The Effects of a Low GI Diet on Cardiometabolic and Inflammatory Parameters in Patients with Type 2 and Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials

 ,
,
Abstract
:1. Introduction
- Evaluates the effect of a low GI diet on cardio-metabolic and inflammatory parameters in patients with type 2 diabetes and women with GDM.
2. Methods
2.1. Outcomes of Interest
- Cardio-metabolic parameters: total cholesterol (TC) mmol/L, low density lipoprotein (LDL) cholesterol mmol/L, high density lipoprotein (HDL) cholesterol mmol/L, and triglycerides (TG) mmol/L.
- Inflammatory parameters: C–reactive protein (CRP) mg/L, Adiponectin mg/L, and Interleukin–6 (IL-6) mg/L.
2.2. Search Terms and Search Strategy
2.3. Inclusion and Exclusion Criteria
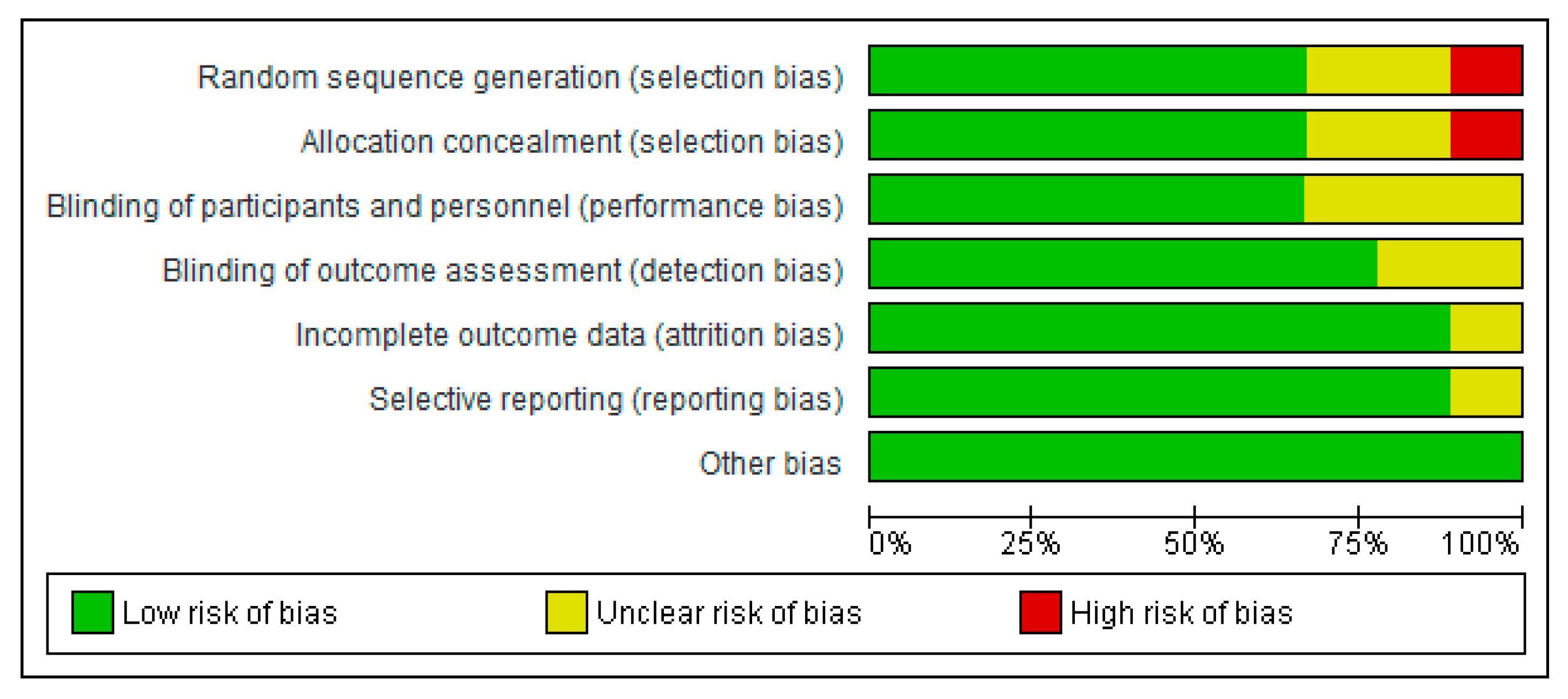
