Effect of Ramadan Fasting on Weight and Body Composition in Healthy Non-Athlete Adults: A Systematic Review and Meta-Analysis

 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Screening of Publications
2.4. Data Extraction and Organization
2.5. Analyses and Subgroups
2.6. Data processing, Meta-Analyses, and Meta-Regressions
3. Results
3.1. Weight Changes
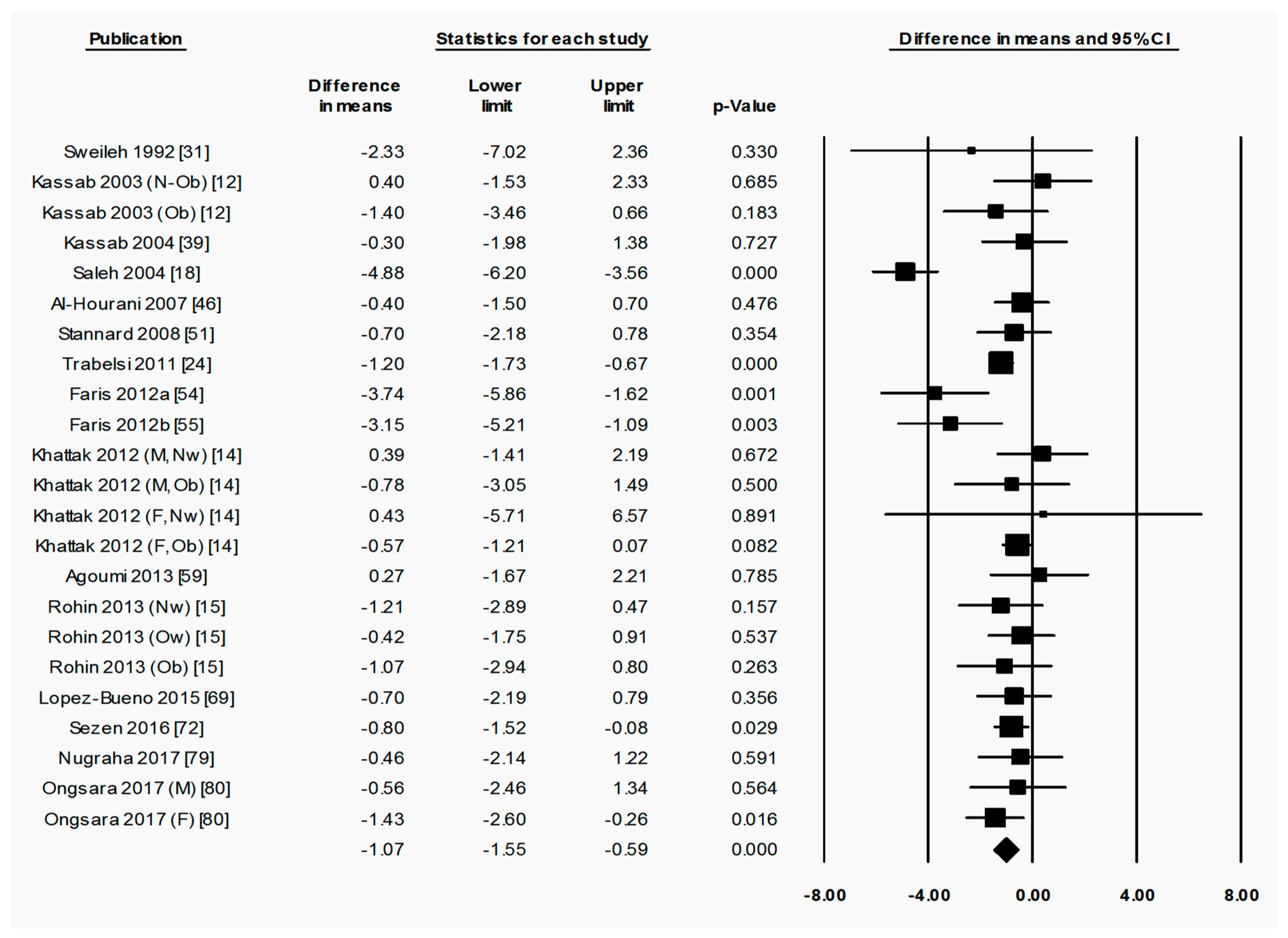
3.1.1. Ramadan Fasting Promoted a Transient Reduction in Weight
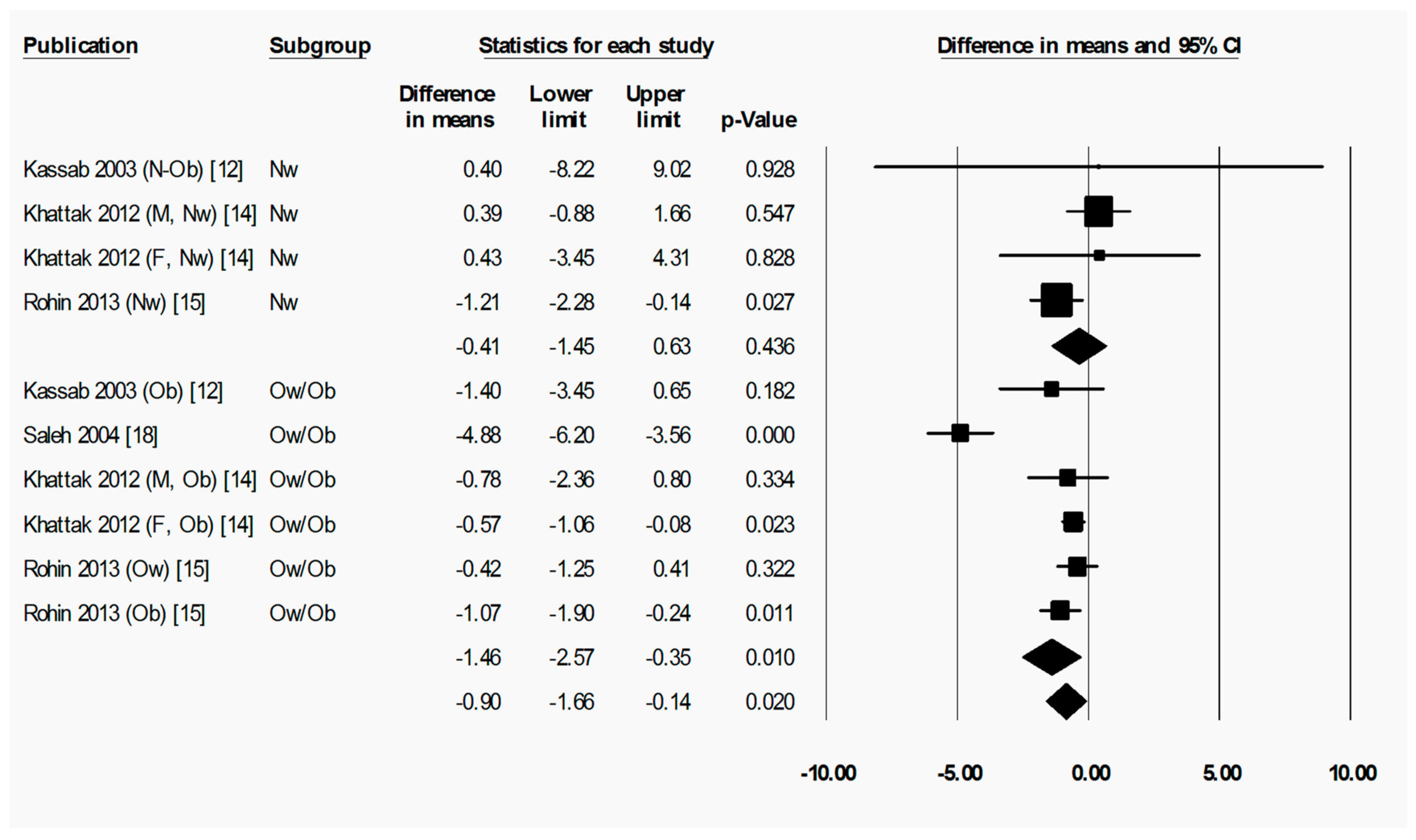
3.1.2. Starting BMI may have Influenced Weight Changes in Response to Ramadan Fasting
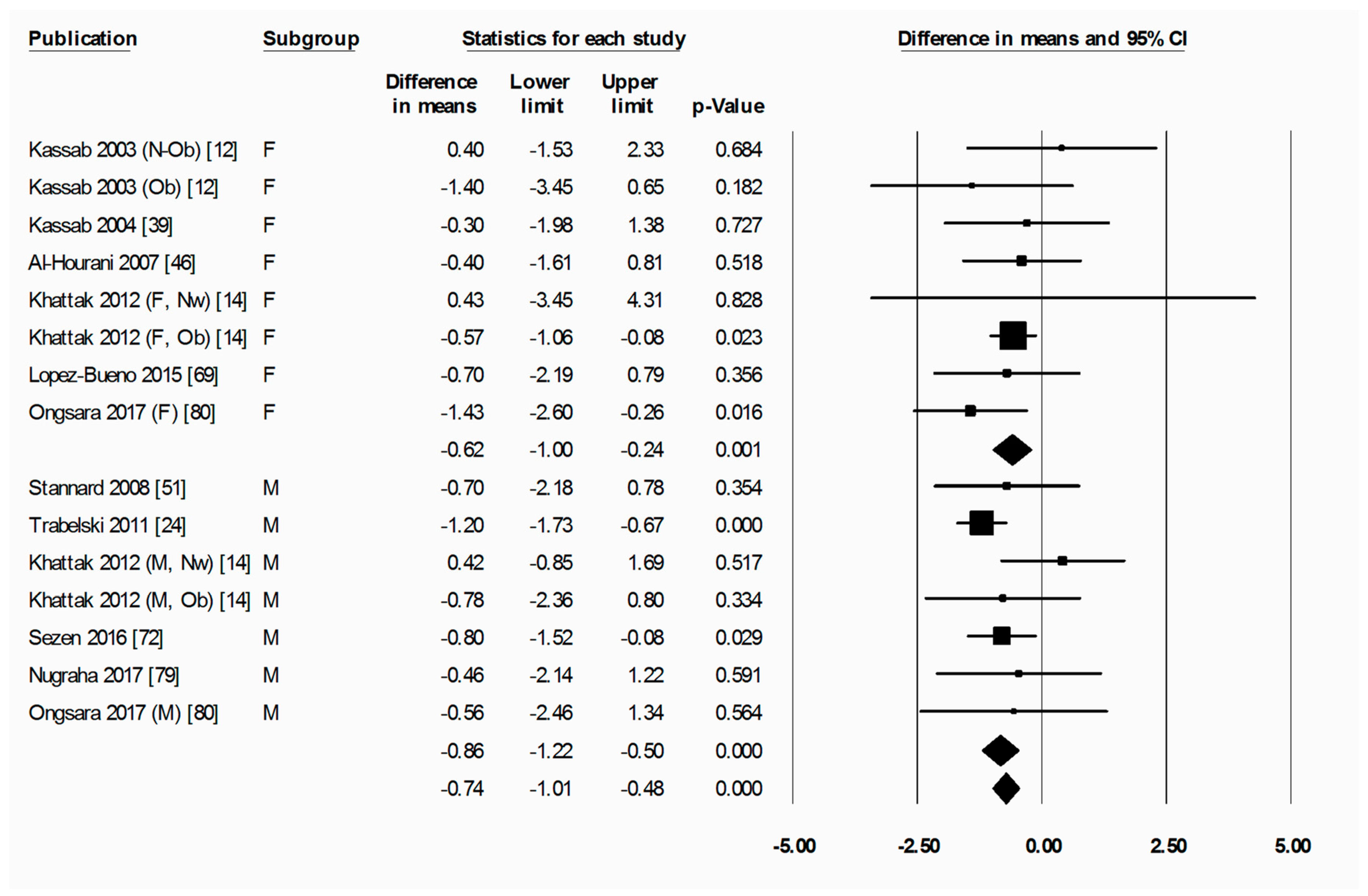
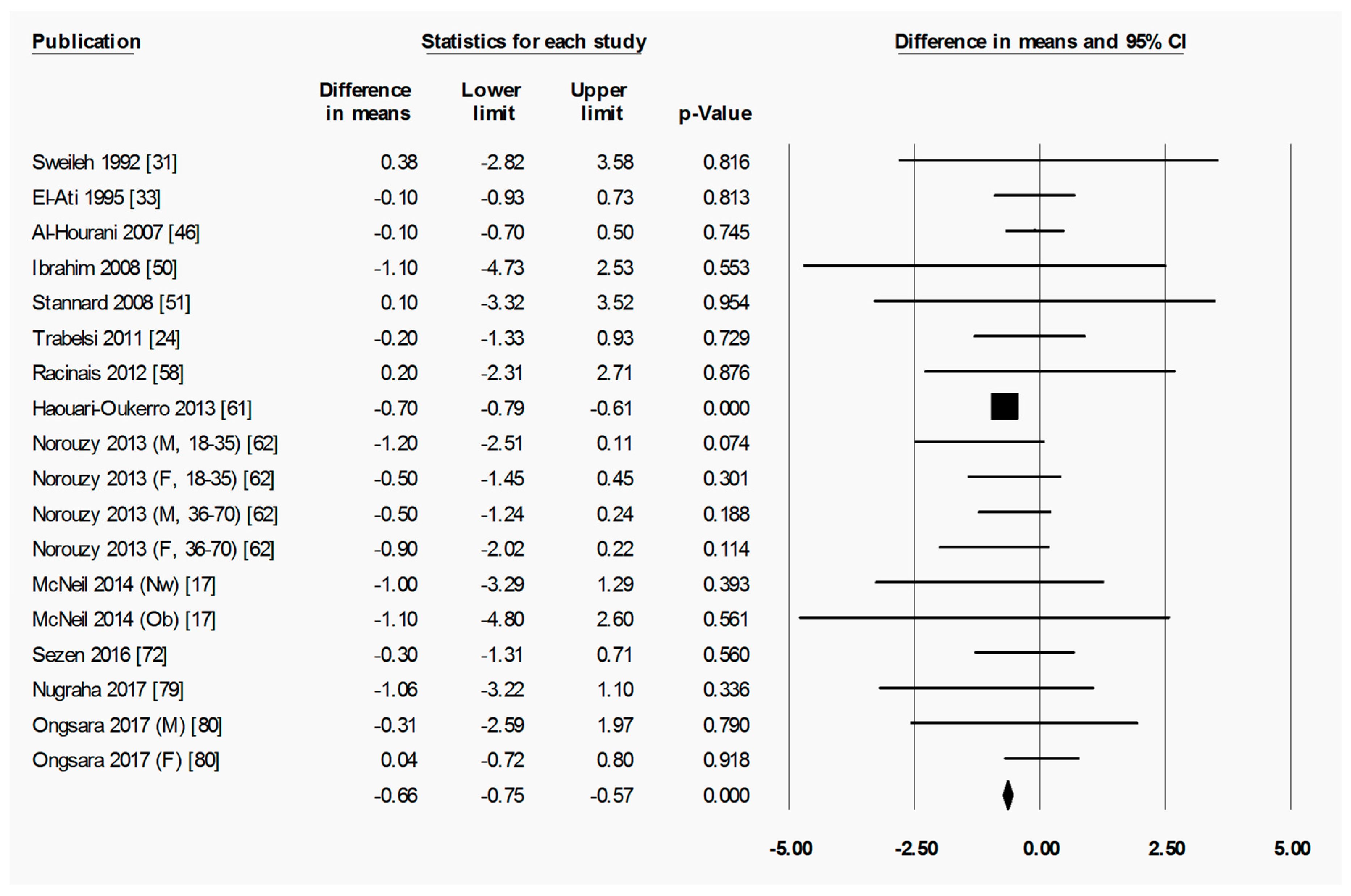
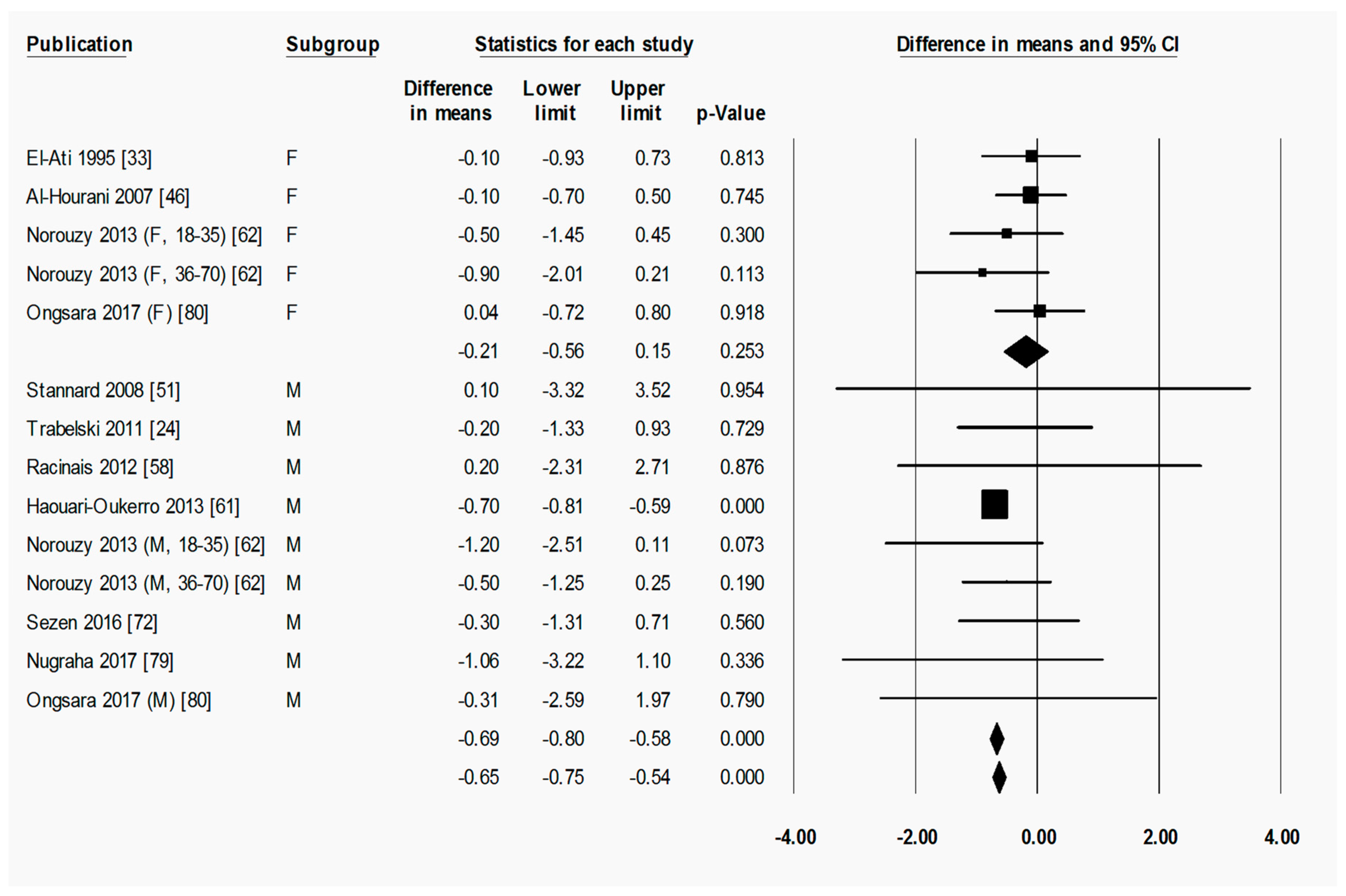
3.1.3. Sex did not Influence Weight Changes in Response to Ramadan Fasting
3.1.4. Location may have Influenced Weight Change in response to Ramadan Fasting
3.2. Body Composition Changes
3.2.1. Ramadan Fasting Promoted a Transient Reduction in Fat Mass as a Percentage of Weight
3.2.2. Ramadan Fasting Promoted a Transient Reduction in Absolute Fat Mass
3.2.3. Ramadan Fasting Promoted a Transient Reduction in Fat-Free Mass
3.3. Physical Activity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kettani, H. World Muslim Population: 1950–2020. Int. J. Environ. Sci. Technol. 2010, 1, 154–164. [Google Scholar]
- Sakr, A.H. Fasting in Islam. J. Am. Diet. Assoc. 1975, 67, 17–21. [Google Scholar] [PubMed]
