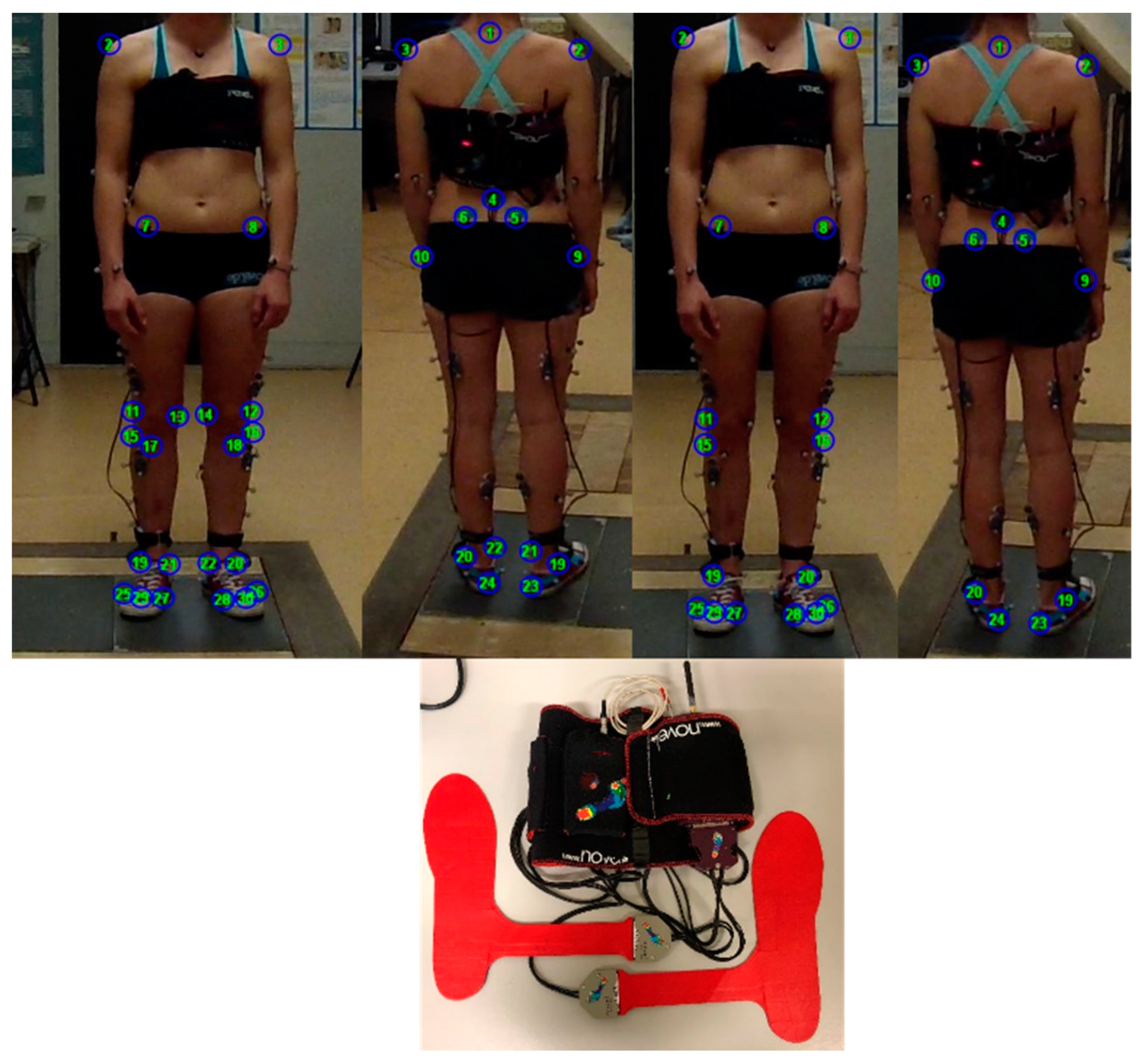
2.2. Instrumental Protocol
2.3. Data Analysis
- hip, knee, ankle abduction-adduction and flexion extension moments considering two different marker sets, the ACL Quick Check® with the complete IORgait marker set [42] (referred to as ACL Quick Check® integrated in the following paragraphs) and the ACL Quick Check® with a simplified marker set as in [47]. Differently from the original publication [42], in both versions the hip joint center was determined according to the regression equations proposed by Harrington et al. (2007) [54]
2.3.1. Reliability Analysis
- 3D joint centers trajectories computed by means of stereophotogrammetry vs. video based (TOF). This comparison aims to identify the influence of differences in the estimation of the joint centers’ trajectories on joint angles and intersegmental moments, given that joint center positions are used either to define the moment arm of the forces acting on the segment or segment length that are involved in the assessment of body segment inertial parameters [49].
- sagittal plane kinematics based on the marker trajectories reconstructed through stereophotogrammetry vs. the ones reconstructed through TOF.
- vertical component of GRF recorded through the force plates vs. the one retrieved through the plantar pressure system.
- COP displacement recorded through the force plates vs. the one retrieved through the plantar pressure system. In order to compare the two COP paths a rigid transformation was applied to define the COP coordinates of the plantar insoles with respect to the force plates reference system [60].
- e.
- flexion-extension and abduction-adduction joint moments retrieved according to inverse dynamics procedures (Newton–Euler) [60] by considering the markers’ trajectories reconstructed through stereophotogrammetry combined with the GRF from the force plate, ACL Quick Check® integrated
- f.
- flexion-extension and abduction-adduction joint moments retrieved according to the Ground Reaction Vector approach, which consists of multiplying the ground reaction force vector by its moment arm at each joint (Ground Reaction Vector 3D) [48] ACL Quick Check® integrated. In this case Ground Reaction Vector 3D was applied by considering the markers’ trajectories reconstructed through stereophotogrammetry.
- g.
- flexion-extension and ab- and adduction joint moments retrieved according to the Ground Reaction Vector approach but considering only the vertical component of the GRF (Ground Reaction Vector 1D) and the markers trajectories reconstructed through stereophotogrammetry vs. ACL Quick Check® integrated
- h.