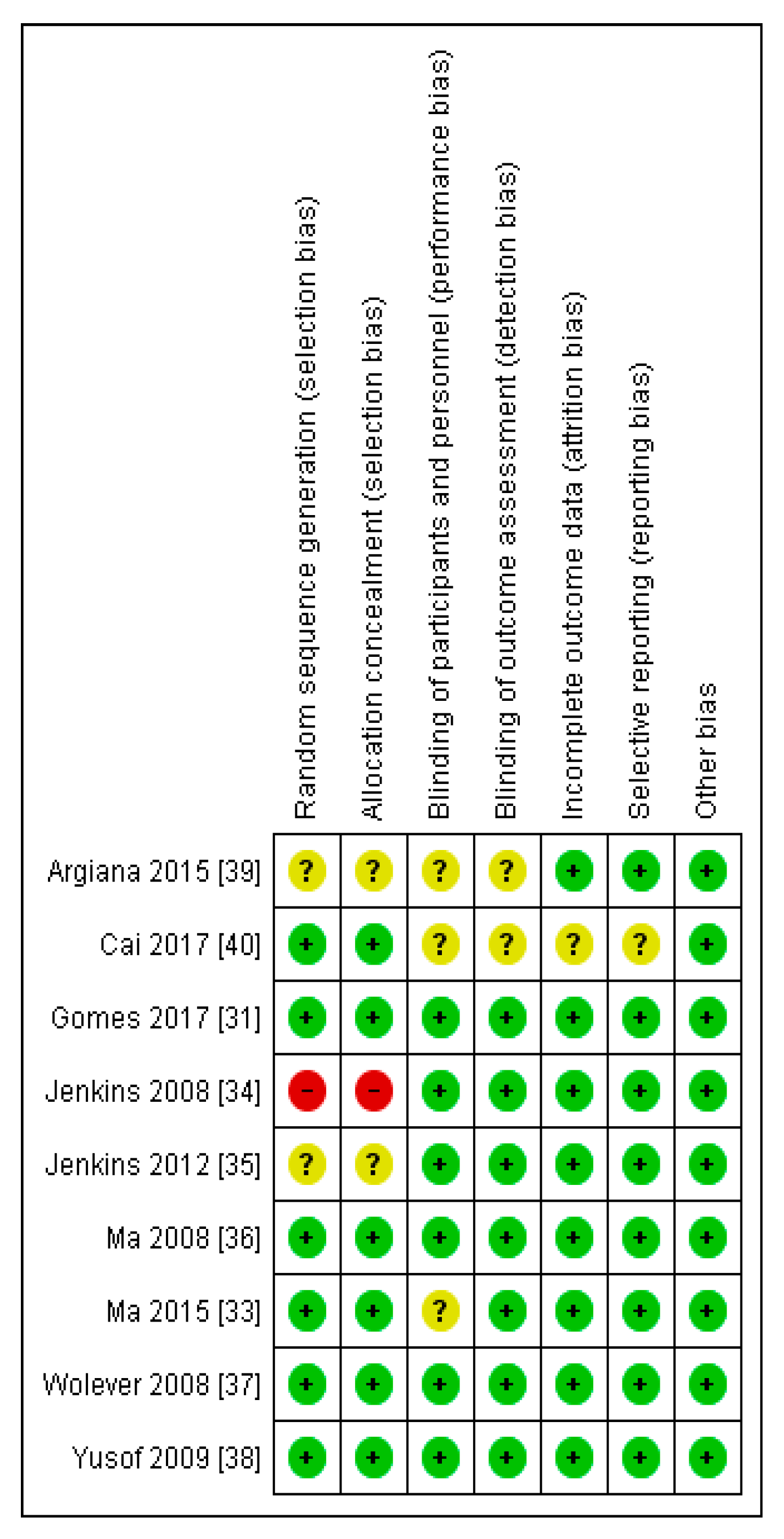
2.4. Quality Assessment and Risk of Bias of Included Studies
2.5. Data Extraction and Management
Statistical Analysis
2.6. Data Inclusion Decisions
3. Results
3.1. Evaluation of the Risk of Bias of the Studies Selected
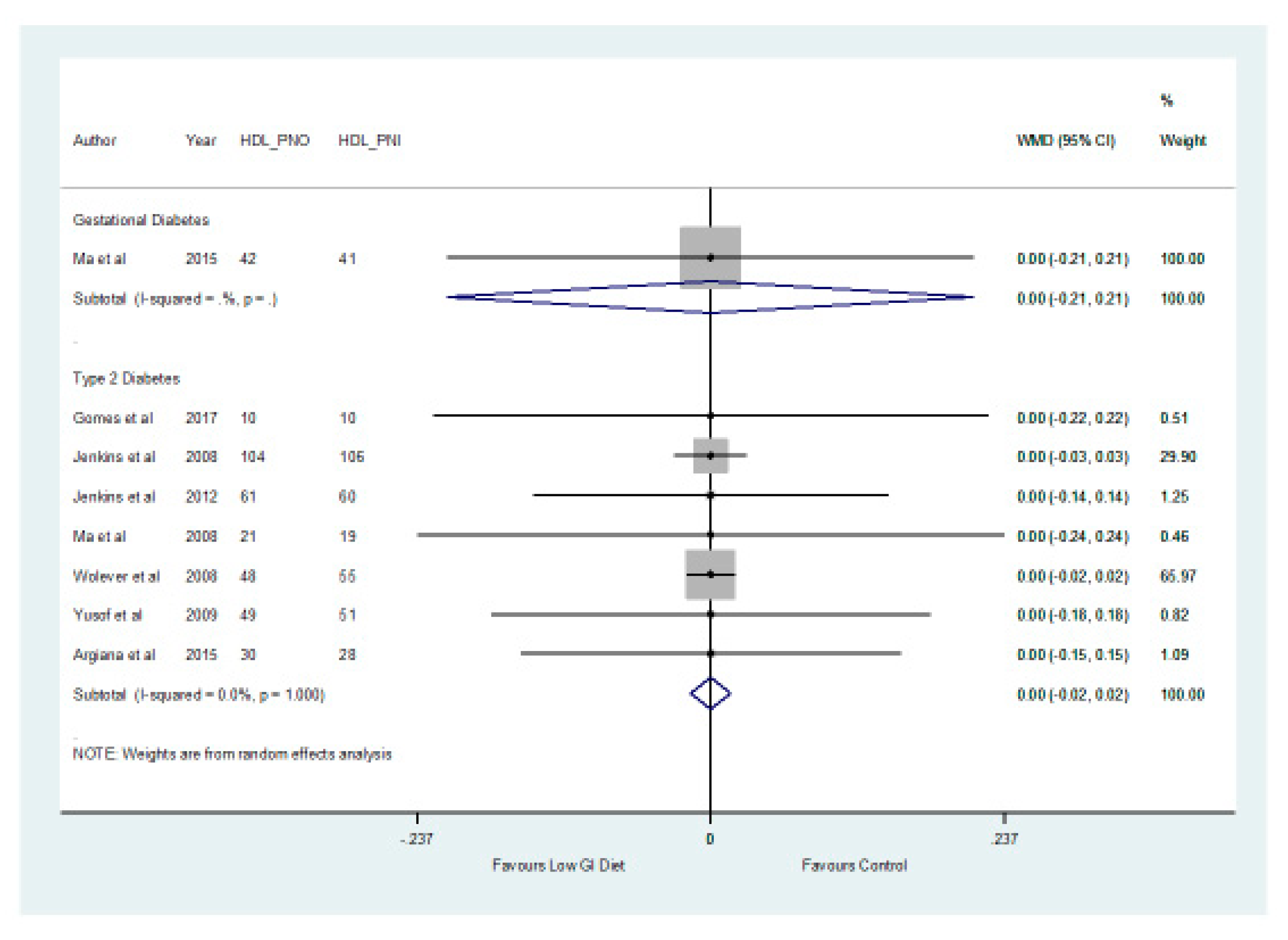
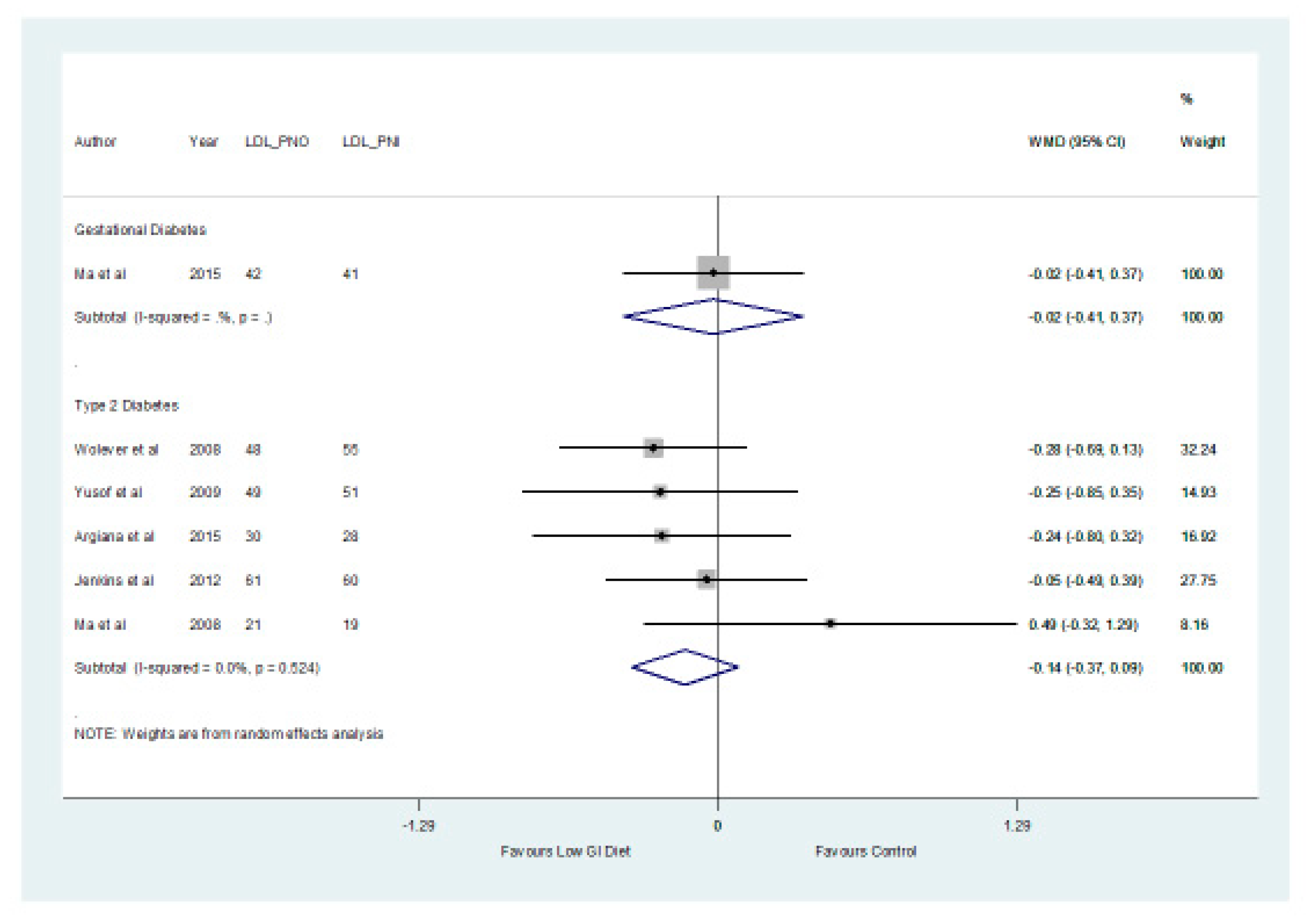
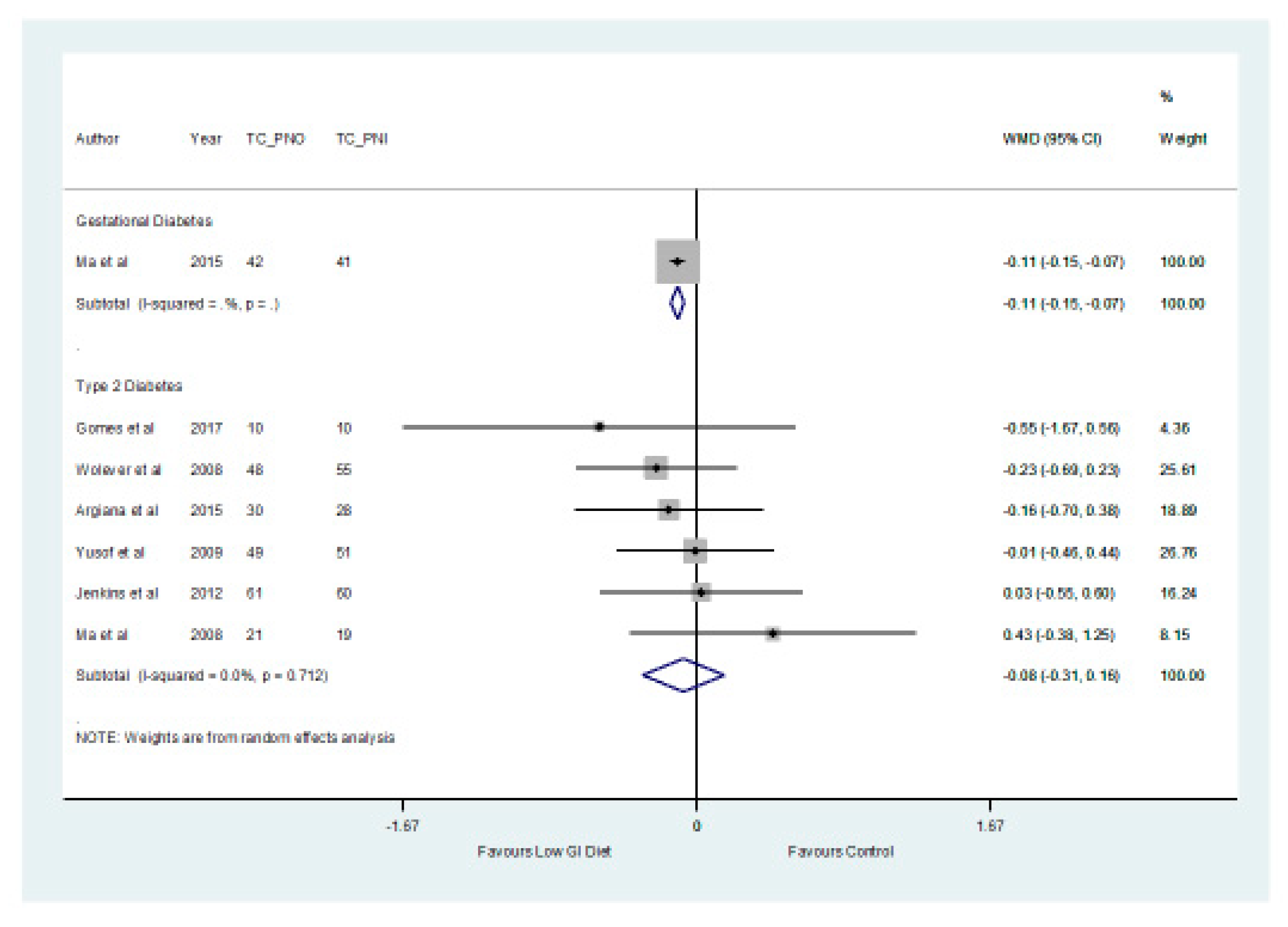
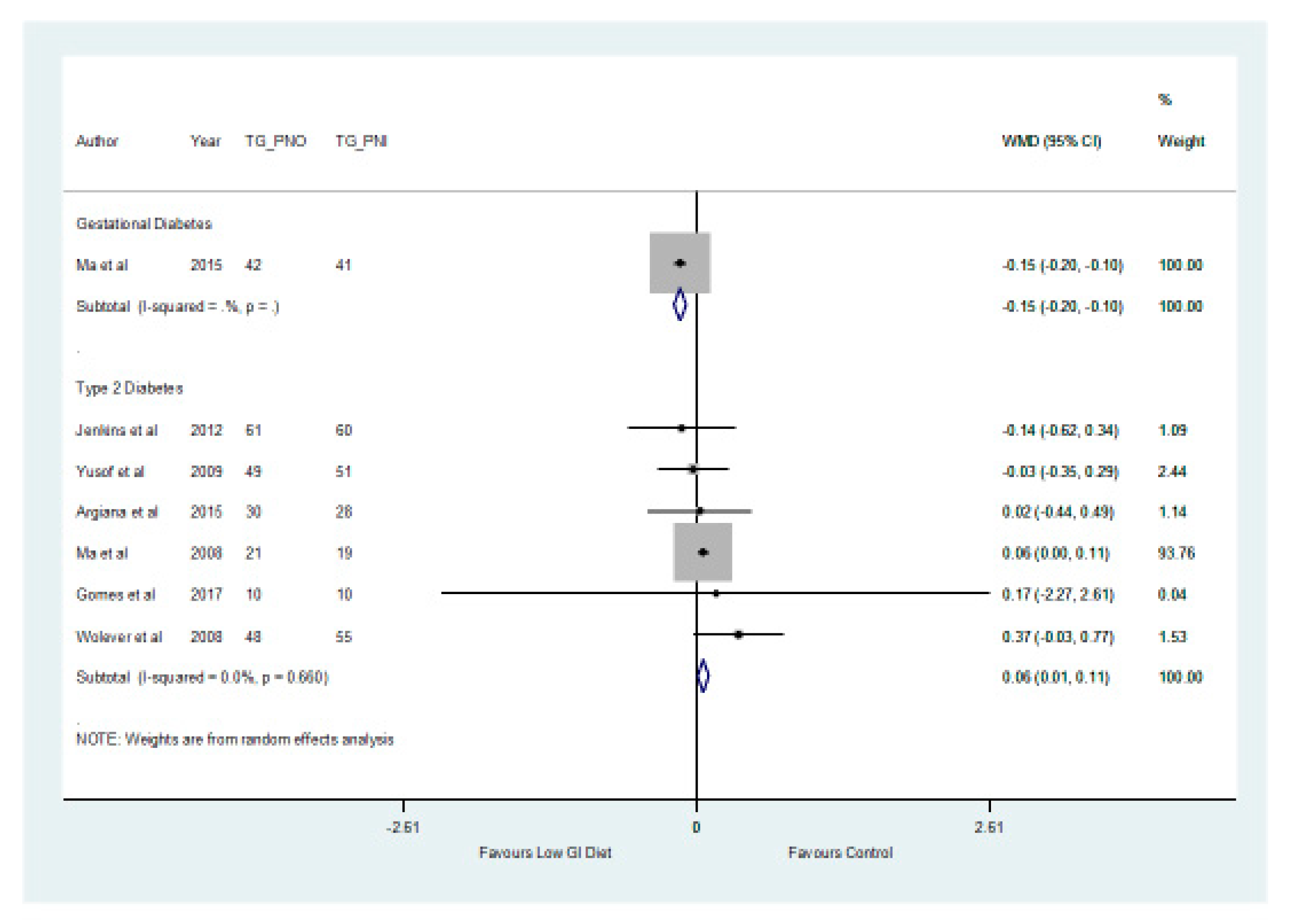
3.2. The Effect of a Low GI Diet on Lipid Profile
3.3. The Effect of a Low GI Diet on Inflammatory Parameters
4. Discussion
4.1. The Effect of a Low GI Diet on Lipid Profile
4.2. The Effect of a Low GI Diet on Inflammatory Parameters
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- International Diabetes Federation. Promoting Diabetes Care, Prevention and a Cure Worldwide. 2019. Available online: https://www.idf.org/ (accessed on 16 March 2019).