- Trepanawski, J.F.; Bloomer, R.J. The impact of religious fasting on human health. Nutr. J. 2010, 9, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azizi, F. Islamic Fasting and Health. Ann. Nutr. Metab. 2010, 56, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Sadeghirad, B.; Motaghipisheh, S.; Kolahdooz, F.; Zahedi, M.J. Islamic fasting and weight loss: A systematic review and meta-analysis. Public Health Nutr. 2014, 17, 396–406. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, J.M.; Barac-Nieto, M. Cardio-respiratory responses to moderately heavy aerobic exercise during the Ramadan fasts. Saudi Med. J. 2000, 21, 238–244. [Google Scholar] [PubMed]
- Bigard, A.X.; Boussif, M.; Chalabi, H.; Guezennec, C.Y. Alterations in muscular performance and orthostatic tolerance during Ramadan. Aviat. Space Environ. Med. 1998, 69, 341–346. [Google Scholar] [PubMed]
- Roky, R.; Houti, I.; Moussamih, S.; Qotbi, S.; Aadil, N. Physiological and Chronobiological Changes during Ramadan Intermittent Fasting. Ann. Nutr. Metab. 2004, 48, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Kahan, D. Prevalence and correlates of adult overweight in the Muslim world: Analysis of 46 countries. Clin. Obes. 2015, 5, 87–98. [Google Scholar] [CrossRef] [PubMed]
- The GBD 2015 Obesity Collaborators. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takruri, H.R. Effect of fasting in Ramadan on body weight. Saudi Med. J. 1989, 10, 491–494. [Google Scholar]
- Kassab, S.; Abdul-Ghaffar, T.; Nagalla, D.S.; Sachdeva, U.; Nayar, U. Serum leptin and insulin levels during chronic diurnal fasting. Asia Pac. J. Clin. Nutr. 2003, 12, 483–487. [Google Scholar] [PubMed]
- Ünalacak, M.; Kara, I.H.; Baltaci, D.; Erdem, Ö.; Bucaktepe, P.G.E. Effects of ramadan fasting on biochemical and hematological parameters and cytokines in healthy and obese individuals. Metab. Syndr. Relat. Disord. 2011, 9, 157–161. [Google Scholar]
