Quality of Life in Chronic Ketogenic Diet Treatment: The GLUT1DS Population Perspective

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Subjects
2.3. Instruments
2.4. Statistical Analysis
3. Results
3.1. Study Population
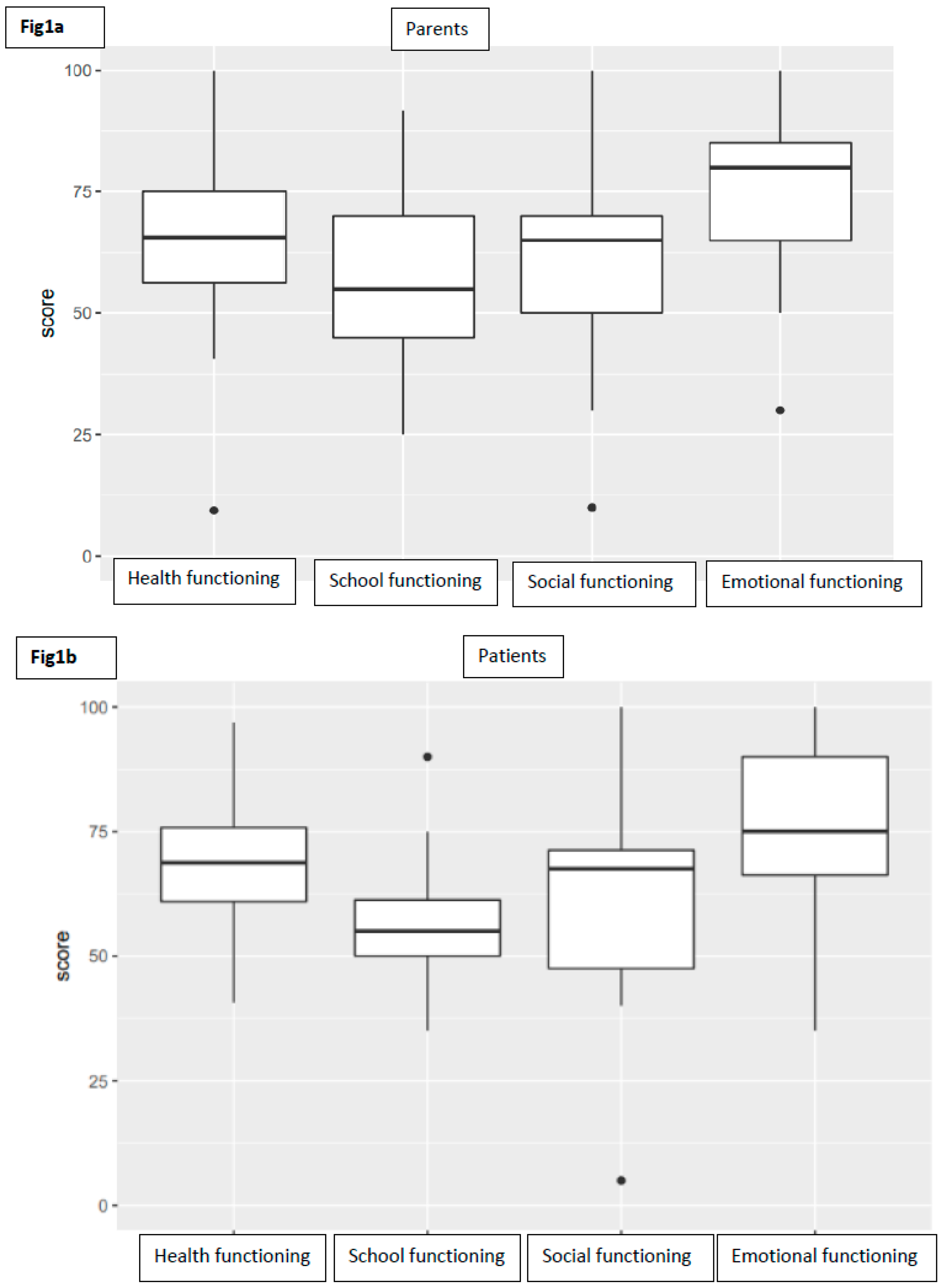
3.2. Health Related Quality of Life
3.3. Factors Influencing HRQOL
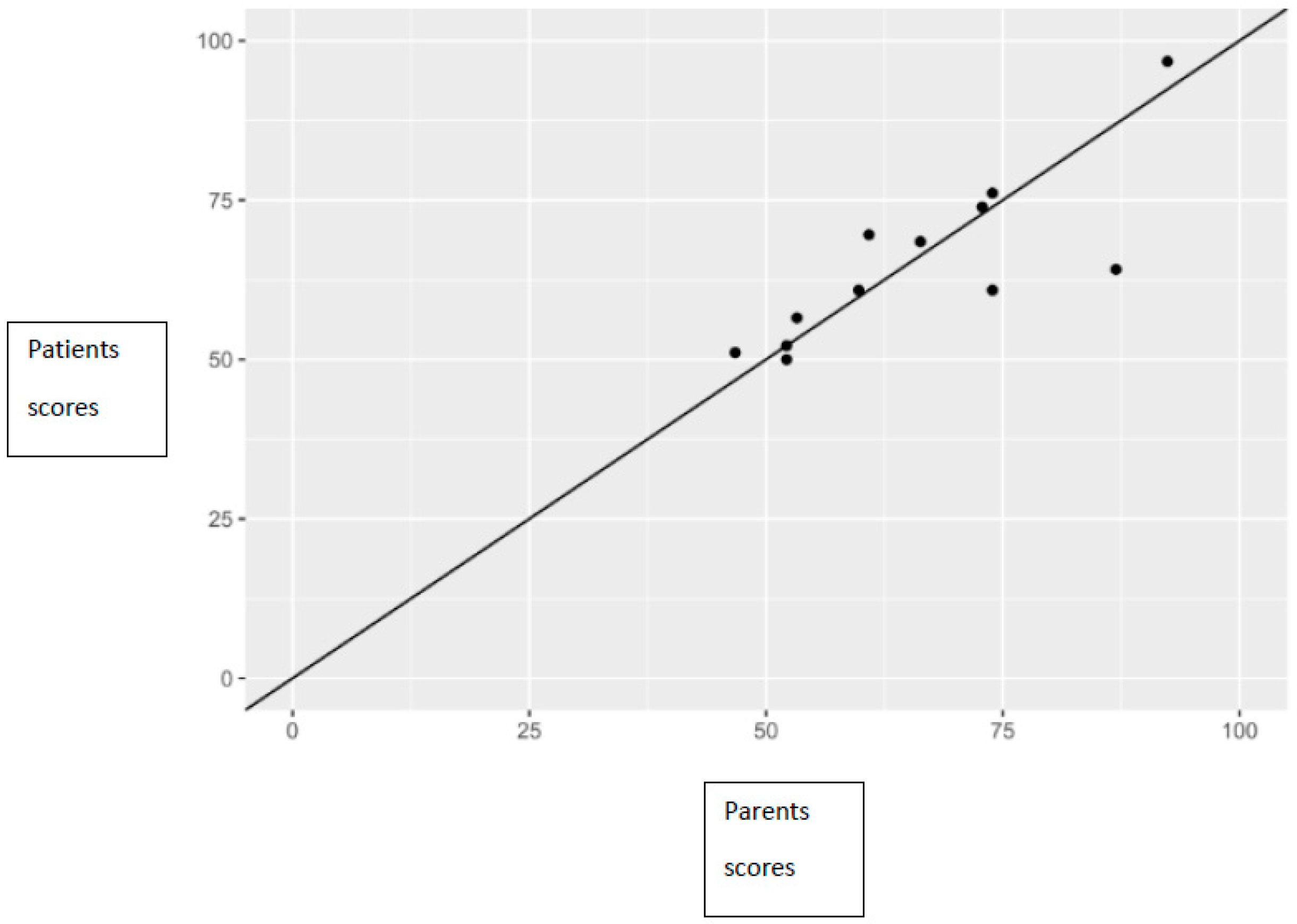
3.4. Concordance between Self and Proxy Reports
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Seidner, G.; Alvarez, M.G.; Yeh, J.I.; O’Driscoll, K.R.; Klepper, J.; Stump, T.S.; Wang, D.; Spinner, N.B.; Birnbaum, M.J.; De Vivo, D.C. Deficiency syndrome caused by haploinsufficiency of the blood-brain barrier hexose carrier. Nat. Genet. 1998, 18, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Klepper, J.; Voit, T. Facilitated glucose transporter protein type 1 (GLUT1) deficiency syndrome: Impaired glucose transport into brain—A review. Eur. J. Pediatr. 2002, 161, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Klepper, J.; Leiendecker, B. GLUT1 deficiency syndrome—2007 update. Dev. Med. Child Neurol. 2007, 49, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Leen, W.G.; Klepper, J.; Verbeek, M.M.; Leferink, M.; Hofste, T.; van Engelen, B.G.; Wevers, R.A.; Arthur, T.; Bahi-Buisson, N.; Ballhausen, D.; et al. Glucose transporter-1 deficiency syndrome: The expanding clinical and genetic spectrum of a treatable disorder. Brain 2010, 33, 655–670. [Google Scholar] [CrossRef] [PubMed]
- Pearson, T.S.; Akman, C.; Hinton, V.J.; Engelstad, K.; De Vivo, D.C. Phenotypic spectrum of Glucose Transporter Type 1 Deficiency Syndrome (Glut1 DS). Curr. Neurol. Neurosci. Rep. 2013, 13, 342. [Google Scholar] [CrossRef]
- De Giorgis, V.; Teutonico, F.; Cereda, C.; Balottin, U.; Bianchi, M.; Giordano, L.; Olivotto, S.; Ragona, F.; Tagliabue, A.; Zorzi, G.; et al. Sporadic and familial glut1ds Italian patients: A wide clinical variability. Seizure 2015, 24, 28–32. [Google Scholar] [CrossRef] [Green Version]
- Koch, H.; Weber, Y.G. The glucose transporter type 1 (Glut1) syndromes. Epilepsy Behav. 2019, 91, 90–93. [Google Scholar] [CrossRef]
- De Giorgis, V.; Varesio, C.; Baldassari, C.; Piazza, E.; Olivotto, S.; Macasaet, J.; Balottin, U.; Veggiotti, P. Atypical Manifestations in Glut1 Deficiency Syndrome. J. Child Neurol. 2016, 31, 1174–1180. [Google Scholar] [CrossRef]
- De Vivo, D.C.; Trifiletti, R.R.; Jacobson, R.I.; Ronen, G.M.; Behmand, R.A.; Harik, S.I. Defective glucose transporter across the blood-brain barrier as a cause of peersisitent hypoglicorrhachia, seizures and developmental delay. N. Engl. J. Med. 1991, 325, 703–709. [Google Scholar] [CrossRef]
