The Effect of Whey Protein Supplementation on the Temporal Recovery of Muscle Function Following Resistance Training: A Systematic Review and Meta-Analysis




Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy and Study Selection
2.3. Data Extraction
3. Analysis
3.1. Study Quality
3.2. Meta-Analysis
4. Results
4.1. Study Quality and Content
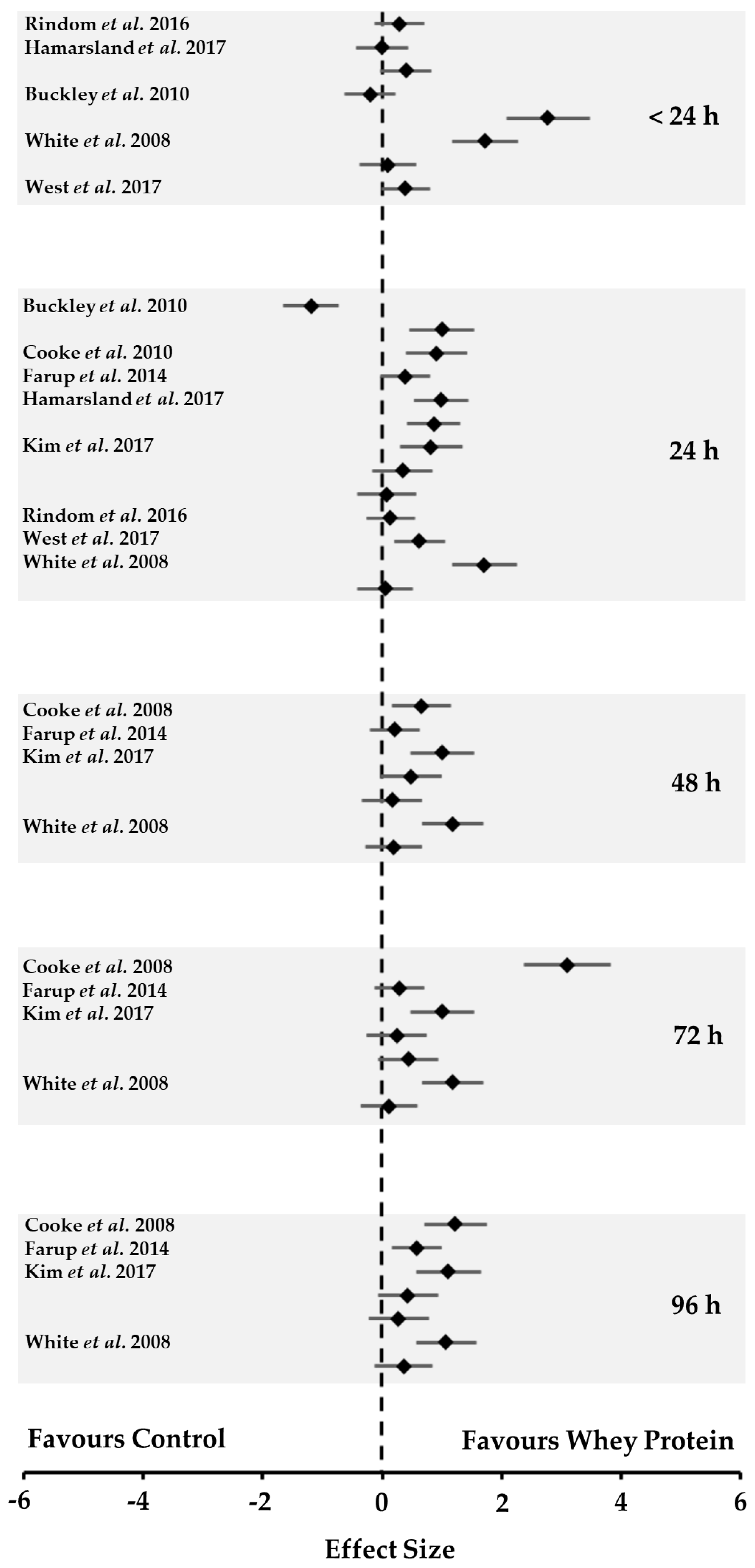
4.2. Muscle Function
4.3. Supplementation Strategy
4.4. Resistance Training Intervention
5. Discussion
5.1. Experimental Approaches to the Problem
5.2. Supplementation Strategy
5.3. Other Considerations
6. Conclusions
Acknowledgments
Author Contributions
Conflict of Interest
References
- Jones, D.A.; Rutherford, O.M.; Parker, D.F. Physiological changes in skeletal muscle as a result of strength training. Q. J. Exp. Physiol. 1989, 74, 233–256. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.; Byrne, R. The effect of exercise-induced muscle damage on isometric and dynamic knee extensor strength and vertical jump performance. J. Sports Sci. 2002, 20, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Warren, G.L.; Lowe, D.A.; Armstrong, R.B. Measurement tools used in the study of eccentric contraction-induced injury. Sports Med. 1999, 27, 43–59. [Google Scholar] [CrossRef] [PubMed]
- Atherton, P.J.; Smith, K. Muscle protein synthesis in response to nutrition and exercise. J. Physiol. 2012, 590, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- West, D.W.; Burd, N.A.; Coffey, V.G.; Baker, S.K.; Burke, L.M.; Hawley, J.A.; Moore, D.R.; Stellingwerff, T.; Phillips, S.M. Rapid aminoacidemia enhances myofibrillar protein synthesis and anabolic intramuscular signaling responses after resistance exercise. Am. J. Clin. Nutr. 2011, 94, 795–803. [Google Scholar] [CrossRef] [PubMed]
- Morton, R.W.; Murphy, K.T.; McKellar, S.R.; Schoenfeld, B.J.; Henselmans, M.; Helms, E.; Aragon, A.A.; Devries, M.C.; Banfield, L.; Krieger, J.W.; et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br. J. Sports Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Witard, O.C.; Jackman, S.R.; Breen, L.; Smith, K.; Selby, A.; Tipton, K.D. Myofibrillar muscle protein synthesis rates subsequent to a meal in response to increasing doses of whey protein at rest and after resistance exercise. Am. J. Clin. Nutr. 2014, 99, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.E.; Moore, D.R.; Kujbida, G.W.; Tarnopolsky, M.A.; Phillips, S.M. Ingestion of whey hydrolysate, casein, or soy protein isolate: Effects on mixed muscle protein synthesis at rest and following resistance exercise in young men. J. Appl. Physiol. 2009, 107, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Buckley, J.D.; Thompson, R.L.; Coates, A.M.; Howe, P.R.; DeNichilo, M.O.; Rowney, M.K. Supplementation with a whey protein hydrolysate enhances recovery of muscle force-generating capacity following eccentric exercise. J. Sci. Med. Sport. 2010, 13, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Cooke, M.B.; Rybalka, E.; Stathis, C.G.; Cribb, P.J.; Hayes, A. Whey protein isolate attenuates strength decline after eccentrically-induced muscle damage in healthy individuals. J. Int. Soc. Sports Nutr. 2010, 7, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farup, J.; Rahbek, S.K.; Knudsen, I.S.; de Paoli, F.; Mackey, A.L.; Vissing, K. Whey protein supplementation accelerates satellite cell proliferation during recovery from eccentric exercise. Amino Acids 2014, 46, 2503–2516. [Google Scholar] [CrossRef] [PubMed]
