Effects of Ergomotor Intervention on Improving Occupational Health in Workers with Work-Related Neck-Shoulder Pain



Abstract
:1. Introduction
2. Materials and Methods
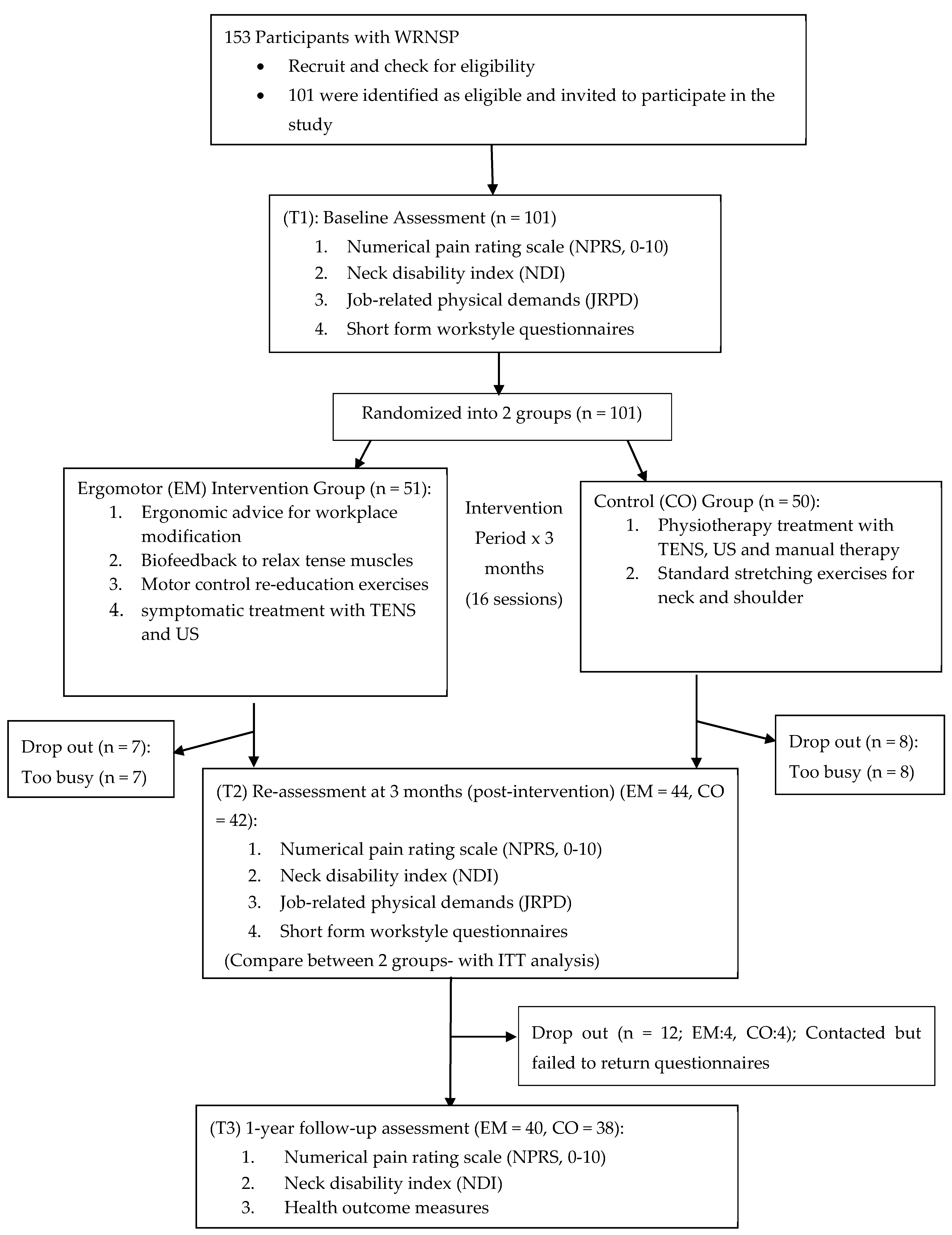
2.1. Study Design
2.2. Sample Size Planning
2.3. Participants
2.4. Intervention Protocols
2.5. Occupational Exposure Measures
2.6. Data Analysis
3. Results
3.1. Demographic Data of Participants
3.2. Results on Occupational Exposure Measures
4. Discussion
4.1. Effects of Ergomotor Approach on Job-Related Physical Demands
4.2. Effects of Ergomotor Approach on Workstyle
4.3. Integrating Ergonomics and Motor Control Interventions
4.4. Cost-Effectiveness of Ergomotor Approach
4.5. Limitations of Study and Suggestions for Future Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Buckle, P.W.; Devereux, J.J. The nature of work-related neck and upper limb musculoskeletal disorders. Appl. Ergon. 2002, 33, 207–217. [Google Scholar] [CrossRef]
- Chen, X.; O’Leary, S.; Johnston, V. Modifiable individual and work-related factors associated with neck pain in 740 office workers: A cross-sectional study. Braz. J. Phys. Ther. 2018, 22, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Shum, S.-L. Occupational Risk Factors for Neck and Shoulder Pain Among Hong Kong Nurses, S; Hong Kong Polytechnic University: Hong Kong, China, 2008. [Google Scholar]
- Van Eerd, D.; Munhall, C.; Irvin, E.; Rempel, D.; Brewer, S.; Van Der Beek, A.J. Effectiveness of workplace interventions in the prevention of upper extremity musculoskeletal disorders and symptoms: An update of the evidence. Occup. Environ. Med. 2016, 73, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Punnett, L.; Wegman, D.H. Work-related musculoskeletal disorders: The epidemiologic evidence and the debate. J. Electromyogr. Kinesiol. 