- Klepper, J. GLUT1 deficiency syndrome in clinical practice. Epilepsy Res. 2012, 100, 272–277. [Google Scholar] [CrossRef]
- Veggiotti, P.; De Giorgis, V. Dietary Treatments and New Therapeutic Perspective in GLUT1 Deficiency Syndrome. Curr. Treat. Options Neurol. 2014, 16, 291. [Google Scholar] [CrossRef] [PubMed]
- Ramm-Pettersen, A.; Nakken, K.O.; Skogseid, I.M.; Randby, H.; Skei, E.B.; Bindoff, L.A.; Selmer, K.K. Good outcome in patients with early dietary treatment of GLUT-1 deficiency syndrome: Results from a retrospective Norwegian study. Dev. Med. Child Neurol. 2013, 55, 440–447. [Google Scholar] [CrossRef] [PubMed]
- De Giorgis, V.; Veggiotti, P. GLUT1 deficiency syndrome 2013: Current state of the art. Seizure 2013, 22, 803–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kass, H.R.; Winesett, S.P.; Bessone, S.K.; Turner, Z.; Kossoff, E.H. Use of dietary therapies amongst patients with GLUT1 deficiency syndrome. Seizure 2016, 35, 83–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, Y.; Oguni, H.; Ito, S.; Oguni, M.; Osawa, M. A modified Atkins diet is promising as a treatment for glucose transporter type 1 deficiency syndrome. Dev. Med. Child Neurol. 2011, 53, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Ramm-Pettersen, A.; Stabell, K.E.; Nakken, K.O.; Selmer, K.K. Does ketogenic diet improve cognitive function in patients with GLUT1-DS? A 6- to 17-month follow-up study. Epilepsy Behav. 2014, 39, 111–115. [Google Scholar] [CrossRef] [PubMed]
- De Giorgis, V.; Masnada, S.; Varesio, C.; Chiappedi, M.A.; Zanaboni, M.; Pasca, L.; Filippini, M.; Macasaet, J.A.; Valente, M.; Ferraris, C.; et al. Overall cognitive profiles in patients with GLUT1 Deficiency Syndrome. Brain Behav. 2019, 9, e01224. [Google Scholar] [CrossRef] [PubMed]
- Donner, E.J.; Guzel, O.; Jehle, R.S.; Klepper, J.; Kang, H.C.; Lambrechts, D.A.; Liu, Y.M.C.; Nathan, J.K.; Nordli, D.R.; Pfeifer, H.H.; et al. Practice Committee of the Child Neurology Society. Optimal clinical management of children receiving dietary therapies for epilepsy: Updated recommendations of the International Ketogenic Diet Study Group. Epilepsia Open. 2018, 3, 175–192. [Google Scholar]
- Freeman, J.M.; Kossoff, E.H.; Hartman, A.L. The ketogenic diet: One decade later. Pediatrics 2007, 119, 535–543. [Google Scholar] [CrossRef]