- Ali Khan Khattak, M.M.; Bakar, I.A.; Yeim, L. Does religious fasting increase fat free mass (FFM) and reduce abdominal obesity? J. Nutr. Food Sci. 2012, 42, 87–96. [Google Scholar] [CrossRef]
- Rohin, M.A.K.; Rozano, N.; Hadi, N.A.; Nor, M.N.M.; Abdullah, S.; Venkateshaiah, M.D. Anthropometry and body composition status during ramadan among higher institution learning centre staffs with different body weight status. Sci. World J. 2013, 2013, 308041. [Google Scholar] [CrossRef] [PubMed]
- Celik, A.; Saricicek, E.; Saricicek, V.; Sahin, E.; Ozdemir, G.; Bozkurt, S.; Okumus, M.; Sucakli, M.H.; Cikim, G.; Coskun, Y.; et al. Effect of Ramadan fasting on serum concentration of apelin-13 and new obesity indices in healthy adult men. Med. Sci. Monit. 2014, 20, 337–342. [Google Scholar] [PubMed] [Green Version]
- McNeil, J.; Mamlouk, M.M.; Duval, K.; Schwartz, A.; Nardo Junior, N.; Doucet, E. Alterations in metabolic profile occur in normal-weight and obese men during the Ramadan fast despite no changes in anthropometry. J. Obes. 2014, 2014, 482547. [Google Scholar] [CrossRef] [PubMed]
- Saleh, S.A.; El-Kemery, T.A.; Farrag, K.A.; Badawy, M.R.; Sarkis, N.N.; Soliman, F.S.; Mangoud, H. Ramadan fasting: Relation to atherogenic risk among obese Muslims. J. Egypt. Public Health Assoc. 2004, 79, 461–483. [Google Scholar] [PubMed]
- Haouari, M.; Haouari-oukerro, F.; Sfaxi, A.; Rayana, M.B.; Kaabachi, N.; Mbazaa, A. How Ramadan fasting affects caloric consumption, body weight and circadian evolution of cortisol serum levels in young, healthy male volunteers. Horm. Metab. Res. 2008, 40, 575–577. [Google Scholar] [CrossRef] [PubMed]
