Lactofermented Annurca Apple Puree as a Functional Food Indicated for the Control of Plasma Lipid and Oxidative Amine Levels: Results from a Randomised Clinical Trial

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Reagents and Standards
2.2. Fruit Collection and Annurca Apple Puree (AAP) Preparation
2.3. Lactofermented AAP (lfAAP) Preparation
2.4. Enumeration of Probiotic Microorganisms in lfAAP
2.5. Preparation of Polyphenolic Extracts from AAP and lfAAP Samples
2.6. HPLC-DAD/ESI-MS Analysis of Polyphenolic Extracts
2.7. Study Population and Protocol
2.8. Randomisation, Concealment, and Blinding
2.9. Study Outcomes and Data Collection
2.9.1. Primary and Secondary Efficacy Outcomes
2.9.2. Safety
2.10. Statistics
2.10.1. Methodology
2.10.2. Analysis Sets
2.10.3. Determination of Sample Size
2.11. Subject Involvement
3. Results
3.1. Polyphenolic Composition of AAP and lfAAP
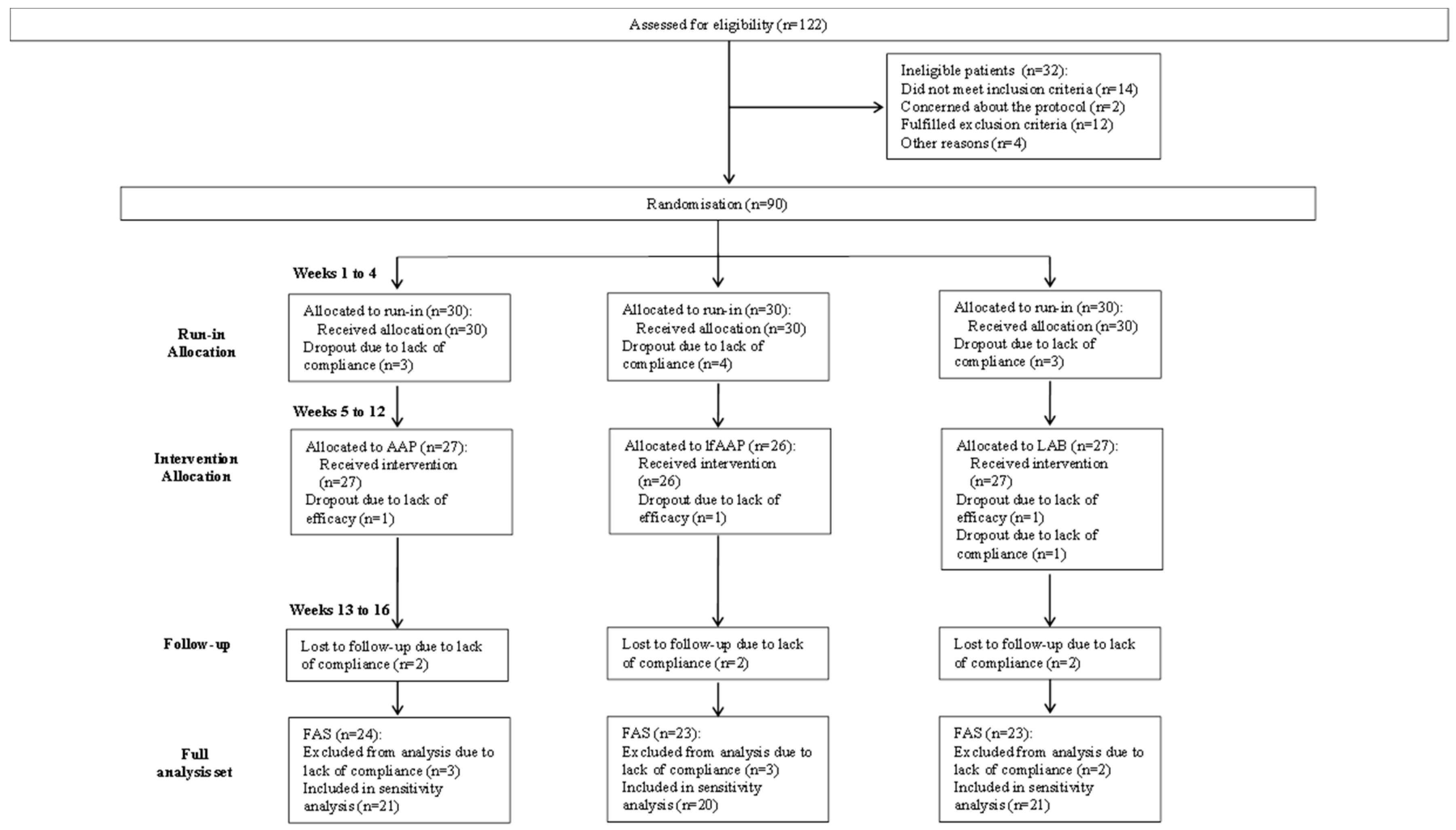
3.2. Enrolment and Subject Attrition
3.3. Participants’ Baseline Characteristics
3.4. Primary Efficacy Outcome Measures
3.5. Secondary Efficacy Outcome Measures
3.6. Study Strength and Limitations
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical approval
Transparency statement
References
- Cheynier, V. Polyphenols in foods are more complex than often thought. Am. J. Clin. Nutr. 2005, 81, 223s–229s. [Google Scholar] [CrossRef] [PubMed]
- Crozier, A.; Jaganath, I.B.; Clifford, M.N. Dietary phenolics: Chemistry, bioavailability and effects on health. Nat. Prod. Rep. 2009, 26, 1001–1043. [Google Scholar] [CrossRef] [PubMed]
- Scalbert, A.; Johnson, I.T.; Saltmarsh, M. Polyphenols: Antioxidants and beyond. Am. J. Clin. Nutr. 2005, 81, 215s–217s. [Google Scholar] [CrossRef] [PubMed]
- Padayachee, A.; Netzel, G.; Netzel, M.; Day, L.; Zabaras, D.; Mikkelsen, D.; Gidley, M. Binding of polyphenols to plant cell wall analogues-Part 1: Anthocyanins. Food Chem. 2012, 134, 155–161. [Google Scholar] [CrossRef]
- Padayachee, A.; Netzel, G.; Netzel, M.; Day, L.; Zabaras, D.; Mikkelsen, D.; Gidley, M.J. Binding of polyphenols to plant cell wall analogues-Part 2: Phenolic acids. Food Chem. 2012, 135, 2287–2292. [Google Scholar] [CrossRef] [PubMed]
- Le Bourvellec, C.; Bouchet, B.; Renard, C.M.G.C. Non-covalent interaction between procyanidins and apple cell wall material. Part III: Study on model polysaccharides. Bba-Gen Subj. 2005, 1725, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Renard, C.M.G.C.; Baron, A.; Guyot, S.; Drilleau, J.F. Interactions between apple cell walls and native apple polyphenols: Quantification and some consequences. Int. J. Biol. Macromol. 2001, 29, 115–125. [Google Scholar] [CrossRef]