- National Collaborating Centre for Chronic Conditions (NCCCC). Type 2 Diabetes: National Clinical Guideline for Management in Primary and Secondary Care (Update); Royal College of Physicians: London, UK, 2008. [Google Scholar]
- Poulakos, P.; Mintziori, G.; Tsirou, E.; Taousani, E.; Savvaki, D.; Harizopoulou, V.; Goulis, D.G. Comments on gestational diabetes mellitus: From pathophysiology to clinical practice. Hormones (Athens, Greece) 2015, 14, 335–344. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy. 2013. Available online: http://apps.who.int/iris/bitstream/handle/10665/85975/WHO_NMH_MND_13.2_eng.pdf;jsessionid=09A82B923EF7A55CC6AB690976A1A1F3?sequence=1 (accessed on 16 March 2019).
- Abell, S.K.; De Courten, B.; Boyle, J.A.; Teede, H.J. Inflammatory and Other Biomarkers: Role in Pathophysiology and Prediction of Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2015, 16, 13442–13473. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. Care and Prevention Improving the Quality of Life of People with Diabetes and Those at Risk. 2019. Available online: https://www.idf.org/our-activities/care-prevention/gdm (accessed on 16 March 2019).
- National Institute for Health and Care Excellence (NICE). Type 2 Diabetes in Adults: Management. 2015. Available online: nice.org.uk/guidance/ng28 (accessed on 1 March 2019).
- National Institute for Health and Care Excellence (NICE). Diabetes in Pregnancy: Management from Preconception to the Postnatal Period. 2015. Available online: http://nice.org.uk/guidance/ng3 (accessed on 16 March 2018).
