A Power Spectral Density-Based Method to Detect Tremor and Tremor Intermittency in Movement Disorders

 , , , and
, , , and
Abstract
:1. Introduction
- Pathological tremors need to be detectable during various tasks.
2. Materials and Methods
2.1. Subjects and Clinical Evaluation
2.2. Experimental Protocol and Data Acquisition
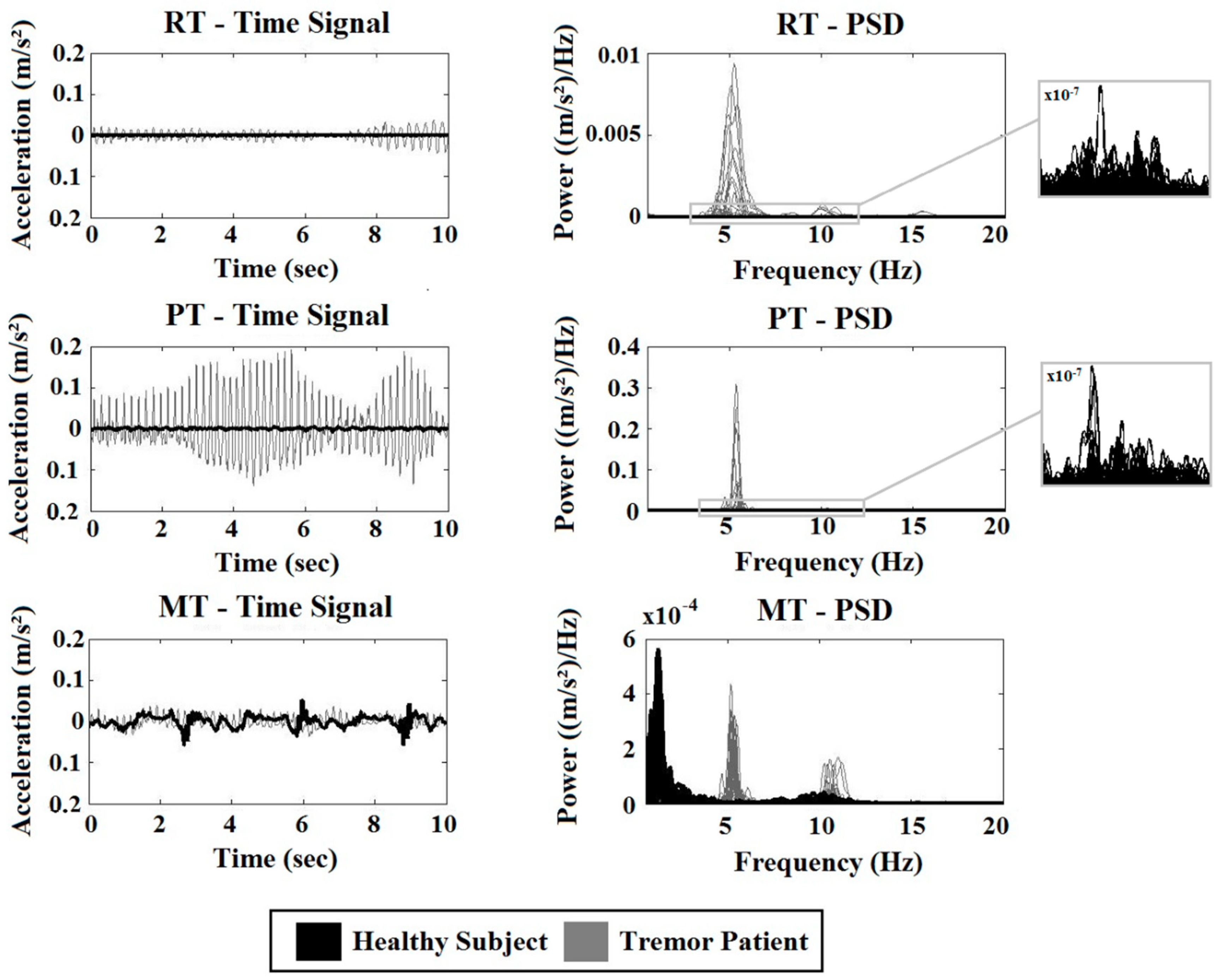
- Resting task (RT): Subjects sit with both hands in supine position resting in their lap; task duration: one min.
