Two-Week Exclusive Supplementation of Modified Ketogenic Nutrition Drink Reserves Lean Body Mass and Improves Blood Lipid Profile in Obese Adults: A Randomized Clinical Trial


Abstract
:1. Introduction
2. Materials and Methods
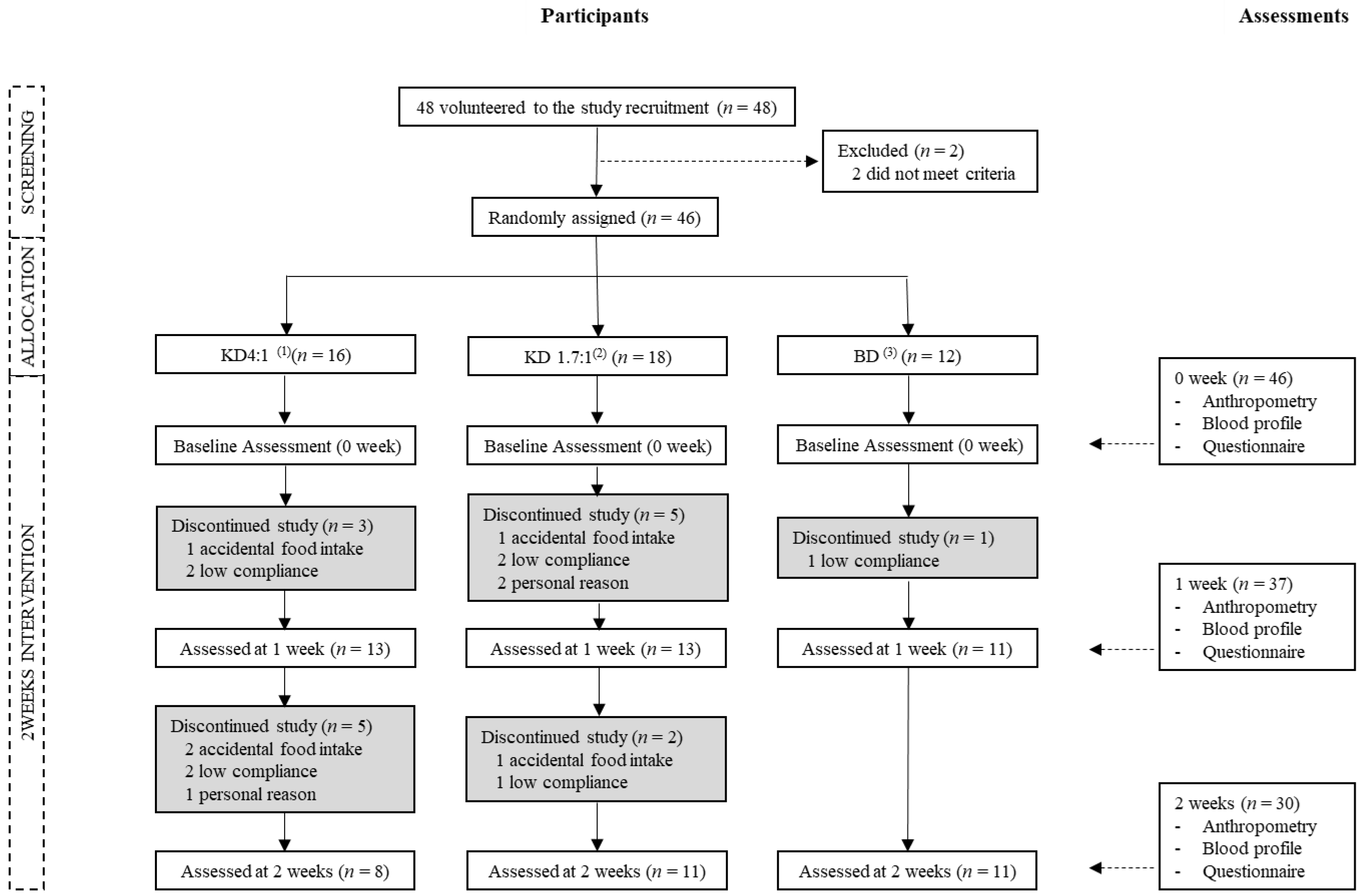
2.1. Study Period and Participants
2.2. Study Design
2.3. Dietary Intervention and Monitoring of Physical Activity
2.3.1. Dietary Intervention through Nutrition Drinks
2.3.2. Monitoring of Physical Activity
2.4. Body Composition and Anthropometric Analysis
2.5. Blood Analysis
2.6. Survey of Physical Symptoms
2.7. Urinary Ketone Bodies
2.8. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Average Intake During the Study Period
3.3. Changes in Body Composition and Anthropometric Measurements
3.4. Changes in Blood Lipids
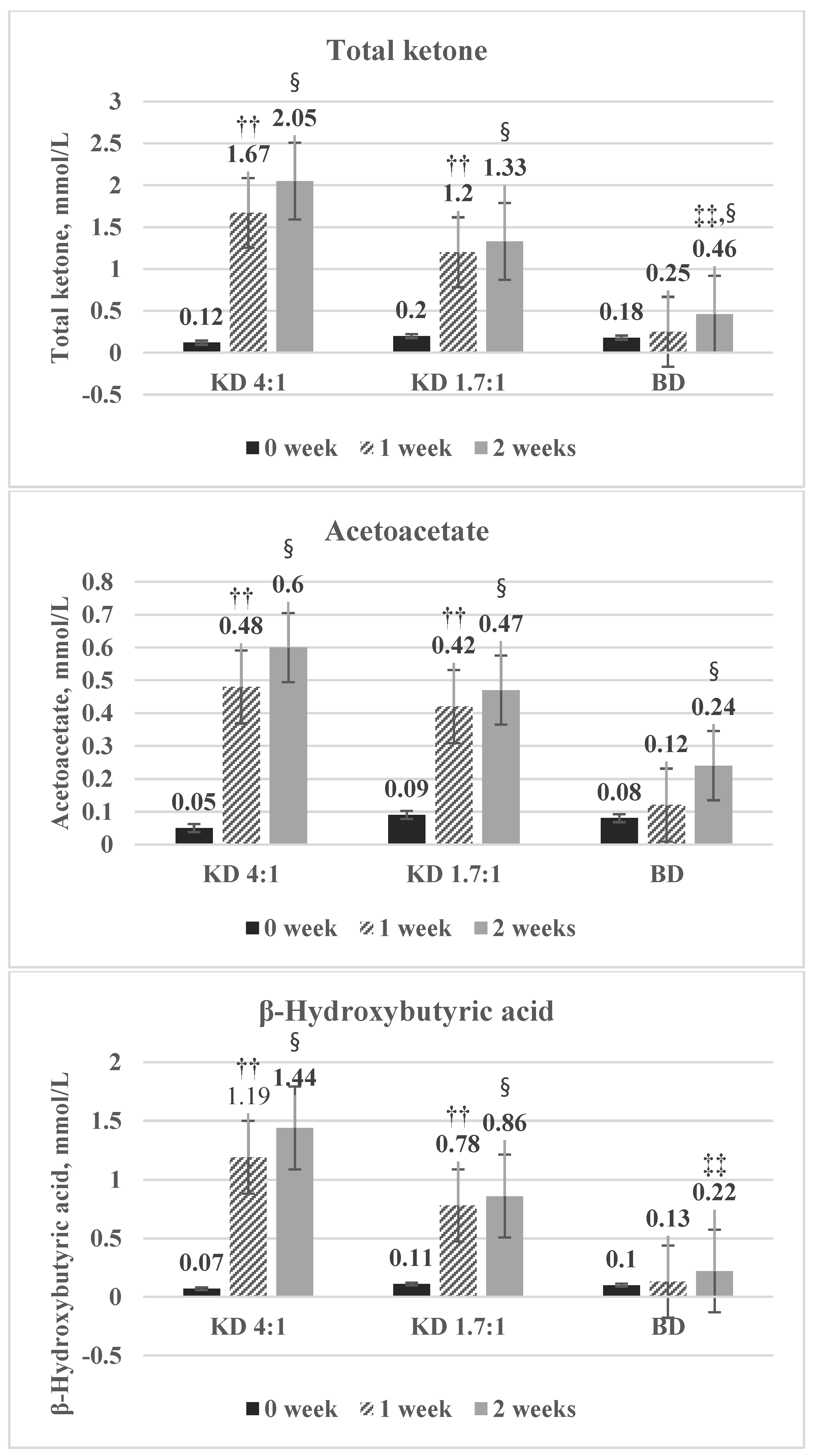
3.5. Changes in Blood Ketone Bodies
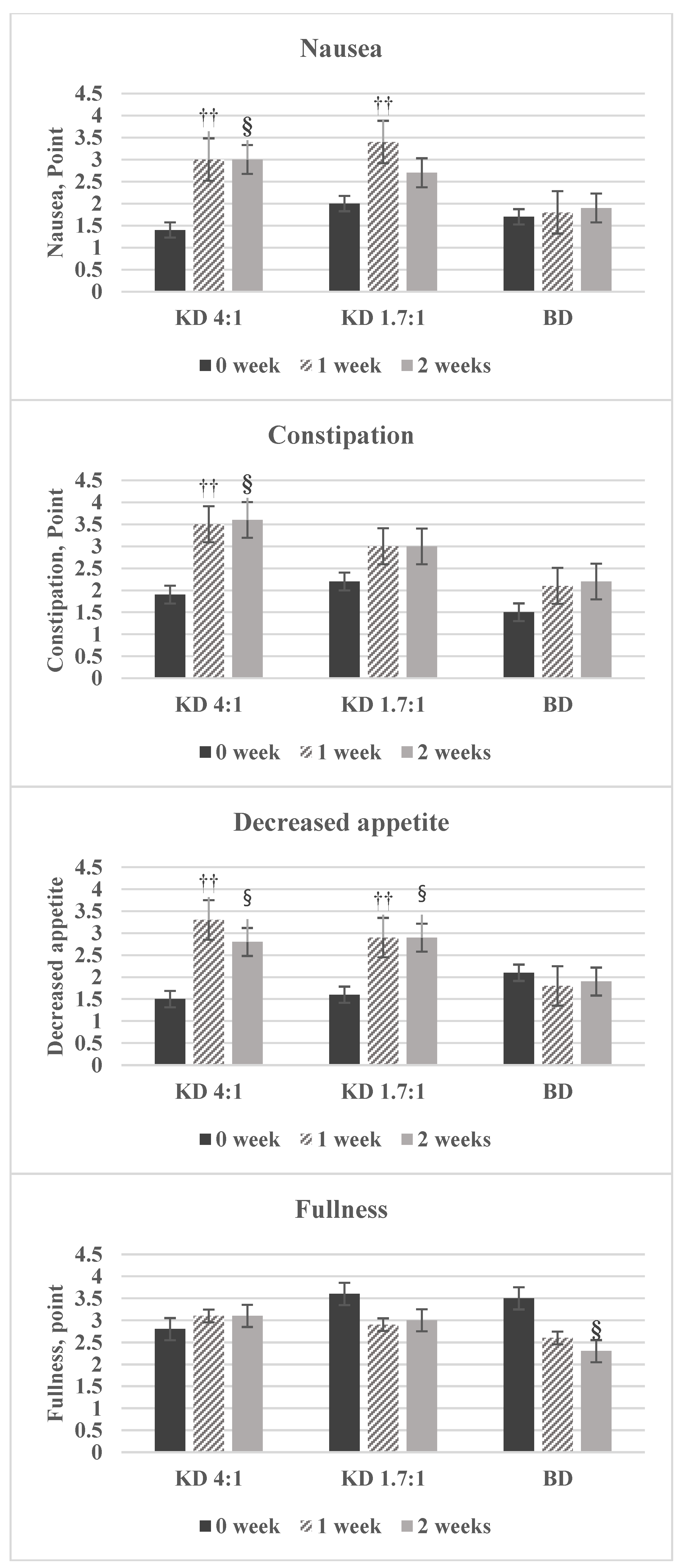
3.6. Changes in Body Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Global Status Report on Noncommunicable Diseases 2014; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Kuczmarski, R.J.; Ogden, C.L.; Grummer-Strawn, L.M.; Flegal, K.M.; Guo, S.S.; Wei, R.; Mei, Z.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. CDC Growth Charts: United States. Adv. Data 2000, 314, 1–27. [Google Scholar]
- Catenacci, V.A.; Wyatt, H.R. The Role of Physical Activity in Producing and Maintaining Weight Loss. Nat. Rev. Endocrinol. 2007, 3, 518. [Google Scholar] [CrossRef] [PubMed]
- Johnston, B.C.; Kanters, S.; Bandayrel, K.; Wu, P.; Naji, F.; Siemieniuk, R.A.; Ball, G.D.; Busse, J.W.; Thorlund, K.; Guyatt, G. Comparison of Weight Loss among Named Diet Programs in Overweight and Obese Adults: A Meta-Analysis. JAMA 2014, 312, 923–933. [Google Scholar] [CrossRef] [PubMed]
