An Active Lifestyle Reinforces the Effect of a Healthy Diet on Cognitive Function: A Population-Based Longitudinal Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Dementia Diagnosis and Cognitive Function Test
2.4. Assessment of Diet
2.5. Assessment of Leisure Activities
2.6. Statistical Methods
3. Results
3.1. Characteristics of the Study Population
3.2. Associations between the NPDP and Leisure Activities with MMSE Change
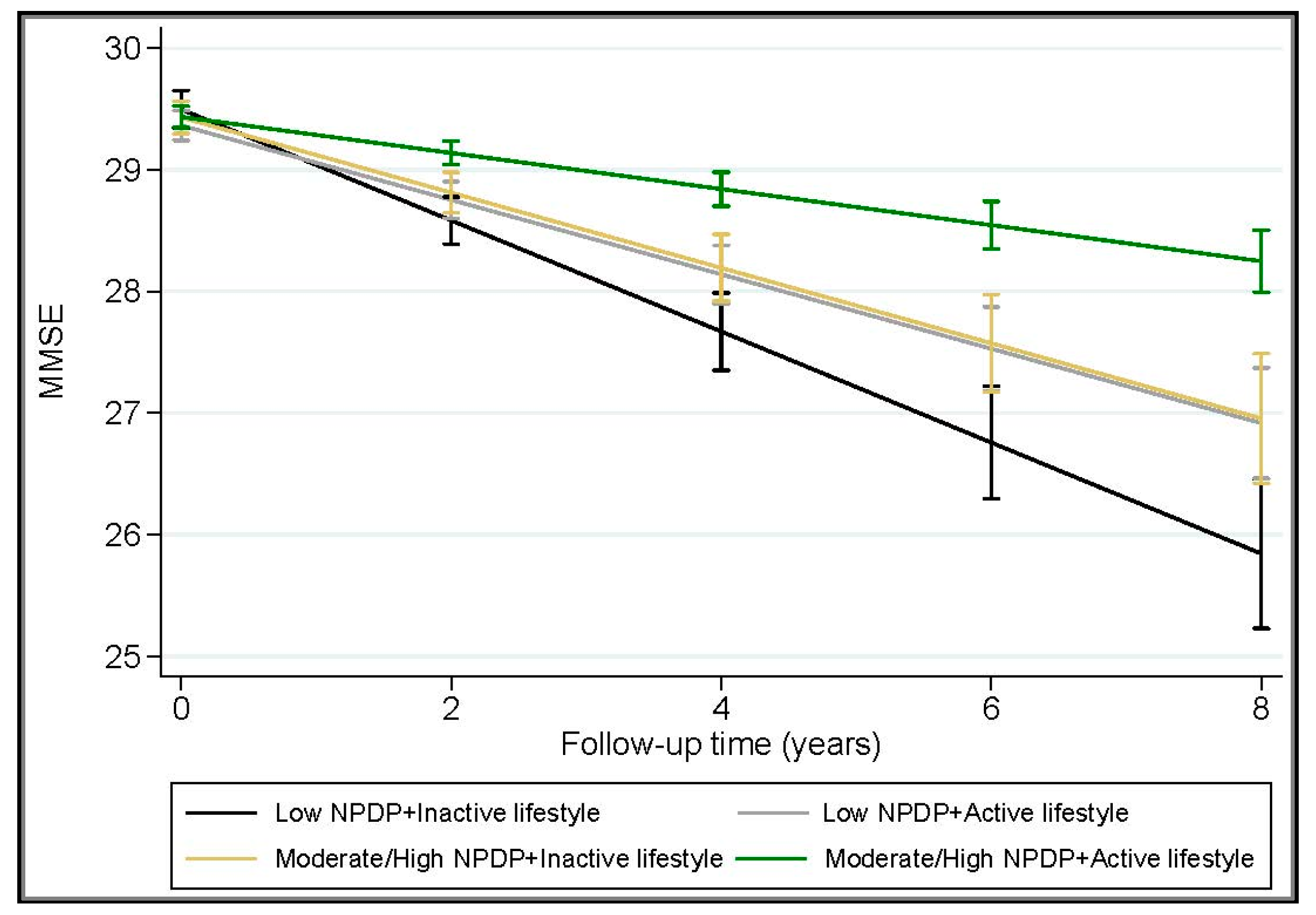
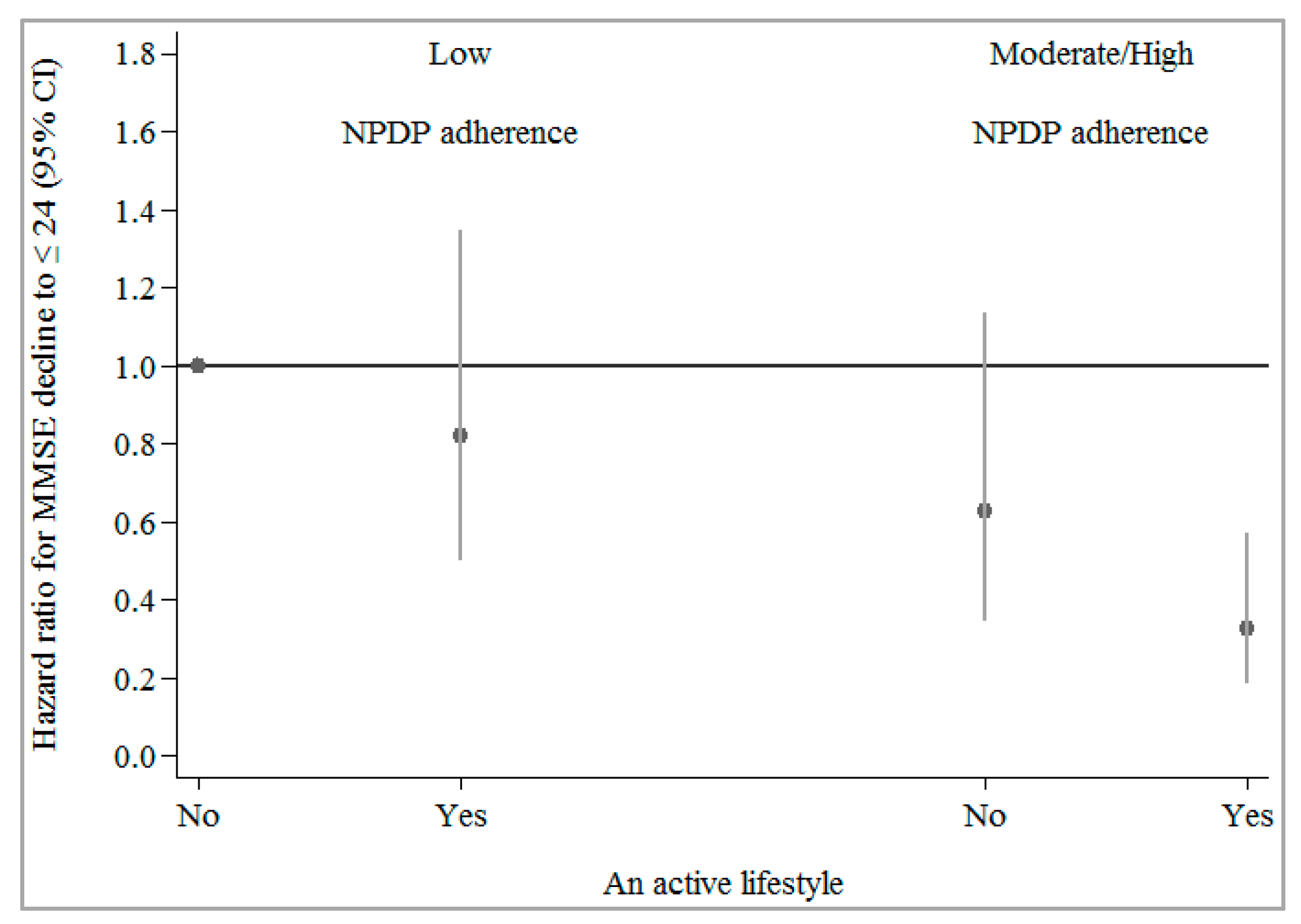
3.3. Joint Effect of Healthy Diet and Leisure Activities on MMSE Decline
3.4. Supplementary Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Barnes, D.E.; Yaffe, K. The projected effect of risk factor reduction on Alzheimer’s disease prevalence. Lancet Neurol. 2011, 10, 819–828. [Google Scholar] [CrossRef]
- Schreiber, S.; Vogel, J.; Schwimmer, H.D.; Marks, S.M.; Schreiber, F.; Jagust, W. Impact of lifestyle dimensions on brain pathology and cognition. Neurobiol. Aging 2016, 40, 164–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sofi, F.; Valecchi, D.; Bacci, D.; Abbate, R.; Gensini, G.F.; Casini, A.; Macchi, C. Physical activity and risk of cognitive decline: A meta-analysis of prospective studies. J. Intern. Med. 2011, 269, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Stern, C.; Munn, Z. Cognitive leisure activities and their role in preventing dementia: A systematic review. Int. J. Evid. Based Healthc. 2010, 8, 2–17. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.X.; Xu, W.L.; Pei, J.J. Leisure activities, cognition and dementia. Biochim. Biophys. Acta 2012, 1822, 482–491. [Google Scholar] [CrossRef] [PubMed]
- Safouris, A.; Tsivgoulis, G.; Sergentanis, T.N.; Psaltopoulou, T. Mediterranean Diet and Risk of Dementia. Curr. Alzheimer Res. 2015, 12, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Gardener, S.; Gu, Y.; Rainey-Smith, S.; Keogh, J.; Clifton, P.; Mathieson, S.L.; Taddei, K.; Mondal, A.; Ward, V.; Scarmeas, N.; et al. Adherence to a Mediterranean diet and Alzheimer’s disease risk in an Australian population. Transl. Psychiatry 2012, 2, e164. [Google Scholar] [CrossRef] [PubMed]
- Van de Rest, O.; Berendsen, A.A.; Haveman-Nies, A.; de Groot, L.C. Dietary patterns, cognitive decline, and dementia: A systematic review. Adv. Nutr. 2015, 6, 154–168. [Google Scholar] [CrossRef] [PubMed]
