USEQ: A Short Questionnaire for Satisfaction Evaluation of Virtual Rehabilitation Systems

 ,
,  ,
,
Abstract
:1. Introduction
1.1. Usability
1.2. Usability in Virtual Rehabilitation
2. USEQ: The User Satisfaction Evaluation Questionnaire
2.1. SEQ: The Suitability Evaluation Questionnaire
2.2. USEQ: Questions
3. Study Design
3.1. Subjects
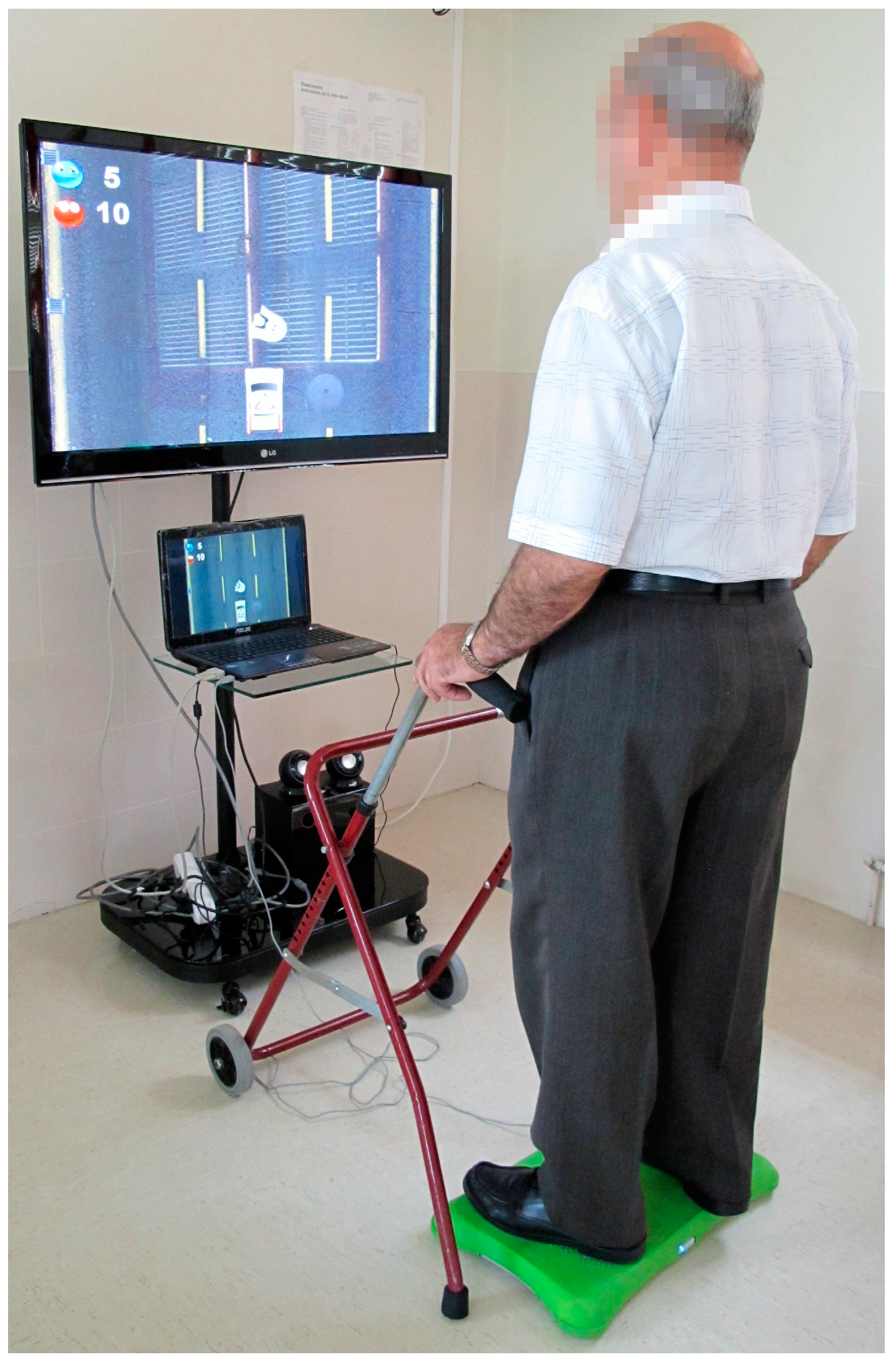
3.2. Study Interventions
3.3. Study Procedures
3.4. Outcome Measures
3.5. Data Analysis
4. Results
4.1. Sample Characteristics
4.2. USEQ Scores
4.3. Item-Total Correlation and Cronbach’s Alpha
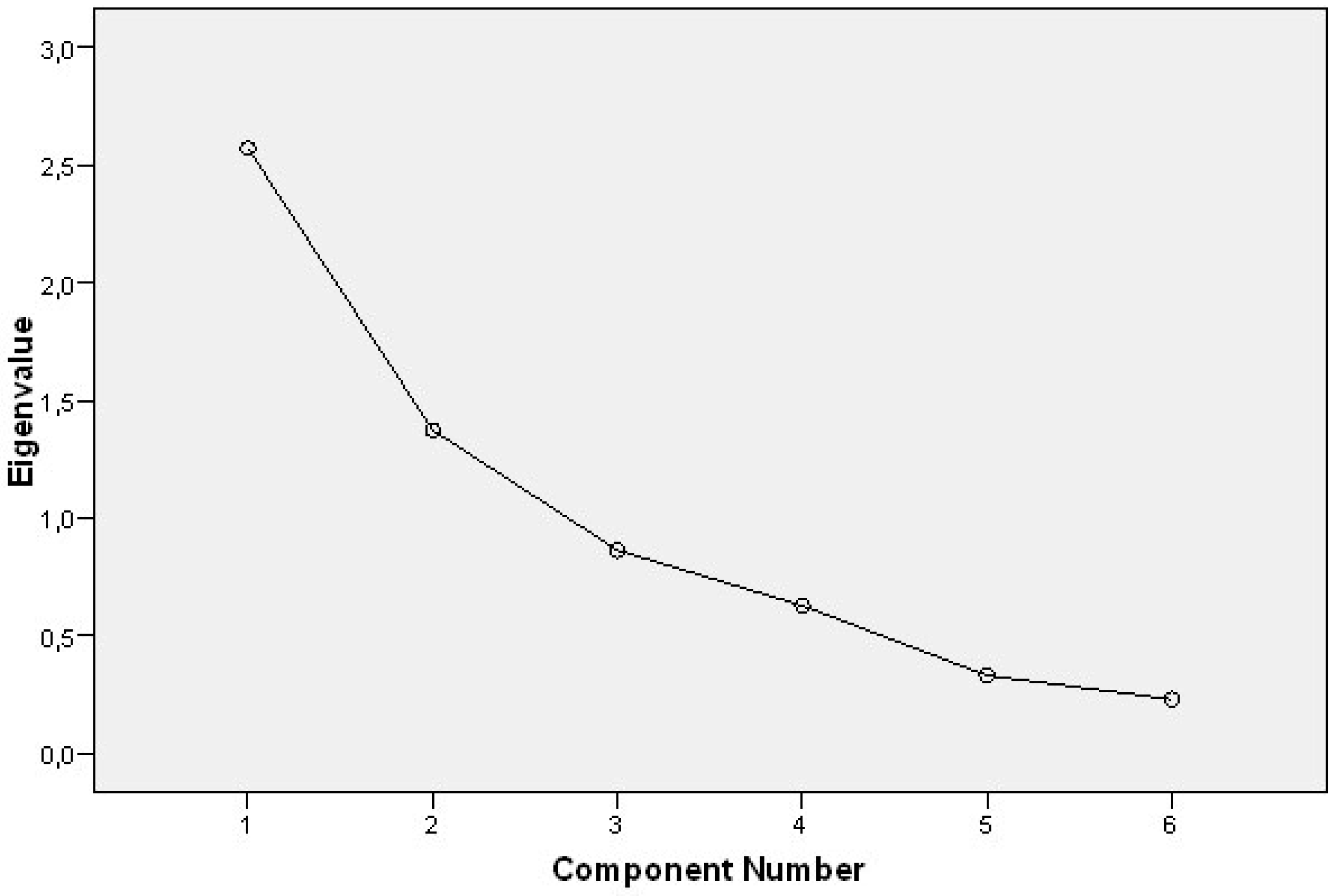
4.4. Factor Structure
4.5. Informal Conversations
5. Discussion and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Nielsen, J. Usability Engineering; Morgan Kaufmann Publishers Inc.: San Francisco, CA, USA, 2008. [Google Scholar]
- Bevan, N. International standards for HCI and usability. Int. J. Hum. Comput. Stud. 2001, 55, 533–552. [Google Scholar] [CrossRef]
- Abran, A.; Khelifi, A.; Suryn, W.; Seffah, A. Usability meanings and interpretations in ISO standards. Softw. Qual. J. 2003, 11, 325–338. [Google Scholar] [CrossRef]
- ISO 9241–11. Ergonomic Requirements for Office Work with Visual Display Terminals (VDTs) Part 11: Guidance on Usability. Available online: http://www.iso.org/iso/catalogue_detail.htm?csnumber=16883 (accessed on 25 April 2017).