- Lamri-Senhadji, M.Y.; El Kebir, B.; Belleville, J.; Bouchenak, M. Assessment of dietary consumption and time-course of changes in serum lipids and lipoproteins before, during and after Ramadan in young Algerian adults. Singap. Med. J. 2009, 50, 288–294. [Google Scholar]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Cllaboration: London, UK, 2011. [Google Scholar]
- Dewanti, L.; Watanabe, C.; Ohtsuka, R. Unexpected changes in blood pressure and hematological parameters among fasting and nonfasting workers during Ramadan in Indonesia. Eur. J. Clin. Nutr. 2006, 60, 877–881. [Google Scholar] [CrossRef] [PubMed]
- Ziaee, V.; Razaei, M.; Ahmadinejad, Z.; Shaikh, H.; Yousefi, R.; Yarmohammadi, L.; Bozorgi, F.; Behjati, M.J. The changes of metabolic profile and weight during Ramadan fasting. Singap. Med. J. 2006, 47, 409–414. [Google Scholar]
- Trabelsi, K.; El Abed, K.; Trepanowski, J.F.; Stannard, S.R.; Ghlissi, Z.; Ghozzi, H.; Masmoudi, L.; Jammoussi, K.; Hakim, A. Effects of Ramadan fasting on biochemical and anthropometric parameters in physically active men. (Special issue on Ramadan fasting.). Asian J. Sports Med. 2011, 2, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.B.; Isawumi, M.A. Effects of fasting on intraocular pressure in a black population. Middle East Afr. J. Ophthalmol. 2014, 21, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Syam, A.F.; Sobur, C.S.; Abdullah, M.; Makmun, D. Ramadan fasting decreases body fat but not protein mass. Int. J. Endocrinol. Metab. 2016, 14, e29687. [Google Scholar]
- Sunrise and Sunset Calculator—City Lookup 2017. Available online: https://www.timeanddate.com (accessed on 16 June 2018).