- Hamarsland, H.; Nordengen, A.L.; Aas, S.N.; Holte, K.; Garthe, I.; Paulsen, G.; Cotter, M.; Børsheim, E.; Benestad, H.B.; Raastad, T. Native whey protein with high levels of leucine results in similar post-exercise muscular anabolic responses as a regular whey protein: A randomized control trial. J. Int. Soc. Sports Nutr. 2017, 14. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Chulhyn, L.; Joohyung, L. Effect of timing of whey protein supplement on muscle damage markers after eccentric exercise. J. Exerc. Rehabil. 2017, 13, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Rindom, E.; Nielsen, M.H.; Kececi, K.; Jensen, M.E.; Vissing, K.; Farup, J. Effect of protein quality on recovery after intense resistance training. Eur. J. Appl. Physiol. 2016, 116, 2225–2236. [Google Scholar] [CrossRef] [PubMed]
- West, D.W.; Abou Sawan, S.; Mazzulla, M.; Williamson, E.; Moore, D.R. Whey protein supplementation enhances whole body protein turnover and performance recovery after resistance exercise: A double-blind crossover study. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- White, J.P.; Wilson, J.M.; Austin, K.G.; Greer, B.K.; St John, N.; Panton, L.B. Effect of carbohydrate-protein supplement timing on acute exercise-induced muscle damage. J. Int. Soc. Sports Nutr. 2008, 5. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting Items for Systematic Review and Meta-analysis: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Warren, G.L.; Park, N.D.; Maresca, R.D.; McKilbans, K.I.; Millard-Stafford, M.L. Effect of caffeine ingestion on muscular strength and endurance: A meta-analysis. Med Sci Sports Exerc. 2010, 42, 1375–1387. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, D.S.; Thomson, J.S. Effects of beta-hydroxy-beta-methylbutyrate supplementation during resistance training on strength, body composition, and muscle damage in trained and untrained young men: A meta-analysis. J. Strength Cond. Res. 2009, 23, 836–846. [Google Scholar] [CrossRef] [PubMed]
- Foure, A.; Bendahan, D. Is Branched-Chain Amino Acid supplementation an Efficient Nutritional Strategy to Alleviate Skeletal Muscle Damage? A Systemic Review. Nutrients 2017, 9. [Google Scholar] [CrossRef]
- Morelli, K.M.; Brown, L.B.; Warren, G.L. Effect of NSAIDs on Recovery from Acute Skeletal Muscle Injury: A Systematic Review and Meta-analysis. Am J Sports Med. 2018, 46. [Google Scholar] [CrossRef] [PubMed]
- AND. Evidence Analysis Manual: Steps in the Academic Evidence Analysis Process. Available online: https://www.andeal.org/vault/2440/web/files/QCC_3.pdf (accessed on 15 December 2017).