- Ojo, O.; Ojo, O.O.; Adebowale, F.; Wang, X.-H. The Effect of Dietary Glycaemic Index on Glycaemia in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2018, 10, 373. [Google Scholar] [CrossRef] [PubMed]
- Hodson, K.; Robson, S.; Taylor, R. Gestational diabetes: Emerging concepts in pathophysiology. Obstet. Med. 2010, 3, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Daher, S. Gestational diabetes, inflammation and obesity: New insights into genetic markers and phenotype. J. Reprod. Immunnol. 2012, 94, 6. [Google Scholar] [CrossRef]
- American Diabetes Association. Life style management: Standards of Medical Care in Diabetes–2018. Diabetes Care 2018, 41 (Suppl. 1), S38–S50. [Google Scholar] [CrossRef] [PubMed]
- Goff, L.M.; Cowland, D.E.; Hooper, L.; Frost, G.S. Low glycaemic index diets and blood lipids: A systematic review and meta-analysis of randomised controlled trials. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Similä, M.E.; Valsta, L.M.; Kontto, J.P.; Albanes, D.; Virtamo, J. Low-, medium-and high-glycaemic index carbohydrates and risk of type 2 diabetes in men. Br. J. Nutr. 2011, 105, 1258–1264. [Google Scholar] [CrossRef]
- Esfahani, A.; Wong, J.W.; Mirrahimi, A.; Villa, C.R.; Kendall, C.C. The application of the glycemic index and glycemic load in weight loss: A review of the clinical evidence. IUBMB Life 2011, 63, 7–13. [Google Scholar] [CrossRef]
- Food and Agricultural Organisation (FAO). Carbohydrates in Human Nutrition. Report of a Joint FAO/WHO Expert Consultation; FAO (Food and Nutrition paper–66); FAO: Rome, Italy, 1998; Available online: http://www.fao.org/docrep/w8079e/w8079e00.htm (accessed on 16 January 2019).
- Chiu, C.; Taylor, A. Dietary hyperglycemia, glycemic index and metabolic retinal diseases. Prog. Retin. Eye Res. 2011, 30, 18–53. [Google Scholar] [CrossRef] [Green Version]
- Chang, K.T.; Lampe, J.W.; Schwarz, Y.; Breymeyer, K.L.; Noar, K.A.; Song, X.; Neuhouser, M.L. Low Glycemic Load Experimental Diet More Satiating Than High Glycemic Load Diet. Nutr. Cancer 2012, 64, 666–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, W.R.; Baka, A.; Björck, I.; Delzenne, N.; Gao, D.; Griffiths, H.R.; Weickert, M.O. Impact of Diet Composition on Blood Glucose Regulation. Crit. Rev. Food Sci. Nutr. 2016, 56, 541–590. [Google Scholar] [CrossRef] [PubMed]
- Bouché, C.; Rizkalla, S.W.; Luo, J.; Vidal, H.; Veronese, A.; Pacher, N.; Fouquet, C.; Lang, V.; Slama, G. Five-week, low-glycemic index diet decreases total fat mass and improves plasma lipid profile in moderately overweight nondiabetic men. Diabetes Care 2002, 25, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Brand, J.C.; Colagiuri, S.; Crossman, S.; Allen, A.; Roberts, D.C.; Truswell, A.S. Low-glycemic index foods improve long-term glycemic control in NIDDM. Diabetes Care 1991, 14, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Clar, C.; Al-Khudairy, L.; Loveman, E.; Kelly, S.A.; Hartley, L.; Flowers, N.; Germanò, R.; Frost, G.; Rees, K. Low glycaemic index diets for the prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2017, 7, CD004467. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Long-term effects of low glycemic index/load vs. high glycemic index/load diets on parameters of obesity and obesity-associated risks: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. NMCD 2013, 23, 699–706. [Google Scholar] [CrossRef]
- Fleming, P.; Godwin, M. Low-glycaemic index diets in the management of blood lipids: A systematic review and meta-analysis. Fam. Pract. 2013, 30, 485–491. [Google Scholar] [CrossRef]
- Mendes, N.; Tavares Ribeiro, R.; Serrano, F. Beyond self-monitored plasma glucose and HbA1c: The role of non-traditional glycaemic markers in gestational diabetes mellitus. J. Obstet. Gynaecol. 2018, 38, 762–769. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme (CASP). Randomised Controlled Trial Checklist. 2017. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Randomised-Controlled-Trial-Checklist-2018.pdf (accessed on 18 January 2019).
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Hoboken, NJ, USA, 2009. [Google Scholar]
- The Nordic Cochrane Centre. Review Manager (RevMan) [Computer Program]; Version 5.3.; The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Denmark, 2014. [Google Scholar]
- Gomes, J.G.; Fabrini, S.P.; Alfenas, R.G. Low glycemic index diet reduces body fat and attenuates inflammatory and metabolic responses in patients with Type 2 diabetes. Arch. Endocrinol. Metab. 2017, 61, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.M.; Wolever, T.M.; O’Connor, D.L.; Nisenbaum, R.; Josse, R.G. Effect of a low glycaemic index diet on blood glucose in women with gestational hyperglycaemia. Diabetes Res. Clin. Pract. 2011, 91, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.J.; Huang, Z.H.; Huang, B.X.; Qi, B.H.; Zhang, Y.J.; Xiao, B.X.; Li, Y.H.; Chen, L.; Zhu, H.L. Intensive low-glycaemic-load dietary intervention for the management of glycaemia and serum lipids among women with gestational diabetes: A randomized control trial. Public Health Nutr. 2015, 18, 1506–1513. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.A.; Kendall, C.C.; McKeown-Eyssen, G.; Josse, R.G.; Silverberg, J.; Booth, G.L.; Leiter, L.A. Effect of a low-glycemic index or a high-cereal fiber diet on Type 2 diabetes: A randomized trial. JAMA 2008, 300, 2742–2753. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.A.; Kendall, C.C.; Augustin, L.A.; Mitchell, S.; Sahye-Pudaruth, S.; Blanco Mejia, S.; Josse, R.G. Effect of legumes as part of a low glycemic index diet on glycemic control and cardiovascular risk factors in type 2 diabetes mellitus: A randomized controlled trial. Arch. Intern. Med. 2012, 172, 1653–1660. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Olendzki, B.C.; Merriam, P.A.; Chiriboga, D.E.; Culver, A.L.; Li, W.; Pagoto, S.L. A randomized clinical trial comparing low-glycemic index versus ADA dietary education among individuals with type 2 diabetes. Nutrition 2008, 24, 45–56. [Google Scholar] [CrossRef]