- Cherbuin, N.; Anstey, K.J. The Mediterranean diet is not related to cognitive change in a large prospective investigation: The PATH Through Life study. Am. J. Geriatr. Psychiatry 2012, 20, 635–639. [Google Scholar] [CrossRef] [PubMed]
- Titova, O.E.; Ax, E.; Brooks, S.J.; Sjögren, P.; Cederholm, T.; Kilander, L.; Kullberg, J.; Larsson, E.M.; Johansson, L.; Ahlström, H.; et al. Mediterranean diet habits in older individuals: Associations with cognitive functioning and brain volumes. Exp. Gerontol. 2013, 48, 1443–1448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samieri, C.; Okereke, O.I.; Devore, E.E.; Grodstein, F. Long-term adherence to the Mediterranean diet is associated with overall cognitive status, but not cognitive decline, in women. J. Nutr. 2013, 143, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y. Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol. 2012, 11, 1006–1012. [Google Scholar] [CrossRef]
- Norton, M.C.; Dew, J.; Smith, H.; Fauth, E.; Piercy, K.W.; Breitner, J.C.; Tschanz, J.; Wengreen, H.; Welsh-Bohmer, K. Cache County Investigators. Lifestyle behavior pattern is associated with different levels of risk for incident dementia and Alzheimer’s disease: The Cache County study. J. Am. Geriatr. Soc. 2012, 60, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Scarmeas, N.; Luchsinger, J.A.; Schupf, N.; Brickman, A.M.; Cosentino, S.; Tang, M.X.; Stern, Y. Physical activity, diet, and risk of Alzheimer disease. JAMA 2009, 302, 627–637. [Google Scholar] [CrossRef] [PubMed]
- Shakersain, B.; Rizzuto, D.; Larsson, S.C.; Faxén-Irving, G.; Fatborn, J.; Fratiglioni, L.; Xu, W.L. The Nordic Prudent Diet Reduces Risk of Cognitive Decline in the Swedish Older Adults: A Population-Based Cohort Study. Nutrients 2018, 10, 229. [Google Scholar] [CrossRef] [PubMed]
- Shakersain, B.; Santoni, G.; Larsson, S.C.; Faxén-Irving, G.; Fratiglioni, L.; Xu, W. Prudent diet may attenuate the adverse effects of Western diet on cognitive decline. Alzheimers Dement. 