- Postural task (PT): Subjects stretch out both arms, unsupported against gravity, approximately parallel to the floor; task duration: one min.
- Movement task (MT): Subjects perform an elbow flexion-extension task (index finger from nose to knee) with the right arm at a self-paced speed, and the left arm remains rested in the lap; task duration: one min.
2.3. Data Analysis
- Accelerometer recordings of ET patients 1–5, PD patients 1–5, and HC subjects 1–5 were used to evaluate the methods (Training set) and parameter settings.
- Accelerometer recordings of ET 6–10, PD 6–10, and HC 6–10 are used to validate the selected method (Validation Group 1).
- EMG recordings of all subjects were used to validate the selected method (Validation Group 2).
2.4. Tremor Classification
2.5. Outcome Parameters
2.6. Statistical Analysis
3. Results
3.1. Sensitivity, Specificity, and Accuracy
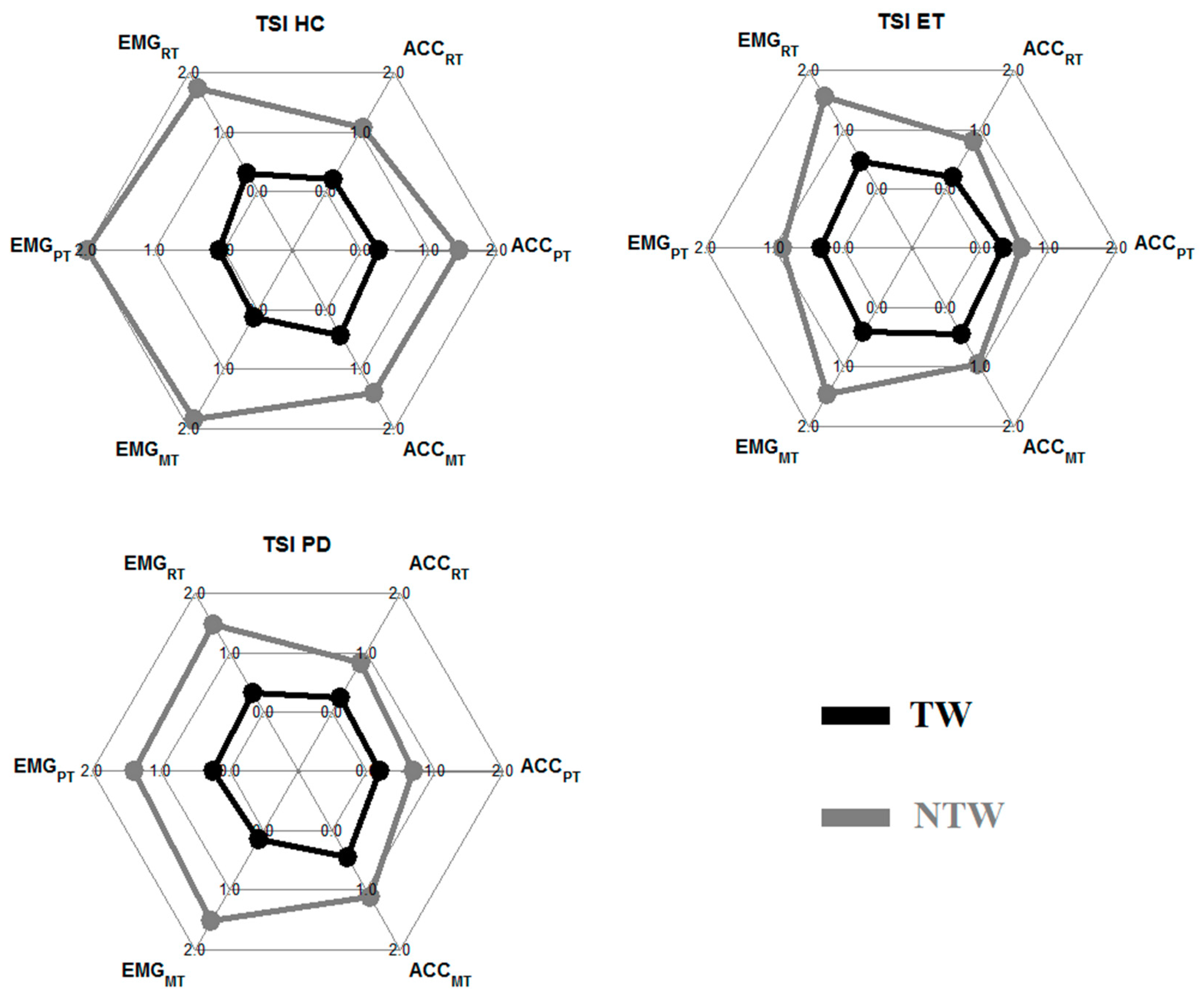
3.2. The Tremor Stability Index
4. Discussion
4.1. Tremor Classification Method
4.2. Tremor Measures
5. Conclusion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bain, P.G. Parkinsonism & related disorders. Tremor. Parkinsonism Relat. Disord. 2007, 13, 369–374. [Google Scholar]
- Hess, C.W.; Pullman, S.L. Tremor: Clinical phenomenology and assessment techniques. Tremor Other Hyperkinet. Mov. 2012, 2. [Google Scholar] [CrossRef]
- Post, B.; Merkus, M.P.; de Bie, R.M.; de Haan, R.J.; Speelman, J.D. Unified Parkinson’s disease rating scale motor examination: Are ratings of nurses, residents in neurology, and movement disorders specialists interchangeable? Mov. Disord. 2005, 20, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, G.; Copetti, M.; Arcuti, S.; Martino, D.; Fontana, A.; Logroscino, G. Accuracy of clinical diagnosis of Parkinson disease: A systematic review and meta-analysis. Neurology 2016, 86, 566–576. [Google Scholar] [CrossRef]
- Jain, S.; Lo, S.E.; Louis, E.D. Common misdiagnosis of a common neurological disorder: How are we misdiagnosing essential tremor? Arch. Neurol. 2006, 63, 1100–1104. [Google Scholar] [CrossRef]
- Barth, J.; Sünkel, M.; Bergner, K.; Schickhuber, G.; Winkler, J.; Klucken, J.; Eskofier, B. Combined analysis of sensor data from hand and gait motor function improves automatic recognition of Parkinson’s disease. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012. [Google Scholar]
