Validity of Prediction Equations of Maximal Heart Rate in Physically Active Female Adolescents and the Role of Maturation

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American college of sports medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Karvonen, M.J.; Kentala, E.; Mustala, O. The effects of training on heart rate; a longitudinal study. Ann. Med. Exp. Biol. Fenn. 1957, 35, 307–315. [Google Scholar] [PubMed]
- Cleary, M.A.; Hetzler, R.K.; Wages, J.J.; Lentz, M.A.; Stickley, C.D.; Kimura, I.F. Comparisons of age-predicted maximum heart rate equations in college-aged subjects. J. Strength Cond. Res. 2011, 25, 2591–2597. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.M., 3rd; Naughton, J.P.; Haskell, W.L. Physical activity and the prevention of coronary heart disease. Ann. Clin. Res. 1971, 3, 404–432. [Google Scholar] [CrossRef]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Nikolaidis, P.T.; Rosemann, T.; Knechtle, B. Age-predicted maximal heart rate in recreational marathon runners: A cross-sectional study on fox’s and tanaka’s equations. Front. Physiol. 2018, 9, 226. [Google Scholar] [CrossRef]
- Nikolaidis, P.T. Age-predicted vs. Measured maximal heart rate in young team sport athletes. Niger. Med. J. J. Niger. Med. Assoc. 2014, 55, 314–320. [Google Scholar] [CrossRef]
- Cicone, Z.S.; Holmes, C.J.; Fedewa, M.V.; MacDonald, H.V.; Esco, M.R. Age-based prediction of maximal heart rate in children and adolescents: A systematic review and meta-analysis. Res. Q. Exerc. Sport 2019, 90, 417–428. [Google Scholar] [CrossRef]
- Gelbart, M.; Ziv-Baran, T.; Williams, C.A.; Yarom, Y.; Dubnov-Raz, G. Prediction of maximal heart rate in children and adolescents. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2017, 27, 139–144. [Google Scholar] [CrossRef]
- Mahon, A.D.; Marjerrison, A.D.; Lee, J.D.; Woodruff, M.E.; Hanna, L.E. Evaluating the prediction of maximal heart rate in children and adolescents. Res. Q. Exerc. Sport 2010, 81, 466–471. [Google Scholar] [CrossRef]