2016, 12, 100–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fratiglioni, L.; Viitanen, M.; Backman, L.; Sandman, P.O.; Winblad, B. Occurrence of dementia in advanced age: The study design of the Kungsholmen Project. Neuroepidemiology 1992, 11, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Lazek, M.D.; Howieson, D.B.; Bigler, E.D.; Tranel, D. Neuropsychological Assessment, 5th ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Johansson, I.; Hallmans, G.; Wikman, A.; Biessy, C.; Riboli, E.; Kaaks, R. Validation and calibration of food-frequency questionnaire measurements in the Northern Sweden Health and Disease cohort. Public Health Nutr. 2002, 5, 487–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neafsey, E.J.; Collins, M.A. Moderate alcohol consumption and cognitive risk. Neuropsychiatr. Dis. Treat. 2011, 7, 465–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.X.; Karp, A.; Winblad, B.; Fratiglioni, L. Late-life engagement in social and leisure activities is associated with a decreased risk of dementia: A longitudinal study from the Kungsholmen project. Am. J. Epidemiol. 2002, 155, 1081–1087. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.X.; Jin, Y.; Hendrie, H.C.; Liang, C.; Yang, L.; Cheng, Y. Late life leisure activities and risk of cognitive decline. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Azur, M.J.; Stuart, E.A.; Frangakis, C.; Leaf, P.J. Multiple imputation by chained equations: What is it and how does it work? Int. J. Methods Psychiatr. Res. 2011, 20, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Valls-Pedret, C.; Sala-Vila, A.; Serra-Mir, M.; Corella, D.; de la Torre, R.; Martínez-González, M.Á.; Martínez-Lapiscina, E.H.; Fitó, M.; Pérez-Heras, A.; Salas-Salvadó, J.; et al. Mediterranean Diet and Age-Related Cognitive Decline: A Randomized Clinical Trial. JAMA Intern. Med. 2015, 175, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.J.; Blumenthal, J.A.; Babyak, M.A.; Corella, D.; de la Torre, R.; Martínez-González, M.Á.; Martínez-Lapiscina, E.H.; Fitó, M.; Pérez-Heras, A.; Salas-Salvadó, J.; et al. Effects of the dietary approaches to stop hypertension diet, exercise, and caloric restriction on neurocognition in overweight adults with high blood pressure. Hypertension 2010, 55, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Barnes, L.L.; Bennett, D.A.; Aggarwal, N.T. MIND diet slows cognitive decline with aging. Alzheimers Dement. 2015, 11, 1015–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blondell, S.J.; Hammersley-Mather, R.; Veerman, J.L. Does physical activity prevent cognitive decline and dementia? A systematic review and meta-analysis of longitudinal studies. BMC Public Health 2014, 14, 510. [Google Scholar] [CrossRef] [PubMed]