- Wolever, T.; Gibbs, A.; Mehling, C.; Chiasson, J.; Connelly, P.; Josse, R.; Ryan, E. The Canadian Trial of Carbohydrates in Diabetes (CCD), a 1-y controlled trial of low-glycemic-index dietary carbohydrate in type 2 diabetes: No effect on glycated hemoglobin but reduction in C-reactive protein. Am. J. Clin. Nutr. 2008, 87, 114–125. [Google Scholar] [CrossRef] [PubMed]
- Yusof, B.M.; Talib, R.A.; Kamaruddin, N.A.; Karim, N.A.; Chinna, K.; Gilbertson, H. A low-GI diet is associated with a short-term improvement of glycaemic control in Asian patients with Type 2 diabetes. Diabetes Obes. Metab. 2009, 11, 387–396. [Google Scholar] [CrossRef]
- Argiana, V.; Kanellos, P.Τ.; Makrilakis, K.; Eleftheriadou, I.; Tsitsinakis, G.; Kokkinos, A.; Perrea, D.; Tentolouris, N. The effect of consumption of low-glycemic-index and low-glycemic-load desserts on anthropometric parameters and inflammatory markers in patients with Type 2 diabetes mellitus. Eur. J. Nutr. 2015, 54, 1173–1180. [Google Scholar] [CrossRef]
- Cai, X.; Wang, L.; Wang, X.; Liu, S. Effect of high dietary fiber low glycemic index diet on intestinal flora, blood glucose and inflammatory response in T2DM patients. Biomed. Res. 2017, 28, 9371–9375. [Google Scholar]
- Pelkman, C.L. Effects of the glycemic index of foods on serum concentrations of high-density lipoprotein cholesterol and triglycerides. Curr. Atheroscler. Rep. 2001, 3, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Huffman, F.G.; Zarini, G.G.; Cooper, V. Dietary glycemic index and load in relation to cardiovascular disease risk factors in Cuban American population. Int. J. Food Sci. Nutr. 2010, 61, 690–701. [Google Scholar] [CrossRef] [PubMed]
- Reaven, G.M. Pathophysiology of insulin resistance in human disease. Physiol. Rev. 1995, 75, 473–486. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, D.S. The glycemic index: Physiological mechanisms relating to obesity, diabetes, and cardiovascular disease. JAMA 2002, 287, 2414–2423. [Google Scholar] [CrossRef] [PubMed]
- Radulian, G.; Rusu, E.; Dragomir, A.; Posea, M. Metabolic effects of low glycaemic index diets. Nutr. J. 2009, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Aston, L.M. Glycaemic index and metabolic disease risk. Proc. Nutr. Soc. 2006, 65, 125–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devaraj, S.; Venugopal, S.K.; Singh, U.; Jialal, I. Hyperglycemia induces monocytic release of interleukin-6 via induction of protein kinase c-{alpha} and -{beta}. Diabetes 2005, 54, 85–91. [Google Scholar] [CrossRef]
- Leiter, L.A.; Ceriello, A.; Davidson, J.A.; Hanefeld, M.; Monnier, L.; Owens, D.R.; Tajima, N.; Tuomilehto, J. Postprandial glucose regulation: New data and new implications. Clin. Ther. 2005, 27 (Suppl. B), S42–S56. [Google Scholar] [CrossRef]
- Risso, A.; Mercuri, F.; Quagliaro, L.; Damante, G.; Ceriello, A. Intermittent high glucose enhances apoptosis in human umbilical vein endothelial cells in culture. Am. J. Physiol. Endocrinol. Metab. 2001, 281, E924–E930. [Google Scholar] [CrossRef]
- Juanola-Falgarona, M.; Salas-Salvado, J.; Ibarrola-Jurado, N.; Rabassa-Soler, A.; Diaz-Lopez, A.; Guasch-Ferré, M.; Hernández-Alonso, P.; Balanza, R.; Bullo, M. Effect of the glycemic index of the diet on weight loss, modulation of satiety, inflammation, and other metabolic risk factors: A randomized controlled trial. Am. J. Clin. Nutr. 2014, 100, 27–35. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Intervention | Comparator | Study Designs | Combining Search Terms |
|---|---|---|---|---|
| Patients with Diabetes | Low Glycemic Index (GI) Diet | Higher GI Diet | Randomised Controlled Trial | |
| Type 2 diabetes OR diabetes OR Patients with diabetes OR diabetes mellitus OR Gestational diabetes OR gestational diabetes mellitus (GDM) OR gestational diabetes mellitus OR diabetes mellitus, gestational OR diabetes in pregnancy | GI diet OR glycemic index OR Glycemic Index Numbers OR glycemic load OR Glycemic Indices OR Glycemic Index Number | #1 Controlled clinical trial OR Randomised controlled trial OR placebo OR randomized OR groups OR drug therapy OR randomly OR trial | Column 1 AND Column 2 AND Column 3 | |
| #2 “Animals” NOT “Humans” | ||||
| #3 #1 NOT #2 |
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Patients with gestational diabetes or patients with type 2 diabetes | Studies involving participants with type 1 diabetes and animal studies. Studies that include children that have diabetes or adults that are healthy. Pre-existing diabetes in patients who are pregnant |
| Intervention | Low GI diet | Studies involving dietary supplements |
| Comparator | higher GI diet | Studies involving additional supplements |
| Outcomes | Primary outcome measures of interest: Cardio-metabolic: total cholesterol, low density lipoprotein (LDL) cholesterol, high density lipoprotein (HDL) cholesterol, triglycerides. Secondary outcome measures of interest: Inflammatory parameters: C–reactive protein, Adiponectin and Interleukin–6 | Qualitative outcomes |