- Olds, T.; Tomkinson, G.; Leger, L.; Cazorla, G. Worldwide variation in the performance of children and adolescents: An analysis of 109 studies of the 20-m shuttle run test in 37 countries. J. Sports Sci. 2006, 24, 1025–1038. [Google Scholar] [CrossRef] [PubMed]
- Eston, R.; Reilly, T. Kinanthropometry and Exercise Physiology Laboratory Manual, Volume 1, Anthropometry, Tests, Procedures and Data, 2nd ed.; Routledge: London, UK, 2001. [Google Scholar]
- Ross, W.D.; Marfell-Jones, M.J. Kinanthropometry. In Physiological Testing of the Highperformance Athlete; MacDougall, J.D., Wenger, H.A., Green, H.J., Eds.; Human Kinetics: Champaign, IL, USA, 1991. [Google Scholar]
- Mirwald, R.L.; Baxter-Jones, A.D.; Bailey, D.A.; Beunen, G.P. An assessment of maturity from anthropometric measurements. Med. Sci. Sports Exerc. 2002, 34, 689–694. [Google Scholar] [PubMed]
- Sarzynski, M.A.; Rankinen, T.; Earnest, C.P.; Leon, A.S.; Rao, D.C.; Skinner, J.S.; Bouchard, C. Measured maximal heart rates compared to commonly used age-based prediction equations in the heritage family study. Am. J. Hum. Biol. Off. J. Hum. Biol. Counc. 2013, 25, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, MI, USA, 1988. [Google Scholar]
- Batterham, A.M.; Hopkins, W.G. Making meaningful inferences about magnitudes. Int. J. Sports Physiol. Perform. 2006, 1, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Royston, P.; Altman, D.G.; Sauerbrei, W. Dichotomizing continuous predictors in multiple regression: A bad idea. Stat. Med. 2006, 25, 127–141. [Google Scholar] [CrossRef]
- Norman, A.C.; Drinkard, B.; McDuffie, J.R.; Ghorbani, S.; Yanoff, L.B.; Yanovski, J.A. Influence of excess adiposity on exercise fitness and performance in overweight children and adolescents. Pediatrics 2005, 115, e690–e696. [Google Scholar] [CrossRef]