- ACL Quick Check® integrated applied by considering the data acquired with the stereophotogrammetric system and the plantar pressure system (ACL Quick Check® integrated STF) vs. ACL Quick Check® integrated applied by considering the data acquired with commercial video cameras and the plantar pressure system.
- i.
- ACL Quick Check® integrated vs. ACL Quick Check®
- 0.65–0.75: moderate
- 0.75–0.85: good
- 0.85–0.95: very good
- 0.95–1: excellent
2.3.2. Repeatability Analysis
3. Results
3.1. Reliability of the Proposed Approach
3.2. Inter-Rater Repeatability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Case Study

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | Age [Years] Mean (SD) | Weight [Kg] Mean (SD) | Height [m] Mean (SD) | BMI [Kg/m2] Mean (SD) | Shoe Size Mean (SD) |
|---|---|---|---|---|---|
| ACL-S | 27 | 68 | 1.77 | 21.7 | 42 |




Appendix B
| Model | Size (mm) | Weight (kg) | Rated Load (kN) | Natural Frequency (hz) | |||||
|---|---|---|---|---|---|---|---|---|---|
| L | W | H | Fz | Fx, Fy | Fz | Fx | Fy | ||
| 4060-08 | 600 | 400 | 83 | 28 | 10 | 5 | 340 | 550 | 540 |
| Shoe Size | 36 to 46 (European) |
|---|---|
| thickness (mm) | 1.9 |
| number of sensors | 99 |
| pressure range (kPa) | 15–600 |
| hysteresis (%) | <7 |
| resolution (kPa) | 2.5 |
| measurement frequency (Hz) | 100 |
| offset temperature drift (kPa/K) | <0.5 |
| minimal bending radius (mm) | 20 |
| DX 400 | |
|---|---|
| Infrared digital cameras per datastation | up to 16 |
| Sensor Resolution | 1 Mpixel |
| Acquisition frequency at maximum resolution | 100 fps |
| Maximum acquisition frequency | 300 fps |
| Accuracy/Volume | <0.3 mm on 4 × 3 × 3m |
Appendix C
Appendix C.1. Joint Moment Calculation Following the “Ground Reaction Vector” Approach
- i
- ith joint (ankle, knee, hip)
- loc
- local reference system at the (ankle, knee, hip)
- glob
- global reference system of the laboratory, the y axes oriented vertically perpendicular to the floor
- M
- joint moment at the ith joint in the local or global reference system
- COP
- point of application of the ground reaction force vector
- JC
- joint center of the ith joint
- F
- ground reaction force vector
- rotation matrix that convert a vector expressed in the global reference system to the ith local reference system
Appendix C.2. Joint Moment Calculation Following the Inverse Dynamic Approach
- Ix, Iy, Iz
- moments of inertia about x–y–z axes
- , ,
- components of angular velocity about x–y–z axes
- , ,
- components of angular acceleration about x–y–z axes
- Mxd, Myd, Mzd
- previously transformed distal moments about x–y–z axes
- Rxd, Rxp, Ryd, Ryp, Rzd, Rzp
- previously transformed joint reaction forces about x–y–z axes
- Ip, Id
- distances from center of mass to proximal and distal joints
Appendix C.3. Joint Moment Calculation Following the ACL Quick Check® Approach
Appendix C.4. Video Based Reconstruction of Anatomical Landmark Points
Appendix C.5. Joint Angles Calculation

References
- Montalvo, A.M.; Schneider, D.K.; Webster, K.E.; Yut, L.; Galloway, M.T.; Heidt, R.S.; Kaeding, C.C.; Kremcheck, T.E.; Magnussen, R.A.; Parikh, S.N.; et al. Anterior Cruciate Ligament Injury Risk in Sport: A Systematic Review and Meta-Analysis of Injury Incidence by Sex and Sport Classification. J. Athl. Train. 2019, 54, 472–482. [Google Scholar] [CrossRef] [PubMed]
- Gans, I.; Retzky, J.S.; Jones, L.C.; Tanaka, M.J. Epidemiology of Recurrent Anterior Cruciate Ligament Injuries in National Collegiate Athletic Association Sports: The Injury Surveillance Program, 2004-2014. Orthop. J. Sports Med. 2018, 6, 2325967118777823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grassi, A.; Macchiarola, L.; Filippini, M.; Lucidi, G.A.; Della Villa, F.; Zaffagnini, S. Epidemiology of Anterior Cruciate Ligament Injury in Italian First Division Soccer Players. Sports Health 2020, 12, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Sawacha, Z.; Ciniglio, A.; Scaldaferro, A.; Spolaor, F. Motion Analysis for ACL Injuries Prevention in Sport: A Systematic Review. Minerva Orthop. 2021, 72, 465–473. [Google Scholar] [CrossRef]
- Montalvo, A.M.; Schneider, D.K.; Yut, L.; Webster, K.E.; Beynnon, B.; Kocher, M.S.; Myer, G.D. “What’s My Risk of Sustaining an ACL Injury While Playing Sports?” A Systematic Review with Meta-Analysis. Br. J. Sports Med. 2019, 53, 1003–1012. [Google Scholar] [CrossRef]