- Beliveau, R. Role of nutrition in preventing cancer. Can. Fam. Physician 2007, 53, 1905–1911. [Google Scholar]
- Ebner, S.; Smug, L.N.; Kneifel, W.; Salminen, S.J.; Sanders, M.E. Probiotics in dietary guidelines and clinical recommendations outside the European Union. World J. Gastroenterol. 2014, 20, 16095–16100. [Google Scholar] [CrossRef]
- Marco, M.L.; Heeney, D.; Binda, S.; Cifelli, C.J.; Cotter, P.D.; Foligne, B.; Ganzle, M.; Kort, R.; Pasin, G.; Pihlanto, A.; et al. Health benefits of fermented foods: Microbiota and beyond. Curr. Opin. Biotech. 2017, 44, 94–102. [Google Scholar] [CrossRef]
- Ray, R.C.; Ward, O.P. Microbial Biotechnology in Horticulture; CRC Press: Plymouth, UK, 2006; Volume 1. [Google Scholar]
- Motarjemi, Y. Impact of small scale fermentation technology on food safety in developing countries. Int. J. Food Microbiol. 2002, 75, 213–229. [Google Scholar] [CrossRef]
- Septembre-Malaterre, A.; Remize, F.; Poucheret, P. Fruits and vegetables, as a source of nutritional compounds and phytochemicals: Changes in bioactive compounds during lactic fermentation. Food Res. Int. 2018, 104, 86–99. [Google Scholar] [CrossRef] [PubMed]
- Granito, M.; Frias, J.; Doblado, R.; Guerra, M.; Champ, M.; Vidal-Valverde, C. Nutritional improvement of beans (Phaseolus vulgaris) by natural fermentation. Eur. Food Res. Technol. 2002, 214, 226–231. [Google Scholar] [CrossRef]
- Martin-Cabrejas, M.A.; Sanfiz, B.; Vidal, A.; Molla, E.; Esteban, R.; Lopez-Andreu, F.J. Effect of fermentation and autoclaving on dietary fiber fractions and anti nutritional factors of beans (Phaseolus vulgaris L.). J. Agric. Food Chem. 2004, 52, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Siebenhandl, S.; Lestario, L.N.; Trimmel, D.; Berghofer, E. Studies on tape ketan-an Indonesian fermented rice food. Int. J. Food Sci. Nutr. 2001, 52, 347–357. [Google Scholar] [CrossRef]
- Tenore, G.C.; Campiglia, P.; Stiuso, P.; Ritieni, A.; Novellino, E. Nutraceutical potential of polyphenolic fractions from Annurca apple (M. pumila Miller cv Annurca). Food Chem. 2013, 140, 614–622. [Google Scholar] [CrossRef] [PubMed]
- Tenore, G.C.; Caruso, D.; Buonomo, G.; D’Urso, E.; D’Avino, M.; Campiglia, P.; Marinelli, L.; Novellino, E. Annurca (Malus pumila Miller cv. Annurca) apple as a functional food for the contribution to a healthy balance of plasma cholesterol levels: Results of a randomized clinical trial. J. Sci. Food Agric. 2017, 97, 2107–2115. [Google Scholar] [CrossRef]