- Ito, S.; Oguni, H.; Ito, Y.; Ishigaki, K.; Ohinata, J.; Osawa, M. Modified Atkins diet therapy for a case with glucose transporter type 1 deficiency syndrome. Brain Dev. 2008, 30, 226–228. [Google Scholar] [CrossRef]
- Haberlandt, E.; Karall, D.; Jud, V.; Baumgartner, S.S.; Zotter, S.; Rostasy, K.; Baumann, M.; Scholl-Buergi, S. Glucose transporter type 1 deficiency syndrome effectively treated with modified Atkins diet. Neuropediatrics 2014, 45, 117–119. [Google Scholar] [PubMed]
- Wang, D.; Pascual, J.M.; Yang, H.; Engelstad, K.; Jhung, S.; Sun, R.P.; De Vivo, D.C. Glut-1 deficiency syndrome: Clinical, genetic, and therapeutic aspects. Ann. Neurol. 2005, 57, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B.H. Prenatal diagnosis of disorders of energy metabolism. Semin Neurol. 2001, 21, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Wheless, J.W. The ketogenic diet: Fa(c)t or fiction. J. Child Neurol. 1995, 10, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Saxena, S.; Orley, J.; WHOQOL Group. Quality of life assessment: The World Health Organization perspective. Eur. Psychiatry 1997, 12, 263–266. [Google Scholar] [CrossRef]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQL TM 4.0: Reliability and validity of the Pediatric Quality of Life Inventory TM Version 4.0 generic core scales in healthy and patient populations. Med. Care. 2001, 39, 800–812. [Google Scholar] [CrossRef]
- Varni, J.W.; Limbers, C.A. The Pe diatric Quality of Life Inventory: Measuring Pediatric Health—Related Quality of Life from the perspective of children and their parents. Pediatr. Clin. North Am. 2009, 56, 843–863. [Google Scholar] [CrossRef]
- Bruce, S.; Devlin, A.; Air, L.; Cook, L. Changes in quality of life as a result of ketogenic diet therapy: A new approach to assessment with the potential for positive therapeutic effects. Epilepsy Behav. 2017, 66, 100–104. [Google Scholar] [CrossRef]
- Barwick, K.; Parker, T.; Murphy, N.; Todd, A.; Leveritt, M.; Wilkinson, S.A. Development and pilot testing of a parent-reported health-related quality of life measure for children on the ketogenic diet: The KetoQoL. Nutr. Diet. 2017, 74, 521–528. [Google Scholar] [CrossRef]
- Kim, J.; Chung, H.; Amtmann, D.; Salem, R.; Park, R.; Askew, R.L. Symptoms and quality of life indicators among children with chronic medical conditions. Disabil. Health J. 2014, 7, 96–104. [Google Scholar] [CrossRef]
- Varni, J.W.; Burwinkle, T.M.; Seid, M.; Skarr, D. The PedsQL TM 4.0 as a pediatric population health measure: Feasibility, reliability, and validity. Ambul. Pediatr. 2003, 3, 329–341. [Google Scholar] [CrossRef]