- Lai, C.C.H.; Ardern, C.L.; Feller, J.A.; Webster, K.E. Eighty-Three per Cent of Elite Athletes Return to Preinjury Sport after Anterior Cruciate Ligament Reconstruction: A Systematic Review with Meta-Analysis of Return to Sport Rates, Graft Rupture Rates and Performance Outcomes. Br. J. Sports Med. 2018, 52, 128–138. [Google Scholar] [CrossRef]
- Bonnette, S.; Diekfuss, J.A.; Grooms, D.R.; Kiefer, A.W.; Riley, M.A.; Riehm, C.; Moore, C.; Barber Foss, K.D.; DiCesare, C.A.; Baumeister, J.; et al. Electrocortical Dynamics Differentiate Athletes Exhibiting Low- and High- ACL Injury Risk Biomechanics. Psychophysiology 2020, 57, e13530. [Google Scholar] [CrossRef]
- Siegel, L.; Vandenakker-Albanese, C.; Siegel, D. Anterior Cruciate Ligament Injuries: Anatomy, Physiology, Biomechanics, and Management. Clin. J. Sport Med. 2012, 22, 349–355. [Google Scholar] [CrossRef] [Green Version]
- Tak, I.; Wiertz, W.-P.; Barendrecht, M.; Langhout, R. Validity of a New 3-D Motion Analysis Tool for the Assessment of Knee, Hip and Spine Joint Angles during the Single Leg Squat. Sensors 2020, 20, 4539. [Google Scholar] [CrossRef]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Paterno, M.V.; Quatman, C.E. Mechanisms, Prediction, and Prevention of ACL Injuries: Cut Risk with Three Sharpened and Validated Tools. J. Orthop. Res. 2016, 34, 1843–1855. [Google Scholar] [CrossRef] [Green Version]
- Bonnette, S.; DiCesare, C.A.; Kiefer, A.W.; Riley, M.A.; Foss, K.D.B.; Thomas, S.; Diekfuss, J.A.; Myer, G.D. A Technical Report on the Development of a Real-Time Visual Biofeedback System to Optimize Motor Learning and Movement Deficit Correction. J. Sports Sci. Med. 2020, 19, 84–94. [Google Scholar]
- Yamazaki, J.; Muneta, T.; Ju, Y.J.; Sekiya, I. Differences in Kinematics of Single Leg Squatting between Anterior Cruciate Ligament-Injured Patients and Healthy Controls. Knee Surg Sports Traumatol. Arthrosc. 2010, 18, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Saito, A.; Okada, K.; Sasaki, M.; Wakasa, M. Influence of the Trunk Position on Knee Kinematics during the Single-Leg Landing: Implications for Injury Prevention. Sports Biomech. 2020, 1–14. [Google Scholar] [CrossRef]
- Fox, A.S.; Bonacci, J.; McLean, S.G.; Saunders, N. Exploring Individual Adaptations to an Anterior Cruciate Ligament Injury Prevention Programme. Knee 2018, 25, 83–98. [Google Scholar] [CrossRef] [PubMed]
- Escamilla, R.F.; Macleod, T.D.; Wilk, K.E.; Paulos, L.; Andrews, J.R. Anterior Cruciate Ligament Strain and Tensile Forces for Weight-Bearing and Non-Weight-Bearing Exercises: A Guide to Exercise Selection. J. Orthop. Sports Phys. 2012, 42, 208–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, M.C.; Murphy, S.; Macpherson, T.; English, B.; Spears, I.; Chesterton, P. Effect of Sand on Knee Load During a Single-Leg Jump Task: Implications for Injury Prevention and Rehabilitation Programs. J. Strength Cond. Res. 2020, 34, 3164–3172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gnacinski, S.L.; Cornell, D.J.; Meyer, B.B.; Arvinen-Barrow, M.; Earl-Boehm, J.E. Functional Movement Screen Factorial Validity and Measurement Invariance Across Sex Among Collegiate Student-Athletes. J. Strength Cond. Res. 2016, 30, 3388–3395. [Google Scholar] [CrossRef]
- Gribble, P.A.; Hertel, J.; Plisky, P. Using the Star Excursion Balance Test to Assess Dynamic Postural-Control Deficits and Outcomes in Lower Extremity Injury: A Literature and Systematic Review. J. Athl. Train. 2012, 47, 339–357. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, S.W.; Teyhen, D.S.; Lorenson, C.L.; Warren, R.L.; Koreerat, C.M.; Straseske, C.A.; Childs, J.D. Y-Balance Test: A Reliability Study Involving Multiple Raters. Mil. Med. 2013, 178, 1264–1270. [Google Scholar] [CrossRef] [Green Version]
- Krosshaug, T.; Steffen, K.; Kristianslund, E.; Nilstad, A.; Mok, K.-M.; Myklebust, G.; Andersen, T.E.; Holme, I.; Engebretsen, L.; Bahr, R. The Vertical Drop Jump Is a Poor Screening Test for ACL Injuries in Female Elite Soccer and Handball Players: A Prospective Cohort Study of 710 Athletes. Am. J. Sports Med. 2016, 44, 874–883. [Google Scholar] [CrossRef] [Green Version]
- Hanzlíková, I.; Hébert-Losier, K. Is the Landing Error Scoring System Reliable and Valid? A Systematic Review. Sports Health 2020, 12, 181–188. [Google Scholar] [CrossRef]
- Myer, G.D.; Ford, K.R.; Hewett, T.E. Tuck Jump Assessment for Reducing Anterior Cruciate Ligament Injury Risk. Athl. Today 2008, 13, 39–44. [Google Scholar] [CrossRef]