2004, 14, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Kwok, H.K.H.; Szeto, G.P.Y.; Cheng, A.S.K.; Siu, H.; Chan, C.C.H. Occupational rehabilitation in Hong Kong: Current status and future needs. J. Occup. Rehabil. 2011, 21 (Suppl. 1), S28–S34. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.; Szeto, G.; Lai, G.; Ching, S. Prevalence of and Factors Associated with Work-Related Musculoskeletal Symptoms in Nursing Assistants Working in Nursing Homes. Int. J. Environ. Res. Public Health 2018, 15, 265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umer, W.; Antwi-Afari, M.F.; Li, H.; Szeto, G.P.; Wong, A.Y. The prevalence of musculoskeletal symptoms in the construction industry: A systematic review and meta-analysis. Int. Arch. Occup. Environ. Health 2018, 1, 125–144. [Google Scholar] [CrossRef]
- Xu, Y.W.; Cheng, A.S.; Li-Tsang, C.W. Prevalence and risk factors of work-related musculoskeletal disorders in the catering industry: A systematic review. Work 2013, 44, 107–116. [Google Scholar] [CrossRef]
- Verhagen, A.P.; Karels, C.; Bierma-Zeinstra, S.M.; Feleus, A.; Dahaghin, S.; Burdorf, A.; Koes, B.W. Exercise proves effective in a systematic review of work-related complaints of the arm, neck, or shoulder. J. Clin. Epidemiol. 2007, 60, 110–117. [Google Scholar] [CrossRef]
- Larsson, B.; Søgaard, K.; Rosendal, L. Work related neck-shoulder pain: A review on magnitude, risk factors, biochemical characteristics, clinical picture and preventive interventions. Best Pract. Res. Clin. Rheumatol. 2007, 21, 447–463. [Google Scholar] [CrossRef]