- Jokela, T.; Iivari, N.; Matero, J.; Karukka, M. The standard of user-centered design and the standard definition of usability: analyzing ISO 13407 against ISO 9241-11. In Proceedings of the Latin American Conference on Human-Computer Interaction, Rio de Janeiro, Brazil, 17–20 August 2003; ACM New York: New York, NY, USA, 2003; pp. 53–60. [Google Scholar]
- Holden, M.K. Virtual environments for motor rehabilitation: Review. Cyberpsychol. Behav. 2005, 8, 187–211. [Google Scholar] [CrossRef] [PubMed]
- Sveistrup, H. Motor rehabilitation using virtual reality. J. Neuroeng. Rehabil. 2004, 1, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lange, B.; Koenig, S.; Chang, C.Y.; McConnell, E.; Suma, E.; Bolas, M.; Rizzo, A. Designing informed game-based rehabilitation tasks leveraging advances in virtual reality. Disabil. Rehabil. 2012, 34, 1863–1870. [Google Scholar] [CrossRef] [PubMed]
- Lewis, G.N.; Rosie, J.A. Virtual reality games for movement rehabilitation in neurological conditions: How do we meet the needs and expectations of the users? Disabil. Rehabil. 2012, 34, 1880–1886. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.K.; Mohd Nordin, N.A.; Abd Aziz, N.A.; Lim, B.K.; Soh, L.C. Effects of substituting a portion of standard physiotherapy time with virtual reality games among community-dwelling stroke survivors. BMC Neurol. 2013, 13, 199. [Google Scholar] [CrossRef] [PubMed]
- Green, D.; Wilson, P.H. Use of virtual reality in rehabilitation of movement in children with hemiplegia-a multiple case study evaluation. Disabil. Rehabil. 2012, 34, 593–604. [Google Scholar] [CrossRef] [PubMed]
- Meldrum, D.; Herdman, S.; Moloney, R.; Murray, D.; Duffy, D.; Malone, K.; French, H.; Hone, S.; Conroy, R.; McConn-Walsh, R. Effectiveness of conventional versus virtual reality based vestibular rehabilitation in the treatment of dizziness, gait and balance impairment in adults with unilateral peripheral vestibular loss: a randomized controlled trial. BMC Ear Nose Throat Disord. 2012, 12, 3. [Google Scholar] [CrossRef] [PubMed]
- Gil-Gómez, J.A.; Lloréns, R.; Alcañiz, M.; Colomer, C. Effectiveness of a Wii balance board-based system (eBaViR) for balance rehabilitation: A pilot randomized clinical trial in patients with acquired brain injury. J. NeuroEng. Rehabil. 2011, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Albiol-Pérez, S.; Gil-Gómez, J.A.; Lloréns, R.; Alcañiz, M.; Font, C.C. The role of virtual motor rehabilitation: A quantitative analysis between acute and chronic patients with acquired brain injury. IEEE J. Biomed. Health Inform. 2014, 18, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Brooke, J. SUS: A “quick and dirty” usability scale. In Usability Evaluation in Industry; Jordan, P.W., Thomas, B., Weerdmeester, B.A., McClelland, A.L., Eds.; Taylor and Francis: London, UK, 1996; pp. 189–194. [Google Scholar]
- Brooke, J. SUS: A Retrospective. J. Usabil. Stud. 2013, 8, 29–40. [Google Scholar]
- DeWitt, A.J.; Kuljis, J. Aligning usability and security: A usability study of Polaris. In Proceedings of the 2nd Symposium on Usable Privacy and Security, Pittsburgh, PA, USA, 12–14 July 2006; ACM: New York, NY, USA, 2006; pp. 1–7. [Google Scholar]
- Jokela, T.; Koivumaa, J.; Pirkola, J.; Salminen, P.; Kantola, N. Methods for quantitative usability requirements: a case study on the development of the user interface of a mobile phone. Pers. Ubiquitous Comput. 2006, 10, 345–355. [Google Scholar] [CrossRef]