- Mostile, G.; Fekete, R.; Giuffrida, J.P.; Yaltho, T.; Davidson, A.; Nicoletti, A.; Zappia, M.; Jankovic, J. Amplitude fluctuations in essential tremor. Parkinsonism Relat. Disord. 2012, 18, 859–863. [Google Scholar] [CrossRef] [PubMed]
- O’Suilleabhain, P.E.; Matsumoto, J.Y. Time-frequency analysis of tremors. Brain 1998, 121, 2127–2134. [Google Scholar] [CrossRef] [PubMed]
- Spieker, S.; Boose, A.; Breit, S.; Dichgans, J. Long-term measurement of tremor. Mov. Disord. 1998, 13, 81–84. [Google Scholar] [CrossRef]
- Breit, S.; Spieker, S.; Schulz, J.B.; Gasser, T. Long-term EMG recordings differentiate between parkinsonian and essential tremor. J. Neurol. 2008, 255, 103–111. [Google Scholar] [CrossRef]
- Mansur, P.H.G.; Cury, L.K.P.; Andrade, A.O.; Pereira, A.A.; Miotto, G.A.A.; Soares, A.B.; Naves, E.L. A review on techniques for tremor recording and quantification. Crit. Rev. Biomed. Eng. 2007, 35, 343–362. [Google Scholar] [CrossRef]
- Zach, H.; Dirkx, M.; Bloem, B.R.; Helmich, R.C. The Clinical Evaluation of Parkinson’s Tremor. J. Parkinsons Dis. 2015, 5, 471–474. [Google Scholar] [CrossRef] [PubMed]
- Ghassemi, N.H.; Marxreiter, F.; Pasluosta, C.F.; Kugler, P.; Schlachetzki, J.; Schramm, A.; Eskofier, B.M.; Klucken, J. Combined accelerometer and EMG analysis to differentiate essential tremor from Parkinson’s disease. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 672–675. [Google Scholar]
- di Biase, L.; Brittain, J.S.; Shah, S.A.; Pedrosa, D.J.; Cagnan, H.; Mathy, A.; Chen, C.C.; Martín-Rodríguez, J.F.; Mir, P.; Timmerman, L.; et al. Tremor stability index: A new tool for differential diagnosis in tremor syndromes. Brain 2017, 140, 1977–1986. [Google Scholar] [CrossRef] [PubMed]
- Heida, T.; Wentink, E.C.; Marani, E. Power spectral density analysis of physiological, rest and action tremor in Parkinson’s disease patients treated with deep brain stimulation. J. Neuroeng. Rehabil. 2013, 10, 70. [Google Scholar] [CrossRef]
