Association between Striatal Brain Iron Deposition, Microbleeds and Cognition 1 Year After a Minor Ischaemic Stroke

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Sample Characteristics
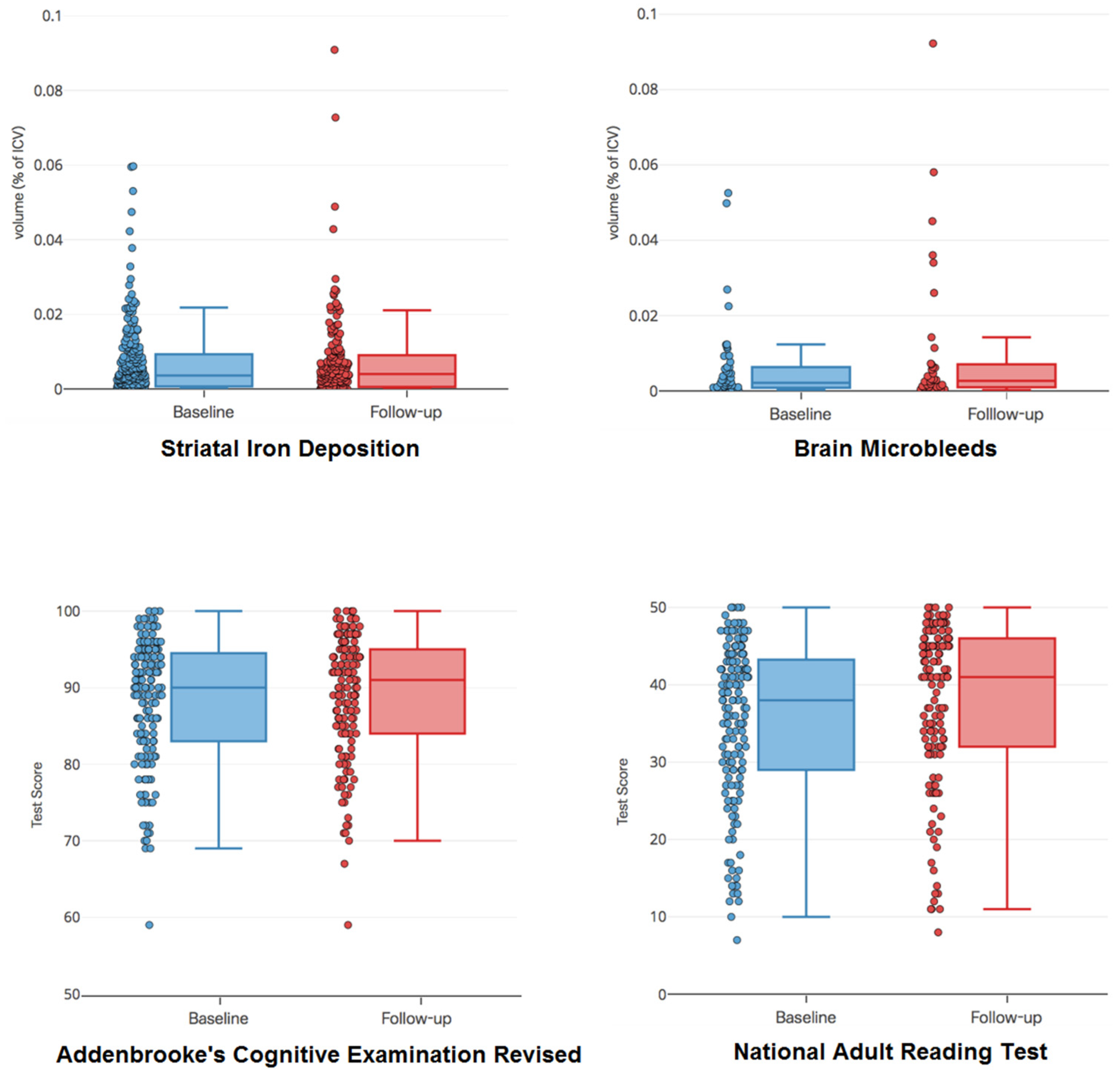
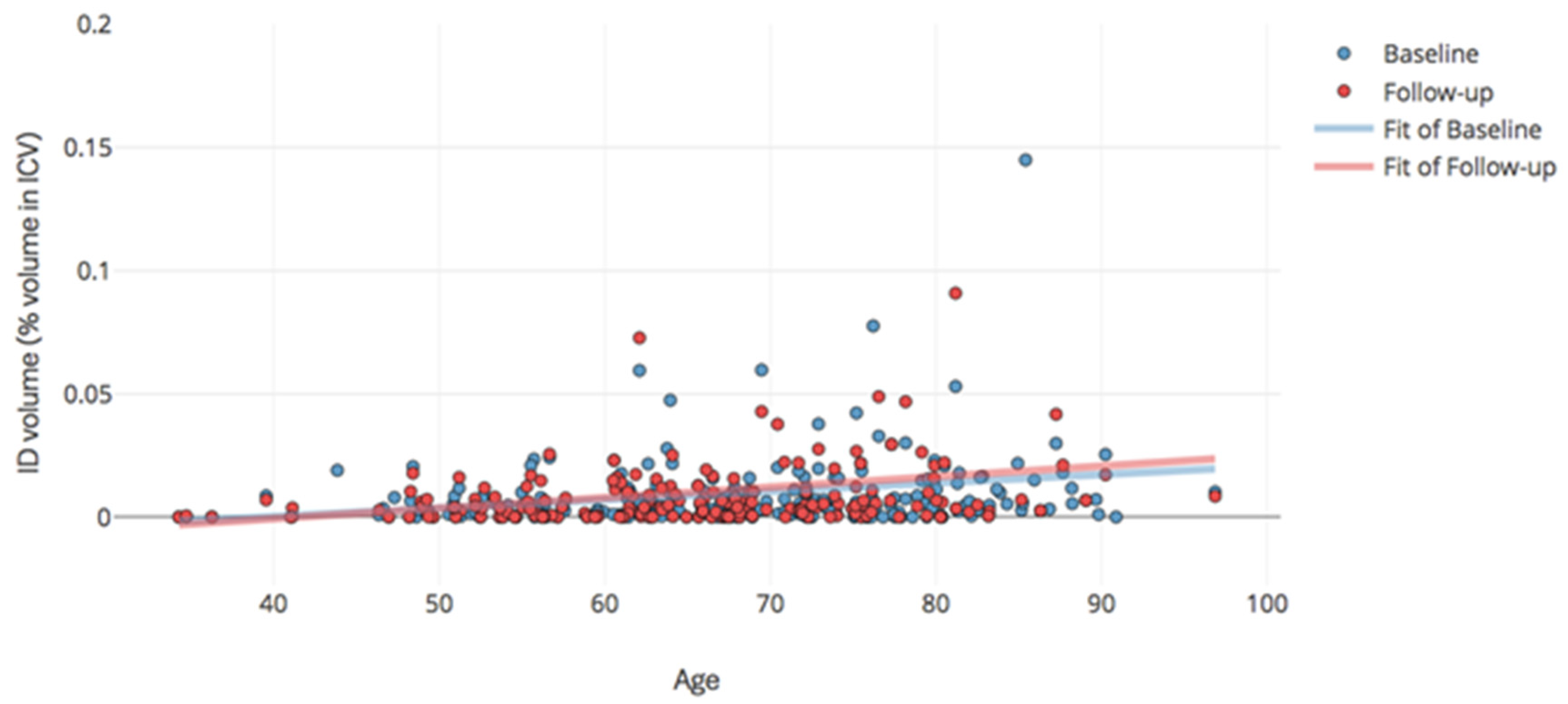
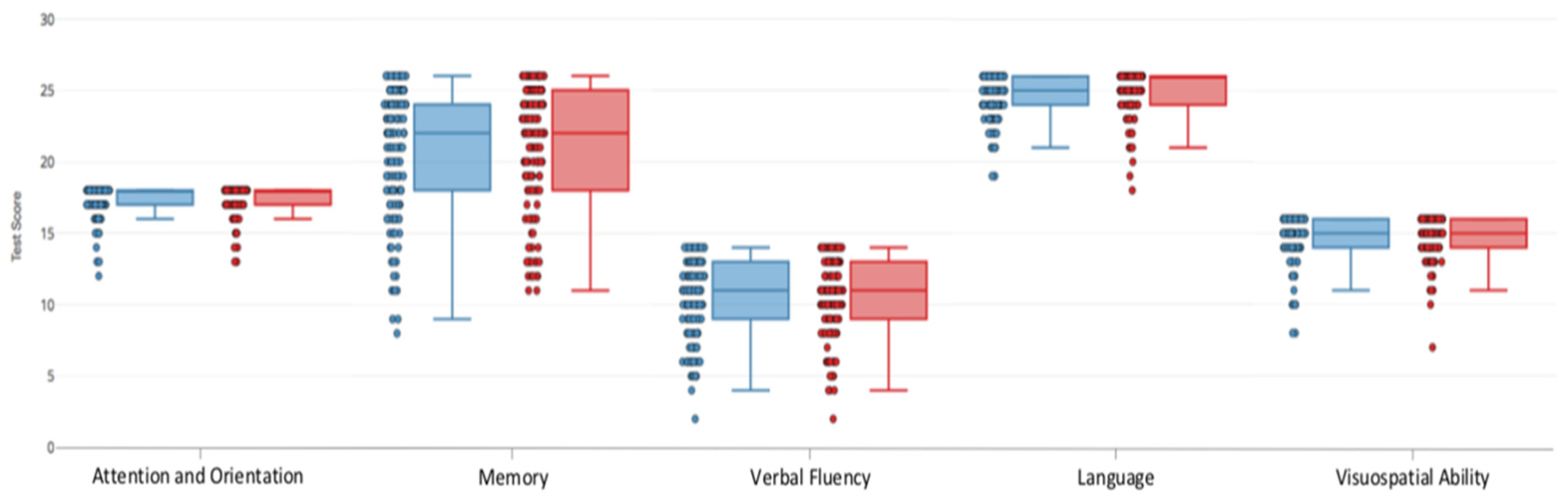
2.2. Progression of Imaging Markers and Cognitive Scores
2.3. Bivariate Relations
2.4. Association Between Baseline Striatal Iron Deposition and 1-year Cognition
2.5. Association Between Baseline Brain Microbleeds and 1-year Cognition
2.6. Risk Factors for ID and BMB Progression
3. Discussion
3.1. Progression Pattern of IDs and BMBs Following a non-Disabling Ischemic Stroke
3.2. ID and BMB Volumes as Predictors of 1-year Cognition following Ischaemic Stroke
3.3. Risk Factors for ID and BMB Progression following Ischaemic Stroke
3.4. Strengths and Limitations
3.5. Future Work
4. Materials and Methods
4.1. Subjects
4.2. Clinical Data
4.3. MRI Acquisition
4.4. Image Analysis
4.5. Cognitive Assessments
4.6. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BGID | Basal Ganglia Iron Deposition |
| BMBs | Brain MicroBleeds |
| NART | National Adult Reading Test |
| ACE-R | Addenbrooke’s Cognitive Examination - Revised |
| WMH | White Matter Hyperintensities |
| MRI | Magnetic Resonance Imaging |
| IDs | Iron Deposits |
| ICV | IntraCranial Volume |
| IQR | Inter Quartile Range |
| ANCOVA | ANalysis of COVAriances |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline measurements | 1 Year | ||
|---|---|---|---|
| Variable Types | |||
| Age (years) [mean (SD)] | 64.47 (10.58) | ||
| Gender [% (n)] | |||
| Male | 65 (84) | ||
| Female | 36 (46) | ||
| Brain Measurements | |||
| Lacunar stroke [% (n)] | 43 (55) | ||
| Cortical stroke [% (n)] | 58 (75) | ||
| White Matter Lesion (%ICV) [median (IQR)] | 0.76 (0.26–2.04) | 0.95 (0.42–1.91) | |
| ID [% (n)] | 77 (99) | 76 (98) | |
| ID (%ICV) [median (IQR)]† | 0.0051 (0.0025–0.011) | 0.0059 (0.0032–0.011) | |
| BMB [% (n)] | 22 (28) | 21 (27) | |
| BMB (%ICV) [median (IQR)]† | 0.0018 (0.00072–0.0051) | 0.0016 (0.00071–0.0042) | |
| Haemorrhage [% (n)] | 5 (6) | 5 (6) | |
| Haemorrhage (%ICV) [median (IQR)]† | 0.031 (0.012–0.14) | 0.045 (0.019–0.083) | |
| Cognitive Test Scores [median (IQR)] | |||
| ACE-R Total | 91 (84–95) | 91 (85–95) | |
| ACE-R Attention & Orientation | 18 (17–18) | 18 (17–18) | |
| ACE-R Memory | 22 (18–25) | 23 (19–25) | |
| ACE-R Verbal Fluency | 11 (9–13) | 11 (9–13) | |
| ACE-R Language | 25 (24–26) | 26 (25–26) | |
| ACE-R Visuospatial Ability | 15 (15–16) | 15 (14–16) | |
| NART Total | 38 (30–43) | 41 (32–46) | |
| Past Medical History [% (n)] | |||
| Hypertension | 73 (94) | ||
| Hyperlipidaemia | 64 (83) | ||
| Current smoker | 31 (40) | ||
| Recent ex-smoker | 4 (5) | ||
| Ex-smoker | 28 (36) | ||
| Never smoker | 37 (48) | ||
| Patients Tested | Patients Not Tested | p-value | |
|---|---|---|---|
| 1–3 Months | n = 157 * | n = 51 | |
| Age at index stroke (IQR) | 66 (56–75) | 71 (63–80) | <0.01 |
| Female gender | 64 (41%) | 24 (47%) | 0.51 |
| Previous stroke (prior to index event) | 19 (12%) | 4 (10%) | 0.8 |
| 1 Year | n = 151 | n = 57 | |
| Age at stroke (IQR) | 66 (56–74) | 73 (61–82) | <0.01 |
| Female gender | 58 (39%) | 30 (52%) | 0.51 |
| Previous stroke (prior to index event) | 19 (13%) | 5 (7%) | 0.58 |
| Stroke during follow-up | 12 (8%) | 5 (9%) | 0.78 |
| Cognition tested at 1–3 months, but not 1 year n = 22 | |||
| Age at stroke (IQR) | 65 (56–72.5) | ||
| Female gender | 12 (55%) | ||
| Stroke during follow-up | 2 (9%) | ||
| Reasons not tested at 1 year | Declined repeat test 11, too unwell 10, deceased 1 | ||
| Cognition not tested at 1–3 months, but tested at 1 year n = 16 | |||