- Lo Scalzo, R.; Testoni, A.; Genna, A. ‘Annurca’ apple fruit, a southern Italy apple cultivar: Textural properties and aroma composition. Food Chem. 2001, 73, 333–343. [Google Scholar] [CrossRef]
- Nazzaro, F.; Fratianni, F.; Sada, A.; Orlando, P. Synbiotic potential of carrot juice supplemented with Lactobacillus spp. and inulin or fructooligosaccharides. J. Sci. Food Agric. 2008, 88, 2271–2276. [Google Scholar] [CrossRef]
- Garbetta, A.; D’Antuono, I.; Sisto, A.; Minervini, F.; Cardinali, A.; Lavermicocca, P. Effect of artichoke fermentation by probiotic strain Lactobacillus paracasei LMG P-22043 and of digestion process on polyphenols and antioxidant activity. J. Funct. Foods 2018, 45, 523–529. [Google Scholar] [CrossRef]
- Beale, R.; Airs, R. Quantification of glycine betaine, choline and trimethylamine N-oxide in seawater particulates: Minimisation of seawater associated ion suppression. Anal. Chim. Acta 2016, 938, 114–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Little, R.J.A.; Rubin, D.B. Statistical Analysis with Missing Data; John Wiley & Sons, Inc.: New York, NY, USA, 2002. [Google Scholar]
- Molenberghs, G.; Thijs, H.; Jansen, I.; Beunckens, C.; Kenward, M.G.; Mallinckrodt, C.; Carroll, R.J. Analyzing incomplete longitudinal clinical trial data. Biostatistics 2004, 5, 445–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Kelly, M.; Ratitch, B. Clinical Trials with Missing Data: A Guide for Practitioners; John Wiley & Sons, Inc.: New York, NY, USA, 2014. [Google Scholar]
- White, I.R.; Carpenter, J.; Horton, N.J. Including all individuals is not enough: Lessons for intention-to-treat analysis. Clin. Trials 2012, 9, 396–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvert, M.; Blazeby, J.; Altman, D.G.; Revicki, D.A.; Moher, D.; Brundage, M.D.; Grp, C.P. Reporting of patient-reported outcomes in randomized trials: The CONSORT PRO extension. J. Am. Med. Assoc. 2013, 309, 814–822. [Google Scholar] [CrossRef] [PubMed]
- Day, A.J.; Canada, F.J.; Diaz, J.C.; Kroon, P.A.; Mclauchlan, R.; Faulds, C.B.; Plumb, G.W.; Morgan, M.R.A.; Williamson, G. Dietary flavonoid and isoflavone glycosides are hydrolysed by the lactase site of lactase phlorizin hydrolase. FEBS Lett. 2000, 468, 166–170. [Google Scholar] [CrossRef] [Green Version]