- Vermeulen, J.; Neyens, J.C.; Spreeuwenberg, M.D.; van Rossum, E.; Sipers, W.; Habets, H.; Hewson, D.J.; de Witte, L.P. User-centered development and testing of a monitoring system that provides feedback regarding physical functioning to elderly people. Patient Preference Adher. 2013, 7, 843–854. [Google Scholar] [CrossRef] [PubMed]
- Költringer, T.; Grechenig, T. Comparing the immediate usability of graffiti 2 and virtual keyboard. Proceedings of CHI ’04 Extended Abstracts on Human Factors in Computing Systems, Vienna, Austria, 24–29 April 2004; ACM: New York, NY, USA, 2004; pp. 1175–1178. [Google Scholar]
- Tsung-han, T.; Fong-gong, W.; Yu-Hsiu, H. The Survey of Usability Evaluation in Social Network Sites’ Reply Mechanism. In Proceedings of the International Conference on Universal Access in Human-Computer Interaction, Las Vegas, NV, USA, 21–26 July 2013; Springer: Berlin, Germany, 2013; pp. 718–725. [Google Scholar]
- Duffy, S.A.; Fowler, K.E.; Flanagan, P.S.; Ronis, D.L.; Ewing, L.A.; Waltje, A.H. The development of the tobacco tactics website. JMIR Res. Protoc. 2013, 2, e22. [Google Scholar] [CrossRef] [PubMed]
- Mathew, D.; McKibbon, K.A.; Lokker, C.; Colquhoun, H. Engaging With a Wiki Related to Knowledge Translation: A Survey of WhatisKT Wiki Users. J. Med. Internet. Res. 2014, 16, e21. [Google Scholar] [CrossRef] [PubMed]
- Tolentino, G.P.; Battaglini, C.; Pereira, A.C.V.; de Oliveria, R.J.; de Paula, M.G.M. Usability of Serious Games for Health. In Proceedings of the 3rd International Conference on Games and Virtual Worlds for Serious Applications, Athens, Greece, 4–6 May 2011; IEEE Computer Society: Los Alamitos, CA, USA, 2011; pp. 172–175. [Google Scholar]
- Mattos, L.S.; Deshpande, N.; Barresi, G.; Guastini, L.; Peretti, G. A novel computerized surgeon-machine interface for robot-assisted laser phonomicrosurgery. Laryngoscope 2013, 124, 1887–1894. [Google Scholar] [CrossRef] [PubMed]
- Meldrum, D.; Glennon, A.; Herdman, S.; Murray, D.; McConn-Walsh, R. Virtual reality rehabilitation of balance: assessment of the usability of the Nintendo Wii(®) Fit Plus. Disabil. Rehabil. Assist. Technol. 2012, 7, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Duvinage, M.; Castermans, T.; Petieau, M.; Seetharaman, K.; Hoellinger, T.; Cheron, G.; Dutoit, T. A subjective assessment of a P300 BCI system for lower-limb rehabilitation purposes. In Proceedings of the 34th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; IEEE Service Center: Piscataway, NJ, USA, 2012; pp. 3845–3849. [Google Scholar]
- Kalawsky, R.S. VRUSE–A computerised diagnostic tool: For usability evaluation of virtual/synthetic environment systems. Appl. Ergon. 1999, 30, 11–25. [Google Scholar] [CrossRef]
- Fitzgerald, D.; Kelly, D.; Ward, T.; Markham, C.; Caulfield, B. Usability Evaluation of E-Motion: A Virtual Rehabilitation System Designed to Demonstrate, Instruct and Monitor a Therapeutic Exercise Programme. In Proceedings of the Virtual Rehabilitation Conference, Vancouver, BC, Canada, 25–27 August 2008; IEEE Service Center: Piscataway, NJ, USA, 2008; pp. 144–149. [Google Scholar]