| Age at stroke (IQR) | 72 (66–79.25) | ||
| Female gender | 6 (38%) | ||
| Stroke during follow-up | 1 (6%) | ||
| Reasons not tested at 1–3 months | Dysphasia which improved 1, forgot reading glasses 2, unable to attend due to work 1, too unwell 1, declined 11 | ||
| Cognition tested at both 1-3 months and 1 year n = 135 | |||
| Age at stroke (IQR) | 65 (56–72.5) | ||
| Female gender | 52 (39%) | ||
| Stroke during follow-up | 11 (8%) | ||

References
- Valdes Hernandez, M.D.C.; Ritchie, S.; Glatz, A.; Allerhand, M.; Maniega, S.M.; Gow, A.J.; Royle, N.A.; Bastin, M.E.; Starr, J.M.; Deary, I.J.; et al. Brain iron deposits and lifespan cognitive ability. Age 2015, 37, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valdes Hernandez, M.D.C.; Allerhand, M.; Glatz, A.; Clayson, L.; Munoz Maniega, S.; Gow, A.; Royle, N.A.; Bastin, M.E.; Starr, J.M.; Deary, I.J.; et al. Do white matter hyperintensities mediate the association between brain iron deposition and cognitive abilities in older people? Eur. J. Neurol. 2016, 23, 1202–1209. [Google Scholar] [CrossRef] [PubMed]
- Penke, L.; Hernandez, M.C.V.; Maniega, S.M.; Gow, A.J.; Murray, C.; Starr, J.M.; Bastin, M.E.; Deary, I.J.; Wardlaw, J.M. Brain iron deposits are associated with general cognitive ability and cognitive aging. Neurobiol. Aging 2012, 33, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Glatz, A.; Hernandez, M.C.V.; Kiker, A.J.; Bastin, M.E.; Deary, I.J.; Wardlaw, J.M. Characterization of multifocal T2*-weighted MRI hypointensities in the basal ganglia of elderly, community-dwelling subjects. NeuroImage 2013, 82, 470–480. [Google Scholar] [CrossRef]
- Ramos, P.; Santos, A.; Rosas Pinto, N.; Mendes, R.; Magalhaes, T.; Almeida, A. Iron levels in the human brain: A post-mortem study of anatomical region differences and age-related changes. J. Trace Elem. Med. Biol. 2014, 28, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Ghribi, O.; Golovko, M.Y.; Larsen, B.; Schrag, M.; Murphy, E.J. Deposition of iron and β-amyloid plaques is associated with cortical cellular damage in rabbits fed with long-term cholesterol-enriched diets. J. Neurochem. 2006, 99, 438–449. [Google Scholar] [CrossRef] [PubMed]
- Davalos, A.; Fernandez-Real, J.M.; Ricart, W.; Soler, S.; Molins, A.; Planas, E.; Genis, D. Iron-related damage in acute ischemic stroke. Stroke 1994, 25, 1543–1546. [Google Scholar] [CrossRef]
- Davalos, A.; Castillo, J.; Marrugat, J.; Fernandez-Real, J.M.; Armengou, A.; Cacabelos, P.; Rama, R. Body iron stores and early neurologic deterioration in acute cerebral infarction. Neurology 2000, 54, 1568–1574. [Google Scholar] [CrossRef]
- Cordonnier, C.; Al-Shahi Salman, R.; Wardlaw, J. Spontaneous brain microbleeds: Systematic review, subgroup analyses and standards for study design and reporting. Brain 2007, 130, 1988–2003. [Google Scholar] [CrossRef]
- Werring, D.J.; Frazer, D.W.; Coward, L.J.; Losseff, N.A.; Watt, H.; Cipolotti, L.; Brown, H.M.; Jager, H.R. Cognitive dysfunction in patients with cerebral microbleeds on T2*-weighted gradient-echo MRI. Brain 2004, 127, 2265–2275. [Google Scholar] [CrossRef] [Green Version]
- Puy, L.; Barbay, M.; Roussel, M.; Canaple, S.; Lamy, C.; Arnoux, A.; Leclercq, C.; Mas, J.L.; Tasseel-Ponche, S.; Constans, J.M.; et al. Neuroimaging Determinants of Poststroke Cognitive Performance. Stroke 2018, 49, 2666–2673. [Google Scholar] [CrossRef] [PubMed]