- Crozier, A. Plant Secondary Metabolites: Occurrence, Structure and Role in the Human Diet; Blackwell Publishing Ltd.: Hoboken, NJ, USA, 2007. [Google Scholar]
- Li, X.S.M.; Obeid, S.; Klingenberg, R.; Gencer, B.; Mach, F.; Raber, L.; Windecker, S.; Rodondi, N.; Nanchen, D.; Muller, O.; et al. Gut microbiota-dependent trimethylamine N-oxide in acute coronary syndromes: A prognostic marker for incident cardiovascular events beyond traditional risk factors. Eur. Heart J. 2017, 38, 814–824. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, S.; Fletcher, C. Trimethylamine N-oxide: Breathe new life. Br. J. Pharmacol. 2018, 175, 1344–1353. [Google Scholar] [CrossRef]
- Ufnal, M.; Zadlo, A.; Ostaszewski, R. TMAO: A small molecule of great expectations. Nutrition 2015, 31, 1317–1323. [Google Scholar] [CrossRef]
- Wang, Z.N.; Klipfell, E.; Bennett, B.J.; Koeth, R.; Levison, B.S.; Dugar, B.; Feldstein, A.E.; Britt, E.B.; Fu, X.M.; Chung, Y.M.; et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011, 472, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Zeisel, S.H.; Wishnok, J.S.; Blusztajn, J.K. Formation of methylamines from ingested choline and lecithin. J. Pharmacol. Exp. Ther. 1983, 225, 320–324. [Google Scholar]
- Bennett, B.J.; Vallim, T.Q.D.; Wang, Z.N.; Shih, D.M.; Meng, Y.H.; Gregory, J.; Allayee, H.; Lee, R.; Graham, M.; Crooke, R.; et al. Trimethylamine-N-Oxide, a metabolite associated with atherosclerosis, exhibits complex genetic and dietary regulation. Cell Metab. 2013, 17, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Koeth, R.A.; Levison, B.S.; Culley, M.K.; Buffa, J.A.; Wang, Z.N.; Gregory, J.C.; Org, E.; Wu, Y.P.; Li, L.; Smith, J.D.; et al. gamma-Butyrobetaine Is a proatherogenic intermediate in gut microbial metabolism of L-Carnitine to TMAO. Cell Metab. 2014, 20, 799–812. [Google Scholar] [CrossRef] [PubMed]
- Lyu, M.; Wang, Y.F.; Fan, G.W.; Wang, X.Y.; Xu, S.Y.; Zhu, Y. Balancing herbal medicine and functional food for prevention and treatment of cardiometabolic diseases through modulating gut microbiota. Front. Microbiol. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Selma, M.V.; Espin, J.C.; Tomas-Barberan, F.A. Interaction between phenolics and gut microbiota: Role in human health. J. Agric. Food Chem. 2009, 57, 6485–6501. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.C.; Jenner, A.M.; Low, C.S.; Lee, Y.K. Effect of tea phenolics and their aromatic fecal bacterial metabolites on intestinal microbiota. Res. Microbiol. 2006, 157, 876–884. [Google Scholar] [CrossRef] [PubMed]