- Chimera, N.J.; Warren, M. Use of Clinical Movement Screening Tests to Predict Injury in Sport. World J. Orthop. 2016, 7, 202–217. [Google Scholar] [CrossRef]
- Camomilla, V.; Bergamini, E.; Fantozzi, S.; Vannozzi, G. Trends Supporting the In-Field Use of Wearable Inertial Sensors for Sport Performance Evaluation: A Systematic Review. Sensors 2018, 18, 873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubans, D.R.; Morgan, P.J.; Cliff, D.P.; Barnett, L.M.; Okely, A.D. Fundamental Movement Skills in Children and Adolescents: Review of Associated Health Benefits. Sports Med. 2010, 40, 1019–1035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myer, G.D.; Kushner, A.M.; Brent, J.L.; Schoenfeld, B.J.; Hugentobler, J.; Lloyd, R.S.; Vermeil, A.; Chu, D.A.; Harbin, J.; McGill, S.M. The Back Squat: A Proposed Assessment of Functional Deficits and Technical Factors That Limit Performance. Strength Cond. J. 2014, 36, 4–27. [Google Scholar] [CrossRef] [Green Version]
- Escamilla, R.F. Knee Biomechanics of the Dynamic Squat Exercise. Med. Sci. Sports Exerc. 2001, 33, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Harrison, J.J.; Yorgey, M.K.; Csiernik, A.J.; Vogler, J.H.; Games, K.E. Clinician-Friendly Physical Performance Tests for the Knee. J. Athl. Train. 2017, 52, 1068–1069. [Google Scholar] [CrossRef]
- Petushek, E.; Nilstad, A.; Bahr, R.; Krosshaug, T. Drop Jump? Single-Leg Squat? Not If You Aim to Predict Anterior Cruciate Ligament Injury From Real-Time Clinical Assessment: A Prospective Cohort Study Involving 880 Elite Female Athletes. J. Orthop. Sports Phys. 2021, 51, 372–378. [Google Scholar] [CrossRef]
- Wilken, J.M.; Rodriguez, K.M.; Brawner, M.; Darter, B.J. Reliability and Minimal Detectible Change Values for Gait Kinematics and Kinetics in Healthy Adults. Gait Posture 2012, 35, 301–307. [Google Scholar] [CrossRef]
- Ferrari, A.; Cutti, A.G.; Cappello, A. A New Formulation of the Coefficient of Multiple Correlation to Assess the Similarity of Waveforms Measured Synchronously by Different Motion Analysis Protocols. Gait Posture 2010, 31, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.H.; Trost, J.P.; Wervey, R.A. Measurement and Management of Errors in Quantitative Gait Data. Gait Posture 2004, 20, 196–203. [Google Scholar] [CrossRef] [Green Version]
- Walter, S.D.; Eliasziw, M.; Donner, A. Sample Size and Optimal Designs for Reliability Studies. Stat. Med. 1998, 17, 101–110. [Google Scholar] [CrossRef]
- Spork, P.; O’Brien, J.; Sepoetro, M.; Plachel, M.; Stöggl, T. The Intra- and Inter-Rater Reliability of a Hip Rotation Range-of-Motion Measurement Using a Smartphone Application in Academy Football (Soccer) Players. Sports 2021, 9, 148. [Google Scholar] [CrossRef]
- van Melick, N.; van Cingel, R.E.H.; Brooijmans, F.; Neeter, C.; van Tienen, T.; Hullegie, W.; Nijhuis-van der Sanden, M.W.G. Evidence-Based Clinical Practice Update: Practice Guidelines for Anterior Cruciate Ligament Rehabilitation Based on a Systematic Review and Multidisciplinary Consensus. Br. J. Sports Med. 2016, 50, 1506–1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, M.J.; Morris, N.; Lane, M.; Barnert, J.; MacGregor, K.; Heard, M.; Robinson, S.; Herzog, W. Monitoring the Return to Sport Transition After ACL Injury: An Alpine Ski Racing Case Study. Front. Sports Act. Living 2020, 2, 12. [Google Scholar] [CrossRef] [PubMed]
- BTS Bioengineering Website. Available online: https://Www.Btsbioengineering.Com/Products/Smart-Dx-Motion-Capture/?Gclid=CjwKCAiAh_GNBhAHEiwAjOh3ZPGV0TeB3pR1v4NOmZ_sXFVyoWQ4oQYKzHa-CHrqffFSj4DaiPyAFRoCHIIQAvD_BwE (accessed on 17 September 2021).
- BTS Bioengineering srl. SMART-E Motion Capture System User Manual—Version 1.7.1; BTS Bioengineering srl: Quincy, MA, USA, 2021. [Google Scholar]
- Bertec Corporation Force Plate User Manual. 2012. Available online: https://www.bertec.com/downloads. (accessed on 17 September 2021).
- Novel Website. Available online: https://Www.Novel.de/Products/Pedar/ (accessed on 17 September 2021).
- Novel Pedar-x System—Manual, v.20. Available online: https://docplayer.net/102726141-Welcome-to-novel-pedar-x-system.html (accessed on 13 December 2021).
- Leardini, A.; Sawacha, Z.; Paolini, G.; Ingrosso, S.; Nativo, R.; Benedetti, M.G. A New Anatomically Based Protocol for Gait Analysis in Children. Gait Posture 2007, 26, 560–571. [Google Scholar] [CrossRef]