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; Wiley: Hoboken, NJ, USA, 2009; ISBN 978-0-470-05724-7. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Blacker, S.D.; Williams, N.C.; Fallowfield, J.L.; Bilzon, J.L.J.; Willems, M.E.T. Carbohydrate vs. protein supplementation for recovery of neuromuscular function following prolonged load carriage. J. Int. Soc. Sports Nutr. 2010, 7, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, M.A.; Stevenson, E.J.; Howatson, G. Whey protein hydrolysate supplementation accelerates recovery from exercise-induced muscle damage in females. Appl. Physiol. Nutr. Metab. 2017. [Google Scholar] [CrossRef] [PubMed]
- Eddens, L.; Browne, S.; Stevenson, E.J.; Sanderson, B.; van Someren, K.; Howatson, G. The efficacy of protein supplementation during recovery from muscle-damaging concurrent exercise. Appl. Physiol. Nutr. Metab. 2017, 42, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Betts, J.A.; Toone, K.A.; Thompson, D. Systematic indices of skeletal muscle damage and recovery of muscle function after exercise: Effect of combined carbohydrate-protein ingestion. Appl. Physiol. Nutr. Metab. 2009, 34, 773–784. [Google Scholar] [CrossRef] [PubMed]
- Cockburn, E.; Bell, P.G.; Stevenson, E. Effect of milk on team sport performance after exercise-induced muscle damage. Med. Sci. Sports Exerc. 2013, 45, 1585–1592. [Google Scholar] [CrossRef] [PubMed]
- Cockburn, E.; Hayes, P.R.; French, D.N.; Stevenson, E.; St Clair Gibson, A. Acute milk-based protein-cho supplementation attenuates exercise-induced muscle damage. Appl. Physiol. Nutr. Metab. 2008, 33, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Cockburn, E.; Robson-Ansley, P.; Hayes, P.R.; Stevenson, E. Effect of volume of milk consumed on the attenuation of exercise-induced muscle damage. Eur. J. Appl. Physiol. 2012, 112, 3187–3194. [Google Scholar] [CrossRef] [PubMed]
- Cockburn, E.; Stevenson, E.; Hayes, P.R.; Robson-Ansley, P.; Howatson, G. Effect of milk-based carbohydrate-protein supplement timing on the attenuation of exercise-induced muscle damage. Appl. Physiol. Nutr. Metab. 2010, 35, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Etheridge, T.; Philp, A.; Watt, P.W. A single protein meal increases recovery of muscle function following an acute eccentric exercise bout. Appl. Physiol. Nutr. Metab. 2008, 33, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Rankin, P.; Stevenson, E.; Cockburn, E. The effect of milk on the attenuation of exercise-induced muscle damage in males and females. Eur. J. Appl. Physiol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Rankin, P.; Lawlor, M.J.; Hills, F.A.; Bell, P.G.; Stevenson, E.J.; Cockburn, E. The effect of milk on recovery from repeat-sprint cycling in female team-sport athletes. Appl. Physiol. Nutr. Metab. 2018, 43, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Pasiakos, S.M.; Lieberman, H.R.; McLellan, T.M. Effects of protein supplements on muscle damage, soreness and recovery of muscle function and physical performance: A systematic review. Sports Med. 2014, 44, 655–670. [Google Scholar] [CrossRef] [PubMed]
- Goston, J.L.; Correia, M.I. Intake of nutritional supplements among people exercise in gyms and influence factors. Nutrition 2010, 26, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Rahbek, S.K.; Farup, J.; Møller, A.B.; Vendelbo, M.H.; Holm, L.; Jessen, N.; Vissing, K. Effects of divergent resistance exercise contraction mode and dietary supplementation type of anabolic signalling, muscle protein synthesis and muscle hypertrophy. Amino Acids 2014, 46, 2377–2392. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Study | Subjects | Design | QA | Exercise | Load | Supplement(s) | Control | Dose and Timing | Function Measure |