- Pi-Sunyer, F.X.; Becker, D.; Bouchard, C.; Carleton, R.; Colditz, G.; Dietz, W.; Foreyt, J.; Garrison, R.; Grundy, S.; Hansen, B. Executive Summary of the Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. J. Am. Diet. Assoc. 1998, 98, 1178–1191. [Google Scholar]
- Heini, A.F.; Weinsier, R.L. Divergent Trends in Obesity and Fat Intake Patterns: The American Paradox. Am. J. Med. 1997, 102, 259–264. [Google Scholar] [CrossRef]
- Willett, W.C.; Leibel, R.L. Dietary Fat is Not a Major Determinant of Body Fat. Am. J. Med. 2002, 113, 47–59. [Google Scholar] [CrossRef]
- Gross, L.S.; Li, L.; Ford, E.S.; Liu, S. Increased Consumption of Refined Carbohydrates and the Epidemic of Type 2 Diabetes in the United States: An Ecologic Assessment. Am. J. Clin. Nutr. 2004, 79, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Park, H. Relationship between Dietary Carbohydrate and Body Weight. J. Korean Soc. Study Obes. 2003, 12, 235–244. [Google Scholar]
- Oh, H.; Ahn, J.; Jun, D.W. Association between a High-Fat Low-Carbohydrate Diet and Non-Alcoholic Fatty Liver Disease: Truth or Myth? Korean J. Med. 2017, 92, 112–117. [Google Scholar] [CrossRef]
- Wilder, R.M. The Effects of Ketonemia on the Course of Epilepsy. Mayo Clin. Proc. 1921, 2, 307–308. [Google Scholar]
- Paoli, A.; Rubini, A.; Volek, J.; Grimaldi, K. Beyond Weight Loss: A Review of the Therapeutic Uses of very-Low-Carbohydrate (Ketogenic) Diets. Eur. J. Clin. Nutr. 2013, 67, 789. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, L.A.; Hu, T.; Reynolds, K.; Yao, L.; Bunol, C.; Liu, Y.; Chen, C.; Klag, M.J.; Whelton, P.K.; He, J. Effects of Low-Carbohydrate and Low-Fat Diets: A Randomized Trial. Ann. Intern. Med. 2014, 161, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Moreno, B.; Bellido, D.; Sajoux, I.; Goday, A.; Saavedra, D.; Crujeiras, A.B.; Casanueva, F.F. Comparison of a very Low-Calorie-Ketogenic Diet with a Standard Low-Calorie Diet in the Treatment of Obesity. Endocrine 2014, 47, 793–805. [Google Scholar] [CrossRef] [PubMed]
- Paoli, A.; Grimaldi, K.; Toniolo, L.; Canato, M.; Bianco, A.; Fratter, A. Nutrition and Acne: Therapeutic Potential of Ketogenic Diets. Skin Pharmacol. Physiol. 2012, 25, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.D.; Li, Y.; Chiuve, S.E.; Stampfer, M.J.; Manson, J.E.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Association of Specific Dietary Fats with Total and Cause-Specific Mortality. JAMA Intern. Med. 2016, 176, 1134–1145. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Mills, K.T.; Yao, L.; Demanelis, K.; Eloustaz, M.; Yancy, W.S., Jr.; Kelly, T.N.; He, J.; Bazzano, L.A. Effects of Low-Carbohydrate Diets Versus Low-Fat Diets on Metabolic Risk Factors: A Meta-Analysis of Randomized Controlled Clinical Trials. Am. J. Epidemiol. 2012, 176, S44–S54. [Google Scholar] [CrossRef] [PubMed]
- Samaha, F.F.; Iqbal, N.; Seshadri, P.; Chicano, K.L.; Daily, D.A.; McGrory, J.; Williams, T.; Williams, M.; Gracely, E.J.; Stern, L. A Low-Carbohydrate as Compared with a Low-Fat Diet in Severe Obesity. N. Engl. J. Med. 2003, 348, 2074–2081. [Google Scholar] [CrossRef] [PubMed]
- Dansinger, M.L.; Gleason, J.A.; Griffith, J.L.; Selker, H.P.; Schaefer, E.J. Comparison of the Atkins, Ornish, Weight Watchers, and Zone Diets for Weight Loss and Heart Disease Risk Reduction: A Randomized Trial. JAMA 2005, 293, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Mifflin, M.D.; St Jeor, S.T.; Hill, L.A.; Scott, B.J.; Daugherty, S.A.; Koh, Y.O. A New Predictive Equation for