- Sawacha, Z.; Guarneri, G.; Cristoferi, G.; Guiotto, A.; Avogaro, A.; Cobelli, C. Diabetic Gait and Posture Abnormalities: A Biomechanical Investigation through Three Dimensional Gait Analysis. Clin. Biomech. 2009, 24, 722–728. [Google Scholar] [CrossRef]
- Benedetti, M.G.; Merlo, A.; Leardini, A. Inter-Laboratory Consistency of Gait Analysis Measurements. Gait Posture 2013, 38, 934–939. [Google Scholar] [CrossRef]
- Manca, M.; Leardini, A.; Cavazza, S.; Ferraresi, G.; Marchi, P.; Zanaga, E.; Benedetti, M.G. Repeatability of a New Protocol for Gait Analysis in Adult Subjects. Gait Posture 2010, 32, 282–284. [Google Scholar] [CrossRef]
- Button, K.; Roos, P.E.; van Deursen, R.W.M. Activity Progression for Anterior Cruciate Ligament Injured Individuals. Clin. Biomech. 2014, 29, 206–212. [Google Scholar] [CrossRef] [Green Version]
- Sawacha, Z.; Spolaor, F.; Piątkowska, W.J.; Cibin, F.; Ciniglio, A.; Guiotto, A.; Ricca, M.; Polli, R.; Murgia, A. Feasibility and Reliability Assessment of Video-Based Motion Analysis and Surface Electromyography in Children with Fragile X during Gait. Sensors 2021, 21, 4746. [Google Scholar] [CrossRef] [PubMed]
- Derrick, T.R.; van den Bogert, A.J.; Cereatti, A.; Dumas, R.; Fantozzi, S.; Leardini, A. ISB Recommendations on the Reporting of Intersegmental Forces and Moments during Human Motion Analysis. J. Biomech. 2020, 99, 109533. [Google Scholar] [CrossRef]
- Winter, D.A. Biomechanics and Motor Control. of Human Movement; John Wiley & Sons: Hoboken, NJ, USA, 2009; ISBN 978-0-470-39818-0. [Google Scholar]
- Prieto, T.E.; Myklebust, J.B.; Hoffmann, R.G.; Lovett, E.G.; Myklebust, B.M. Measures of Postural Steadiness: Differences between Healthy Young and Elderly Adults. IEEE Trans. Biomed. Eng 1996, 43, 956–966. [Google Scholar] [CrossRef] [PubMed]
- Cappozzo, A.; Catani, F.; Della Croce, U.; Leardini, A. Position and Orientation in Space of Bones during Movement: Anatomical Frame Definition and Determination. Clin. Biomech. 1995, 10, 171–178. [Google Scholar] [CrossRef]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB Recommendation on Definitions of Joint Coordinate System of Various Joints for the Reporting of Human Joint Motion—Part I: Ankle, Hip, and Spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Grood, E.; Suntay, W.J. A Joint Coordinate System for the Clinical Description of Three-Dimensional Motions: Application to the Knee. J. Biomech. Eng. 1983, 105, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Harrington, M.E.; Zavatsky, A.B.; Lawson, S.E.M.; Yuan, Z.; Theologis, T.N. Prediction of the Hip Joint Centre in Adults, Children, and Patients with Cerebral Palsy Based on Magnetic Resonance Imaging. J. Biomech. 2007, 40, 595–602. [Google Scholar] [CrossRef]
- Fantozzi, S.; Garofalo, P.; Cutti, A.; Stagni, R. 3D Joint Moments in Transfemoral and Transtibial Amputees: When Is the ground Reaction Vector Technique” an Alternative to Inverse Dynamics? J. Mech. Med. Biol. 2012, 12, 1250061. [Google Scholar] [CrossRef]
- Camomilla, V.; Cereatti, A.; Cutti, A.G.; Fantozzi, S.; Stagni, R.; Vannozzi, G. Methodological Factors Affecting Joint Moments Estimation in Clinical Gait Analysis: A Systematic Review. Biomed. Eng. Online 2017, 16, 106. [Google Scholar] [CrossRef] [Green Version]
- Krabbe, B.; Farkas, R.; Baumann, W. Influence of Inertia on Intersegment Moments of the Lower Extremity Joints. J. Biomech. 1997, 30, 517–519. [Google Scholar] [CrossRef]
- Benedetti, M.; Catani, F.; Leardini, A.; Pignotti, E.; Giannini, S. Data Management in Gait Analysis for Clinical Applications. Clin. Biomech. 1998, 13, 204–215. [Google Scholar] [CrossRef]
- Zatsiorsky, V.M. Kinetics of Human Motion; Human Kinetics: Champaign, IL, USA, 2002; ISBN 978-0-7360-3778-5. [Google Scholar]
- Sawacha, Z.; Guarneri, G.; Cristoferi, G.; Guiotto, A.; Avogaro, A.; Cobelli, C. Integrated Kinematics–Kinetics–Plantar Pressure Data Analysis: A Useful Tool for Characterizing Diabetic Foot Biomechanics. Gait Posture 2012, 36, 20–26. [Google Scholar] [CrossRef]
- Kalpen, A.; Seitz, P. Comparison between the Force Values Measured with the Pedar System and Kistler Platform. Gait Posture 1994, 2, 236–237. [Google Scholar] [CrossRef]
- McPoil, T.G.; Cornwall, M.W.; Yamada, W. A Comparison of Two In-Shoe Plantar Pressupe Measurement Systems. Low. Extrem. 1995, 2, 95–103. [Google Scholar]