- Dainoff, M.J.; Aarås, A.; Horgen, G.; Konarska, M.; Larsen, S.; Thoresen, M.; Cohen, B.G. The effect of an ergonomic intervention on musculoskeletal, psychosocial and visual strain of VDT entry work: organization and methodology of the international study. Int. J. Occup. Saf. Ergon. 2005, 11, 9–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ting, J.Z.R.; Chen, X.; Johnston, V. Workplace-Based Exercise Intervention Improves Work Ability in Office Workers: A Cluster Randomised Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 2633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, C.; Szeto, G.P.; Yan, T.; Wu, S.; Lin, C.; Li, L. Comparing biofeedback with active exercise and passive treatment for the management of work-related neck and shoulder pain: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2011, 92, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Johnston, V.; O’Leary, S.; Comans, T.; Straker, L.; Melloh, M.; Khan, A.; Sjøgaard, G. A workplace exercise versus health promotion intervention to prevent and reduce the economic and personal burden of non-specific neck pain in office personnel: Protocol of a cluster-randomised controlled trial. J. Physiother. 2014, 60, 233. [Google Scholar] [CrossRef]
- So, B.; Cheng, A.; Szeto, G. Cumulative IT Use Is Associated with Psychosocial Stress Factors and Musculoskeletal Symptoms. Int. J. Environ. Res. Public Health 2017, 14, 1541. [Google Scholar]
- Daniels, C.; Huang, G.D.; Feuerstein, M.; Lopez, M. Self-report measure of low back-related biomechanical exposures: Clinical validation. J. Occup. Rehabil. 2005, 15, 113–128. [Google Scholar] [CrossRef]
- Dane, D.; Feuerstein, M.; Huang, G.D.; Dimberg, L.; Ali, D.; Lincoln, A. Measurement properties of a self-report index of ergonomic exposures for use in an office work environment. J. Occup. Environ. Med. 2002, 44, 73–81. [Google Scholar] [CrossRef] [Green Version]