Resting Energy Expenditure in Healthy Individuals. Am. J. Clin. Nutr. 1990, 51, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare (KR); The Korean Nutrition Society. Dietary Reference Intakes for Koreans 2015; Ministry of Health and Welfare: Sejong, Korea, 2016.
- Accurso, A.; Bernstein, R.K.; Dahlqvist, A.; Draznin, B.; Feinman, R.D.; Fine, E.J.; Gleed, A.; Jacobs, D.B.; Larson, G.; Lustig, R.H. Dietary Carbohydrate Restriction in Type 2 Diabetes Mellitus and Metabolic Syndrome: Time for a Critical Appraisal. Nutr. Metab. 2008, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F. 2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society. J. Am. Coll. Cardiol. 2014, 63, 2985–3023. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Hu, F.B. Popular Weight-Loss Diets: From Evidence to Practice. Nat. Rev. Cardiol. 2007, 4, 34. [Google Scholar] [CrossRef] [PubMed]
- Westerterp-Plantenga, M.; Nieuwenhuizen, A.; Tome, D.; Soenen, S.; Westerterp, K. Dietary Protein, Weight Loss, and Weight Maintenance. Annu. Rev. Nutr. 2009, 29, 21–41. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W. Effects of a Low-Carbohydrate, High-Fat Diet. Korean J. Obes. 2016, 25, 176–183. [Google Scholar] [CrossRef]
- National Heart, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults; National Institutes of Health: Bethesda, MD, USA, 1998. [Google Scholar]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Sumithran, P.; Prendergast, L.A.; Delbridge, E.; Purcell, K.; Shulkes, A.; Kriketos, A.; Proietto, J. Ketosis and Appetite-Mediating Nutrients and Hormones After Weight Loss. Eur. J. Clin. Nutr. 2013, 67, 759. [Google Scholar] [CrossRef] [PubMed]