- Hurkmans, H.L.P.; Bussmann, J.B.J.; Benda, E.; Verhaar, J.A.N.; Stam, H.J. Accuracy and Repeatability of the Pedar Mobile System in Long-Term Vertical Force Measurements. Gait Posture 2006, 23, 118–125. [Google Scholar] [CrossRef]
- Gurney, J.K.; Kersting, U.G.; Rosenbaum, D. Between-Day Reliability of Repeated Plantar Pressure Distribution Measurements in a Normal Population. Gait Posture 2008, 27, 706–709. [Google Scholar] [CrossRef]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Cerin, E.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Objectively Measured Light-Intensity Physical Activity Is Independently Associated With 2-h Plasma Glucose. Dia. Care 2007, 30, 1384–1389. [Google Scholar] [CrossRef] [Green Version]
- Stöggl, T.; Martiner, A. Validation of Moticon’s OpenGo Sensor Insoles during Gait, Jumps, Balance and Cross-Country Skiing Specific Imitation Movements. J. Sports Sci. 2017, 35, 196–206. [Google Scholar] [CrossRef] [Green Version]
- Putti, A.B.; Arnold, G.P.; Cochrane, L.; Abboud, R.J. The Pedar In-Shoe System: Repeatability and Normal Pressure Values. Gait Posture 2007, 25, 401–405. [Google Scholar] [CrossRef]
- Ramanathan, A.K.; Kiran, P.; Arnold, G.P.; Wang, W.; Abboud, R.J. Repeatability of the Pedar-X in-Shoe Pressure Measuring System. Foot Ankle Surg. 2010, 16, 70–73. [Google Scholar] [CrossRef]
- Trulsson, A.; Miller, M.; Hansson, G.-Å.; Gummesson, C.; Garwicz, M. Altered Movement Patterns and Muscular Activity during Single and Double Leg Squats in Individuals with Anterior Cruciate Ligament Injury. BMC Musculoskelet. Disord. 2015, 16, 28. [Google Scholar] [CrossRef] [Green Version]
- Monajati, A.; Larumbe-Zabala, E.; Goss-Sampson, M.; Naclerio, F. Surface Electromyography Analysis of Three Squat Exercises. J. Hum. Kinet. 2019, 67, 73–83. [Google Scholar] [CrossRef] [Green Version]
- Roos, P.E.; Button, K.; van Deursen, R.W.M. Motor Control Strategies during Double Leg Squat Following Anterior Cruciate Ligament Rupture and Reconstruction: An Observational Study. J. Neuroeng. Rehabil. 2014, 11, 19. [Google Scholar] [CrossRef]
- Giacomozzi, C. Hardware Performance Assessment Recommendations and Tools for Baropodometric Sensor Systems. Annali dell’Istituto Super. Sanita 2010, 46, 158–167. [Google Scholar] [CrossRef]
- Price, C.; Parker, D.; Nester, C. Validity and Repeatability of Three In-Shoe Pressure Measurement Systems. Gait Posture 2016, 46, 69–74. [Google Scholar] [CrossRef] [Green Version]
- Saggin, B.; Scaccabarozzi, D.; Tarabini, M. Metrological Performances of a Plantar Pressure Measurement System. IEEE Trans. Instrum. Meas. 2013, 62, 766–776. [Google Scholar] [CrossRef]
- Donohue, M.R.; Ellis, S.M.; Heinbaugh, E.M.; Stephenson, M.L.; Zhu, Q.; Dai, B. Differences and Correlations in Knee and Hip Mechanics during Single-Leg Landing, Single-Leg Squat, Double-Leg Landing, and Double-Leg Squat Tasks. Res. Sports Med. 2015, 23, 394–411. [Google Scholar] [CrossRef]
- Cerfoglio, S.; Galli, M.; Tarabini, M.; Bertozzi, F.; Sforza, C.; Zago, M. Machine Learning-Based Estimation of Ground Reaction Forces and Knee Joint Kinetics from Inertial Sensors While Performing a Vertical Drop Jump. Sensors 2021, 21, 7709. [Google Scholar] [CrossRef]









| Dataset | Age (Years) Mean (SD) | Weight (kg) Mean (SD) | Height (m) Mean (SD) | BMI (kg/m2) Mean (SD) | Shoe Size Mean (SD) |
|---|---|---|---|---|---|
| HS | 26.6 (3.66) | 66.7 (10.84) | 1.73 (0.07) | 22.04 (2.28) | 40.4 (2.27) |
| STF Mean (SD) (mm) or (Degrees) | TOF Mean (SD) (mm) or (Degrees) | RMSE% of STF (Min < Mean < Max) | r (Pearson/Spearman) (Min < Mean < Max) | |
|---|---|---|---|---|
| RHJC-ML | −8.04 (13.10) | −8.67 (14.75) | (2.63 < 18.29 < 25.41) | (−0.46 < 0.54 < 1) |
| RHJC-V | −190.27 (55.58) | −184.28 (56.70) | (0.92 < 7.16 < 12.31) | (0.84 < 0.97 < 1) |
| RHJC-AP | −88.38 (40.88) | −85.12 (36.37) | (1.01 < 11.65 < 16.52) | (0.27 < 0.93 < 1) |
| LHJC-ML | −8.28 (13.52) | −9.03 (14.74) | (2.58 < 17.19 < 23.64) | (−0.48 < 0.55 < 1) |
| LHJC-V | −188.31 (55.47) | −181.40 (55.85) | (0.84 < 7.33 < 13.25) | (0.83 < 0.97 < 1) |
| LHJC-AP | −88.44 (37.26) | −84.10 (35.16) | (1.20 < 13.65 < 18.25) | (0.3 < 0.93 < 1) |
| RKJC-ML | −25.06 (12.20) | −24.38 (20.75) | (1.34 < 16.46 < 21.59) | (0.67 < 0.9 < 1) |
| RKJC-V | −44.93 (24.71) | −40.90 (12.92) | (0.74 < 5.92 < 8.74) | (0.84 < 0.97 < 1) |
| RKJC-AP | 105.48 (27.03) | 96.80 (33.29) | (1.19 < 10.52 < 18.80) | (0.82 < 0.95 < 1) |