- Uiterwijk, R.; Staals, J.; Huijts, M.; de Leeuw, P.W.; Kroon, A.A.; van Oostenbrugge, R.J. MRI progression of cerebral small vessel disease and cognitive decline in patients with hypertension. J. Hypertens. 2017, 35, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Kidwell, C.S.; Saver, J.L.; Starkman, S.; Duckwiler, G.; Jahan, R.; Vespa, P.; Villabalanca, J.P.; Liebeskind, D.S.; Gobin, Y.P.; Vinuela, F.; et al. Late secondary ischemic injury in patients receiving intraarterial thrombolysis. Ann. Neurol. 2002, 52, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Liu, K.F.; Silva, M.D.; Omae, T.; Sotak, C.H.; Fenstermacher, J.D.; Fisher, M.; Hsu, C.Y.; Lin, W. Transient and permanent resolution of ischemic lesions on diffusion-weighted imaging after brief periods of focal ischemia in rats: Correlation with histopathology. Stroke 2000, 31, 946–954. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, R.B.; Bradley, W.G., Jr. Iron accumulation in the basal ganglia following severe ischemic-anoxic insults in children. Radiology 1988, 168, 203–206. [Google Scholar] [CrossRef] [PubMed]
- van Overbeek, E.C.; Staals, J.; van Oostenbrugge, R.J. Decreased kidney function relates to progression of cerebral microbleeds in lacunar stroke patients. Int. J. Stroke 2016, 11, 695–700. [Google Scholar] [CrossRef] [PubMed]
- van Middelaar, T.; Argillander, T.E.; Schreuder, F.H.B.M.; Deinum, J.; Richard, E.; Klijn, C.J.M. Effect of Antihypertensive Medication on Cerebral Small Vessel Disease: A Systematic Review and Meta-Analysis. Stroke 2018, 49, 1531–1533. [Google Scholar] [CrossRef]
- Arntz, R.M.; van den Broek, S.M.; van Uden, I.W.; Ghafoorian, M.; Platel, B.; Rutten-Jacobs, L.C.; Maaijwee, N.A.; Schaapsmeerders, P.; Schoonderwaldt, H.C.; van Dijk, E.J.; et al. Accelerated development of cerebral small vessel disease in young stroke patients. Neurology 2016, 87, 1212–1219. [Google Scholar] [CrossRef] [Green Version]
- Harper, A.M.; Clayson, L.; Wardlaw, J.M.; Valdés Hernández, M.; Alzheimer’s Disease Neuroimaging Initiative. Considerations on accuracy, pattern and possible underlying factors of brain microbleed progression in older adults with absence or mild presence of vascular pathology. J. Int. Med. Res. 2018, 46, 3518–3538. [Google Scholar] [CrossRef]
- De Guio, F.; Jouvent, E.; Biessels, G.J.; Black, S.E.; Brayne, C.; Chen, C.; Cordonnier, C.; De Leeuw, F.E.; Dichgans, M.; Doubal, F.; et al. Reproducibility and variability of quantitative magnetic resonance imaging markers in cerebral small vessel disease. J. Cereb. Blood Flow Metab. 2016, 36, 1319–1337. [Google Scholar] [CrossRef] [Green Version]
- Wardlaw, J.M.; Makin, S.J.; Hernandez, M.C.V.; Armitage, P.A.; Heye, A.K.; Chappell, F.M.; Muñoz-Maniega, S.; Sakka, E.; Shuler, K.; Dennis, M.S.; et al. Blood-brain barrier failure as a core mechanism in cerebral small vessel disease and dementia: Evidence from a cohort study. Alz. Dement. 2017, 13, 634–643. [Google Scholar] [CrossRef]
- Lee, S.H.; Lee, S.T.; Kim, B.J.; Park, H.K.; Kim, C.K.; Jung, K.H.; Roh, J.K. Dynamic temporal change of cerebral microbleeds: Long-term follow-up MRI study. PLoS ONE 2011, 6, e25930. [Google Scholar] [CrossRef] [PubMed]
- Bradley, W.G., Jr. MR appearance of hemorrhage in the brain. Radiology 1993, 189, 15–26. [Google Scholar] [CrossRef]
- Valdes Hernandez, M.D.C.; Glatz, A.; Kiker, A.J.; Dickie, D.A.; Aribisala, B.S.; Royle, N.A.; Muñoz Maniega, S.; Bastin, M.E.; Deary, I.J.; Wardlaw, J.M. Differentiation of calcified regions and iron deposits in the ageing brain on conventional structural MR images. J. Magn. Reson. Imaging 2014, 40, 324–333. [Google Scholar] [CrossRef]
- Kato, H.; Izumiyama, M.; Izumiyama, K.; Takahashi, A.; Itoyama, Y. Silent cerebral microbleeds on T2*-weighted MRI: Correlation with stroke subtype, stroke recurrence, and leukoaraiosis. Stroke 2002, 33, 1536–1540. [Google Scholar] [CrossRef] [PubMed]
- Tsushima, Y.; Aoki, J.; Endo, K. Brain microhemorrhages detected on T2*-weighted gradient-echo MR images. Am. J. Neuroradiol. 2003, 24, 88–96. [Google Scholar]