- Deuschl, G.; Bain, P.; Brin, M. Consensus statement of the Movement Disorder Society on Tremor. Ad Hoc Scientific Committee. Mov. Disord. 1998, 13, 2–23. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, K.P.; Bain, P.; Bajaj, N.; Elble, R.J.; Hallett, M.; Louis, E.D.; Raethjen, J.; Stamelou, M.; Testa, C.M.; Deuschl, G. Consensus Statement on the classification of tremors. From the task force on tremor of the International Parkinson and Movement Disorder Society. Mov. Disord. 2018, 33, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Buijink, A.W.; Contarino, M.F.; Koelman, J.H.; Speelman, J.D.; van Rootselaar, A.F. How to tackle tremor—Systematic review of the literature and diagnostic work-up. Front. Neurol. 2012, 3, 146. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, R.C. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- Gelb, D.J.; Oliver, E.; Gilman, S. Diagnostic criteria for Parkinson disease. Arch. Neurol. 1999, 56, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Chouinard, S.; Louis, E.D.; Fahn, S. Agreement among movement disorder specialists on the clinical diagnosis of essential tremor. Mov. Disord. 1997, 12, 973–976. [Google Scholar] [CrossRef]
- Deuschl, G.; Lauk, M.; Timmer, J. Tremor classification and tremor time series analysis. Chaos 1995, 5, 48–51. [Google Scholar] [CrossRef]
- Cohen, O.; Pullman, S.; Jurewicz, E.; Watner, D.; Louis, E.D. Rest tremor in patients with essential tremor: Prevalence, clinical correlates, and electrophysiologic characteristics. Arch. Neurol. 2003, 60, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.B. Analysis of amplitude and frequency variations of essential and Parkinsonian tremors. Med. Biol. Eng. Comput. 2004, 42, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Salarian, A.; Russmann, H.; Wider, C.; Burkhard, P.R.; Vingerhoets, F.J.; Aminian, K. Quantification of tremor and bradykinesia in Parkinson’s disease using a novel ambulatory monitoring system. IEEE Trans. Biomed. Eng. 2007, 54, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Elble, R.J. Characteristics of physiologic tremor in young and elderly adults. Clin. Neurophysiol. 2003, 114, 624–635. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Subject | Gender | Age | Disease Onset | Medication |
|---|---|---|---|---|
| * PD 1 | M | 58 | 50 | Levodopa, Trihexyphenidyl |
| * PD 2 | M | 69 | 64 | Rasagiline, propranolol |
| * PD 3 | M | 67 | 63 | Trihexyphenidyl |