- Fedail, S.S.; Murphy, D.; Salih, S.Y. Changes in certain blood constituents during Ramadan. Am. J. Clin. Nutr. 1982, 36, 350–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husain, R.; Duncan, M.T.; Cheah, S.H.; Ch’ng, S.L. Effects of fasting in Ramadan on Tropical Asiatic Moslems. Br. J. Nutr. 1987, 58, 41–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azizi, F.; Rasouli, H.A. Serum glucose, bilirubin, calcium, phosphorus, protein and albumin concentrations during Ramadan. Med. J. Islam. Repub. Iran 1992, 6 (Suppl. S3), 43–46. [Google Scholar]
- Sweileh, N.; Schnitzler, A.; Hunter, G.R.; Davis, B. Body composition and energy metabolism in resting and exercising muslims during Ramadan fast. J. Sports Med. Phys. Fitness 1992, 32, 156–163. [Google Scholar] [PubMed]
- Maislos, M.; Khamaysi, N.; Assali, A.; Abou-Rabiah, Y.; Zvili, I.; Shany, S. Marked increase in plasma high-density-lipoprotein cholesterol after prolonged fasting during Ramadan. Am. J. Clin. Nutr. 1993, 57, 640–642. [Google Scholar] [CrossRef] [PubMed]
- El-Ati, J.; Beji, C.; Danguir, J. Increased fat oxidation during Ramadan fasting in healthy women: An adaptative mechanism for body-weight maintenance. Am. J. Clin. Nutr. 1995, 62, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Adlouni, A.; Ghalim, N.; Saile, R.; Had, N.; Parra, H.J.; Benslimane, A. Beneficial effect on serum apo AI, apo B and Lp AI levels of Ramadan fasting. Clin. Chim. Acta 1998, 271, 179–189. [Google Scholar] [CrossRef]
- Bilto, Y.Y. Effects of Ramadan fasting on body weight and the biochemical and haematological parameters of the blood. Arab Gulf J. Sci. Res. 1998, 16, 1–13. [Google Scholar]
- Finch, G.M.; Day, J.E.L.; Welch, D.A.; Rogers, P.J. Appetite changes under free-living conditions during Ramadan fasting. Appetite 1998, 31, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Kayikçioǧlu, Ö.; Erkin, E.F.; Erakgün, T. The influence of religious fasting on basal tear secretion and tear break-up time. Int. Ophthalmol. 1998, 22, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Fakhrzadeh, H.; Larijani, B.; Sanjari, M.; Baradar-Jalili, R.; Amini, M.R. Effect of Ramadan fasting on clinical and biochemical parameters in healthy adults. Ann. Saudi Med. 2003, 23, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Kassab, S.E.; Abdul-Ghaffar, T.; Nagalla, D.S.; Sachdeva, U.; Nayar, U. Interactions between leptin, neuropeptide-Y and insulin with chronic diurnal fasting during Ramadan. Ann. Saudi Med. 2004, 24, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Rashid, M.; Basher, S.; Sultana, S.; Nomani, M.Z.A. Improved serum HDL cholesterol profile among Bangladeshi male students during Ramadan fasting. East. Mediterr. Health J. 2004, 10, 131–137. [Google Scholar] [PubMed]
- Yucel, A.; Degirmenci, B.; Acar, M.; Albayrak, R.; Haktanir, A. The effect of fasting month of Ramadan on the abdominal fat distribution: Assessment by computed tomography. Tohoku J. Exp. Med. 2004, 204, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Aksungar, F.B.; Eren, A.; Ure, S.; Teskin, O.; Ates, G. Effects of Intermittent Fasting on Serum Lipid Levels, Coagulation Status and Plasma Homocysteine Levels. Ann. Nutr. Metab. 2005, 49, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Al-Numair, K. Body weight and some biochemical changes associated with Ramadan fasting in healthy Saudi men. J. Med. Sci. 2006, 6, 112–116. [Google Scholar]
- Lamine, F.; Bouguerra, R.; Jabrane, J.; Marrakchi, Z.; Ben, M.R.; Ben, C.S.; Gaigi, S. Food intake and high density lipoprotein cholesterol levels changes during Ramadan fasting in healthy young subjects. Tunis. Med. 2006, 84, 647–650. [Google Scholar] [PubMed]
- Subhan, M.F.; Siddiqui, Q.A.; Khan, M.N.; Sabir, S. Does Ramadan Fasting Affect Expiratory Flow Rates in Healthy Subjects. Saudi Med. J. 2006, 27, 1656–1660. [Google Scholar] [PubMed]
- Al-Hourani, H.M.; Atoum, M.F. Body composition, nutrient intake and physical activity patterns in young women during Ramadan. Singap. Med. J. 2007, 48, 906–910. [Google Scholar]
- Mansi, K.M.S. Study the effects of Ramadan fasting on the serum glucose and lipid profile among healthy Jordanian students. Am. J. Appl. Sci. 2007, 4, 565–569. [Google Scholar]
- Moosavi, S.A.J.; Kabir, A.; Moghimi, A.; Chehrei, A.; Rad, M.B. Evaluation of the effect of islamic fasting on lung volumes and capacities in the healthy persons. Saudi Med. J. 2007, 28, 1666–1670. [Google Scholar] [PubMed]
- Souissi, N.; Souissi, H.; Sahli, S.; Tabka, Z.; Dogui, M.; Ati, J.; Davenne, D. Effect of Ramadan on the diurnal variation in short-term high power output. Chronobiol. Int. 2007, 24, 991–1007. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, W.H.; Habib, H.M.; Jarrar, A.H.; Baz, S.A. Effect of Ramadan Fasting on Markers of Oxidative Stress and Serum Biochemical Markers of Cellular Damage in Healthy Subjects. Ann. Nutr. Metab. 2008, 53, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Stannard, S.R.; Thompson, M.W. The effect of participation in Ramadan on substrate selection during submaximal cycling exercise. J. Sci. Med. Sport 2008, 11, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Pathan, M.; Patil, R. Effect of Ramadan fasting on body weight and lipid profile. Biomed. Pharmacol. J. 2010, 3, 167–170. [Google Scholar]
- Assadi, A.; Akrami, A.; Beikzadeh, F.; Larijani, B.; Afarid, M.; Seidali, E. Impact of ramadan fasting on intraocular pressure, visual acuity and refractive errors. Singap. Med. J. 2011, 52, 263–266. [Google Scholar]