| LKJC-ML | 34.56 (10.68) | 31.78 (23.61) | (1.73 < 12.93 < 17.41) | (0.65 < 0.95 < 1) |
| LKJC-V | −43.30 (24.59) | −39.31 (12.17) | (0.90 < 6.66 < 9.96) | (0.87 < 0.97 < 1) |
| LKJC-AP | 105.00 (28.70) | 94.55 (30.49) | (1.26 < 10.45 < 18.16) | (0.82 < 0.96 < 1) |
| RAJC-ML | 2.61 (1.42) | 2.70 (2.78) | (1.13 < 12.38 < 16.04) | (0.28 < 0.85 < 0.99) |
| RAJC-V | −1.81 (0.87) | −1.93 (1.20) | (2.39 < 25.66 < 35.75) | (−0.1 < 0.68 < 0.98) |
| RAJC-AP | 7.58 (2.64) | 6.80 (2.83) | (1.35 < 13.67 < 18.52) | (0.54 < 0.9 < 0.99) |
| LAJC-ML | −0.79 (0.88) | −0.58 (2.63) | (1.78 < 12.52 < 15.73) | (0.26 < 0.68 < 0.99) |
| LAJC-V | −0.95 (0.52) | −1.23 (1.25) | (6.16 < 48.60 < 61.84) | (0.13 < 0.64 < 0.96) |
| LAJC-AP | 7.78 (2.98) | 7.02 (3.29) | (2.05 < 17.33 < 23.55) | (0.71 < 0.91 < 0.99) |
| Hip—Flexion-Extension | 65.99 (20.02) | 73.34 (21.19) | (8.89 < 11.20 < 13.79) | (0.77 < 0.96 < 1) |
| Knee—Flexion-Extension | 70.85 (25.67) | 69.88 (26.72) | (4.13 < 6.83 < 9.98) | (0.86 < 0.97 < 1) |
| Ankle—Flexion-Extension | 25.91 (8.47) | 24.35 (8.97) | (6.48 < 9.54 < 15.59) | (0.87 < 0.97 < 1) |
| Bertec Mean (SD) | Novel Mean (SD) | RMSE% of Bertec (Min < Mean < Max) | r (Pearson/Spearman) (Min < Mean < Max) | % of Tests with p < 0.05 | |
|---|---|---|---|---|---|
| GRF (%BW)—Vertical Component | 53.05 (4.33) | 35.02 (6.9) | (27.71 < 30.61 < 32.6) | (0.11 < 0.37 < 0.86) | 86% |
| Bertec Mean (SD) | Novel Mean (SD) | RMSE% of Bertec | r (Pearson/Spearman) | p (p < 0.05) | |
|---|---|---|---|---|---|
| COP Range ML (mm) | 14.65 (6.22) | 6.26 (4.07) | 33.14 | 0.6 | p < 0.001 |
| COP Range AP (mm) | 55.85 (19.16) | 46.5 (23.87) | 24.6 | 0.47 | p < 0.001 |
| COP SD ML (mm) | 5.3 (1.71) | 3.14 (1.15) | 31.53 | 0.96 | p < 0.001 |
| COP SD AP (mm) | 26.05 (8.14) | 24.29 (6.95) | 9.07 | 0.94 | p < 0.001 |
| COP path length ML (mm) | 30.44 (9.15) | 12.94 (7.37) | 35.84 | 0.49 | p < 0.001 |
| COP path length AP (mm) | 143.16 (35.67) | 101.85 (53.21) | 29.42 | 0.3 | p < 0.05 |
| Joint Moments (% BWx H) | Hip Flex/Extension | Hip Add-Abduction | Knee Flex-Extension | Knee Varus-Valgus | Ankle Dorsi-Plantarflexion | Ankle Inv-Eversion | |
|---|---|---|---|---|---|---|---|
| ACL Quick Check® integrated | Mean (SD) | 5.81 (2.32) | 0.44 (1.87) | 3.08 (1.15) | 1.17 (−1.04) | −0.05 (0.62) | −0.28 (0.47) |
| Inverse Dynamic approach | Mean (SD) | 3.15 (1.39) | −0.81 (0.88) | 3.88 (0.61) | 0.32 (0.77) | 0.89 (0.68) | 0.04 (0.56) |
| Ground Reaction Vector 1D | Mean (SD) | 4.73 (1.37) | −1.91 (1.3) | 3.85 (0.74) | 1.12 (1.11) | 0.97 (0.73) | 0.38 (0.57) |
| Ground Reaction Vector 3D | Mean (SD) | 4.02 (1.69) | −0.25 (1.02) | 4.25 (0.68) | 0.22 (0.85) | 0.91 (0.69) | 0.05 (0.58) |
| ACL Quick Check® integrated STF | Mean (SD) | 5.4 (2.17) | −0.77 (1.35) | 3.31 (1.11) | 0.9 (0.94) | 0.22 (0.45) | −0.44 (0.33) |
| ACL Quick Check® | Mean (SD) | 5.61 (2.33) | −0.82 (1.53) | 3.02 (1.18) | 0.91 (0.87) | 0.19 (0.44) | −0.39 (0.33) |
| Comparison e—Inverse Dynamic approach vs. ACL Quick Check® integrated | RMSE% (min < mean < max) | (29.68 < 51.27 < 58.42) | (24.59 < 34.42 < 59.45) | (8.25 < 22.24 < 24.99) | (17.4 < 42.07 < 53.67) | (10.3 < 40.32 < 50.65) | (9.24 < 17.88 < 19.81) |
| r (Pearson/Spearman) (min < mean < max) | (0.49 < 0.81 < 0.97) | (−0.83 < 0.44 < 0.96) | (0.65 < 0.9 < 0.99) | (−0.5 < 0.27 < 0.88) | (−0.9 < −0.1 < 0.93) | (−0.76 < 0.34 < 0.93) | |
| % of tests with p < 0.05 | 98% | 93% | 100% | 83% | 87% | 83% | |
| Comparison f—Ground Reaction Vector 3D vs. ACL Quick Check® integrated | RMSE% (min < mean < max) | (20.91 < 35.32 < 40.23) | (30.56 < 36.29 < 55.38) | (13.21 < 24.05 < 26.76) | (25.78 < 41.75 < 52.38) | (39.93 < 47.73 < 64.51) | (16.82 < 18.41 < 19.81) |
| r (Pearson/Spearman) (min < mean < max) | (0.31 < 0.81 < 0.98) | (−0.8 < 0.33 < 0.94) | (0.68 < 0.91 < 0.99) | (−0.47 < 0.26 < 0.88) | (−0.91 < −0.11 < 0.85) | (−0.79 < 0.34 < 0.92) | |
| % of tests with p < 0.05 | 100% | 87% | 100% | 73% | 83% | 87% | |
| Comparison g—Ground Reaction Vector 1D vs. ACL Quick Check® integrated | RMSE% (min < mean < max) | (15.64 < 30.33 < 35.57) | (39.62 < 44.43 < 58.36) | (13.25 < 21.26 < 25.5) | (32.75 < 35.62 < 45.92) | (40.05 < 47.55 < 64.11) | (22.99 < 25.89 < 26.73) |
| r (Pearson/Spearman) (min < mean < max) | (0.46 < 0.83 < 0.98) | (−0.9 < 0.39 < 0.96) | (0.63 < 0.92 < 0.99) | (−0.8 < 0.26 < 0.95) | (−0.92 < −0.11 < 0.87) | (−0.68 < 0.23 < 0.86) | |