- De Filippis, F.; Pellegrini, N.; Vannini, L.; Jeffery, I.B.; La Storia, A.; Laghi, L.; Serrazanetti, D.I.; Di Cagno, R.; Ferrocino, I.; Lazzi, C.; et al. High-level adherence to a Mediterranean diet beneficially impacts the gut microbiota and associated metabolome. Gut 2016, 65, 1812–1821. [Google Scholar] [CrossRef] [PubMed]
- Barrett, E.L.; Kwan, H.S. Bacterial reduction of trimethylamine oxide. Annu. Rev. Microbiol. 1985, 39, 131–149. [Google Scholar] [CrossRef] [PubMed]
- Baugh, M.E.; Steele, C.N.; Angiletta, C.J.; Mitchell, C.M.; Neilson, A.P.; Davy, B.M.; Hulver, M.W.; Davy, K.P. Inulin supplementation does not reduce plasma trimethylamine n-oxide concentrations in individuals at risk for type 2 diabetes. Nutrients 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Angiletta, C.J.; Griffin, L.E.; Steele, C.N.; Baer, D.J.; Novotny, J.A.; Davy, K.P.; Neilson, A.P. Impact of short-term flavanol supplementation on fasting plasma trimethylamine N-oxide concentrations in obese adults. Food Func. 2018, 9, 5350–5361. [Google Scholar] [CrossRef]
- Islamova, Z.I.; Ogai, D.K.; Abramenko, O.I.; Lim, A.L.; Abduazimov, B.B.; Malikova, M.K.; Rakhmanberdyeva, R.K.; Khushbaktova, Z.A.; Syrov, V.N. Comparative assessment of the prebiotic activity of some pectin polysaccharides. Pharm. Chem. J. 2017, 51, 288–291. [Google Scholar] [CrossRef]
- Chung, W.S.F.; Meijerink, M.; Zeuner, B.; Hoick, J.; Louis, P.; Meyer, A.S.; Wells, J.M.; Flint, H.J.; Duncan, S.H. Prebiotic potential of pectin and pectic oligosaccharides to promote anti-inflammatory commensal bacteria in the human colon. FEMS Microbiol. Ecol. 2017, 93. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.T.; Teixeira, M.M.; Martins, F.S. The role of probiotics and prebiotics in inducing gut immunity. Front. Immunol. 2013, 4. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| AAP | lfAAP (by L. rhamnosus at 24 h) | lfAAP (by L. rhamnosus at 48 h) | lfAAP (by L. plantarum at 24 h) | lfAAP (by L. plantarum at 48 h) | |
|---|---|---|---|---|---|
| Chlorogenic acid | 8.98 ± 0.02 a | 10.78 ± 0.03 b | 9.88 ± 0.02 c | 9.16 ± 0.04 a | 9.07 ± 0.05 a |
| [+]-Catechin | 1.20 ± 0.04 a | 1.52 ± 0.03 b | 1.34 ± 0.05 c | 1.25 ± 0.04 a | 1.22 ± 0.06 a |
| [−]-Epicatechin | 2.80 ± 0.06 a | 3.48 ± 0.05 b | 3.14 ± 0.04 c | 2.91 ± 0.03 a | 2.86 ± 0.07 a |
| Procyanidin B1 | 0.70 ± 0.02 a | 1.01 ± 0.03 b | 0.84 ± 0.05 c | 0.78 ± 0.03 a | 0.75 ± 0.02 a |
| Procianidin B2 | 1.78 ± 0.02 a | 2.58 ± 0.04 b | 2.14 ± 0.02 c | 1.99 ± 0.03 d | 1.88 ± 0.05 a,d |