- Faris, M.A.E.; Kacimi, S.; Ref’at, A.; Fararjeh, M.A.; Bustanji, Y.K.; Mohammad, M.K.; Salem, M.L. Intermittent fasting during Ramadan attenuates proinflammatory cytokines and immune cells in healthy subjects. Nutr. Res. 2012, 32, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Faris, M.A.E.; Hussein, R.N.; Al-Kurd, R.A.; Al-Fararjeh, M.A.; Bustanji, Y.K.; Mohammad, M.K. Impact of Ramadan intermittent fasting on oxidative stress measured by urinary 15-f(2t)-isoprostane. J. Nutr. Metab. 2012, 2012, 802924. [Google Scholar] [CrossRef] [PubMed]
- Hajek, P.; Myers, K.; Dhanji, A.-R.; West, O.; McRobbie, H. Weight change during and after Ramadan fasting. J. Public Health 2012, 34, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Shehab, A.; Abdulle, A.; El-Issa, A.; Al-Suwaidi, J.; Nagelkerke, N. Favorable changes in lipid profile: The effects of fasting after Ramadan. PLoS ONE 2012, 7, e47615. [Google Scholar] [CrossRef] [PubMed]
- Racinais, S.; Périard, J.D.; Li, C.K.; Grantham, J. Activity patterns, body composition and muscle function during Ramadan in a middle-east Muslim Country. Int. J. Sports Med. 2012, 33, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Agoumi, A.; Martinez Martinez, F.; Garcia de la Serrana, H.L. The assessment of the follow-up of Muslim population during the period of Ramadan. J. Nutr. Food Sci. 2013, 3, 1–6. [Google Scholar]
- Develioglu, O.N.; Kucur, M.; Ipek, H.D.; Celebi, S.; Can, G.; Kulekci, M. Effects of ramadan fasting on serum immunoglobulin g and m, and salivary immunoglobulin a concentrations. J. Int. Med. Res. 2013, 41, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Haouari-Oukerro, F.; Ben-Attia, M.; Kaabachi, N.; Haouari, M. Ramadan fasting influences on food intake consumption, sleep schedule, body weight and some plasma parameters in healthy fasting volunteers. Afr. J. Biotechnol. 2013, 12, 3327–3332. [Google Scholar]
- Norouzy, A.; Salehi, M.; Philippou, E.; Arabi, H.; Shiva, F.; Mehrnoosh, S.; Mohajeri, S.M.R.; Mohajeri, S.R.; Motaghedi Larijani, A.; Nematy, M. Effect of fasting in Ramadan on body composition and nutritional intake: A prospective study. J. Hum. Nutr. Diet. 2013, 26, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Sayedda, K.; Kamal, S.; Ahmed, Q.S. Effect of Ramadan fasting on anthropometric parameters, blood pressure, creatine phosphokinase activity, serum calcium and phosphorus in healthy students of Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly-UP. Natl. J. Physiol. Pharm. Pharmacol. 2013, 3, 48–52. [Google Scholar] [CrossRef]
- Akaberi, A.; Golshan, A.; Moojdekanloo, M.; Hashemian, M. Does fasting in Ramadan ameliorate lipid profile? A prospective observational study. Pak. J. Med. Sci. 2014, 30, 708–711. [Google Scholar] [PubMed]
- Feizollahzadeh, S.; Rasuli, J.; Kheirouri, S.; Alizadeh, M. Augmented plasma adiponectin after prolonged fasting during Ramadan in men. Health Promot. Perspect. 2014, 4, 77–81. [Google Scholar] [PubMed]
- Cansel, M.; Taşolar, H.; Yağmur, J.; Ermiş, N.; Açıkgöz, N.; Eyyüpkoca, F.; Pekdemir, H.; Özdemir, R. The effects of Ramadan fasting on heart rate variability in healthy individuals: A prospective study. Anatol. J. Cardiol. 2014, 14, 413–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gnanou, J.V.; Caszo, B.A.; Khalil, K.M.; Abdullah, S.L.; Knight, V.F.; Bidin, M.Z. Effects of Ramadan fasting on glucose homeostasis and adiponectin levels in healthy adult males. J. Diabetes Metab. Disord. 2015, 14, 55. [Google Scholar] [CrossRef] [PubMed]
- Soori, M.; Mohaghegh, S.; Hajain, M.; Moraadi, B. Effects of Ramadan Fasting on Inspiratory Muscle Function. Asian J. Sports Med. 2015, 7, e35201. [Google Scholar] [CrossRef] [PubMed]
- López-Bueno, M.; González-Jiménez, E.; Navarro-Prado, S.; Montero-Alonso, M.A.; Schmidt-RioValle, J. Influence of age and religious fasting on the body composition of muslim women living in a westernized context. Nutr. Hosp. 2015, 31, 1067–1073. [Google Scholar]
- Talib, R.A.; Canguven, O.; Al-Rumaihi, K.; Al-Ansari, A.; Alani, M. The effect of fasting on erectile function and sexual desire on men in the month of Ramadan. Urol. J. 2015, 12, 2099–2102. [Google Scholar] [PubMed]
- Sarici, A.M.; Yuksel Elgin, C.; Dikkaya, F. Effect of Fasting on Corneal Biomechanical and Structural Parameters. Curr. Eye Res. 2016, 41, 908–912. [Google Scholar] [CrossRef] [PubMed]
- Sezen, Y.; Altiparmak, I.H.; Erkus, M.E.; Kocarslan, A.; Kaya, Z.; Gunebakmaz, O.; Demirbag, R. Effects of Ramadan fasting on body composition and arterial stiffness. J. Pak. Med. Assoc. 2016, 66, 1522–1527. [Google Scholar] [PubMed]
- Alsubheen, S.A.; Ismail, M.; Baker, A.; Blair, J.; Adebayo, A.; Kelly, L.; Chandurkar, V.; Cheema, S.; Joanisse, D.R.; Basset, F.A. The effects of diurnal Ramadan fasting on energy expenditure and substrate oxidation in healthy men. Br. J. Nutr. 2017, 118, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Rasheed, A.; Ahmed, H.; Aslam, F.; Kanwal, F. Effect of ramadan fasting on glucose level, lipid profile, HbA1c and uric acid among medical students in Karachi, Pakistan. East. Mediterr. Health J. 2017, 23, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Kiyani, M.M.; Memon, A.R.; Amjad, M.I.; Ameer, M.R.; Sadiq, M.; Mahmood, T. Study of Human Biochemical Parameters During and After Ramadan. J. Relig. Health. 2017, 56, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Latiri, I.; Sandid, S.; Fennani, M.A.; Hadrich, M.; Masmoudi, T.; Maatoug, C.; Zammit-Chatti, M.; Chamari, K.; Ben Saad, H. The Effects of Ramadan Fasting on the Spirometric Data of Healthy Adult Males. Am. J. Men’s Health 2017, 11, 1214–1223. [Google Scholar] [CrossRef] [PubMed]
- Malekmakan, L.; Sayadi, M.; Pakfetrat, M.; Moosavi, B.; Mousavinezhad, H. The effect of fasting on anthropometric parameters and blood pressure levels: A report from Southern Iran. Int. Cardiovasc. Res. J. 2017, 11, 143–147. [Google Scholar]