- Feuerstein, M.; Nicholas, R.A.; Huang, G.D.; Dimberg, L.; Ali, D.; Rogers, H. Job stress management and ergonomic intervention for work-related upper extremity symptoms. Appl. Ergon. 2004, 35, 565–574. [Google Scholar] [CrossRef]
- Meijer, E.M.; Sluiter, J.K.; Frings-Dresen, M.H. Is workstyle a mediating factor for pain in the upper extremity over time? J. Occup. Rehabil. 2008, 18, 262–266. [Google Scholar] [CrossRef] [Green Version]
- Harrington, C.B.; Siddiqui, A.; Feuerstein, M. Workstyle as a predictor of pain and restricted work associated with upper extremity disorders: A prospective study. J. Hand Surg. Am. 2009, 34, 724–731. [Google Scholar] [CrossRef]
- Cheng, A.S.; Szeto, G.P.; Xu, Y.W.; Feuerstein, M. Chinese translation and cross cultural adaptation of the workstyle short form. J. Occup. Rehabil. 2014, 24, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.; Ching, S.; Ma, K.; Szeto, G. Psychometric Evaluation of the Workstyle Short Form among Nursing Assistants with Work-Related Musculoskeletal Symptoms. Int. J. Environ. Res. Public Health 2018, 15, 823. [Google Scholar] [CrossRef] [Green Version]
- Szeto, G.P.; Lam, P. Work-related musculoskeletal disorders in urban bus drivers of Hong Kong. J. Occup. Rehabil. 2007, 17, 181–198. [Google Scholar] [CrossRef] [PubMed]
- Szeto, G.P.; Ho, P.; Ting, A.C.; Poon, J.T.; Cheng, S.W.; Tsang, R.C. Work-related musculoskeletal symptoms in surgeons. J. Occup. Rehabil. 2009, 19, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. J. Clin. Epidemiol. 2010, 63, 834–840. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, M.L.; Herbert, R.D.; Ferreira, P.H.; Latimer, J.; Ostelo, R.W.; Nascimento, D.P.; Smeets, R.J. A critical review of methods used to determine the smallest worthwhile effect of interventions for low back pain. J. Clin. Epidemiol. 2012, 65, 253–261. [Google Scholar] [CrossRef]