- Boden, G.; Sargrad, K.; Homko, C.; Mozzoli, M.; Stein, T.P. Effect of a Low-Carbohydrate Diet on Appetite, Blood Glucose Levels, and Insulin Resistance in Obese Patients with Type 2 Diabetes. Ann. Intern. Med. 2005, 142, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, A.M.; Horgan, G.W.; Murison, S.D.; Bremner, D.M.; Lobley, G.E. Effects of a High-Protein Ketogenic Diet on Hunger, Appetite, and Weight Loss in Obese Men Feeding Ad Libitum. Am. J. Clin. Nutr. 2008, 87, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Phillips, K.M.; Ruggio, D.M.; Ashraf-Khorassani, M. Phytosterol Composition of Nuts and Seeds Commonly Consumed in the United States. J. Agric. Food Chem. 2005, 53, 9436–9445. [Google Scholar] [CrossRef] [PubMed]
- Kris-Etherton, P.M.; Pearson, T.A.; Wan, Y.; Hargrove, R.L.; Moriarty, K.; Fishell, V.; Etherton, T.D. High–monounsaturated Fatty Acid Diets Lower both Plasma Cholesterol and Triacylglycerol Concentrations. Am. J. Clin. Nutr. 1999, 70, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Kang, J. Effectiveness and Safety of Low-Carbohydrate Diets. J. Korean Med. Assoc. 2017, 60, 40–46. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| KD4:1 (1) | KD1.7:1 (2) | BD (3) | |
|---|---|---|---|
| Energy (kcal) | 200 | 200 | 200 |
| C:P:F (% of kcal) (4) | 3:7:90 | 4:16:80 | 54:16:30 |
| Carbohydrate (g) (5) | 1.7 | 2.3 | 28.0 |
| Fiber (g) (6) | 0.0 | 0.7 | 1.0 |
| Protein (g) (7) | 3.3 | 8.0 | 8.0 |
| Fat (g) (8) | 20.0 | 17.7 | 7.0 |
| Saturated fat (g) (9) | 4.2 | 0.0 | 2.0 |
| Variables | KD4:1 (3) (n = 13) | KD1.7:1 (4) (n = 13) | BD (5) (n = 11) | p-Value (9) |
|---|---|---|---|---|
| Age (years) | 29.5 ± 9.0 (1) | 24.5 ± 4.8 | 26.0 ± 7.5 | 0.141 |
| Sex (%) | ||||
| Female | 4 (30.8) (2) | 5 (38.5) | 4 (36.4) | 0.739 |
| Male | 9 (69.2) | 8 (61.5) | 7 (63.6) | |
| Height (cm) | 170.3 ± 12.4 | 169.9 ± 10.0 | 171.1 ± 7.6 | 0.962 |