- Yakushiji, Y.; Yokota, C.; Yamada, N.; Kuroda, Y.; Minematsu, K. Clinical characteristics by topographical distribution of brain microbleeds, with a particular emphasis on diffuse microbleeds. J. Stroke Cerebrovasc. Dis. 2011, 20, 214–221. [Google Scholar] [CrossRef]
- Hanyu, H.; Tanaka, Y.; Shimizu, S.; Takasaki, M.; Fujita, H.; Kaneko, N.; Yamamoto, Y.; Harada, M. Cerebral microbleeds in Binswanger’s disease: A gradient-echo T2*-weighted magnetic resonance imaging study. Neurosci. Lett. 2003, 340, 213–216. [Google Scholar] [CrossRef]
- Fan, Y.H.; Zhang, L.; Lam, W.W.; Mok, V.C.; Wong, K.S. Cerebral microbleeds as a risk factor for subsequent intracerebral hemorrhages among patients with acute ischemic stroke. Stroke 2003, 34, 2459–2462. [Google Scholar] [CrossRef]
- Schonewille, W.J.; Singer, M.B.; Atlas, S.W.; Tuhrim, S. The prevalence of microhemorrhage on gradient-echo magnetic resonance imaging in acute lacunar infarction. J. Stroke Cerebrovasc. Dis. 2005, 14, 141–144. [Google Scholar] [CrossRef]
- Glatz, A.; Bastin, M.E.; Kiker, A.J.; Deary, I.J.; Wardlaw, J.M.; Hernandez, M.C.V. Automated segmentation of multifocal basal ganglia T2*-weighted MRI hypointensities. NeuroImage 2015, 105, 332–346. [Google Scholar] [CrossRef] [Green Version]
- Gottesman, R.F.; Hillis, A.E. Predictors and assessment of cognitive dysfunction resulting from ischaemic stroke. Lancet Neurol. 2010, 9, 895–905. [Google Scholar] [CrossRef] [Green Version]
- Hofgren, C.; Björkdahl, A.; Esbjörnsson, E.; Sunnerhagen, K.S. Recovery after stroke: Cognition, ADL function and return to work. Acta Neurol. Scand. 2007, 115, 73–80. [Google Scholar] [CrossRef] [PubMed]
- McHutchison, C.A.; Cvoro, V.; Makin, S.; Chappell, F.M.; Shuler, K.; Wardlaw, J.M. Functional, cognitive and physical outcomes 3 years after minor lacunar or cortical ischaemic stroke. J. Neurol. Neurosurg. Psychiatr. 2018. [Google Scholar] [CrossRef]
- Sullivan, E.V.; Adalsteinsson, E.; Rohlfing, T.; Pfefferbaum, A. Relevance of iron deposition in deep gray matter brain structures to cognitive and motor performance in healthy elderly men and women: Exploratory findings. Brain Imaging Behav. 2009, 3, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Killiany, R.J. Why is the study of iron important for magnetic resonance imaging? Top. Magn. Reson. Imaging 2006, 17, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.K.; Chen, Y.K.; Lu, J.Y.; Wong, A.; Mok, V.; Chu, W.C.; Ungvari, G.S.; Wong, K.S. Absence of cerebral microbleeds predicts reversion of vascular ‘cognitive impairment no dementia’ in stroke. Int. J. Stroke 2011, 6, 498–505. [Google Scholar] [CrossRef]
- Gregoire, S.M.; Smith, K.; Jager, H.R.; Benjamin, M.; Kallis, C.; Brown, M.M.; Cipolotti, L.; Werring, D.J. Cerebral microbleeds and long-term cognitive outcome: Longitudinal cohort study of stroke clinic patients. Cerebrovasc. Dis. 2012, 33, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Yakushiji, Y.; Nishiyama, M.; Yakushiji, S.; Hirotsu, T.; Uchino, A.; Nakajima, J.; Eriguchi, M.; Nanri, Y.; Hara, M.; Horikawa, E.; et al. Brain microbleeds and global cognitive function in adults without neurological disorder. Stroke 2008, 39, 3323–3328. [Google Scholar] [CrossRef] [PubMed]
- Takashima, Y.; Mori, T.; Hashimoto, M.; Kinukawa, N.; Uchino, A.; Yuzuriha, T.; Yao, H. Clinical correlating factors and cognitive function in community-dwelling healthy subjects with cerebral microbleeds. J. Stroke Cerebrovasc. Dis. 2011, 20, 105–110. [Google Scholar] [CrossRef]