- Maher, C.G. Natural course of acute neck and low back pain in the general population: The HUNT study. Pain 2013, 154, 1480–1481. [Google Scholar] [CrossRef]
- Cohen, S.P. Epidemiology, diagnosis, and treatment of neck pain. Mayo Clin. Proc. 2015, 90, 284–299. [Google Scholar] [CrossRef] [Green Version]
- Tsang, S.M.; So, B.C.; Lau, R.W.; Dai, J.; Szeto, G.P. Comparing the effectiveness of integrating ergonomics and motor control to conventional treatment for pain and functional recovery of work-related neck-shoulder pain: A randomized trial. Eur. J. Pain 2019, 23, 1141–1152. [Google Scholar] [CrossRef]
- Tsang, S.M.; So, B.C.; Lau, R.W.; Dai, J.; Szeto, G.P. Effects of combining ergonomic interventions and motor control exercises on muscle activity and kinematics in people with work-related neck-shoulder pain. Eur. J. Appl. Physiol. 2018, 118, 751–765. [Google Scholar] [CrossRef]
- Nicholas, R.A.; Feuerstein, M.; Suchday, S. Workstyle and upper-extremity symptoms: A biobehavioral perspective. J. Occup. Environ. Med. 2005, 47, 352–361. [Google Scholar] [CrossRef] [PubMed]
- Santos, K.O.B.; de Araújo, T.M.; Carvalho, F.M.; Karasek, R. The job content questionnaire in various occupational contexts: Applying a latent class model. BMJ Open 2017, 7, e013596. [Google Scholar] [CrossRef] [PubMed]
- Oliv, S.; Gustafsson, E.; Baloch, A.N.; Hagberg, M.; Sandén, H. The Quick Exposure Check (QEC)—Inter-rater reliability in total score and individual items. Appl. Ergon. 2019, 76, 32–37. [Google Scholar] [CrossRef] [Green Version]