- Varni, J.W.; Limbers, C.A.; Burwinkle, T.M. How young can children reliably and validly self-report their health-related quality of life? An analysis of 8591 children across age subgroups with the PedsQL TM 4.0 Generic Core Scales. Health Qual. Life Outcomes 2007, 5, 1. [Google Scholar] [CrossRef]
- Varni, J.W.; Limbers, C.A.; Burwinkle, T.M. Parent proxy-report of their children’s health-related quality of life: An analysis of 13,878 parents’ reliability and validity across age subgroups using the PedsQL TM 4.0 Generic Core Scales. Health Qual. Life Outcomes 2007, 5, 1–2. [Google Scholar] [CrossRef]
- Bertoli, S.; Neri, I.G.; Trentani, C.; Ferraris, C.; De Amicis, R.; Battezzati, A.; Veggiotti, P.; De Giorgis, V.; Tagliabue, A. Short-term effects of ketogenic diet on anthropometric parameters, body fat distribution, and inflammatory cytokine production in GLUT1 deficiency syndrome. Nutrition 2015, 31, 981–987. [Google Scholar] [CrossRef]
- Oguni, H.; Ito, Y.; Otani, Y.; Nagata, S. Questionnaire survey on the current status of ketogenic diet therapy in patients with glucose transporter 1 deficiency syndrome (GLUT1DS) in Japan. Eur. J. Paediatr. Neurol. 2018, 22, 482–487. [Google Scholar] [CrossRef]
- Fujii, T.; Ito, Y.; Takahashi, S.; Shimono, K.; Natsume, J.; Yanagihara, K.; Oguni, H. Outcome of ketogenic diets in GLUT1 deficiency syndrome in Japan: A nationwide survey. Brain Dev. 2016, 38, 628–637. [Google Scholar] [CrossRef]
- Bertoli, S.; Trentani, C.; Ferraris, C.; De Giorgis, V.; Veggiotti, P.; Tagliabue, A. Long-term effects of a ketogenic diet on body composition and bone mineralization in GLUT-1 deficiency syndrome: A case series. Nutrition 2014, 30, 726–728. [Google Scholar] [CrossRef]
- Pasca, L.; De Giorgis, V.; Macasaet, J.A.; Trentani, C.; Tagliabue, A.; Veggiotti, P. The changing face of dietary therapy for epilepsy. Eur. J. Pediatr. 2016, 175, 1267–1276. [Google Scholar] [CrossRef]
- Ferraris, C.; Guglielmetti, M.; Pasca, L.; De Giorgis, V.; Ferraro, O.E.; Brambilla, I.; Leone, A.; De Amicis, R.; Bertoli, S.; Veggiotti, P.; et al. Impact of the Ketogenic Diet on Linear Growth in Children: A Single-Center Retrospective Analysis of 34 Cases. Nutrition 2019, 11, 1442. [Google Scholar] [CrossRef]
- Bekker, Y.A.C.; Lambrechts, D.A.; Verhoeven, J.S.; Van Boxtel, J.; Troost, C.; Kamsteeg, E.J.; Willemsen, M.A.; Braakman, H.M.H. Failure of ketogenic diet therapy in GLUT1 deficiency syndrome. Eur. J. Paediatr. Neurol. 2019, 23, 404–409. [Google Scholar] [CrossRef]