| Types of Study: Quantitative | Randomised controlled trials | Observational studies Letters Comments Reviews Editorials |
| Citation | Country | Type of Diabetes | Length of Study | Study Type | Age (Years) | Sample Size | Interventions/Glycemic Index (GI) Values | Results/Conclusion |
|---|---|---|---|---|---|---|---|---|
| Gomes et al. [31] | Brazil | Type 2 diabetes | 1 month | Parallel Design | 42.4 ± 5.1 | n = 20 | Low GI diet v. higher GI diet (Mean ± SD) Baseline Higher GI: 66 ± 4 Low GI: 63 ± 6 Post-intervention Higher GI: 72 ± 3 Low GI: 54 ± 4 | Serum non esterified fatty acid level increased in the higher GI group compared to the low GI group after intervention (p = 0.032). Low GI diet prevented the inflammatory responses induced by higher GI diet. |
| Grant et al. [32] | Canada | GDM | From 28 weeks gestation until delivery | Parallel Design | Higher GI: 34 ± 1.1 Low GI: 34 ± 0.1 | Low GI: n = 23 Higher GI: n = 24 | Higher GI v. Low GI (Mean ± SD) Higher GI: 58 ± 0.5 Low GI: 49 ± 0.8 | The difference between the low GI and higher GI groups in respect of lipids and CRP were not statistically significant (p > 0.05). |
| Ma et al. [33] | China | GDM | 12–14 Weeks | Parallel Design | Higher GI: 30.0 ± 3.5 Low GI: 30.1 ± 3.8 p = 0.901 | Higher GI: n = 42 Low GL: n = 41 | Higher GI v. Low GI (Mean ± SD) Baseline Higher GI: 56.1 ± 2.4 Low GI: 56.0 ± 2.1 Post-intervention Higher GI: 53.8 ± 2.5 Low GI: 50.1 ± 2.2 | The increases in TC, TG and the decrease in HDL cholesterol were significantly lower (p < 0.05) in the low GI group compared with the higher GI group. |
| Jenkins et al. [34] | Canada | Type 2 diabetes | 6 months | Parallel Design | (Mean ± SD) High-cereal fibre diet = 61 ± 9 Low-GI diet = 60 ± 10 | 210 | Low GI diet v. high-cereal fibre diet Mean (95% CI) Baseline Higher GI: 81.5 (80.4–82.7) Low GI: 80.8 (79.6–82.0) Post-intervention Higher GI: 83.5 (82.4–84.7) Low GI: 69.6 (67.7–71.4) | HDL cholesterol increased by 1.7 mg/dL in the low GI group and decreased by −0.2 mg/dL in the higher GI group (p = 0.005). Reductions of the CRP were similar in the low GI and higher GI groups. |
| Jenkins et al. [35] | Canada | Type 2 diabetes | 3 months | Parallel Design | (Mean±SEM) High-wheat fibre diet: 61 ± 1.0 Low-GI legume diet: 58 ± 1.3 | 121 | Low GI legume diet v. high-wheat fibre diet Mean (95% CI) Baseline Higher GI: 78 (77–80) Low GI: 80 (79–82) Post-intervention Higher GI: 82 (81–83) Low GI: 66 (64–67) | Low GI legume produced significant decreases in TC (p < 0.001) and TG (p < 0.001) with no significant change in HDL cholesterol (p = 0.19). The relative reduction in TC and HDL cholesterol were greater in the low GI legume diet group compared with the higher GI diet group. No other lipid treatment differences were significant. |
| Ma et al. [36] | USA | Type 2 diabetes | 12 months | Parallel Design | (Mean ± SD) 53.53 ± 8.40 | 40 | Low GI diet v. American Diabetes Association diet (ADA) (Mean ± SEM) Baseline ADA: 82.03 ± 1.31 Low GI: 79.35 ± 1.36 Post-intervention ADA: 80.36 ± 1.40 Low GI: 76.64 ± 1.46 | There were no significant differences between low GI and higher GI groups with respect to TC, HDL and TG. |
| Wolever et al. [37] | Canada | Type 2 diabetes | 12 months | Parallel Design | (Mean ± SEM) Higher GI diet: 60.4 ± 1.1 Low GI diet: 60.6 ± 1.0 | 162 | Low GI diet v. higher GI diet (Mean ± SEM) Baseline Higher GI: 61.5 ± 0.4 Low GI: 60.3 ± 0.4 Post-intervention Higher GI: 63.2 ± 0.4 Low GI: 55.1 ± 0.4 | There were no significant effects for TC. With the low GI diet, mean triacylglycerol was 12% higher, HDL was 4% lower, the higher GI values were intermediate. The CRP with the low GI diet was 29% less than the higher GI diet (p < 0.05). |
| Yusof et al. [38] | Malaysia | Type 2 diabetes | 12 weeks | Parallel Design | Not data | 104 | Low GI diet v. conventional carbohydrate exchange (CCE) (Mean ± SD) Baseline Higher GI: 64 ± 6 Low GI: 63 ± 5 Post-intervention Higher GI: 64 ± 5 Low GI: 57 ± 6 | TG increased at week 4, then decreased at week 12 in the Low GI group and this was reversed in the CCE group. Serum HDL cholesterol increased significantly in both groups over time, although no significant differences were found between the two groups. |
| Argiana et al. [39] | Greece | Type 2 diabetes | 12 weeks | Parallel Design | Control: 63.0 ± 1.3 Low GI: 61.3 ± 1.4 | n = 61 | Low GI diet v. Higher GI diet | The differences between the low GI diet and control diet with respect to HDL cholesterol at the end of the study was statistically significant (p = 0.007). A significant decrease (p = 0.02) in CRP was found in participants in the low GI diet group and the differences between the low GI and the higher GI groups were significant (p = 0.007) after the study. Serum IL–6 and adiponectin did not differ significantly in both groups at week 0 and week 12. |
| Cai et al. [40] | China | Type 2 diabetes | 12 months | Parallel Design | 56.7 ± 3.5 | n = 130 | Low GI diet v. Higher GI diet | After intervention, the levels of CRP-reactive protein and IL–6 in the low GI diet were significantly lower than the control group (p < 0.05). |
| Citation | Baseline Versus Post-Intervention | HDL Cholesterol | LDL Cholesterol | Total Cholesterol | Triglyceride | C–Reactive Protein | Adiponectin | Interleukin–6 |
|---|---|---|---|---|---|---|---|---|