- McAtamney, H.S. Rapid Entire Body Assessment. In Handbook of Human Factors and Ergonomics Methods; Stanton, N., Hedge, A., Salas, E., Hendrick, H.W., Eds.; CRC Press: Boca Raton, FL, USA, 2005; pp. 1–11. [Google Scholar]
- Takala, E.P.; Pehkonen, I.; Forsman, M.; Hansson, G.Å.; Mathiassen, S.E.; Neumann, W.P. Systematic evaluation of observational methods assessing biomechanical exposures at work. Scand. J. Work Environ. Health 2010, 36, 3–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harari, Y.; Bechar, A.; Riemer, R. Workers’ biomechanical loads and kinematics during multiple-task manual material handling. Appl. Ergon. 2019, 83, 102985. [Google Scholar] [CrossRef] [PubMed]
- Sharan, D.; Parijat, P.; Sasidharan, A.P.; Ranganathan, R.; Mohandoss, M.; Jose, J. Workstyle risk factors for work related musculoskeletal symptoms among computer professionals in India. J. Occup. Rehabil. 2011, 21, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Hoe, V.C.; Urquhart, D.M.; Kelsall, H.L.; Zamri, E.N.; Sim, M.R. Ergonomic interventions for preventing work-related musculoskeletal disorders of the upper limb and neck among office workers. Cochrane Database Syst. Rev. 2018, 10, CD008570. [Google Scholar] [CrossRef] [PubMed]
- Prall, J.; Ross, M. The management of work-related musculoskeletal injuries in an occupational health setting: The role of the physical therapist. J. Exerc. Rehabil. 2019, 15, 193–199. [Google Scholar] [CrossRef]
- Pereira, M.; Comans, T.; Sjøgaard, G.; Straker, L.; Melloh, M.; O’leary, S. The impact of workplace ergonomics and neck-specific exercise versus ergonomics and health promotion interventions on office worker productivity: A cluster-randomized trial. Scand. J. Work Environ. Health 2019, 45, 42–52. [Google Scholar] [CrossRef] [Green Version]