- Poels, M.M.; Ikram, M.A.; van der Lugt, A.; Hofman, A.; Krestin, G.P.; Breteler, M.M.; Vernooij, M.W. Incidence of cerebral microbleeds in the general population: The Rotterdam Scan Study. Stroke 2011, 42, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Mijajlović, M.D.; Pavlović, A.; Brainin, M.; Heiss, W.D.; Quinn, T.J.; Ihle-Hansen, H.B.; Hermann, D.M.; Assayag, E.B.; Richard, E.; Thiel, A.; et al. Post-stroke dementia—A comprehensive review. BMC Med. 2017, 15, 11. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, P.S.; Lipnicki, D.M.; Crawford, J.D.; Wen, W.; Brodaty, H. Progression of cognitive impairment in stroke/TIA patients over 3 years. J. Neurol. Neurosurg. Psychiatry 2014, 85, 1324–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brainin, M.; Tuomilehto, J.; Heiss, W.; Bornstein, N.M.; Bath, P.M.; Teuschl, Y.; Richard, E.; Guekht, A.; Quinn, T.; the Post Stroke Cognition Study Group. Post-stroke cognitive decline: An update and perspectives for clinical research. Eur. J. Neurol. 2015, 22, 229-e16. [Google Scholar] [PubMed]
- Molad, J.; Kliper, E.; Korczyn, A.D.; Ben Assayag, E.; Ben Bashat, D.; Shenhar-Tsarfaty, S.; Aizenstein, O.; Shopin, L.; Bornstein, N.M.; Auriel, E. Only White Matter Hyperintensities Predicts Post-Stroke Cognitive Performances Among Cerebral Small Vessel Disease Markers: Results from the TABASCO Study. J. Alzheimers Dis. 2017, 56, 1293–1299. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed]
- Romero, J.R.; Preis, S.R.; Beiser, A.; DeCarli, C.; Viswanathan, A.; Martinez-Ramirez, S.; Kase, C.S.; Wolf, P.A.; Seshadri, S. Risk factors, stroke prevention treatments, and prevalence of cerebral microbleeds in the Framingham Heart Study. Stroke 2014, 45, 1492–1494. [Google Scholar] [CrossRef] [PubMed]
- Shams, S.; Martola, J.; Granberg, T.; Li, X.; Shams, M.; Fereshtehnejad, S.M.; Cavallin, L.; Aspelin, P.; Kristoffersen-Wiberg, M.; Wahlund, L.O. Cerebral microbleeds: Different prevalence, topography, and risk factors depending on dementia diagnosis—The Karolinska Imaging Dementia Study. Am. J. Neuroradiol. 2015, 36, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Raz, N.; Rodrigue, K.M.; Haacke, E. Brain aging and its modifiers. Ann. N. Y. Acad. Sci. 2007, 1097, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Rodrigue, K.M.; Haacke, E.M.; Raz, N. Differential effects of age and history of hypertension on regional brain volumes and iron. Neuroimage 2011, 54, 750–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, C.; Brosnan, M.J.; Fennell, J.; Hamilton, C.A.; Dominiczak, A.F. Oxidative stress and vascular damage in hypertension. Curr. Opin. Nephrol. Hypertens. 2001, 10, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, A.M.; Haacke, E.M.; Raz, N. Striatal iron content predicts its shrinkage and changes in verbal working memory after two years in healthy adults. J. Neurosci. 2015, 35, 6731–6743. [Google Scholar] [CrossRef]
- Hare, D.J.; Ayton, S.; Bush, A.I.; Lei, P. A delicate balance: Iron metabolism and diseases of the brain. Front. Aging Neurosci. 2013, 5, 34. [Google Scholar] [CrossRef] [PubMed]
- Deane, R.; Zheng, W.; Zlokovic, B.V. Brain capillary endothelium and choroid plexus epithelium regulate transport of transferrin-bound and free iron into the rat brain. J. Neurochem. 2004, 88, 813–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henskens, L.H.; Van Oostenbrugge, R.J.; Kroon, A.A.; De Leeuw, P.W.; Lodder, J. Brain microbleeds are associated with ambulatory blood pressure levels in a hypertensive population. Hypertension 2008, 51, 62–68. [Google Scholar] [CrossRef]
- Goodman, S.N.; Berlin, J.A. The use of predicted confidence intervals when planning experiments and the misuse of power when interpreting results. Ann. Int. Med. 1994, 121, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Chiang, G.C.; Hernandez, J.C.; Kantarci, K.; Jack, C.R.; Weiner, M.W.; Alzheimer’s Disease Neuroimaging Initiative. Cerebral microbleeds, CSF p-tau, and cognitive decline: Significance of anatomic distribution. Am. J. Neuroradiol. 2015, 36, 1635–1641. [Google Scholar] [CrossRef]