- Nes, B.M.; Janszky, I.; Wisloff, U.; Stoylen, A.; Karlsen, T. Age-predicted maximal heart rate in healthy subjects: The hunt fitness study. Scand. J. Med. Sci. Sports 2013, 23, 697–704. [Google Scholar] [CrossRef]
- White, D.W.; Raven, P.B. Autonomic neural control of heart rate during dynamic exercise: Revisited. J. Physiol. 2014, 592, 2491–2500. [Google Scholar] [CrossRef]
- Cooper, D.M. Cardiorespiratory and metabolic responses to exercise: Maturation and growth. In The Child and Adolescent Athlete; Bar-Or, O., Ed.; Blackwell Science: Oxford, UK, 1996. [Google Scholar]
- Zavorsky, G.S. Evidence and possible mechanisms of altered maximum heart rate with endurance training and tapering. Sports Med. 2000, 29, 13–26. [Google Scholar] [CrossRef]
- Washington, R.L.; Bricker, J.T.; Alpert, B.S.; Daniels, S.R.; Deckelbaum, R.J.; Fisher, E.A.; Gidding, S.S.; Isabel-Jones, J.; Kavey, R.E.; Marx, G.R.; et al. Guidelines for exercise testing in the pediatric age group. From the committee on atherosclerosis and hypertension in children, council on cardiovascular disease in the young, the american heart association. Circulation 1994, 90, 2166–2179. [Google Scholar] [CrossRef]
- Rowland, T.W.; Maresh, C.M.; Charkoudian, N.; Vanderburgh, P.M.; Castellani, J.W.; Armstrong, L.E. Plasma norepinephrine responses to cycle exercise in boys and men. Int. J. Sports Med. 1996, 17, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Marsh, C.E. Validity of oxygen uptake cut-off criteria in plateau identification during horizontal treadmill running. J. Sports Med. Phys. Fit. 2019, 59, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Aziz, A.R.; Tan, F.H.; Teh, K.C. A pilot study comparing two field tests with the treadmill run test in soccer players. J. Sports Sci. Med. 2005, 4, 105–112. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 71) | Less Matured (n = 37) | More Matured (n = 34) |
|---|---|---|---|