|---|---|---|---|---|---|---|---|---|---|
| Buckley et al. 2010 [9] | Untrained men | Parallel Groups | + | Unilateral, isokinetic, eccentric, knee extensions | 100 MVCs no rest reported | WP isolate (n = 11) WP hydrolysate (n = 6) | Flavoured Water (n = 11) No dietary control | 25 g 0 h, 6 h, 22 h post-exercise | Peak isometric knee extensor strength |
| Cooke et al. 2010 [10] | Untrained men | Parallel Groups | + | Unilateral, eccentric knee extensions, flexions, leg presses | 4 sets × 10 reps 120% 1 RM 3 min rest each set | WP hydrolysate + CHO (9:1) (n = 9) | Isocaloric CHO (n = 8) No dietary control | 1.5 g/kg 0.5 h post-exercise plus ~30 g with meals each day | Isometric and isokinetic knee extensor and flexor strength |
| Farup et al. 2014 [11] | Untrained men | Parallel Groups | + | Unilateral, isokinetic, eccentric knee extensions | 15 sets × 10 MVCs 1 min rest each set | WP hydrolysate + CHO (1:1) (n = 12) | Isocaloric CHO (n = 12) No dietary control | 56 g 0 h, 24 h, 48 h post-exercise | Peak isometric knee extensor strength |
| Hamarsland et al. 2017 [12] | Trained men and women | Parallel Groups | + | Bilateral knee extensions leg presses | 4 sets × 8 reps 100% 8 RM 3 min each set | WP concentrate (n = 10) Native WP (n = 10) | Milk (n = 12) Fixed dietary control | 20 g 0 h and 2 h post-exercise | Peak isometric knee extensor strength |
| Kim et al. 2017 [13] | Untrained men | Parallel Groups | + | Bilateral, isokinetic eccentric elbow flexions | 2 sets × 25 MVCs | WP (n = 24) (3 groups × n = 8) | No placebo/control No dietary control | 1.5 g/kg. Immediately before or after or before & after exercise | Peak isometric elbow flexor strength |
| Rindom et al. 2016 [14] | Trained men | Crossover | + | Whole body 5 exercises | 3–5 sets × ≤ 12 reps per exercise, 100% 15 RM 1.5 min rest each set | WP (n = 12) | Collagen protein (n = 12) Fixed dietary control | 25 g immediately before and after exercise 24 & 48 h post-exercise | Peak isometric knee extensor and flexor strength, CMJ, 30 s Wingate test, 3 RMs |
| West et al. 2017 [15] | Trained men | Crossover | + | Whole body 6 exercises | 4 sets × 8 reps per exercise, 75% 1 RM 2 min rest each set | WP isolate, concentrate and peptides (n = 12) | Isocaloric CHO (n = 12) Fixed dietary control | 25 g 0 h and 10 h post-exercise | Peak isometric knee extensor strength and maximum reps at 75% 1 RM, CMJ, 30 s Wingate |
| White et al. 2008 [16] | Untrained men | Parallel Groups | + | Unilateral, isokinetic, eccentric knee extensions | 5 sets × 10 MVCs 1 min rest each set | WP + CHO (1:3) (n = 18) (2 groups × n = 9) | Flavoured water (n = 9). No dietary control | 98 g Immediately before or after exercise | Peak isometric knee extensor strength |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davies, R.W.; Carson, B.P.; Jakeman, P.M. The Effect of Whey Protein Supplementation on the Temporal Recovery of Muscle Function Following Resistance Training: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 221. https://doi.org/10.3390/nu10020221
Davies RW, Carson BP, Jakeman PM. The Effect of Whey Protein Supplementation on the Temporal Recovery of Muscle Function Following Resistance Training: A Systematic Review and Meta-Analysis. Nutrients. 2018; 10(2):221. https://doi.org/10.3390/nu10020221
Chicago/Turabian StyleDavies, Robert W., Brian P. Carson, and Philip M. Jakeman. 2018. "The Effect of Whey Protein Supplementation on the Temporal Recovery of Muscle Function Following Resistance Training: A Systematic Review and Meta-Analysis" Nutrients 10, no. 2: 221. https://doi.org/10.3390/nu10020221