| Procyanidin trimer | 1.28 ± 0.02 a | 1.87 ± 0.04 b | 1.54 ± 0.02 c | 1.43 ± 0.03 d | 1.36 ± 0.01 e |
| Cyanidin-3-O-galactoside | 0.04 ± 0.02 a | 0.05 ± 0.02 a | 0.05 ± 0.02 a | 0.04 ± 0.03 a | 0.04 ± 0.02 a |
| Rutin (Quercetin-3-O-rutinoside) | 0.80 ± 0.02 a | 1.08 ± 0.03 b | 0.93 ± 0.04 c | 0.86 ± 0.02 d | 0.83 ± 0.05 a |
| Hyperin (Quercetin-3-O-galactoside) | 8.90 ± 0.04 a | 12.1 ± 0.06 b | 10.3 ± 0.04 c | 9.61 ± 0.05 d | 9.26 ± 0.03 e |
| Isoquercitrin (Quercetin-3-O-glucoside) | 3.52 ± 0.02 a | 4.75 ± 0.03 b | 4.08 ± 0.06 c | 3.80 ± 0.05 d | 3.66 ± 0.03 e |
| Reynoutrin (Quercetin-3-O-xyloside) | 2.04 ± 0.08 a | 2.75 ± 0.05 b | 2.37 ± 0.07 c | 2.20 ± 0.06 d | 2.12 ± 0.08 a |
| Guajaverin (Quercetin 3-O-arabinopyranoside) | 1.74 ± 0.02 a | 2.35 ± 0.04 b | 2.02 ± 0.03 c | 1.88 ± 0.06 d | 1.81 ± 0.05 a |
| Avicularin (Quercetin 3-O-arabinofuranoside) | 3.96 ± 0.02 a | 5.35 ± 0.07 b | 4.59 ± 0.02 c | 4.28 ± 0.09 d | 4.12 ± 0.08 e |
| Quercetin-O-pentoside | 1.22 ± 0.02 a | 1.65 ± 0.04 b | 1.39 ± 0.03 c | 1.32 ± 0.02 d | 1.27 ± 0.05 a |
| Quercitrin (Quercetin-3-O-rhamnoside) | 2.34 ± 0.02 a | 3.16 ± 0.02 b | 2.71 ± 0.04 c | 2.53 ± 0.06 d | 2.43 ± 0.07 a |
| Phloretin-2-O-xyloglucoside | 2.70 ± 0.02 a | 3.78 ± 0.05 b | 3.19 ± 0.08 c | 2.97 ± 0.04 d | 2.83 ± 0.02 e |
| Phloridzin (phloretin-2-O-glucoside) | 3.02 ± 0.02 a | 4.23 ± 0.07 b | 3.56 ± 0.06 c | 3.32 ± 0.04 d | 3.17 ± 0.02 e |
| Total polyphenols | 47.02 ± 0.09 a | 62.40 ± 0.12 b | 54.07 ± 0.14 c | 50.33 ± 0.11 d | 46.25 ± 0.10 a |
| Run-in | |||
|---|---|---|---|
| Characteristics | AAP (n = 30) | lfAAP (n = 30) | LAB (n = 30) |
| Demographics | |||
| Age (years) | 46.9 ± 10.6 | 45.8 ± 11.1 | 47.6 ± 10.4 |
| Male sex (No (%)) | 17 (56.7%) | 18 (60.0%) | 16 (53.3%) |
| White ethnicity (No (%)) | 30 (100%) | 30 (100%) | 30 (100%) |
| Clinical parameters | |||
| TC (mg/dL) | 234.1 ± 13.2 | 238.5 ± 12.1 | 236.2 ± 11.8 |
| LDL-C (mg/dL) | 154.0 ± 11.1 | 155.7 ± 12.4 | 166.9 ± 12.0 |
| HDL-C (mg/dL) | 37.8 ± 6.3 | 38.3 ± 7.4 | 40.5 ± 6.6 |
| Glucose (mg/dL) | 100.5 ± 8.2 | 102.2 ± 9.3 | 110.2 ± 9.1 |
| Triglycerides (mg/dL) | 178.1 ± 9.6 | 188.1 ± 11.7 | 197.6 ± 11.6 |
| TMAO (μM) | 2.01 ± 0.05 | 2.68 ± 0.06 | 1.72 ± 0.06 |
| Treatment | |||
| Characteristics | AAP (n = 27) | lfAAP (n = 26) | LAB (n = 27) |
| Demographics | |||
| Age (years) | 45.1 ± 10.3 | 46.2 ± 10.7 | 48.2 ± 10.2 |
| Male sex (No (%)) | 15 (55.5%) | 16 (61.5%) | 15 (55.5%) |
| White ethnicity (No (%)) | 27 (100%) | 26 (100%) | 27 (100%) |