- Heye, A.K.; Thrippleton, M.J.; Chappell, F.M.; Valdes Hernandez, M.D.C.; Armitage, P.A.; Makin, S.D.; Muñoz Maniega, S.; Sakka, E.; Flatman, P.W.; Dennis, M.S.; et al. Blood pressure and sodium: Association with MRI markers in cerebral small vessel disease. J. Cereb. Blood Flow Metab. 2016, 36, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Valdes Hernández, M.D.C.; Armitage, P.A.; Thrippleton, M.J.; Chappell, F.; Sandeman, E.; Muñoz Maniega, S.; Shuler, K.; Wardlaw, J.M. Rationale, design and methodology of the image analysis protocol for studies of patients with cerebral small vessel disease and mild stroke. Brain Behav. 2015, 5, e00415. [Google Scholar] [CrossRef] [PubMed]
- Mioshi, E.; Dawson, K.; Mitchell, J.; Arnold, R.; Hodges, J.R. The Addenbrooke’s Cognitive Examination Revised (ACE-R): A brief cognitive test battery for dementia screening. Int. J. Geriatr. Psychiatr. 2006, 21, 1078–1085. [Google Scholar] [CrossRef] [PubMed]
- Nelson, H.E.; Willison, J. National Adult Reading Test (NART); Nfer-Nelson: Windsor, ON, Canada, 1991. [Google Scholar]
- Pernet, C.R.; Wilcox, R.R.; Rousselet, G.A. Robust correlation analyses: False positive and power validation using a new open source Matlab toolbox. Front. Psychol. 2013, 3, e606. [Google Scholar] [CrossRef] [PubMed]



| Baseline Measurements | 1 Year | ||
|---|---|---|---|
| Variable Types | (n = 264) | (n = 190) | |
| Age (years) [mean (SD)] | 67 (11.84) | 65 (11.28) | |
| Gender [% (n)] | |||
| Male | 58 (154) | 58 (111) | |
| Female | 42 (110) | 42 (79) | |
| Brain Measurements | |||
| Lacunar stroke [% (n)] | 45 (118) | 46 (88) | |
| Cortical stroke [% (n)] | 55 (146) | 54 (102) | |
| ICV (ml) [mean (SD)] | 1478.33(146.47) | 1479.81 (147.85) | |
| WMH (%ICV) [median (IQR)] | 0.89 (0.31–2.39) | 0.98 (0.42–2.16) | |
| ID [% (n)] | 79 (209) | 80 (152) | |
| ID (%ICV) [median (IQR)] | 0.0039 (0.00060–0.0099) | 0.0043 (0.00057–0.010) | |
| BMB [% (n)] | 22 (58) | 22 (42) | |
| BMB (%ICV) [median (IQR)]† | 0.0019 (0.00076–0.0049) | 0.0019 (0.00061–0.0038) | |
| Haemorrhage [% (n)] | 2 (6) | 3 (6) | |
| Haemorrhage (%ICV) [median (IQR)]† | 0.014 (0.0091 - 0.048) | 0.036 (0.011–0.054) | |
| Cognitive Test Scores [median (IQR)] | *(n = 157) | *(n = 151) | |
| ACE-R Total | 90 (83–94) | 91 (84.75–95) | |
| ACE-R Attention & Orientation | 18 (17–18) | 18 (17–18) | |
| ACE-R Memory | 22 (18–24) | 22.5 (18–25) | |
| ACE-R Verbal Fluency | 11 (9–13) | 11 (9–13) | |
| ACE-R Language | 25 (24–26) | 26 (24.75–26) | |
| ACE-R Visuospatial Ability | 15 (14–16) | 15 (14–16) | |
| NART Total | 37.5 (29–43) | 41 (32–46) | |
| Past Medical History [% (n)] | |||
| Hypertension | 72 (191) | 74 (141) | |
| Hyperlipidaemia | 61 (161) | 61 (116) | |
| Current smoker | 34 (90) | 34 (65) | |
| Recent ex-smoker | 5 (12) | 4 (8) | |
| Ex-smoker | 28 (74) | 25 (48) | |
| Never smoker | 33 (87) | 36 (69) | |
| Index Stroke Lesion Subtype, Arterial Territory and Cerebral Hemisphere | No. of Patients without BMB | No. of Patients with at Least 1 BMB | Average Volume of BMB Expressed as % in ICV (SD) | Total no. of Patients (%) |
|---|---|---|---|---|
| Cortical in the Middle Cerebral Artery (MCA) territory | 43 | 8 | 0.00059 (0.0017) | 51 (19.3) |
| Cortical in the Anterior Cerebral Artery (ACA) territory | 4 | 0 | 0 | 4 (1.5) |
| Cortical in the Posterior Cerebral Artery (PCA) territory | 20 | 5 | 0.00058 (0.0019) | 25 (9.5) |
| Cortical in the border zone (i.e., watershed) territories | 18 | 5 | 0.00055 (0.0015) | 23 (8.7) |