- Mani, K.; Provident, I.; Eckel, E. Evidence-based ergonomics education: Promoting risk factor awareness among office computer workers. Work 2016, 55, 913–922. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CO Group | EM Group | p | ||||
|---|---|---|---|---|---|---|
| Age (yr) | 36.4 ± 8.9 | (22–54) | 35.6 ± 8.7 | (20–49) | 0.494 | |
| Gender | Male | 26 | 52% | 25 | 49% | 0.766 |
| Female | 24 | 48% | 26 | 51% | ||
| Weight (kg) | 64.4 ± 13.7 | (39.1–101.2) | 62.6± 11.8 | (42.3–82.7) | 0.561 | |
| Height (cm) | 167.9 ± 10.2 | (145.0–188.5) | 166.4 ± 9.3 | (145.0–180.0) | 0.734 | |
| BMI (kg/m2) | 22.7± 3.8 | (16.6–32.3) | 22.4± 2.6 | (17.6–29.3) | 0.529 | |
| Job categories | ||||||
| Banking and Finance | 2 | 4.0% | 6 | 11.76% | ||
| Food and Catering | 1 | 1.96% | ||||
| Engineering | 4 | 8.0% | 1 | 1.96% | ||
| Photographer/Tourism | 2 | 4.0% | 1 | 1.96% | ||
| Education (primary, secondary school teacher) | 2 | 4.0% | 4 | 7.84% | ||
| Healthcare | 7 | 14.0% | 6 | 11.76% | ||
| Sales and Retail | 5 | 10.0% | ||||
| Clerical/Admin | 15 | 30.0% | 19 | 37.25% | ||
| IT | 3 | 6.0% | 2 | 3.92% | ||
| Driver | 2 | 4.0% | 1 | 1.96% | ||
| Academic | 8 | 16.0% | 10 | 19.61% | ||
| Total | 50 | 100.0% | 51 | 100.00% | ||
| Occupational Exposure Measure | (T1) Pre-Intervention | (T2) Post-Intervention | Statistical Analysis (Univariate) F, p Values | ||||
|---|---|---|---|---|---|---|---|
| EM | CO | EM | CO | Time | Group | Time * Group | |
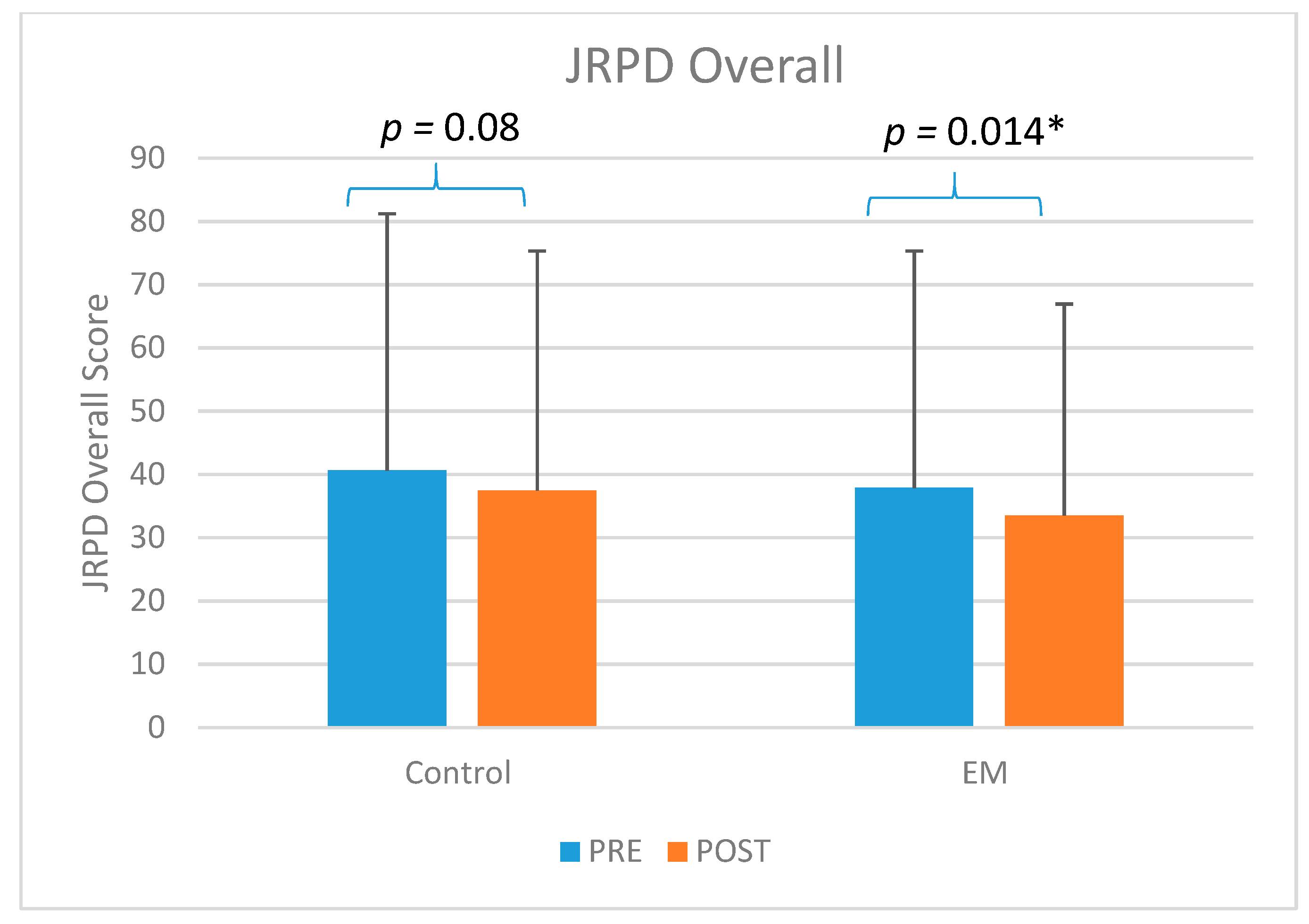
| JRPD (total) | 37.8(14) | 40.6(14.5) | 33.5(13.5) | 37.5(12.5) | F1,99 = 9.05, p = 0.003 ** | F1,99 = 1.94, p = 0.166 | F1,99 = 0.24, p = 0.623 |
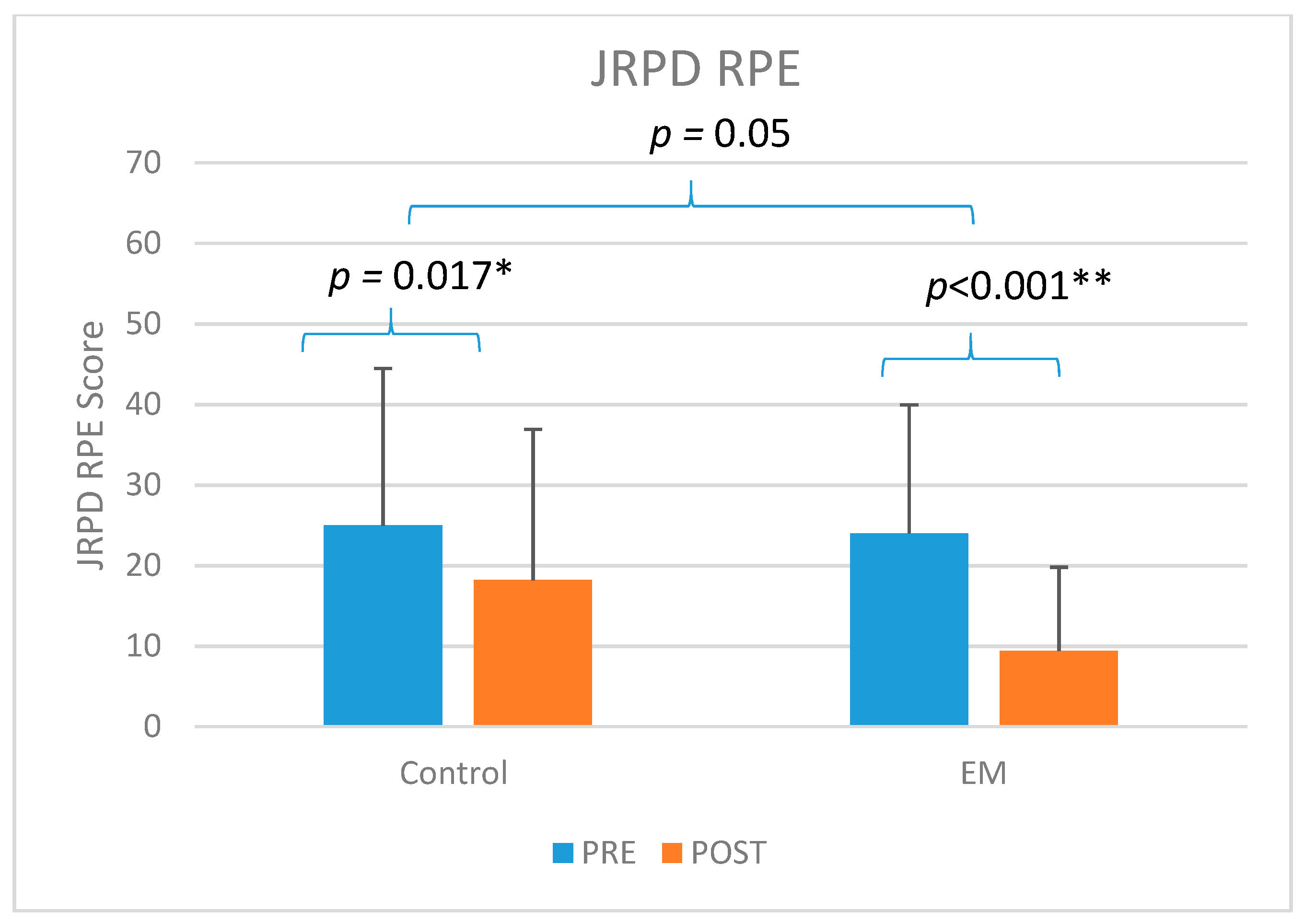