- Fratiglioni, L.; Paillard-Borg, S.; Winblad, B. An active and socially integrated lifestyle in late life might protect against dementia. Lancet Neurol. 2004, 3, 343–353. [Google Scholar] [CrossRef]
- Antoniou, M.; Gunasekera, G.M.; Wong, P.C. Foreign language training as cognitive therapy for age-related cognitive decline: A hypothesis for future research. Neurosci. Biobehav. Rev. 2013, 37, 2689–2698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karp, A.; Paillard-Borg, S.; Wang, H.X.; Silverstein, M.; Winblad, B.; Fratiglioni, L. Mental, physical and social components in leisure activities equally contribute to decrease dementia risk. Dement. Geriatr. Cogn. Disord. 2006, 21, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Jhamnani, S.; Patel, D.; Heimlich, L.; King, F.; Walitt, B.; Lindsay, J. Meta-analysis of the effects of lifestyle modifications on coronary and carotid atherosclerotic burden. Am. J. Cardiol. 2015, 115, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Rafnsson, S.B.; Dilis, V.; Trichopoulou, A. Antioxidant nutrients and age-related cognitive decline: A systematic review of population-based cohort studies. Eur. J. Nutr. 2013, 52, 1553–1567. [Google Scholar] [CrossRef] [PubMed]
- Orhan, I.E.; Daglia, M.; Nabavi, S.F.; Loizzo, M.R.; Sobarzo-Sánchez, E.; Nabavi, S.M. Flavonoids and dementia: An update. Curr. Med. Chem. 2015, 22, 1004–1015. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.; Ying, Z.; Gomez-Pinilla, F. Docosahexaenoic acid dietary supplementation enhances the effects of exercise on synaptic plasticity and cognition. Neuroscience 2008, 155, 751–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez-Pinilla, F. The combined effects of exercise and foods in preventing neurological and cognitive disorders. Prev. Med. 2011, 52, S75–S80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arenaza-Urquijo, E.M.; Wirth, M.; Chetelat, G. Cognitive reserve and lifestyle: Moving towards preclinical Alzheimer’s disease. Front. Aging Neurosci. 2015, 7, 134. [Google Scholar] [CrossRef] [PubMed]