- Eminoglu, T.F.; Soysal, S.A.; Tumer, L.; Okur, I.; Hasanoglu, A. Quality of life in children treated with restrictive diet for inherited. Ped. Int. 2013, 55, 428–433. [Google Scholar] [CrossRef]
- Bosch, A.M.; Burlina, A.; Cunningham, A.; Bettiol, E.; Moreau-Stucker, F.; Koledova, E.; Benmedjahed, K.; Regnault, A. Assessment of the impact of phenylketonuria and its treatment on quality of life of patients and parents from seven European countries. Orphanet J. Rare Dis. 2015, 10, 80. [Google Scholar] [CrossRef]
- Eggink, H.; Kuiper, A.; Peall, K.J.; Contarino, M.F.; Bosch, A.M.; Post, B.; Sival, D.A.; Tijssen, M.A.J.; Koning, T. Rare inborn errors of metabolism with movement disorders: A case study to evaluate the impact upon quality of life and adaptive functioning. Orphanet J. Rare Diseases 2014, 9, 177. [Google Scholar] [CrossRef]
- Hallbook, T.; Lundgren, J.; Rosén, I. Ketogenic diet improves sleep quality in children with therapy-resistant epilepsy. Epilepsia 2007, 48, 59–65. [Google Scholar] [CrossRef]
- Alter, A.S.; Engelstad, K.; Hinton, V.J.; Montes, J.; Pearson, T.S.; Akman, C.I.; De Vivo, D.C. Long-term clinical course of Glut1 deficiency syndrome. J. Child Neurol. 2015, 30, 160–169. [Google Scholar] [CrossRef]
- Eiser, C.; Varni, J.W. Health-related quality of life and symptom reporting: Similarities and differences between children and their parents. Eur. J. Pediatr. 2013, 172, 1299–1304. [Google Scholar] [CrossRef]
- Upton, P.; Lawford, J.; Eiser, C. Parent—Child agreement across child health-related quality of life instruments: A review of the literature. Qual. Life Res. 2008, 17, 895–913. [Google Scholar] [CrossRef]
- Costello, E.J.; Edelbrock, C.; Costello, A.J.; Dulcan, M.K.; Burns, B.J.; Brent, D. Psychopathology in pediatric primary care: The new hidden morbidity. Pediatrics 1988, 82, 415–424. [Google Scholar]
- Seid, M.; Varni, J.W.; Segall, D.; Kurtin, P.S. Health-related quality of life as a predictor of pediatric healthcare costs: A two-year prospective cohort analysis. Health Qual. Life Outcomes 2004, 10, 1–10. [Google Scholar]



{kind=link}
{kind=link}
| ID | Age | Seizures | MD | ID | KD Ratio | Concomitant AED | PedsQoL Score | Parents | Patient |
|---|---|---|---|---|---|---|---|---|---|
| pt 1 | 4 | absent | absent | absent | 3.0:1 | no | Total functioning | 94 | NA |
| health functioning | 97 | NA | |||||||
| emotional functioning | 97 | NA | |||||||
| social functioning | 100 | NA | |||||||