- Norouzy, A.; Hasanzade Daloee, M.; Khoshnasab, A.H.; Khoshnasab, A.; Farrokhi, J.; Nematy, M.; Safarian, M.; Nezafati, P.; Alinezhad-Namaghi, M. Trend of blood pressure in hypertensive and normotensive volunteers during Ramadan fasting. Blood Press. Monit. 2017, 22, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Nugraha, B.; Ghashang, S.K.; Hamdan, I.; Gutenbrunner, C. Effect of Ramadan fasting on fatigue, mood, sleepiness, and health-related quality of life of healthy young men in summer time in Germany: A prospective controlled study. Appetite 2017, 111, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Ongsara, S.; Boonpol, S.; Prompalad, N.; Jeenduang, N. The effect of ramadan fasting on biochemical parameters in healthy thai subjects. J. Clin. Diagn. Res. 2017, 11, BC14. [Google Scholar] [CrossRef] [PubMed]
- Almeneessier, A.S.; Bahammam, A.S.; Sharif, M.M.; Bahammam, S.A.; Nashwan, S.Z.; Perumal, S.R.P.; Cardinali, D.P.; Alzoghaibi, M. The influence of intermittent fasting on the circadian pattern of melatonin while controlling for caloric intake, energy expenditure, light exposure, and sleep schedules: A preliminary report. Ann. Thorac. Med. 2017, 12, 183–190. [Google Scholar] [PubMed]
- Almeneessier, A.S.; Alzoghaibi, M.; BaHammam, A.A.; Ibrahim, M.G.; Olaish, A.H.; Nashwan, S.Z.; BaHammam, A.S. The effects of diurnal intermittent fasting on the wake-promoting neurotransmitter orexin-A. Ann. Thorac. Med. 2018, 13, 48–54. [Google Scholar] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Identifying and Quantifying Heterogeneity; Introduction to Meta-Analysis; John Wiley & Sons: West Sussex, UK, 2009; pp. 107–119. [Google Scholar]
- Higgins, J.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogunbode, A.M.; Fatiregun, A.A.; Ogunbode, O.O. Health Risks of Obesity. Ann. Ib. Postgrad. Med. 2009, 7, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Marks, B.; Rippe, J.M. The importannce of fat-free mass maintenance in weight loss programmes. Sports Med. 1996, 22, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Chaston, T.B.; Dixon, J.B.; O’Brien, P.B. Changes in fat-free mass during significant weight loss: A systematic review. Int. J. Obes. 2007, 31, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Kehoe, S.H.; Krishnaveni, G.V.; Lubree, H.G.; Wills, A.K.; Guntupalli, A.M.; Veena, S.R.; Bhat, D.S.; Kishore, R.; Fall, C.H.; Yajnik, C.S.; et al. Prediction of body fat percentage from skinfold and bio-impedance measurements in Indian school children. Eur. J. Clin. Nutr. 2011, 65, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Kuriyan, R.; Thomas, T.; Ashok, S.; Jayakumar, J.; Kurpad, A.V. A 4-compartment model based validation of air displacement plethysmography, dual energy X-ray absorptiometry, skinfold technique & bio-electrical impedance for measuring body fat in Indian adults. Indian J. Med. Res. 2014, 139, 700–707. [Google Scholar] [PubMed]
- Nickerson, B.S.; Esco, M.R.; Bishop, P.A.; Schumacker, R.E.; Richardson, M.T.; Fedewa, M.V.; Wingo, J.E.; Welborn, B.A. Validity Of Selected Bioimpedance Equations For Estimating Body Composition In Men And Women: A Four-Compartment Model Comparison. J. Strength Cond. Res. 2016, 31, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Minderico, C.S.; Silva, A.M.; Keller, K.; Branco, T.L.; Martins, S.S.; Palmeira, A.L.; Barata, J.T.; Carnero, E.A.; Rocha, P.M.; Teixeira, P.J. Usefulness of different techniques for measuring body composition changes during weight loss in overweight and obese women. Br. J. Nutr. 2008, 99, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.M.; Fields, D.A.; Quiterio, A.L.; Sardinha, L.B. Are skinfold-based models accurate and suitable for assessing changes in body composition in highly trained athletes? J. Strength Cond. Res. 2009, 23, 1688–1696. [Google Scholar] [CrossRef] [PubMed]
- Matias, C.N.; Santos, D.A.; Fields, D.A.; Sardinha, L.B.; Silva, A.M. Is bioelectrical impedance spectroscopy accurate in estimating changes in fat-free mass in judo athletes? J. Sports Sci. 2012, 30, 1225–1233. [Google Scholar] [CrossRef] [PubMed]
- Verdich, C.; Barbe, P.; Petersen, M.; Grau, K.; Ward, L.; Macdonald, I.; Sørensen, T.I.; Oppert, J.M. Changes in body composition during weight loss in obese subjects in the NUGENOB study: Comparison of bioelectrical impedance vs. dual-energy X-ray absorptiometry. Diabetes Metab. 2011, 37, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Wan, C.S.; Ward, L.C.; Halim, J.; Gow, M.L.; Ho, M.; Briody, J.N.; Leung, K.; Cowell, C.T.; Garnett, S.P. Bioelectrical impedance analysis to estimate body composition, and change in adiposity, in overweight and obese adolescents: Comparison with dual-energy x-ray absorptiometry. BMC Pediatr. 2014, 14, 249. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, I.M.; Faber, P.; Gibney, E.R.; Lobley, G.E.; Stubbs, R.J.; Siervo, M. Measurement of body composition changes during weight loss in obese men using multi-frequency bioelectrical impedance analysis and multi-compartment models. Obes. Res. Clin. Pract. 2014, 8, e46–e54. [Google Scholar] [CrossRef] [PubMed]
- Kreitzman, S.N.; Coxon, A.Y.; Szaz, K.F. Glycogen storage: Illusions of easy weight loss, excessive weight regain, and distortions in estimates of body composition. Am. J. Clin. Nutr. 1992, 56 (Suppl. S1), 292S–293S. [Google Scholar] [CrossRef] [PubMed]
- Cava, E.; Yeat, N.C.; Mittendorfer, B. Preserving Healthy Muscle during Weight Loss. Adv. Nutr. 2017, 8, 511–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingstone, M.B.; Prentice, A.M.; Strain, J.J.; Coward, W.A.; Black, A.E.; Barker, M.E.; McKenna, P.G.; Whitehead, R.G. Accuracy of weighed dietary records in studies of diet and health. Br. Med. J. 1990, 300, 708–712. [Google Scholar] [CrossRef]