| Gomes et al. [31] | Baseline mg/dL Median (Minimum/Maximum) Post-intervention | Higher GI: 43 (30/59) Low GI: 38 (27.6/45.2) Higher GI: 40 (30/54) Low GI: 41 (24.5/47) | No Data | Higher GI: 210.1 (180/273.5) Low GI: 200.4 (123/248.1) Higher GI: 211 (172/284) Low GI: 214.1 (145/288.5) | Higher GI: 180.2 (88.7/287) Low GI: 195 (68/372) Higher GI: 175.3 (132/311.2) Low GI: 205.1 (63/384.1) | (mg/L) Higher GI: 2.6 (0.8/7.3) Low GI: 2.7 (0.5/5.5) Higher GI: 2.8 (0.6/6.13) Low GI: 2.5 (0.1/6.9) p = 0.44 | ng/mL Higher GI: 30.9 (29.8/31.4 Low GI: 30.1 (29.4/31.3) Higher GI: 30.8 (30.2/31.6) Low GI: 30.5 (26.7/93) p = 0.74 | No Data |
| Ma et al. [33] | Baseline mmol/L (Mean ± SD) Post-intervention | Higher GI: 1.96 ± 0.39 Low GI: 1.89 ± 0.33 Higher GI: 1.85 ± 0.36 Low GI: 1.87 ± 0.34 | Higher GI: 2.13 ± 0.60 Low GI: 2.19 ± 0.58 Higher GI: 2.16 ± 0.81 Low GI: 2.20 ± 0.54 | Higher GI: 5.74 ± 0.74 Low GL: 5.79 ± 1.01 Higher GI: 5.97 ± 0.89 Low GI: 5.96 ± 1.02 | Higher GI: 2.20 ± 0.60 Low GI:2.67 ± 1.27 Higher GI: 3.14 ± 1.05 Low GI: 3.09 ± 1.14 | No Data | No Data | No Data |
| Jenkins et al. [34] | Baseline mg/dL (Mean) Post-intervention | Higher GI: 43.1 Low GI: 41.9 Higher GI: 42.8 Low GI: 43.6 | Higher GI: 101.1 Low GI: 96.9 Higher GI: 101.3 Low GI: 95.3 | Higher GI: 168.4 Low GI: 164.3 Higher GI: 168.4 Low GI: 162.6 | Higher GI: 122.0 Low GI: 128.1 Higher GI: 122.2 Low GI: 124.6 | Higher GI: 4.59 Low GI: 4.62 Higher GI: 2.82 Low GI: 3.02 | No Data | No Data |
| Jenkins et al. [35] | Baseline mg/dL (95% CI) Post-intervention | Higher GI: 47 (44, 50) Low GI: 43 (40, 46) Higher GI: 48 (45, 52) Low GI: 43 (40, 45) | Higher GI: 91 (81, 101) Low GI: 84 (77, 92) Higher GI: 90 (81, 99) Low GI: 81 (74, 89) | Higher GI: 163 (151, 174) Low GI: 158 (147, 168) Higher GI: 161 (150, 172) Low GI: 149 (139, 160) | Higher GI: 124 (104, 145) Low GI: 149 (125, 173) Higher GI: 115 (96, 133) Low GI: 128 (107, 148) | No Data | No Data | No Data |
| Ma et al. [36] | Baseline mg/dL (Mean ± SEM) Post-intervention | Higher GI: 42.95 ± 2.26 Low GI: 45.42 ± 2.38 Higher GI: 44.29 ± 2.30 Low GI: 47.53 ± 2.43 | Higher GI: 88.95 ± 7.52 Low GI: 93.16 ± 8.07 Higher GI: 71.49 ± 7.81 Low GI: 94.50 ± 8.32 | Higher GI: 168.10 ± 9.06 Low GI: 175.58 ± 9.53 Higher GI: 149.71 ± 9.35 Low GI: 173.63 ± 0.06 p = 0.09 | * Higher GI: 5.05 (0.14) Low GI: 4.99 (0.15) Higher GI: 4.93 (0.15) Low GI: 4.90 (0.16) | No Data | No Data | No Data |
| Wolever et al. [37] | Baseline mmol/L (Mean ± SEM) Post-intervention | Higher GI: 1.14 ± 0.05 Low GI: 1.21 ± 0.03 Higher GI: 1.19 ± 0.03 Low GI: 1.16 ± 0.03 | Higher GI: 2.82 ± 0.13 Low GI: 3.02 ± 0.13 Higher GI: 3.0 ± 0.08 Low GI: 2.92 ± 0.05 | Higher GI: 4.86 ± 0.16 Low GI: 5.09 ± 0.13 Higher GI: 5.04 ± 0.08 Low GI: 5.04 ± 0.08 | Higher GI: 2.07 ± 0.15 Low GI: 1.87 ± 0.10 Higher GI: 2.0 ± 0.07 Low GI: 2.17 ± 0.07 | ** Higher GI: 3.34 (2.56, 4.26) Low GI: 2.64 (1.89, 3.70) Higher GI: 2.75 (2.33, 3.24) Low GI: 1.95 (1.68, 2.27) | No Data | No Data |
| Yusof et al. [38] | Baseline mmol/L (Mean ± SEM) Post-intervention | Higher GI: 1.18 ± 0.34 Low GI: 1.08 ± 0.30 Higher GI: 1.21 ± 0.05 Low GI: 1.14 ± 0.04 | Higher GI: 2.78 ± 0.67 Low GI: 2.78 ± 0.67 Higher GI: 2.93 ± 0.14 Low GI: 2.67 ± 0.11 | Higher GI: 4.56 ± 0.80 Low GI: 4.54 ± 0.75 Higher GI: 4.80 ± 0.16 Low GI: 4.54 ± 0.12 | Higher GI: 1.35 ± 0.53 Low GI: 1.5 ± 0.47 Higher GI: 1.46 ± 0.08 Low GI: 1.59 ± 0.10 | No Data | No Data | No Data |
| Argiana et al. [39] | Baseline mg/dL (Mean ± SEM) Post-intervention | Higher GI: 46.4 ± 1.8 Low GI: 43.1 ± 1.3 Higher GI: 46.1 ± 1.7 Low GI: 43.3 ± 1.2 | Higher GI: 104.9 ± 5.1 Low GI: 107.0 ± 5.5 Higher GI: 104.2 ± 5.2 Low GI: 97.2 ± 6.2 | Higher GI: 176.6 ± 5.2 Low GI: 173.9 ± 6.4 Higher GI: 175.8 ± 5.2 Low GI: 167.0 ± 4.1 | Higher GI: 126.5 ± 10.8 Low GI: 119.2 ± 11.6 Higher GI: 127.5 ± 10.3 Low GI: 122 ± 9.3 | *** Higher GI: 2.1 ± 0.5 Low GI: 4.4 ± 1.2 Higher GI: 2.8 ± 0.6 Low GI: 3.0 ± 0.8 | *** Higher GI: 7.4 ± 1.6 Low GI: 12.2 ± 3.4 Higher GI: 8.3 ± 2.1 Low GI: 12.5 ± 1.5 | **** Higher GI: 1.3 ± 0.2 Low GI: 1.4 ± 0.3 Higher GI: 2.0 ± 0.5 Low GI: 1.3 ± 0.2 |
| Cai et al. [40] | Baseline mg/L (Not stated whether Mean or SD) Post-intervention | No Data | No Data | No Data | No Data | Higher GI: 8.03 ± 0.72 Low GI: 8.04 ± 0.75 Higher GI: 5.01 ± 0.32 Low GI: 3.68 ± 0.29 | No Data | **** Higher GI: 12.26 ± 1.57 Low GI: 12.29 ± 1.44 Higher GI: 9.01 ± 0.83 Low GI: 7.97 ± 0.86 |
| Outcomes | Patients with Type 2 Diabetes | |||
|---|---|---|---|---|
| N Studies | Weighted Mean Difference (95% CI) mg/L | p-Value | I2 % | |
| Interleukin–6 | 2 | −1.01 (−1.55, −0.48) | 0.001 | 0.0 |
| C–eactive Protein | 5 | −0.32 (−1.17, 0.53) | 0.467 | 0.0 |
| Adiponectin | 2 | 0.01 (−0.00, 0.03) | 0.072 | 0.0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ojo, O.; Ojo, O.O.; Wang, X.-H.; Adegboye, A.R.A. The Effects of a Low GI Diet on Cardiometabolic and Inflammatory Parameters in Patients with Type 2 and Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients 2019, 11, 1584. https://doi.org/10.3390/nu11071584
Ojo O, Ojo OO, Wang X-H, Adegboye ARA. The Effects of a Low GI Diet on Cardiometabolic and Inflammatory Parameters in Patients with Type 2 and Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients. 2019; 11(7):1584. https://doi.org/10.3390/nu11071584
Chicago/Turabian StyleOjo, Omorogieva, Osarhumwese Osaretin Ojo, Xiao-Hua Wang, and Amanda Rodrigues Amorim Adegboye. 2019. "The Effects of a Low GI Diet on Cardiometabolic and Inflammatory Parameters in Patients with Type 2 and Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials" Nutrients 11, no. 7: 1584. https://doi.org/10.3390/nu11071584