| school functioning | 92 | NA | |||||||
| pt 2 | 11 | absent | absent | mild | 3.0:1 | no | Total functioning | 73 | 74 |
| health functioning | 69 | 81 | |||||||
| emotional functioning | 80 | 90 | |||||||
| social functioning | 65 | 65 | |||||||
| school functioning | 80 | 55 | |||||||
| pt 3 | 15 | absent | daily | moderate | 3.0:1 | no | Total functioning | 60 | 61 |
| health functioning | 56 | 63 | |||||||
| emotional functioning | 100 | 95 | |||||||
| social functioning | 45 | 50 | |||||||
| school functioning | 40 | 35 | |||||||
| pt 4 | 22 | absent | less than monthly | mild | 3.0:1 | no | Total functioning | 47 | 51 |
| health functioning | 72 | 75 | |||||||
| emotional functioning | 30 | 35 | |||||||
| social functioning | 30 | 50 | |||||||
| school functioning | 40 | 40 | |||||||
| pt 5 | 16 | absent | absent | mild | 3.0:1 | LTG | Total functioning | 52 | 50 |
| health functioning | 44 | 41 | |||||||
| emotional functioning | 50 | 50 | |||||||
| social functioning | 40 | 40 | |||||||
| school functioning | 80 | 75 | |||||||
| pt 6 | 5 | absent | absent | mild | 3.0:1 | no | Total functioning | 61 | 70 |
| health functioning | 56 | 69 | |||||||
| emotional functioning | 65 | 70 | |||||||
| social functioning | 80 | 80 | |||||||
| school functioning | 45 | 60 | |||||||
| pt 7 | 7 | absent | absent | absent | 2.0:1 | no | Total functioning | 74 | 61 |
| health functioning | 75 | 56 | |||||||
| emotional functioning | 85 | 70 | |||||||
| social functioning | 70 | 70 | |||||||
| school functioning | 65 | 50 | |||||||
| pt 8 | 13 | absent | less than monthly | absent | 2.0:1 | no | Total functioning | 92 | 97 |
| health functioning | 94 | 97 | |||||||
| emotional functioning | 100 | 100 | |||||||
| social functioning | 100 | 100 | |||||||
| school functioning | 75 | 90 | |||||||
| pt 9 | 3 | absent | weekly | absent | 3.0:1 | no | Total functioning | 58 | NA |
| health functioning | 63 | NA | |||||||
| emotional functioning | 50 | NA | |||||||
| social functioning | 65 | NA | |||||||
| school functioning | 50 | NA | |||||||
| pt 10 | 3 | absent | less than monthly | mild | 2.0:1 | no | Total functioning | 43 | NA |
| health functioning | 10 | NA | |||||||
| emotional functioning | 80 | NA | |||||||
| social functioning | 70 | NA | |||||||
| school functioning | 15 | NA | |||||||
| pt 11 | 19 | absent | monthly | mild | 3.0:1 | VPA | Total functioning | 66 | 68 |
| health functioning | 72 | 69 | |||||||
| emotional functioning | 65 | 80 | |||||||
| social functioning | 70 | 70 | |||||||