- Jeon, W.; Clamann, M.; Zhu, B.; Gil, G.H.; Kaber, D. Usability evaluation of a virtual reality system for motor skill training. In Advances in Usability Evaluation Part II; Rebelo, F., Soares, M.M., Eds.; CRC Press: Boca Raton, FL, USA, 2012; pp. 86–95. [Google Scholar]
- Cameirão, M.S.; Badia, S.B.; Oller, E.D.; Verschure, P.F. Neurorehabilitation using the virtual reality based Rehabilitation Gaming System: methodology, design, psychometrics, usability and validation. J. Neuroeng. Rehabil. 2010, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Regenbrecht, H.; Hoermann, S.; McGregor, G.; Dixon, B.; Franz, E.; Ott, C.; Hale, L.; Schubert, T.; Hoermann, J. Visual manipulations for motor rehabilitation. Comput. Graph. 2012, 36, 819–834. [Google Scholar] [CrossRef]
- Shin, J.H.; Ryu, H.; Jang, S.H. A task-specific interactive game-based virtual reality rehabilitation system for patients with stroke: A usability test and two clinical experiments. J. Neuroeng. Rehabil. 2014, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kizony, R.; Katz, N.; Weiss, P.L. Adapting an immersive virtual reality system for rehabilitation. J. Vis. Comput. Animat. 2003, 14, 261–268. [Google Scholar] [CrossRef]
- Witmer, B.G.; Singer, M.J. Measuring Presence in Virtual Environments: A Presence Questionnaire. Presence Teleoper. Virtual Environ. 1998, 7, 225–240. [Google Scholar] [CrossRef]
- Kizony, R.; Katz, N.; Rand, D.; Weiss, P.L. Short Feedback Questionnaire (SFQ) to enhance client-centered participation in virtual environments. CyberPsychol. Behav. 2006, 9, 687–688. [Google Scholar]
- Kizony, R.; Raz, L.; Katz, N.; Weingarden, H.; Weiss, P.L. Using a video projected VR system for patients with spinal cord injury. J. Rehabil. Res. Dev. 2005, 42, 595–608. [Google Scholar] [CrossRef] [PubMed]
- Iman, B.; Miller, W.C.; McLaren, L.; Chapman, P.; Finlayson, H. Feasibility of the Nintendo WiiFit™ for improving walking in individuals with a lower limb amputation. SAGE Open Med. 2013, 1, 1–11. [Google Scholar]
- Gil-Gómez, J.A.; Manzano-Hernández, P.; Albiol-Pérez, S.; Aula-Valero, C.; Gil-Gómez, H.; Lozano-Quilis, J.A. SEQ: Suitability evaluation questionnaire for virtual rehabilitation systems. Application in a virtual rehabilitation system for balance rehabilitation. In Proceedings of the 7th International Conference on Pervasive Computing Technologies for Healthcare, Venice, Italy, 5–8 May 2013; pp. 335–338. [Google Scholar]
- Muñoz Tomás, M.T.; Gil-Gómez, J.A.; Gil-Gómez, H.; Lozano-Quilis, J.A.; Albiol-Pérez, S.; Forcano García, M. Suitability of virtual rehabilitation for the elderly: A study of a virtual rehabilitation system using the SEQ. Eur. Geriatr. Med. 2013, 4, S109. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.; Mchugh, P.R. Mini-Mental State: A practical method for grading the cognitive state of patients for the clinicians. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Forcano García, M.; Albiol-Pérez, S.; Aula Valero, M.C.; Gil-Gómez, J.A.; Solsona Hernández, S.; Manzano Hernández, P. Balance virtual rehabilitation in the elderly: The use of the “ABAR” system. Eur. Geriatr. Med. 2013, 4, S109. [Google Scholar] [CrossRef]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Babikian, T.; Asarnow, R. Neurocognitive outcomes and recovery after pediatric TBI: Meta-analytic review of the literature. Neuropsychology 2009, 23, 283–296. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L. Starting at the beginning: an introduction to coefficient alpha and internal consistency. J. Personal. Assess. 2003, 80, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.E.C.; Taketomi, T.; Sandor, C.; Polvi, J.; Yamamoto, G.; Kato, H. A usability scale for handheld augmented reality. In Proceedings of the 20th ACM Symposium on Virtual Reality Software and Technology, Edinburgh, UK, 11–13 November 2014; ACM: New York, NY, USA, 2014; pp. 167–176. [Google Scholar]