- Gibson, A.A.; Hsu, M.S.; Rangan, A.M.; Seimon, R.V.; Lee, C.M.; Das, A.; Finch, C.H.; Sainsbury, A. Accuracy of hands v. household measures as portion size estimation aids. Br. Med. J. 2016, 5, e29. [Google Scholar] [CrossRef] [PubMed]
- Hatori, M.; Vollmers, C.; Zarrinpar, A.; DiTacchio, L.; Bushong, E.A.; Gill, S.; Leblanc, M.; Chaix, A.; Joens, M.; Fitzpatrick, J.A.; et al. Time-Restricted Feeding without Reducing Caloric Intake Prevents Metabolic Diseases in Mice Fed a High-Fat Diet. Cell Metab. 2012, 15, 848–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzoghaibi, M.A.; Pandi-Perumal, S.R.; Sharif, M.M.; BaHammam, A.S. Diurnal intermittent fasting during ramadan: The effects on Leptin and Ghrelin levels. PLoS ONE 2014, 9, e92214. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, T.J.; Wong, J.; Markovic, T.; Yue, D.; Wu, T.; Brooks, B.; Hetherington, J.; Seimon, R.; Gibson, A.A.; Toth, K.; et al. Brief report: Ramadan as a model of intermittent fasting: Effects on body composition, metabolic parameters, gut hormones and appetite in adults with and without type 2 diabetes mellitus. Obes. Med. 2017, 6, 15–17. [Google Scholar] [CrossRef]
- Maddison, R.; Jiang, Y.; Vander Hoorn, S.; Ni Mhurchu, C.; Lawes, C.M.; Rodgers, A.; Rush, E. Estimating energy expenditure with the RT3 triaxial accelerometer. Res. Q. Exerc. Sport 2009, 80, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Johannsen, D.L.; Calabro, M.A.; Stewart, J.; Franke, W.; Rood, J.C.; Welk, G.J. Accuracy of armband monitors for measuring daily energy expenditure in healthy adults. Med. Sci. Sports Exerc. 2010, 42, 2134–2140. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.; Shamsuddin, K.; Latiff, K.A.; Saad, H.A.; Majid, L.A.; Otman, F.M. Voluntary Fasting to Control Post-Ramadan Weight Gain among Overweight and Obese Women. Sultan Qaboos Univ. Med. J. 2015, 15, e98–e104. [Google Scholar] [PubMed]
- Charakida, M.; Khan, T.; Johnson, W.; Finer, N.; Woodside, J.; Whincup, P.H.; Sattar, N.; Kuh, D.; Hardy, R.; Deanfield, J. Lifelong patterns of BMI and cardiovascular phenotype in individuals aged 60–64 years in the 1946 British birth cohort study: An epidemiological study. Lancet Diabetes Endocrinol. 2014, 2, 648–654. [Google Scholar] [CrossRef]
- Li, G.; Zhang, P.; Wang, J.; An, Y.; Gong, Q.; Gregg, E.W.; Yang, W.; Zhang, B.; Shuai, Y.; Hong, J.; et al. Cardiovascular mortality, all-cause mortality, and diabetes incidence after lifestyle intervention for people with impaired glucose tolerance in the Da Qing Diabetes Prevention Study: A 23-year follow-up study. Lancet Diabetes Endocrinol. 2014, 2, 474–480. [Google Scholar] [CrossRef]
- Salim, I.; Suwaidi, A.I.; Ghadban, W.; Alkilani, H.; Salam, A.M. Impact of religious Ramadan fasting on cardiovascular disease: A systematic review of the literature. Curr. Med. Res. Opin. 2013, 29, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Mazidi, M.; Rezaie, P.; Chaudhri, O.; Karimi, E.; Nematy, M. The effect of Ramadan fasting on cardiometabolic risk factors and anthropometrics parameters: A systematic review. Pak. J. Med. Sci. 2015, 31, 1250–1255. [Google Scholar] [CrossRef] [PubMed]
- Kul, S.; Savas, E.; Ozturk, Z.A.; Karadag, G. Does Ramadan fasting alter body weight and blood lipids and fasting blood glucose in a healthy population? A meta-analysis. J. Relig. Health 2014, 53, 929–942. [Google Scholar] [CrossRef] [PubMed]
- Khatib, F.A.; Shafagoj, Y.A. Metabolic alterations as a result of Ramadan fasting in non-insulin-dependent diabetes mellitus patients in relation to food intake. Saudi Med. J. 2004, 25, 1858–1863. [Google Scholar] [PubMed]
- Khaled, B.M.; Bendahmane, M.; Belbraouet, S. Ramadan fasting induces modifications of certain serum components in obese women with type 2 diabetes. Saudi Med. J. 2006, 27, 23–26. [Google Scholar] [PubMed]
- Yarahmadi, S.H.; Larijani, B.; Bastanhagh, M.H.; Pajouhi, M.; Baradar, R.J.; Zahedi, F.; Zendehdel, K.; Akrami, S.M. Metabolic and clinical effects of Ramadan fasting in patients with type II diabetes. J. Coll. Physicians Surg. Pak. 2003, 13, 329–332. [Google Scholar] [PubMed]
- Comoglu, S.; Temizhan, A.; Pesinci, E.; Tandogan, I.; Ozbakir, S. Effects of Ramadan Fasting on Stroke. Turk J. Med. Sci. 2003, 33, 237–241. [Google Scholar]
- Bener, A.; Hamad, A.; Fares, A.; Al-Sayed, H.M.; Al-Suwaidi, J. Is there any effect of Ramadan fasting on stroke incidence? Singap. Med. J. 2006, 47, 404–408. [Google Scholar]
- PRISMA Checklist. PRISMA: Transparent Reporting of Systematic Reviews and Meta-Analyses. Available online: http://www.prisma-statement.org/PRISMAStatement/ (accessed on 20 June 2018).








© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernando, H.A.; Zibellini, J.; Harris, R.A.; Seimon, R.V.; Sainsbury, A. Effect of Ramadan Fasting on Weight and Body Composition in Healthy Non-Athlete Adults: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 478. https://doi.org/10.3390/nu11020478
Fernando HA, Zibellini J, Harris RA, Seimon RV, Sainsbury A. Effect of Ramadan Fasting on Weight and Body Composition in Healthy Non-Athlete Adults: A Systematic Review and Meta-Analysis. Nutrients. 2019; 11(2):478. https://doi.org/10.3390/nu11020478
Chicago/Turabian StyleFernando, Hamish A., Jessica Zibellini, Rebecca A. Harris, Radhika V. Seimon, and Amanda Sainsbury. 2019. "Effect of Ramadan Fasting on Weight and Body Composition in Healthy Non-Athlete Adults: A Systematic Review and Meta-Analysis" Nutrients 11, no. 2: 478. https://doi.org/10.3390/nu11020478