| school functioning | 55 | 55 | |||||||
| pt 12 | 13 | absent | absent | absent | 2.0:1 | no | Total functioning | 74 | 76 |
| health functioning | 75 | 78 | |||||||
| emotional functioning | 90 | 90 | |||||||
| social functioning | 65 | 70 | |||||||
| school functioning | 65 | 65 | |||||||
| pt 13 | 13 | absent | absent | moderate | 3.0:1 | no | Total functioning | 52 | 52 |
| health functioning | 66 | 66 | |||||||
| emotional functioning | 65 | 70 | |||||||
| social functioning | 10 | 5 | |||||||
| school functioning | 60 | 60 | |||||||
| pt 14 | 12 | absent | absent | mild | 3.0:1 | no | Total functioning | 87 | 64 |
| health functioning | 100 | 72 | |||||||
| emotional functioning | 90 | 55 | |||||||
| social functioning | 80 | 75 | |||||||
| school functioning | 70 | 50 | |||||||
| pt 15 | 7 | absent | daily | mild | 4.0:1 | no | Total functioning | 48 | NA |
| health functioning | 41 | NA | |||||||
| emotional functioning | 80 | NA | |||||||
| social functioning | 50 | NA | |||||||
| school functioning | 25 | NA | |||||||
| pt 16 | 4 | absent | less than monthly | NA | 3.0:1 | no | Total functioning | 64 | NA |
| health functioning | 60 | NA | |||||||
| emotional functioning | 65 | NA | |||||||
| social functioning | 60 | NA | |||||||
| school functioning | 50 | NA | |||||||
| pt 17 | 6 | less than monthly | daily | absent | 4.0:1 | no | Total functioning | 53 | 57 |
| health functioning | 41 | 44 | |||||||
| emotional functioning | 70 | 80 | |||||||
| social functioning | 65 | 60 | |||||||
| school functioning | 45 | 50 | |||||||
| Child Self Report | Parent Proxy Report | |||||||
|---|---|---|---|---|---|---|---|---|
| Age | KD Ratio | MD Frequency | ID | Age | KD Ratio | MD Frequency | ID | |
| Health/Physical Functioning | 0.81 | 0.31 | 0.68 | 0.61 | 0.36 | 0.09 | 0.046 | 0.19 |
| 1. Hard to walk more than a block | 0.84 | 0.2 | 0.76 | 0.79 | 0.35 | 0.47 | 0.15 | 0.68 |
| 2. Hard to run | 0.79 | 0.1 | 0.74 | 0.53 | 0.32 | 0.61 | 0.25 | 0.84 |
| 3. Hard to sports or exercise | 0.87 | 0.92 | 0.8 | 0.23 | 0.9 | 0.38 | 0.94 | 0.54 |
| 4. Hard to lift something heavy | 0.43 | 0.76 | 0.93 | 0.72 | 0.3 | 0.9 | 0.57 | 0.41 |
| 5. Hard to take a bath or shower | 0.63 | 0.11 | 0.56 | 0.27 | 0.35 | 0.12 | 0.88 | 0.13 |
| 6. Hard to chores around house | 0.98 | 0.73 | 0.33 | 0.01 | 0.62 | 0.55 | 0.44 | <0.009 |
| 7. Hurt or Ache | 0.83 | 0.39 | 0.66 | 0.77 | 0.22 | 0.009 | 0.95 | 0.70 |
| 8. Low energy | 0.19 | 0.63 | 0.69 | 0.16 | 0.94 | 0.2 | 0.41 | 0.44 |