| Body composition | ||||
| Body water (L) | 41.8 ± 8.9 | 41.1 ± 9.1 | 41.7 ± 7.9 | 0.974 |
| Protein (kg) | 11.3 ± 2.5 | 11.2 ± 2.5 | 11.3 ± 2.2 | 0.975 |
| Mineral (kg) | 4.0 ± 0.9 | 4.0 ± 0.9 | 4.0 ± 0.7 | 0.998 |
| Body weight (kg) | 87.3 ± 17.1 | 82.9 ± 14.3 | 85.8 ± 14.8 | 0.764 |
| Skeletal muscle (kg) | 32.2 ± 7.4 | 31.6 ± 7.6 | 32.1 ± 6.5 | 0.974 |
| Body fat mass (kg) | 30.2 ± 10.1 | 26.7 ± 7.3 | 28.8 ± 7.6 | 0.862 |
| BMI (kg/m2) (6) | 30.0 ± 4.2 | 28.5 ± 2.8 | 29.2 ± 4.0 | 0.779 |
| Waist circumference (cm) | 100.0 ± 11.3 | 94.2 ± 7.3 | 96.3 ± 10.1 | 0.318 |
| Hip circumference (cm) | 107.9 ± 7.5 | 108.6 ± 6.2 | 108.7 ± 7.2 | 0.950 |
| Blood lipid profile | ||||
| Total cholesterol (mg/dL) | 184.9 ± 31.2 | 179.8 ± 30.2 | 182.8 ± 28.9 | 0.912 |
| Triglyceride (mg/dL) | 142.4 ± 69.6 | 106.2 ± 45.8 | 101.5 ± 63.4 | 0.218 |
| LDL cholesterol (mg/dL) (7) | 116.2 ± 28.4 | 111.4 ± 31.3 | 120.3 ± 23.3 | 0.742 |
| HDL cholesterol (mg/dL) (8) | 50.8 ± 9.5 | 57.9 ± 11.7 | 52.6 ± 16.0 | 0.331 |
| KD4:1 (2) (n = 8) | KD1.7:1 (3) (n = 11) | BD (4) (n = 11) | p-Value (6) | |
|---|---|---|---|---|
| Energy (kcal) | 1159.1 ± 416.1 (1) | 1280.8 ± 262.2 | 1357.1 ± 292.5 | 0.583 |
| Energy deficit (5) | 799.7 ± 373.2 | 743.8 ± 157.5 | 716.2 ± 94.4 | 0.765 |
| Carbohydrate (g) | 9.7 ± 3.5 c | 14.5 ± 3.0 b | 190.0 ± 40.9 a | 0.000 |
| Fiber (g) | 0.0 ± 0.0 c | 4.3 ± 0.9 b | 6.8 ± 1.5 a | 0.000 |
| Protein (g) | 19.3 ± 6.9 b | 51.2 ± 10.5 a | 54.3 ± 11.7 a | 0.000 |
| Fat (g) | 115.9 ± 41.6 a | 113.6 ± 23.2 a | 47.5 ± 10.2 b | 0.000 |
| Saturated fat (g) | 24.1 ± 8.7 a | 0.0 ± 0.0 c | 13.6 ± 2.9 b | 0.000 |