- Keogh, R.H.; White, I.R. A toolkit for measurement error correction, with a focus on nutritional epidemiology. Stat. Med. 2014, 33, 2137–2155. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Adherence to NPDP | p-Value * | ||
|---|---|---|---|---|
| Low (n = 720) | Moderate (n = 779) | High (n = 724) | ||
| NPDP score range | 8 to 29 | 29 to 38 | 38 to 62 | |
| Age, years | 72.7 (66.3 to 81.3) | 67.0 (60.8 to 78.3) * | 66.2 (60.5 to 72.3) * | <0.001 |
| Sex, women | 437 (60.6) | 474 (60.8) | 442 (61.0) | 0.985 |
| Education | <0.001 | |||
| University | 193 (26.8) | 283 (36.3) | 337 (46.6) | |
| High school | 330 (45.8) | 344 (44.2) | 300 (41.4) | |
| Elementary school | 197 (27.4) | 152 (19.5) | 87 (12.0) | |
| Civil status | <0.001 | |||
| Married | 315 (43.7) | 406 (52.0) | 417 (57.6) | |
| Single | 124 (17.3) | 126 (16.2) | 110 (15.1) | |
| Widow/Divorced | 281 (39.0) | 247 (31.8) | 197 (27.3) | |
| Smoking | <0.001 | |||
| Never | 343 (47.7) | 341 (43.7) | 291 (40.1) | |
| Former | 234 (32.5) | 329 (42.3) | 347 (47.9) | |
| Current | 143 (19.8) | 109 (14.0) | 87 (12.0) | |
| Smoking (duration) | 35 (19 to 45) | 29 (15 to 42) | 25 (15 to 38) | <0.001 |
| Physical activity | <0.001 | |||
| Low | 165 (22.9) | 133 (17.0) | 92 (12.7) | |
| Moderate | 428 (59.5) | 431 (55.4) | 390 (53.9) | |
| Intense | 127 (17.6) | 215 (27.6) | 242 (33.4) | |
| Mental activity | <0.001 | |||
| Low | 364 (50.5) | 278 (34.8) | 180 (24.8) | |
| Moderate | 247 (34.3) | 322 (40.3) | 281 (38.8) | |
| Intense | 109 (15.2) | 199 (24.9) | 263 (36.4) | |
| Social activity | 0.001 | |||
| Low | 466 (64.8) | 503 (63.0) | 393 (54.2) | |
| Moderate | 162 (22.5) | 190 (23.8) | 204 (28.2) | |
| High | 92 (12.7) | 106 (13.2) | 127 (17.6) | |
| BMI, kg/m2 | 25.0 (22.9 to 27.7) | 25.5 * (23.2 to 27.9) | 26.2 * (23.8 to 28.7) | <0.001 |
| MMSE | 29 (28 to 30) | 29 (29 to 30) | 29 (29 to 30) | 1.000 |
| Vascular disorders † | 646 (89.8) | 704 (88.1) | 614 (84.8) * | 0.014 |
| Other chronic diseases ‡ | 297 (41.3) | 328 (41.1) | 267 (36.9) | 0.168 |
| Any APOE ɛ4 allele carriage | 217 (30.2) | 214 (26.8) | 222 (30.6) | 0.279 |
| Dietary supplement use | 211 (29.3) | 216 (27.0) | 197 (27.1) | 0.550 |