| % of tests with p < 0.05 | 100% | 83% | 100% | 75% | 83% | 83% | |
| Comparison h—ACL Quick Check® integrated vs. ACL Quick Check® integrated STF | RMSE% (min < mean < max) | (4.73 < 6.88 < 8.21) | (6.18 < 10.06 < 14.39) | (7.02 < 11.9 < 14.77) | (7.1 < 8.87 < 10.53) | (11.14 < 26.02 < 36.17) | (9.78 < 23.03 < 27.3) |
| r (Pearson/Spearman) (min < mean < max) | (0.35 < 0.88 < 1) | (−0.97 < 0.44 < 0.98) | (0.63 < 0.94 < 1) | (−0.36 < 0.73 < 0.99) | (−1 < 0.4 < 1) | (−0.98 < 0.59 < 1) | |
| % of tests with p < 0.05 | 100% | 92% | 100% | 97% | 89% | 89% | |
| Comparison i—ACL Quick Check® vs. ACL Quick Check® integrated | RMSE% (min < mean < max) | (1.54 < 3.99 < 5.23) | (24.31 < 54 < 61.6) | (2.98 < 7.12 < 8.37) | (3.21 < 9.74 < 13.51) | (30.18 < 50.24 < 62.67) | (21.95 < 27.91 < 33.77) |
| r (Pearson/Spearman) (min < mean < max) | (0.92 < 0.99 < 1) | (−0.97 < 0.41 < 0.94) | (0.96 < 1 < 1) | (−0.59 < 0.7 < 0.99) | (−1 < 0.25 < 1) | (−0.8 < 0.55 < 1) | |
| % of tests with p < 0.05 | 100% | 94% | 100% | 92% | 100% | 91% |
| Op 1 Mean (SD) (mm) | Op 2 Mean (SD) (mm) | Op 3 Mean (SD) (mm) | RMSE% (Min < Mean < Max) | CMC | |
|---|---|---|---|---|---|
| HJC-ML-r | 20.5 (0.65) | 20.35 (0.86) | 19.89 (0.67) | (0.79 < 2.68 < 5.21) | 0.9703 |
| HJC-V-r | 78.75 (2.83) | 74.89 (2.28) | 76.69 (2.17) | (0.69 < 3.8 < 7.85) | 0.9683 |
| HJC-AP-r | −4.47 (1.32) | −4.13 (1.09) | −4.83 (1.1) | (1.96 < 6.54 < 12.4) | 0.9687 |
| Knee center-ML-r | 30.61 (0.44) | 30.57 (0.39) | 30.43 (0.43) | (0.36 < 0.87 < 5.39) | 0.9687 |
| Knee center-V-r | 44.43 (0.96) | 44.71 (1.06) | 44.02 (0.86) | (0.74 < 1.35 < 3.13) | 0.9688 |
| Knee center-AP-r | 39.13 (1.47) | 40.57 (1.2) | 39.88 (1.2) | (0.97 < 2.67 < 9.52) | 0.9694 |
| Ankle center-ML-r | 25.82 (0.13) | 25.98 (0.2) | 25.48 (0.41) | (0.91 < 1.41 < 3.15) | 0.9694 |
| Ankle center-V-r | 10.41 (0.08) | 10.62 (0.09) | 10.47 (0.14) | (0.85 < 1.52 < 3.07) | 0.9694 |
| Ankle center-AP-r | 19.6 (0.14) | 19.69 (0.28) | 19.8 (0.35) | (0.99 < 1.65 < 4.18) | 0.9694 |
| HJC-ML-l | −52.49 (0.66) | −52.74 (0.9) | −52.18 (0.7) | (0.56 < 1.19 < 3.68) | 0.9694 |
| HJC-V-l | 80.45 (2.66) | 77.02 (2.27) | 78.59 (2.08) | (0.47 < 3.46 < 7.12) | 0.9706 |
| HJC-AP-l | −8.25 (1.37) | −7.66 (1.53) | −8.66 (1.27) | (2.25 < 6.45 < 11.06) | 0.9708 |
| Knee center-ML-l | −51.55 (0.25) | −51.36 (0.36) | −51.35 (0.34) | (0.17 < 0.55 < 2.04) | 0.9708 |
| Knee center-V-l | 45.27 (0.79) | 45.4 (0.94) | 44.78 (0.78) | (0.65 < 1.18 < 3.29) | 0.9709 |
| Knee center-AP-l | 37.01 (1.6) | 38.54 (1.17) | 37.93 (1.24) | (1.09 < 3.36 < 10.29) | 0.9708 |
| Ankle center-ML-l | −53.96 (0.09) | −53.93 (0.22) | −53.5 (0.32) | (0.4 < 0.77 < 2.48) | 0.9708 |
| Ankle center-V-l | 10.49 (0.17) | 10.52 (0.09) | 10.44 (0.1) | (0.79 < 1.29 < 2.69) | 0.9708 |
| Ankle center-AP-l | 19.3 (0.23) | 19.08 (0.18) | 19.89 (0.59) | (2.25 < 3.18 < 6.28) | 0.9708 |
| Hip-FE-r | 67.29 (4.06) | 61.86 (2.99) | 68.85 (2.36) | (3.07 < 7.37 < 11.28) | 0.9622 |
| Knee-FE-r | 75 (5.09) | 80.06 (3.97) | 78.05 (3.58) | (2.38 < 4.09 < 7.43) | 0.9834 |
| Ankle-FE-r | 28.58 (2.72) | 30.8 (2.13) | 32.29 (4.06) | (4.47 < 7.63 < 14.94) | 0.9781 |
| Hip-FE-l | 67.28 (4.19) | 61.28 (3) | 67.49 (2.31) | (3.07 < 6.92 < 11.34) | 0.976 |
| Knee-FE-l | 69.87 (4.88) | 74.96 (3.4) | 73.09 (3.13) | (1.36 < 4.93 < 12.77) | 0.9786 |
| Ankle-FE-l | 25.36 (2.74) | 28.03 (1.6) | 30.39 (1.95) | (4.56 < 9.59 < 26.74) | 0.9784 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guiotto, A.; Ciniglio, A.; Spolaor, F.; Pavan, D.; Cibin, F.; Scaldaferro, A.; Sawacha, Z. Reliability and Repeatability of ACL Quick Check®: A Methodology for on Field Lower Limb Joint Kinematics and Kinetics Assessment in Sport Applications. Sensors 2022, 22, 259. https://doi.org/10.3390/s22010259
Guiotto A, Ciniglio A, Spolaor F, Pavan D, Cibin F, Scaldaferro A, Sawacha Z. Reliability and Repeatability of ACL Quick Check®: A Methodology for on Field Lower Limb Joint Kinematics and Kinetics Assessment in Sport Applications. Sensors. 2022; 22(1):259. https://doi.org/10.3390/s22010259
Chicago/Turabian StyleGuiotto, Annamaria, Alfredo Ciniglio, Fabiola Spolaor, Davide Pavan, Federica Cibin, Alex Scaldaferro, and Zimi Sawacha. 2022. "Reliability and Repeatability of ACL Quick Check®: A Methodology for on Field Lower Limb Joint Kinematics and Kinetics Assessment in Sport Applications" Sensors 22, no. 1: 259. https://doi.org/10.3390/s22010259