| KD4:1 (2) | KD1.7:1 (3) | BD (4) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Δ1 week-0 week (5) (n = 13) | Δ2 week-1 week (6) (n = 8) | Δ2 week-0 week (7) (n = 8) | Δ1 week-0 week (5) (n = 13) | Δ2 week-1 week (6) (n = 11) | Δ2 week-0 week (7) (n = 11) | Δ1 week-0 week (5) (n = 11) | Δ2 week-1 week (6) (n = 11) | Δ2 week-0 week (7) (n = 11) | |
| Body water (L) | −2.2 ± 1.3 ∫(1) | −0.5 ± 0.8 | −2.8 ± 1.1 ∫ | −1.1 ± 1.4 † | −0.3 ± 1.0 | −1.5 ± 1.1 ‡ | −1.2 ± 0.7 ∫ | −0.3 ± 0.5 | −1.5 ± 0.8 ∫ |
| Protein (kg) | −0.5 ± 0.3 ∫ | −0.2 ± 0.2 † | −0.7 ± 0.3 ∫ | −0.3 ± 0.4 | −0.1 ± 0.3 | −0.4 ± 0.3 ‡ | −0.3 ± 0.2 ∫ | −0.1 ± 0.2 † | −0.4 ± 0.2 ∫ |
| Mineral (kg) | −0.2 ± 0.1 ∫ | −0.0 ± 0.1 | −0.3 ± 0.1 ‡ | −0.1 ± 0.1 † | −0.0 ± 0.1 | −0.2 ± 0.1 ∫ | −0.1 ± 0.1 ∫ | −0.1 ± 0.1 | −0.2 ± 0.1 ‡ |
| Body weight (kg) | −3.9 ± 1.4 ∫ | −1.7 ± 0.7 ∫ | −5.9 ± 1.8 ∫ | −3.3 ± 1.2 ∫ | −1.0 ± 1.1 † | −4.4 ± 1.5 ∫ | −2.3 ± 1.0 ∫ | −1.1 ± 0.7 ∫ | −3.4 ± 1.3 ∫ |
| Skeletal muscle (kg) | −1.5 ± 1.0 † | −0.4 ± 0.5 † | −2.1 ± 0.8 ∫ | −0.7 ± 1.2 | −0.3 ± 0.8 | −1.0 ± 1.0 ‡ | −0.9 ± 0.5 ∫ | −0.3 ± 0.4 † | −1.2 ± 0.6 ∫ |
| Body fat mass (kg) | −1.1 ± 1.0 † | −1.0 ± 0.8 ‡ | −2.2 ± 1.4 ∫ | −1.8 ± 2.0 ‡ | −0.5 ± 0.8 † | −2.5 ± 1.9 ‡ | −0.8 ± 0.5 ‡ | −0.6 ± 0.6 † | −1.3 ± 0.7 ‡ |
| BMI (kg/m2) (8) | −1.4 ± 0.5 ∫ | −0.5 ± 0.2 ∫ | −2.1 ± 0.6 † | −1.1 ± 0.4 ∫ | −0.3 ± 0.4 † | −1.5 ± 0.5 ∫ | −0.8 ± 0.3 ‡ | −0.4 ± 0.3 ‡ | −1.2 ± 0.4 ‡ |
| Waist circumference (cm) | −3.5 ± 2.5 ∫ | −1.4 ± 1.7 | −4.8 ± 2.1 ∫ | −3.7 ± 2.6 ∫ | −0.8 ± 2.2 | −4.6 ± 3.9 ‡ | −3.0 ± 1.9 ‡ | −1.5 ± 1.7 † | −4.5 ± 2.0 ‡ |
| Hip circumference (cm) | −2.0 ± 1.8 ‡ | −2.0 ± 1.5 ‡ | −3.9 ± 2.0 ‡ | −1.8 ± 1.8 ‡ | −1.1 ± 0.9 ‡ | −3.1 ± 1.0 ∫ | −1.2 ± 0.8 ‡ | −0.9 ± 1.5 | −2.1 ± 1.6 ‡ |