- Fackrell, K.; Fearnley, C.; Hoare, D.J.; Sereda, M. Hyperacusis Questionnaire as a Tool for Measuring Hypersensitivity to Sound in a Tinnitus Research Population. BioMed Res. Int. 2015, 2015, 1–12. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Question | Response |
|---|---|
| Not at All–Very Much | |
| Q1. Did you enjoy your experience with the system? | 1 2 3 4 5 |
| Q2. Were you successful using the system? | 1 2 3 4 5 |
| Q3. Were you able to control the system? | 1 2 3 4 5 |
| Q4. Is the information provided by the system clear? | 1 2 3 4 5 |
| Q5. Did you feel discomfort during your experience with the system? | 1 2 3 4 5 |
| Q6. Do you think that this system will be helpful for your rehabilitation? | 1 2 3 4 5 |
| Mean | SD | |
|---|---|---|
| Age (years) | 74.25 | 14.59 |
| Duration of the balance disorders (years) | 3.39 | 5.51 |
| n | % | |
| Sex | ||
| Male | 19 | 47.50 |
| Female | 21 | 52.50 |
| Chronicity | ||
| Postacute (0–5 months post-injury) | 10 | 25.00 |
| Acute (6–23 months post-injury) | 11 | 27.50 |
| Chronic (24 months or more post-injury) | 19 | 47.50 |
| Background domicile | ||
| Urban | 30 | 75.00 |
| Rural | 10 | 25.00 |
| Level of studies | ||
| No studies | 3 | 7.50 |
| Primary studies | 24 | 60.00 |
| Secondary studies | 10 | 25.00 |
| Higher studies | 3 | 7.50 |
| Question | Mean | SD | Scale Mean if Item Deleted | Corrected Item-Total Correlation | Cronbach’s Alpha if Item Deleted |
|---|---|---|---|---|---|
| Q1 | 4.43 | 0.874 | 21.38 | 0.326 | 0.712 |
| Q2 | 4.23 | 1.097 | 21.58 | 0.666 | 0.597 |
| Q3 | 3.80 | 1.224 | 22.00 | 0.572 | 0.637 |
| Q4 | 4.65 | 0.662 | 21.15 | 0.404 | 0.694 |
| 6-Q5 | 4.70 | 0.608 | 21.10 | 0.496 | 0.678 |
| Q6 | 4.00 | 0.961 | 21.80 | 0.321 | 0.716 |
| Component | ||
|---|---|---|
| 1 | 2 | |
| Questions | ||
| Q2 | 0.816 | |
| Q3 | 0.780 | |
| Q5 | 0.669 | 0.647 |
| Q4 | 0.582 | −0.414 |
| Q6 | 0.541 | 0.672 |
| Q1 | 0.468 | −0.490 |
| Variance explained (%) | 42.869% | 22.908% |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil-Gómez, J.-A.; Manzano-Hernández, P.; Albiol-Pérez, S.; Aula-Valero, C.; Gil-Gómez, H.; Lozano-Quilis, J.-A. USEQ: A Short Questionnaire for Satisfaction Evaluation of Virtual Rehabilitation Systems. Sensors 2017, 17, 1589. https://doi.org/10.3390/s17071589
Gil-Gómez J-A, Manzano-Hernández P, Albiol-Pérez S, Aula-Valero C, Gil-Gómez H, Lozano-Quilis J-A. USEQ: A Short Questionnaire for Satisfaction Evaluation of Virtual Rehabilitation Systems. Sensors. 2017; 17(7):1589. https://doi.org/10.3390/s17071589
Chicago/Turabian StyleGil-Gómez, José-Antonio, Pilar Manzano-Hernández, Sergio Albiol-Pérez, Carmen Aula-Valero, Hermenegildo Gil-Gómez, and José-Antonio Lozano-Quilis. 2017. "USEQ: A Short Questionnaire for Satisfaction Evaluation of Virtual Rehabilitation Systems" Sensors 17, no. 7: 1589. https://doi.org/10.3390/s17071589