| Total energy intake, kcal/day | 1620.0 (1289.0 to 2035.5) | 1571.1 (1235.3 to 1937.9) | 1628.8 (1324.4 to 1968.7) | 0.984 |
| Deaths at follow-ups | 192 (26.7) | 136 (17.4) | 71 (9.8) | <0.001 |
| Lifestyle Factors | n | β (95% CI) | |||
|---|---|---|---|---|---|
| Model 1 * | p-Value | Model 2 † | p-Value | ||
| Adherence to NPDP | |||||
| Low | 720 | Reference | Reference | ||
| Moderate-to-high | 1503 | 0.19 (0.13 to 0.25) | <0.001 | 0.19 (0.14 to 0.24) | <0.001 |
| Moderate | 779 | 0.14 (0.08 to 0.21) | <0.001 | 0.14 (0.08 to 0.20) | <0.001 |
| High | 724 | 0.24 (0.18 to 0.31) | <0.001 | 0.24 (0.18 to 0.30) | <0.001 |
| p-value for trend | 0.12 (0.09 to 0.15) | <0.001 | 0.12 (0.09 to 0.15) | <0.001 | |
| Physical Activity | |||||
| Low | 390 | Reference | Reference | ||
| Moderate-to-intense | 1833 | 0.13 (0.06 to 0.20) | <0.001 | 0.13 (0.07 to 0.20) | <0.001 |
| Moderate | 1249 | 0.11 (0.03 to 0.18) | 0.005 | 0.11 (0.04 to 0.18) | 0.003 |
| Intense | 584 | 0.18 (0.10 to 0.26) | <0.001 | 0.19 (0.11 to 0.26) | <0.001 |
| p-value for trend | 0.09 (0.05 to 0.13) | <0.001 | 0.09 (0.05 to 0.13) | <0.001 | |
| Mental Activity | |||||
| Low | 815 | Reference | Reference | ||
| Moderate-to-intense | 1408 | 0.15 (0.09 to 0.22) | <0.001 | 0.15 (0.09 to 0.21) | <0.001 |
| Moderate | 842 | 0.11 (0.03 to 0.18) | 0.006 | 0.10 (0.03 to 0.18) | 0.006 |
| Intense | 566 | 0.22 (0.15 to 0.29) | <0.001 | 0.22 (0.15 to 0.29) | <0.001 |
| p-value for trend | 0.11 (0.07 to 0.14) | <0.001 | 0.11 (0.07 to 0.14) | <0.001 | |
| Social Activity | |||||
| Low | 1349 | Reference | Reference | ||
| Moderate-to-intense | 874 | 0.09 (0.04 to 0.15) | 0.001 | 0.09 (0.04 to 0.14) | <0.001 |
| Moderate | 552 | 0.08 (0.01 to 0.14) | 0.019 | 0.08 (0.02 to 0.14) | 0.011 |
| Intense | 322 | 0.12 (0.04 to 0.20) | 0.003 | 0.12 (0.04 to 0.19) | 0.003 |
| p-value for trend | 0.06 (0.03 to 0.10) | 0.001 | 0.06 (0.03 to 0.10) | <0.001 | |
| Leisure Activity Score | |||||
| 0 (Inactive) | 614 | Reference | Reference | ||
| ≥1 (Active) | 1609 | 0.20 (0.14 to 0.26) | <0.001 | 0.20 (0.14 to 0.26) | <0.001 |
| 1 | 1269 | 0.18 (0.12 to 0.25) | <0.000 | 0.18 (0.12 to 0.25) | <0.001 |
| 2 | 340 | 0.26 (0.18 to 0.34) | <0.001 | 0.26 (0.18 to 0.34) | <0.001 |