| Clinical parameters | |||
| TC (mg/dL) | 235.5 ± 13.3 | 237.6 ± 14.3 | 239.1 ± 11.9 |
| LDL-C (mg/dL) | 152.1 ± 11.1 | 156.4 ± 11.6 | 165.8 ± 11.7 |
| HDL-C (mg/dL) | 36.7 ± 7.5 | 37.4 ± 6.7 | 38.5 ± 7.2 |
| Glucose (mg/dL) | 99.1 ± 2.7 | 100.0 ± 8.9 | 107.2 ± 8.5 |
| Triglycerides (mg/dL) | 180.4 ± 16.8 | 185.2 ± 18.3 | 200.1 ± 19.0 |
| TMAO (μM) | 2.37 ± 0.04 | 3.01 ± 0.05 | 2.02 ± 0.06 |
| AAP | Δ (%) | lfAAP | Δ (%) | LAB | Δ (%) | ||
|---|---|---|---|---|---|---|---|
| TC (mg/dL) | t 0 | 235.5 ± 13.3 | 237.6 ± 14.3 | 239.1 ± 11.9 | |||
| t 30 | 246.1 ± 14.2 | +4.5 | 257.1 ± 12.8 | +8.2 | 242.2 ± 13.5 | +1.3 | |
| t 60 | 246.8 ± 13.6 | +4.8 | 259.0 ± 12.1 | +9.0 | 243.4 ± 13.8 | +1.8 | |
| t 90 | 248.2 ± 14.0 | +5.4 | 259.5 ± 16.7 | +9.2 | 253.1 ± 14.2 | +5.8 | |
| LDL-C (mg/dL) | t 0 | 152.1 ± 11.1 | 156.4 ± 11.6 | 165.8 ± 11.7 | |||
| t 30 | 157.3 ± 11.3 | +2.7 | 163.5 ± 10.9 | +3.6 | 168.7 ± 10.8 | +1.5 | |
| t 60 | 158.6 ± 13.6 | +3.4 | 164.8 ± 11.2 | +4.3 | 169.7 ± 11.2 | +2.0 | |
| t 90 | 160.0 ± 12.5 | +5.2 | 166.2 ± 11.1 | +6.3 | 172.6 ± 10.7 | +4.1 | |
| HDL-C (mg/dL) | t 0 | 36.7 ± 7.5 | 35.4 ± 6.7 | 38.5 ± 7.2 | |||
| t 30 | 53.6 ± 7.5 * | +46.1 # | 56.2 ± 7.9 * | +58.9 # | 44.3 ± 8.0 * | +15.2 # | |
| t 60 | 54.5 ± 7.0 * | +48.4 # | 57.3 ± 8.1 * | +61.8 # | 45.3 ± 8.3 * | +17.7 # | |
| t 90 | 49.6 ± 6.8 * | +35.1 # | 53.6 ± 7.5 * | +51.4 # | 42.8 ± 7.6 * | +11.1 # | |
| Glucose (mg/dL) | t 0 | 99.1 ± 8.7 | 100.0 ± 8.9 | 107.2 ± 8.5 | |||
| t 30 | 102.0 ± 10.8 | +2.9 | 103.8 ± 12.0 | +3.8 | 109.4 ± 12.4 | +2.1 | |
| t 60 | 102.5 ± 11.6 | +3.4 | 104.5 ± 13.1 | +4.5 | 109.9 ± 10.3 | +2.5 | |
| t 90 | 103.0 ± 12.1 | +3.9 | 105.1 ± 12.4 | +5.1 | 110.2 ± 11.9 | +2.8 | |
| Triglycerides (mg/dL) | t 0 | 180.4 ± 16.8 | 185.2 ± 18.3 | 200.1 ± 19.0 | |||
| t 30 | 185.1 ± 19.3 | +2.6 | 192.2 ± 16.4 | +3.8 | 203.3 ± 21.1 | +1.6 | |
| t 60 | 186.2 ± 14.7 | +3.2 | 193.5 ± 17.3 | +4.5 | 204.5 ± 15.2 | +2.2 | |
| t 90 | 189.0 ± 16.2 | +4.8 | 194.6 ± 17.0 | +5.1 | 206.9 ± 18.7 | +3.4 | |
| TMAO (μM) | t 0 | 2.37 ± 0.04 | 3.01 ± 0.05 | 2.02 ± 0.06 | |||
| t 30 | 1.45 ± 0.02 * | −38.9 # | 1.24 ± 0.06 * | −58.7 # | 1.56 ± 0.07 * | −22.9 # | |
| t 60 | 1.36 ± 0.05 * | −42.3 # | 1.11 ± 0.04 * | −63.1 # | 1.49 ± 0.04 * | −25.8 # | |
| t 90 | 1.54 ± 0.04 * | −35.1 # | 1.50 ± 0.06 * | −50.2 # | 1.66 ± 0.04 * | −17.8 # |
| AAP | Δ (%) | lfAAP | Δ (%) | LAB | Δ (%) | ||
|---|---|---|---|---|---|---|---|
| Bifidobacterium (CFU/mL) | t 0 | 10,499 ± 2458 | 20,341 ± 4316 | 15,239 ± 3104 | |||