| JRPD (RPE) | 24.0(18.7) | 25.0(19.5) | 9.4(10.4) | 18.2(16) | F1,99 = 29.61, p < 0.000 ** | F1,99 = 3.43, p = 0.067 | F1,99 = 3.93, p = 0.05 * |
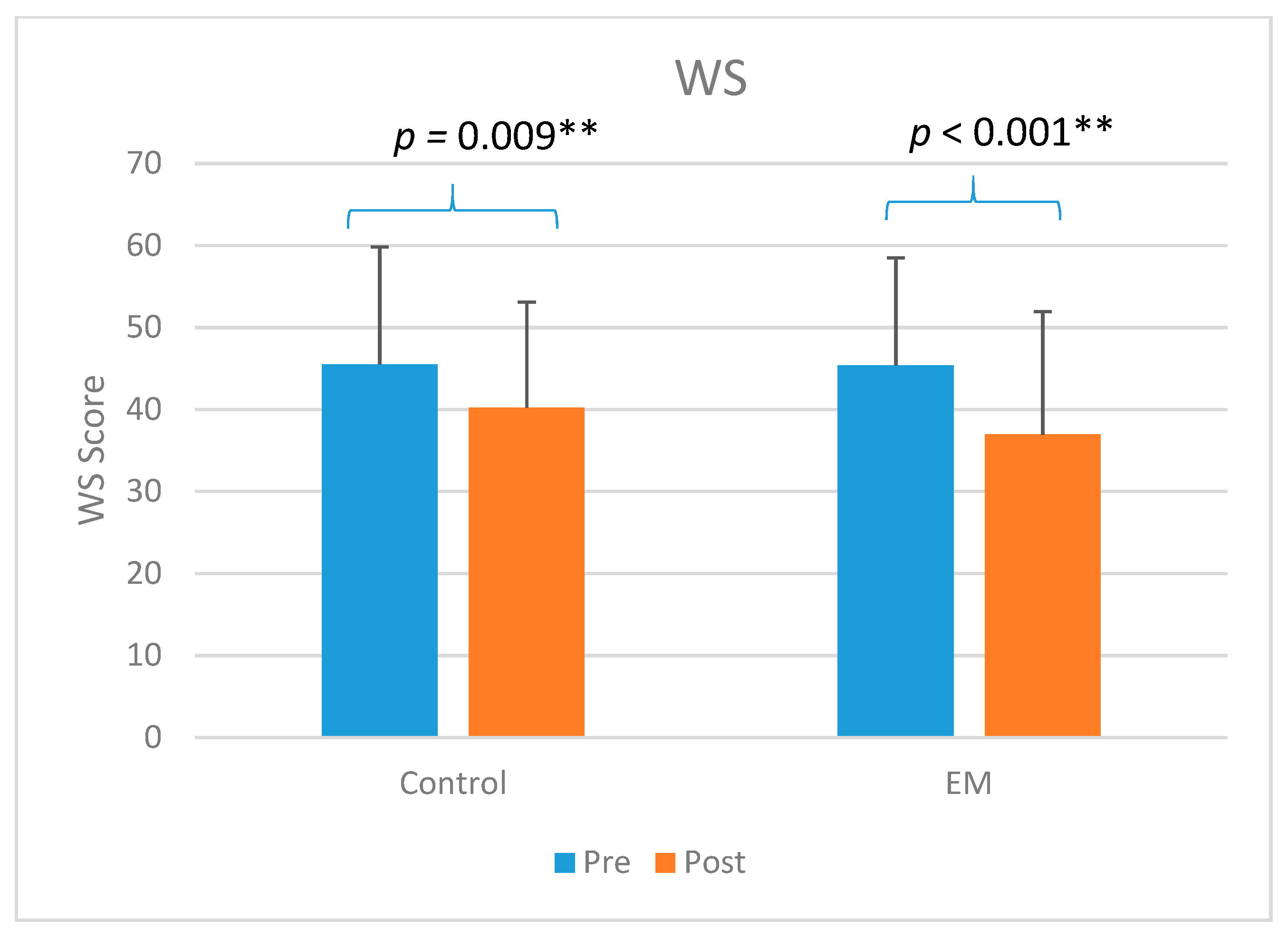
| WS (total) | 45.4(13.1) | 45.5(14.3) | 36.9(15) | 40.2(12.9) | F1,99 = 24.26, p < 0.000 ** | F1,99 = 0.51, p = 0.476 | F1,99 = 1.28, p = 0.260 |
| NUMBER OF SESSIONS | FEES PER SESSION (Estimated in HKD) | TOTAL FEES (HKD) | |||
|---|---|---|---|---|---|
| CO Group | EM Group | CO Group | EM Group | ||
| Med Doctor_public | 6 | 0 | 100 | 600 | 0 |
| Med Doctor_private | 10 | 2 | 300 | 3000 | 600 |
| Physiotherapy_public | 8 | 18 | 60 | 480 | 1080 |
| Physiotherapy_private | 31 | 53 | 500 | 15,500 | 26,500 |
| TCM_public | 0 | 1 | 100 | 0 | 100 |
| TCM_private | 147 | 88 | 300 | 44,100 | 26,400 |
| Total sessions | 202 | 162 | Total fees | 63,680 | 54,680 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
So, B.C.L.; Szeto, G.P.Y.; Lau, R.W.L.; Dai, J.; Tsang, S.M.H. Effects of Ergomotor Intervention on Improving Occupational Health in Workers with Work-Related Neck-Shoulder Pain. Int. J. Environ. Res. Public Health 2019, 16, 5005. https://doi.org/10.3390/ijerph16245005
So BCL, Szeto GPY, Lau RWL, Dai J, Tsang SMH. Effects of Ergomotor Intervention on Improving Occupational Health in Workers with Work-Related Neck-Shoulder Pain. International Journal of Environmental Research and Public Health. 2019; 16(24):5005. https://doi.org/10.3390/ijerph16245005
Chicago/Turabian StyleSo, Billy C. L., Grace P. Y. Szeto, Rufina W. L. Lau, Jie Dai, and Sharon M. H. Tsang. 2019. "Effects of Ergomotor Intervention on Improving Occupational Health in Workers with Work-Related Neck-Shoulder Pain" International Journal of Environmental Research and Public Health 16, no. 24: 5005. https://doi.org/10.3390/ijerph16245005