| Lacunar | 47 | 28 | 0.0017 (0.0038) | 75 (28.4) |
| Cortical in Cerebellum | 7 | 0 | 0 | 7 (2.7) |
| Cortical in Brainstem | 1 | 3 | 0.0012 (0.0013) | 4 (1.5) |
| Ischemic stroke in Right Hemisphere | 81 | 23 | 0.00064 (0.0017) | 104 (39.4) |
| Ischemic stroke in Left Hemisphere | 59 | 26 | 0.0014 (0.0035) | 85 (32.2) |
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) Age | 1 | 0.009 | 0.443 ** | 0.296 ** | 0.209 * | −0.305 ** | 0.074 | 0.297 ** | 0.184 * | −0.242 ** | 0.109 |
| (2) Gender | −0.043 | 1 | 0.131 | 0.177 | 0.016 | 0.051 | 0.246 ** | 0.227 * | 0.042 | 0.081 | 0.148 |
| (3) Baseline WMH volume (% in ICV) | 0.506 ** | 0.011 | 1 | 0.377 ** | 0.292 ** | −0.143 | 0.225 * | 0.408 ** | 0.306 ** | −0.155 | 0.135 |
| (4) Baseline BGID volume (% in ICV) | 0.248 ** | 0.031 | 0.279 ** | 1 | 0.156 | 0.040 | 0.219 * | 0.799 ** | 0.171 | 0.024 | 0.194 * |
| (5) Baseline BMB volume (% in ICV) | 0.129 * | 0.065 | 0.294 ** | 0.238 ** | 1 | −0.100 | 0.092 | 0.179 | 0.977 ** | −0.055 | 0.039 |
| (6) Baseline ACE-R | −0.322 ** | 0.038 | −0.131 | −0.023 | -0.104 | 1 | 0.462 ** | 0.018 | −0.081 | 0.758 ** | 0.470 ** |
| (7) Baseline NART | 0.087 | 0.202 * | 0.204 * | 0.198 * | 0.071 | 0.468 ** | 1 | 0.270 ** | 0.117 | 0.535 ** | 0.866 ** |
| (8) Follow-up BGID vol. (% in ICV) | 0.271 ** | 0.146 * | 0.367 ** | 0.835 ** | 0.192 ** | −0.028 | 0.241 ** | 1 | 0.200 * | 0.033 | 0.219 * |
| (9) Follow-up BMB vol. (% in ICV) | 0.142 | 0.068 | 0.309 ** | 0.191 ** | 0.985 ** | −0.126 | 0.071 | 0.204 ** | 1 | −0.037 | 0.057 |
| (10) Follow-up ACE-R | −0.241 ** | 0.091 | −0.177 * | −0.008 | −0.057 | 0.788 ** | 0.526 ** | −0.014 | −0.053 | 1 | 0.559 ** |
| (11) Follow-up NART | 0.113 | 0.138 | 0.092 | 0.132 | 0.011 | 0.477 ** | 0.854 ** | 0.182 * | 0.032 | 0.568 ** | 1 |
| Outcome Variable (Dependent) | Predictor (Independent Variable) | Main Effect (B, (SE)) | Covariates | |||||
|---|---|---|---|---|---|---|---|---|
| Age | Gender | Hypertension | Hyper-lipidemia | Smoking | % Baseline WMH vol. in ICV | |||
| Follow-up ACER | Baseline % striatal ID vol. in ICV | −17.35 (11.60) | −0.0081 (0.044) | 0.30 (0.84) | 0.72 (0.95) | 0.54 (0.89) | −1.38 (0.89) | −0.091 (0.32) |
| Baseline % BMB vol. in ICV | 130.32 (215.68) | −0.018 (0.045) | 0.43 (0.85) | 0.76 (0.96) | 0.49 (0.91) | −1.25 (0.90) | −0.23 (0.34) | |
| ACE-R change | Baseline % striatal ID vol. in ICV | −17.36 (11.60) | −0.0081 (0.044) | 0.30 (0.84) | 0.72 (0.95) | 0.54 (0.89) | −1.38 (0.89) | −0.091 (0.32) |
| Baseline % BMB vol. in ICV | 130.32 (215.68) | −0.018 (0.045) | 0.32 (0.85) | 0.75 (0.96) | 0.49 (0.91) | −1.25 (0.90) | −0.23 (0.34) | |
| Follow-up Orientation (†) | Baseline % striatal ID vol. in ICV | −2.25 (7.52) | 0.02 (0.02) | −0.10 (0.43) | −0.60 (0.46) | −0.33 (0.43) | 0.083 (0.46) | 0.15 (0.16) |
| Baseline % BMB vol. in ICV | −18.45 (103.11) | 0.024 (0.023) | 0.21 (0.46) | −0.64 (0.50) | −0.50 (0.48) | 0.014 (0.49) | 0.17 (0.18) | |
| Orientation change | Baseline % striatal ID vol. in ICV | 0.46 (1.16) | −0.0045 (0.0043) | −0.029 (0.084) | 0.12 (0.094) | 0.094 (0.089) | −0.0025 (0.089) | −0.035 (0.032) |
| Baseline % BMB vol. in ICV | 2.26 (21.38) | −0.0045 (0.0043) | −0.035 (0.084) | 0.12 (0.095) | 0.095 (0.090) | −0.0042 (0.090) | −0.033 (0.034) | |
| Follow-up Memory | Baseline % striatal ID vol. in ICV | −12.79 (8.05) | −0.023 (0.030) | −0.10 (0.58) | 0.63 (0.67) | 0.74 (0.62) | −0.22 (0.62) | 0.095 (0.22) |
| Baseline % BMB vol. in ICV | 66.67 (150.32) | −0.029 (0.031) | −0.055 (0.59) | 0.66 (0.68) | 0.71 (0.63) | −0.14 (0.63) | 0.0015 (0.23) | |
| Memory change | Baseline % striatal ID vol. in ICV | −12.793 (8.05) | −0.023 (0.031) | −0.10 (0.58) | 0.63 (0.67) | 0.74 (0.62) | −0.22 (0.62) | 0.095 (0.22) |