| p-value for trend | 0.14 (0.10 to 0.18) | <0.001 | 0.14 (0.10 to 0.18) | <0.001 | |
| Joint Exposure | n | Model 1 * | p-Value | Model 2 † | p-Value | |
|---|---|---|---|---|---|---|
| Physical Activity | NPDP Adherence | β (95% CI) | β (95% CI) | |||
| Low | Low | 165 | Reference | Reference | ||
| Moderate/intense | Low | 554 | 0.18 (0.05 to 0.31) | 0.007 | 0.18 (0.05 to 0.30) | 0.005 |
| Low | Moderate/high | 224 | 0.28 (0.12 to 0.43) | 0.001 | 0.27 (0.12 to 0.42) | 0.001 |
| Moderate/intense | Moderate/high | 1280 | 0.34 (0.23 to 0.46) | <0.001 | 0.34 (0.23 to 0.45) | <0.001 |
| p-value for trend | 0.09 (0.07 to 0.12) | <0.001 | 0.09 (0.07 to 0.12) | <0.001 | ||
| Mental Activity | NPDP Adherence | |||||
| Low | Low | 362 | Reference | Reference | ||
| Moderate/intense | Low | 357 | 0.14 (0.04 to 0.24) | 0.006 | 0.13 (0.02 to 0.24) | 0.016 |
| Low | Moderate/high | 452 | 0.18 (0.09 to 0.27) | <0.001 | 0.18 (0.09 to 0.26) | <0.001 |
| Moderate/intense | Moderate/high | 1052 | 0.30 (0.22 to 0.37) | <0.001 | 0.29 (0.21 to 0.37) | <0.001 |
| p-value for trend | 0.09 (0.07 to 0.12) | <0.001 | 0.09 (0.07 to 0.12) | <0.001 | ||
| Social Activity | NPDP Adherence | |||||
| Low | Low | 467 | Reference | Reference | ||
| Moderate/intense | Low | 252 | 0.10 (−0.02 to 0.21) | 0.097 | 0.10 (−0.01 to 0.20) | 0.066 |
| Low | Moderate/high | 883 | 0.19 (0.12 to 0.27) | <0.001 | 0.19 (0.12 to 0.27) | <0.001 |
| Moderate/intense | Moderate/high | 621 | 0.27 (0.19 to 0.34) | <0.001 | 0.27 (0.19 to 0.34) | <0.001 |
| p-value for trend | 0.09 (0.07 to 0.11) | <0.001 | 0.09 (0.07 to 0.11) | <0.001 | ||
| Leisure Activity Score | NPDP Adherence | |||||
| 0 (Inactive) | Low | 275 | Reference | Reference | ||
| ≥1 (Active) | Low | 445 | 0.17 (0.06 to 0.29) | 0.003 | 0.17 (0.06 to 0.28) | 0.003 |
| 0 (Inactive) | Moderate/high | 339 | 0.16 (0.05 to 0.28) | 0.007 | 0.16 (0.05 to 0.28) | 0.006 |
| ≥1 (Active) | Moderate/high | 1164 | 0.33 (0.24 to 0.42) | <0.001 | 0.33 (0.24 to 0.42) | <0.001 |
| p-value for trend | 0.07 (0.05 to 0.08) | <0.001 | 0.07 (0.05 to 0.08) | <0.001 | ||
| Joint Exposure | n | Model 1 * | p-Value | Model 2 † | p-Value | |
|---|---|---|---|---|---|---|
| Physical Activity | NPDP Adherence | HR (95% CI) | HR (95% CI) | |||