| * PD 4 | F | 81 | 76 | Levodopa-Carbidopa, metoprolol tartrate |
| * PD 5 | F | 62 | 60 | Levodopa |
| Ϯ PD 6 | M | 49 | 47 | Levodopa-Carbidopa, ropinirole hydrochloride |
| Ϯ PD 7 | M | 71 | 71 | - |
| Ϯ PD 8 | F | 43 | 40 | Trihexyphenidyl, ropinirole hydrochloride |
| Ϯ PD 9 | M | 78 | 76 | Levodopa-Carbidopa, Rasagiline, perindopril, omeprazole, pravastatin |
| Ϯ PD 10 | M | 68 | 60 | Levodopa-Carbidopa |
| * ET 1 | M | 45 | Childhood | - |
| * ET 2 | F | 81 | Childhood | - |
| * ET 3 | M | 85 | Childhood | Propranolol |
| * ET 4 | M | 65 | Teenager | - |
| * ET 5 | F | 51 | Childhood | - |
| Ϯ ET 6 | M | 49 | 40 | Propranolol |
| Ϯ ET 7 | M | 54 | Teenager | - |
| Ϯ ET 8 | M | 70 | Childhood | - |
| Ϯ ET 9 | M | 64 | Teenager | - |
| Ϯ ET 10 | M | 55 | Teenager | - |
| Threshold (Training Set) | ValGroup 1 | ValGroup 2 | ||||
|---|---|---|---|---|---|---|
| 0.35 | 0.40 | 0.45 | 0.50 | 0.40 | 0.40 | |
| Sensitivity (%) | 92.64 | 84.84 | 76.09 | 66.20 | 78.31 | 92.12 |
| Specificity (%) | 87.13 | 96.45 | 99.10 | 99.70 | 95.00 | 95.00 |
| Accuracy (%) | 89.81 | 90.80 | 87.90 | 83.40 | 90.06 | 94.38 |
| TW HC (%) | 7.22 | 1.20 | 0 | 0 | 6.76 | 1.62 |
| Parameter | Task | p-Value TW | p-Value NTW | ||
|---|---|---|---|---|---|
| EMG | ACC | EMG | ACC | ||
| TSI | RT | - | - | - | - |
| PT | < 0.001 Ϯ | - | < 0.001 * | < 0.001 Ϯ | |
| MT | 0.004 * | - | - | 0.02 * | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luft, F.; Sharifi, S.; Mugge, W.; Schouten, A.C.; Bour, L.J.; van Rootselaar, A.-F.; Veltink, P.H.; Heida, T. A Power Spectral Density-Based Method to Detect Tremor and Tremor Intermittency in Movement Disorders. Sensors 2019, 19, 4301. https://doi.org/10.3390/s19194301
Luft F, Sharifi S, Mugge W, Schouten AC, Bour LJ, van Rootselaar A-F, Veltink PH, Heida T. A Power Spectral Density-Based Method to Detect Tremor and Tremor Intermittency in Movement Disorders. Sensors. 2019; 19(19):4301. https://doi.org/10.3390/s19194301
Chicago/Turabian StyleLuft, Frauke, Sarvi Sharifi, Winfred Mugge, Alfred C. Schouten, Lo J. Bour, Anne-Fleur van Rootselaar, Peter H. Veltink, and Tijtske Heida. 2019. "A Power Spectral Density-Based Method to Detect Tremor and Tremor Intermittency in Movement Disorders" Sensors 19, no. 19: 4301. https://doi.org/10.3390/s19194301