| KD4:1 (2) | KD1.7:1 (3) | BD (4) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Δ1 week-0 week (5) (n = 13) | Δ2 week-1 week (6) (n = 8) | Δ2 week-0 week (7) (n = 8) | Δ1 week-0 week (5) (n = 13) | Δ2 week-1 week (6) (n = 11) | Δ2 week-0 week (7) (n = 11) | Δ1 week-0 week (5) (n = 11) | Δ2 week-1 week (6) (n = 11) | Δ2 week-0 week (7) (n = 11) | |
| Total cholesterol (mg/dL) | 2.5 ± 21.9 (1) | −23.0 ± 15.1 ‡ | −18.3 ± 22.0 | 1.3 ± 18.9 | −18.9 ± 18.2 ‡ | −14.0 ± 13.9 ‡ | 2.6 ± 16.0 | −14.6 ± 17.2 † | −11.9 ± 15.2 † |
| Triglyceride (mg/dL) | −18.4 ± 99.9 | 7.4 ± 57.8 | −27.7 ± 43.9 | −7.9 ± 44.3 | −5.0 ± 30.1 | −14.3 ± 33.9 | −8.4 ± 44.6 | 7.2 ± 22.6 | −1.2 ± 40.9 |
| LDL cholesterol (mg/dL) (8) | 8.2 ± 20.6 | −24.5 ± 15.3 ‡ | −11.6 ± 22.6 | 3.4 ± 17.4 | −15.5 ± 18.2 † | −9.6 ± 13.2 † | 4.6 ± 13.9 | −15.0 ± 14.8 ‡ | −10.4 ± 9.2 ‡ |
| HDL cholesterol (mg/dL) (9) | −1.5 ± 10.6 | 0.6 ± 6.8 | −0.6 ± 13.7 | −2.8 ± 5.9 | −0.1 ± 3.8 | −2.3 ± 3.8 | −0.8 ± 6.8 | −2.9 ± 3.2 † | −3.7 ± 8.2 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.-R.; Kim, J.; Lim, H.; Park, Y.K. Two-Week Exclusive Supplementation of Modified Ketogenic Nutrition Drink Reserves Lean Body Mass and Improves Blood Lipid Profile in Obese Adults: A Randomized Clinical Trial. Nutrients 2018, 10, 1895. https://doi.org/10.3390/nu10121895
Choi H-R, Kim J, Lim H, Park YK. Two-Week Exclusive Supplementation of Modified Ketogenic Nutrition Drink Reserves Lean Body Mass and Improves Blood Lipid Profile in Obese Adults: A Randomized Clinical Trial. Nutrients. 2018; 10(12):1895. https://doi.org/10.3390/nu10121895
Chicago/Turabian StyleChoi, Hae-Ryeon, Jinmin Kim, Hyojung Lim, and Yoo Kyoung Park. 2018. "Two-Week Exclusive Supplementation of Modified Ketogenic Nutrition Drink Reserves Lean Body Mass and Improves Blood Lipid Profile in Obese Adults: A Randomized Clinical Trial" Nutrients 10, no. 12: 1895. https://doi.org/10.3390/nu10121895