| Low | Low | 165 | Reference | Reference | ||
| Moderate/intense | Low | 554 | 0.62 (0.38 to 1.02) | 0.058 | 0.80 (0.48 to 1.33) | 0.394 |
| Low | Moderate/high | 224 | 0.28 (0.12 to 0.63) | 0.002 | 0.55 (0.24 to 1.27) | 0.160 |
| Moderate/intense | Moderate/high | 1280 | 0.16 (0.09 to 0.27) | <0.001 | 0.39 (0.22 to 0.67) | 0.001 |
| p-value for trend | 0.53 (0.45 to 0.62) | <0.001 | 0.72 (0.61 to 0.85) | <0.001 | ||
| Mental Activity | NPDP Adherence | |||||
| Low | Low | 362 | Reference | Reference | ||
| Moderate/intense | Low | 357 | 0.73 (0.46 to 1.17) | 0.189 | 1.04 (0.63 to 1.71) | 0.884 |
| Low | Moderate/high | 452 | 0.37 (0.22 to 0.62) | <0.001 | 0.63 (0.37 to 1.09) | 0.096 |
| Moderate/intense | Moderate/high | 1052 | 0.16 (0.09 to 0.27) | <0.001 | 0.40 (0.22 to 0.73) | 0.003 |
| p-value for trend | 0.55 (0.47 to 0.64) | <0.001 | 0.74 (0.62 to 0.87) | <0.001 | ||
| Social Activity | NPDP Adherence | |||||
| Low | Low | 467 | Reference | Reference | ||
| Moderate/intense | Low | 252 | 0.69 (0.41 to 1.17) | 0.170 | 0.83 (0.49 to 1.41) | 0.498 |
| Low | Moderate/high | 883 | 0.31 (0.21 to 0.48) | <0.001 | 0.57 (0.37 to 0.88) | 0.011 |
| Moderate/intense | Moderate/high | 621 | 0.11 (0.06 to 0.22) | <0.001 | 0.28 (0.14 to 0.57) | <0.001 |
| p-value for trend | 0.52 (0.44 to 0.61) | <0.001 | 0.70 (0.59 to 0.83) | <0.001 | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shakersain, B.; Rizzuto, D.; Wang, H.-X.; Faxén-Irving, G.; Prinelli, F.; Fratiglioni, L.; Xu, W. An Active Lifestyle Reinforces the Effect of a Healthy Diet on Cognitive Function: A Population-Based Longitudinal Study. Nutrients 2018, 10, 1297. https://doi.org/10.3390/nu10091297
Shakersain B, Rizzuto D, Wang H-X, Faxén-Irving G, Prinelli F, Fratiglioni L, Xu W. An Active Lifestyle Reinforces the Effect of a Healthy Diet on Cognitive Function: A Population-Based Longitudinal Study. Nutrients. 2018; 10(9):1297. https://doi.org/10.3390/nu10091297
Chicago/Turabian StyleShakersain, Behnaz, Debora Rizzuto, Hui-Xin Wang, Gerd Faxén-Irving, Federica Prinelli, Laura Fratiglioni, and Weili Xu. 2018. "An Active Lifestyle Reinforces the Effect of a Healthy Diet on Cognitive Function: A Population-Based Longitudinal Study" Nutrients 10, no. 9: 1297. https://doi.org/10.3390/nu10091297