| t 30 | 637,289 ± 82,567 * | +6970 # | 62,040 ± 5018 * | +205 # | 335,258 ± 45,128 * | +2100 # | |
| t 60 | 776,961 ± 74,329 * | +7300 # | 70,379 ± 6894 * | +246 # | 396,214 ± 45,219 * | +2500 # | |
| t 90 | 623,640 ± 77,241 * | +5840 # | 57,971 ± 5746 * | +185 # | 274,302 ± 39,489 * | +1700 # | |
| Lactobacillus (CFU/mL) | t 0 | 3584 ± 532 | 2989 ± 387 | 3467 ± 478 | |||
| t 30 | 748,339 ± 64,651 * | +20,780 # | 6127 ± 597 * | +105 # | 124,812 ± 49,731 * | +3500 # | |
| t 60 | 1,078,784 ± 109,657 * | +30,000 # | 6486 ± 529 * | +117 # | 140,413 ± 14,521 * | +3950 # | |
| t 90 | 644,761 ± 58,452 * | +17,890 # | 5843 ± 509 * | +95.5 # | 104,010 ± 23,464 * | +2900 # | |
| Bacteroides (CFU/mL) | t 0 | 7843 ± 755 | 5671 ± 487 | 6891 ± 337 | |||
| t 30 | 3529 ± 550 * | −55.1 # | 4139 ± 364 * | −27.5 # | 5168 ± 499 * | −25.8 # | |
| t 60 | 2901 ± 351 * | −63.2 # | 3856 ± 405 * | −32.1 # | 4410 ± 461 * | −36.0 # | |
| t 90 | 4062 ± 259 * | −48.2 # | 4360 ± 422 * | −23.1 # | 5499 ± 415 * | −20.2 # | |
| Enterococcus (CFU/mL) | t 0 | 6914 ± 419 | 8317 ± 575 | 7819 ± 561 | |||
| t 30 | 6706 ± 731 | −3.7 # | 7651 ± 645 * | −8.4 # | 5082 ± 484 * | −35.5 # | |
| t 60 | 6568 ± 457 | −5.3 # | 7402 ± 534 * | −11.6 # | 4456 ± 379 * | −43.0 # | |
| t 90 | 6713 ± 610 | −2.9 # | 7693 ± 625 * | −7.5 # | 5614 ± 404 * | −28.2 # |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tenore, G.C.; Caruso, D.; Buonomo, G.; D’Avino, M.; Ciampaglia, R.; Maisto, M.; Schisano, C.; Bocchino, B.; Novellino, E. Lactofermented Annurca Apple Puree as a Functional Food Indicated for the Control of Plasma Lipid and Oxidative Amine Levels: Results from a Randomised Clinical Trial. Nutrients 2019, 11, 122. https://doi.org/10.3390/nu11010122
Tenore GC, Caruso D, Buonomo G, D’Avino M, Ciampaglia R, Maisto M, Schisano C, Bocchino B, Novellino E. Lactofermented Annurca Apple Puree as a Functional Food Indicated for the Control of Plasma Lipid and Oxidative Amine Levels: Results from a Randomised Clinical Trial. Nutrients. 2019; 11(1):122. https://doi.org/10.3390/nu11010122
Chicago/Turabian StyleTenore, Gian Carlo, Domenico Caruso, Giuseppe Buonomo, Maria D’Avino, Roberto Ciampaglia, Maria Maisto, Connie Schisano, Bruno Bocchino, and Ettore Novellino. 2019. "Lactofermented Annurca Apple Puree as a Functional Food Indicated for the Control of Plasma Lipid and Oxidative Amine Levels: Results from a Randomised Clinical Trial" Nutrients 11, no. 1: 122. https://doi.org/10.3390/nu11010122