| Age (years) | 13.3 ± 0.7 | 12.9 ± 0.7 | 13.8 ± 0.4 * |
| ΔAPHV (years) | 1.9 ± 0.5 | 1.5 ± 0.3 | 2.3 ± 0.3 * |
| Weight (kg) | 62.0 ± 7.2 | 59.1 ± 6.1 | 65.1 ± 7.2 * |
| Height (m) | 1.72 ± 0.06 | 1.68 ± 0.05 | 1.75 ± 0.04 * |
| BMI (kg.m-2) | 21.1 ± 2.2 | 20.9 ± 2.1 | 21.2 ± 2.4 |
| BF (%) | 21.2 ± 4.6 | 20.8 ± 4.6 | 21.6 ± 4.5 |
| SRT (min:s) | 5:00 ± 1:17 | 5:08 ± 1:20 | 4:51 ± 1:13 |
| Variable | Total (n = 71) | Less Matured (n = 37) | More Matured (n = 34) |
|---|---|---|---|
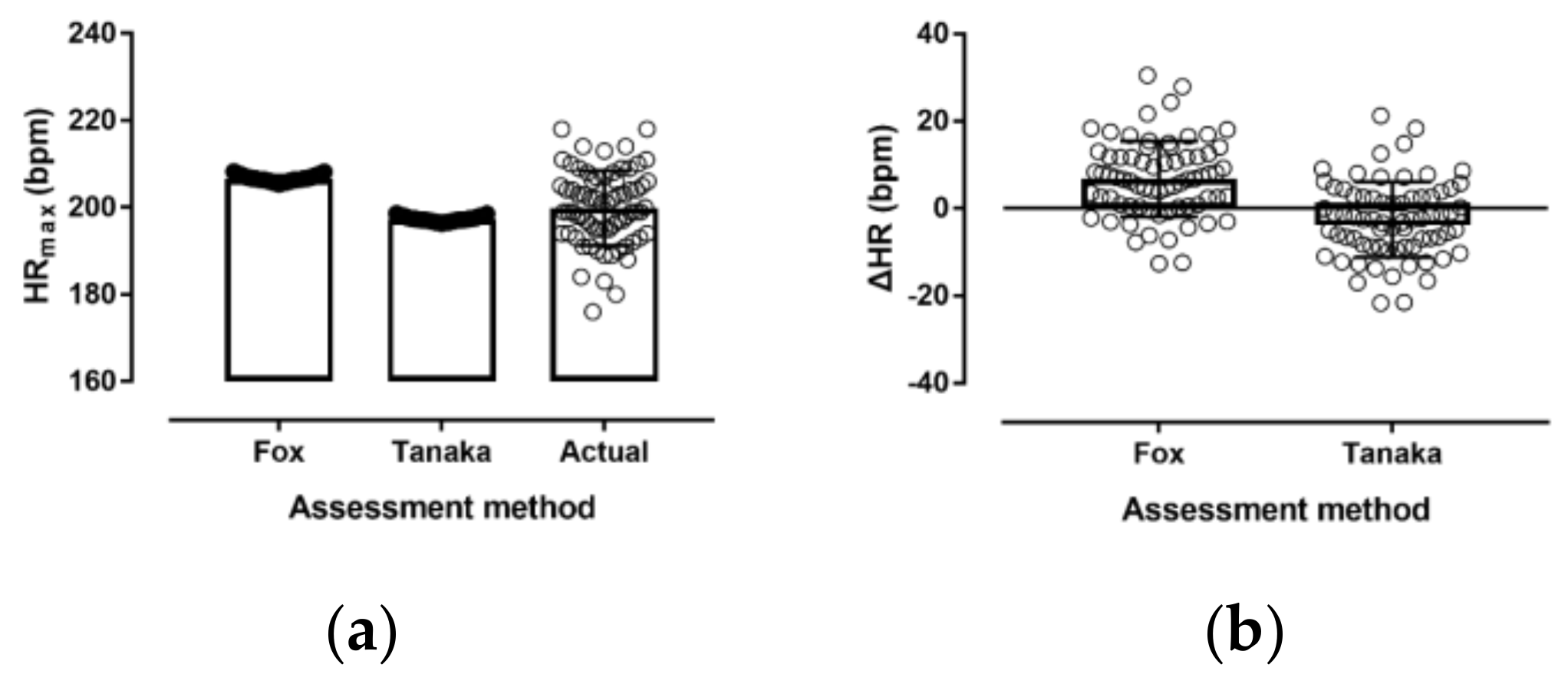
| Actual HRmax (bpm) | 199.9 ± 8.6 | 201.1 ± 8.4 | 198.7 ± 8.8 |
| Fox HRmax (bpm) | 206.7 ± 0.7 | 207.1 ± 0.7 | 206.2 ± 0.4 * |
| Tanaka HRmax (bpm) | 197.3 ± 0.6 | 197.7 ± 0.5 | 197.0 ± 0.3 * |
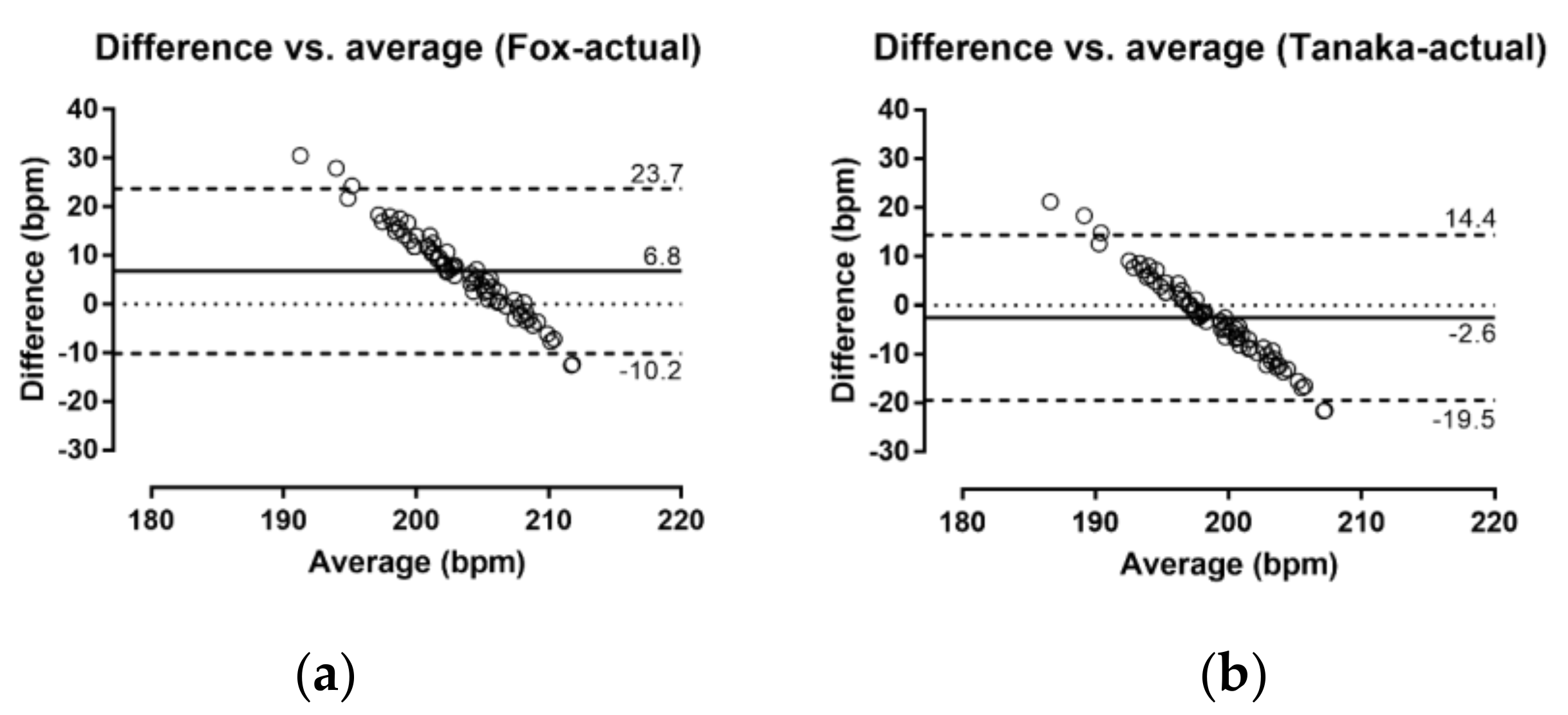
| Fox - Actual HRmax (bpm) | 6.8 ± 8.7 | 6.0 ± 8.5 | 7.6 ± 8.9 |
| Tanaka - Actual HRmax (bpm) | −2.6 ± 8.6 | −3.4 ± 8.5 | −1.7 ± 8.8 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadopoulou, S.D.; Papadopoulou, S.K.; Alipasali, F.; Hatzimanouil, D.; Rosemann, T.; Knechtle, B.; Nikolaidis, P.T. Validity of Prediction Equations of Maximal Heart Rate in Physically Active Female Adolescents and the Role of Maturation. Medicina 2019, 55, 735. https://doi.org/10.3390/medicina55110735
Papadopoulou SD, Papadopoulou SK, Alipasali F, Hatzimanouil D, Rosemann T, Knechtle B, Nikolaidis PT. Validity of Prediction Equations of Maximal Heart Rate in Physically Active Female Adolescents and the Role of Maturation. Medicina. 2019; 55(11):735. https://doi.org/10.3390/medicina55110735
Chicago/Turabian StylePapadopoulou, Sophia D., Sousana K. Papadopoulou, Foteini Alipasali, Dimitris Hatzimanouil, Thomas Rosemann, Beat Knechtle, and Pantelis T. Nikolaidis. 2019. "Validity of Prediction Equations of Maximal Heart Rate in Physically Active Female Adolescents and the Role of Maturation" Medicina 55, no. 11: 735. https://doi.org/10.3390/medicina55110735