| Baseline % BMB vol. in ICV | 66.67 (150.32) | −0.029 (0.031) | −0.055 (0.59) | 0.66 (0.68) | 0.71 (0.63) | −0.14 (0.63) | 0.0015 (0.23) | |
| Follow-up Verbal Fluency | Baseline % striatal ID vol. in ICV | −8.00 (5.26) | −0.0091 (0.020) | 0.39 (0.38) | 0.43 (0.43) | −0.14 (0.40) | −1.13 (0.41) (p = 0.0067) | 0.12 (0.15) |
| Baseline % BMB vol. in ICV | 7.62 (97.81) | −0.012 (0.020) | 0.41 (0.39) | 0.41 (0.43) | −0.19 (0.41) | −1.06 (0.41) (p = 0.011) | 0.08 (0.16) | |
| Verbal Fluency change | Baseline % striatal ID vol. in ICV | −8.01 (5.26) | −0.0091 (0.020) | 0.39 (0.38) | 0.43 (0.43) | −0.14 (0.40) | −1.13 (0.41) (p = 0.0067) | 0.12 (0.15) |
| Baseline % BMB vol. in ICV | 7.62 (97.81) | −0.012 (0.020) | 0.41 (0.39) | 0.41 (0.43) | −0.19 (0.41) | −1.06 (0.41) (p = 0.011) | 0.08 (0.16) | |
| Follow-up Language (†) | Baseline % striatal ID vol. in ICV | −14.058 (13.88) | 0.01 (0.02) | -0.048 (0.45) | 0.39 (0.48) | 0.53 (0.45) | −0.77 (0.48) | 0.079 (0.16) |
| Baseline % BMB vol. in ICV | −39.90 (123.038) | 0.014 (0.023) | 0.11 (0.47) | 0.51 (0.52) | 0.32 (0.49) | −0.77 (0.50) | 0.072 (0.18) | |
| Language change | Baseline % striatal ID vol. in ICV | 2.41 (2.35) | −0.0062 (0.0088) | 0.13 (0.18) | −0.13 (0.19) | −0.21 (0.18) | 0.15 (0.18) | −0.034 (0.065) |
| Baseline % BMB vol. in ICV | −19.45 (46.74) | −0.0055 (0.0096) | 0.050 (0.19) | −0.064 (0.21) | −0.23 (0.19) | 0.14 (0.20) | −0.013 (0.073) | |
| Follow-up Visuospatial (†) | Baseline % striatal ID vol. in ICV | 2.93 (10.10) | 0.019 (0.022) | −0.62 (0.41) | 0.37 (0.45) | −0.18 (0.42) | 1.00 (0.45) | 0.19 (0.16) |
| Baseline % BMB vol. in ICV | −110.92 (118.39) | 0.022 (0.023) | −0.75 (0.44) | 0.65 (0.50) | −0.52 (0.47) | 0.88 (0.47) | 0.36 (0.19) | |
| Visuospatial change | Baseline % striatal ID vol. in ICV | 1.44 (2.41) | −0.0018 (0.0091) | 0.27 (0.18) | −0.22 (0.20) | 0.12 (0.19) | −0.29 (0.19) | −0.22 (0.067) (p = 0.0015) |
| Baseline % BMB vol. in ICV | 90.34 (45.56) (p = 0.05) | −0.0045 (0.0094) | 0.11(0.17) | −0.15 (0.20) | 0.11 (0.19) | −0.33 (0.19) | −0.21 (0.071) (p = 0.0044) | |
| Follow-up NART | Baseline % striatal ID vol. in ICV | 6.92 (14.50) | 0.030 (0.054) | -0.51(1.07) | 0.33 (1.18) | −1.86 (1.12) | −0.88 (1.12) | −0.59 (0.41) |
| Baseline % BMB vol. in ICV | 86.72 (268.56) | 0.020 (0.054) | −0.57 (1.075) | 0.39 (1.20) | −1.79 (1.13) | −0.94 (1.13) | −0.60 (0.43) | |
| NART change | Baseline % striatal ID vol. in ICV | 6.92 (14.50) | 0.030 (0.054) | −0.51 (1.07) | 0.33 (1.18) | −1.86 (1.12) | −0.88 (1.12) | −0.59 (0.41) |
| Baseline % BMB vol. in ICV | 86.72 (268.56) | 0.020 (0.054) | −0.57 (1.075) | 0.39 (1.20) | −1.79 (1.13) | −0.94 (1.13) | −0.60 (0.43) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valdés Hernández, M.d.C.; Case, T.; Chappell, F.M.; Glatz, A.; Makin, S.; Doubal, F.; Wardlaw, J.M. Association between Striatal Brain Iron Deposition, Microbleeds and Cognition 1 Year After a Minor Ischaemic Stroke. Int. J. Mol. Sci. 2019, 20, 1293. https://doi.org/10.3390/ijms20061293
Valdés Hernández MdC, Case T, Chappell FM, Glatz A, Makin S, Doubal F, Wardlaw JM. Association between Striatal Brain Iron Deposition, Microbleeds and Cognition 1 Year After a Minor Ischaemic Stroke. International Journal of Molecular Sciences. 2019; 20(6):1293. https://doi.org/10.3390/ijms20061293
Chicago/Turabian StyleValdés Hernández, Maria del C., Tessa Case, Francesca M. Chappell, Andreas Glatz, Stephen Makin, Fergus Doubal, and Joanna M. Wardlaw. 2019. "Association between Striatal Brain Iron Deposition, Microbleeds and Cognition 1 Year After a Minor Ischaemic Stroke" International Journal of Molecular Sciences 20, no. 6: 1293. https://doi.org/10.3390/ijms20061293