| Emotional Functioning | 0.67 | 0.51 | 0.2 | 0.5 | 0.76 | 0.11 | 0.86 | 0.49 |
| 1. Feel afraid or scared | 0.92 | 0.57 | 0.60 | 0.84 | 0.99 | 0.51 | 0.55 | 0.29 |
| 2. Feel sad or blue | 0.12 | 0.74 | 0.91 | 0.96 | 0.28 | 0.49 | 0.22 | 0.67 |
| 3. Feel angry | 0.92 | 0.69 | 0.38 | 0.32 | 0.84 | 0.43 | 0.52 | 0.71 |
| 4. Trouble sleeping | 0.36 | 0.06 | 0.016 | 0.65 | 0.14 | 0.06 | 0.006 | 0.42 |
| 5. Worry about what will happen | 0.64 | 0.63 | 0.14 | 0.25 | 0.05 | 0.78 | 0.8 | 0.6 |
| Social Functioning | 0.14 | 0.57 | 0.72 | 0.08 | 0.08 | 0.32 | 0.38 | 0.045 |
| 1. Trouble getting along with peers | 0.23 | 0.58 | 0.84 | 0.23 | 0.02 | 0.47 | 0.75 | 0.08 |
| 2. Other kids not wanting to be friends | 0.14 | 0.3 | 0.44 | 0.23 | 0.11 | 0.78 | 0.5 | 0.02 |
| 3. Teased | 0.35 | 0.87 | 0.84 | 0.007 | 0.52 | 0.58 | 0.8 | 0.01 |
| 4. Doing things other peers do | 0.57 | 0.12 | 0.87 | 0.1 | 0.19 | 0.07 | 0.55 | 0.11 |
| 5. Hard to keep up when play with others | 0.3 | 0.09 | 0.79 | 0.28 | 0.62 | 0.32 | 0.97 | 0.17 |
| School Functioning | 0.92 | 0.13 | 0.15 | 0.41 | 0.62 | 0.16 | 0.002 | 0.2 |
| 1. Hard to concentrate | 0.94 | 0.026 | 0.42 | 0.42 | 0.71 | 0.031 | 0.29 | 0.056 |
| 2. Forget things | 0.69 | 0.84 | 0.87 | 0.87 | 0.82 | 0.35 | 0.53 | 0.05 |
| 3. Trouble keeping up school/work | 0.47 | 0.77 | 0.68 | 0.006 | 0.58 | 0.01 | 0.06 | 0.14 |
| 4. Miss school- Not well | 0.72 | 0.47 | 0.8 | 0.94 | 0.60 | 0.41 | 0.27 | 0.96 |
| 5. Miss school- Doctor appointement | 0.88 | 0.41 | 0.64 | 0.95 | 0.90 | 0.6 | <0.01 | 0.63 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varesio, C.; Pasca, L.; Parravicini, S.; Zanaboni, M.P.; Ballante, E.; Masnada, S.; Ferraris, C.; Bertoli, S.; Tagliabue, A.; Veggiotti, P.; et al. Quality of Life in Chronic Ketogenic Diet Treatment: The GLUT1DS Population Perspective. Nutrients 2019, 11, 1650. https://doi.org/10.3390/nu11071650
Varesio C, Pasca L, Parravicini S, Zanaboni MP, Ballante E, Masnada S, Ferraris C, Bertoli S, Tagliabue A, Veggiotti P, et al. Quality of Life in Chronic Ketogenic Diet Treatment: The GLUT1DS Population Perspective. Nutrients. 2019; 11(7):1650. https://doi.org/10.3390/nu11071650
Chicago/Turabian StyleVaresio, Costanza, Ludovica Pasca, Stefano Parravicini, Martina Paola Zanaboni, Elena Ballante, Silvia Masnada, Cinzia Ferraris, Simona Bertoli, Anna Tagliabue, Pierangelo Veggiotti, and et al. 2019. "Quality of Life in Chronic Ketogenic Diet Treatment: The GLUT1DS Population Perspective" Nutrients 11, no. 7: 1650. https://doi.org/10.3390/nu11071650