1. Introduction
Osteoarthritis (OA) is a chronic and degenerative joint disease that is part of the aging process. It is characterized by loss and degradation of articular cartilage in addition to synovial inflammation, leading to joint stiffness, swelling, pain, and loss of mobility [
1,
2,
3]. The cause of the onset of OA is not clear, but some factors are considered to be influencing factors (such as aging, obesity, inflammation, trauma, joint overuse, metabolic disorders, heredity, and so on.) [
3,
4]. The treatment of OA has been a kind of staged treatment, and mainly a nonoperative treatment, such as physical activity, nutrition, and drug treatment [
5]. OA usually occurs in knee, lumbar, cervical, hand, and hip joints, and because of the higher knee’s vulnerability to direct (knocked) and indirect (twisted) trauma, along with the high load supported by this joint, the knee is seen as the most frequently affected joint by OA [
1], and also the most studied joint.
OA is a major public health problem [
6]. It has been listed as the fastest increasing major health condition and ranked second as a cause of disability by the World Health Organization (WHO) [
7]. The WHO Scientific Group on Rheumatic Diseases estimates that 10% of the world’s population who are 60 years or older have significant clinical problems that can be attributed to OA [
8]. Because the burden of osteoarthritis has been heavier and heavier, prevention, treatments, and management for OA have been the focus of research on OA. Internationally, in 2013, American Academy of Orthopaedic Surgeons (AAOS) published a treatment guideline for knee OA to provide the recommendations based on the results of evidence-based medicine [
8]. In 2012, the OA Research Society International (OARSI) published an update to their evidence-based, consensus recommendations for the treatment of OA of the hip and knee joints [
9]. In China, the Chinese Medical Association Orthopaedic Society released the guidelines for diagnosis and treatment of osteoarthritis in 2018, providing great recommendations [
10].
The epidemiological character of OA in China can play a vital role in making policy for diagnosis, treatment, and management, which is also the precondition when making policy. The prevalence of osteoarthritis in different joints is consistently seen to increase with age [
11], and with the acceleration of China’s aging process and longer life expectancy, the prevalence of OA may increase significantly in the future. Only by having an exact knowledge of the number of patients and the distribution, the policy could be made more scientific. While in China, there are very limited data of large, multicenter, epidemic research on the prevalence of OA [
12]. Previous research has been conducted in the scale of one province or one city. Furthermore, huge differences between the current studies can be found due to the difference in mean age, geographic regions, ratio of sex, diagnosis criteria, and so on. For example, Wang et al. conducted an epidemic research study in Xi’an City (northern city) in 2007 and they reported a 9.5% prevalence of knee osteoarthritis among people aged 40 years old and over [
13]. Meanwhile, Ren ZhiJian conducted research in Wenzhou City, Zhejiang Province in 2017, and the prevalence of knee osteoarthritis they reported was 39.11% (southern city) [
14]. The overall prevalence of osteoarthritis is still not clear, which causes great confusion when making some strategies for OA patients. In addition to the population-based survey, there was a review conducted by Tie (published in a Chinese journal) to summarize the prevalence of knee OA, based on the existing articles, which reported that the prevalence of knee OA was 17% [
12]. As we know, there has been no other evidence-based review to report the prevalence of OA in lumbar, cervical, hip, and hand joints in the middle-aged and elderly in China.
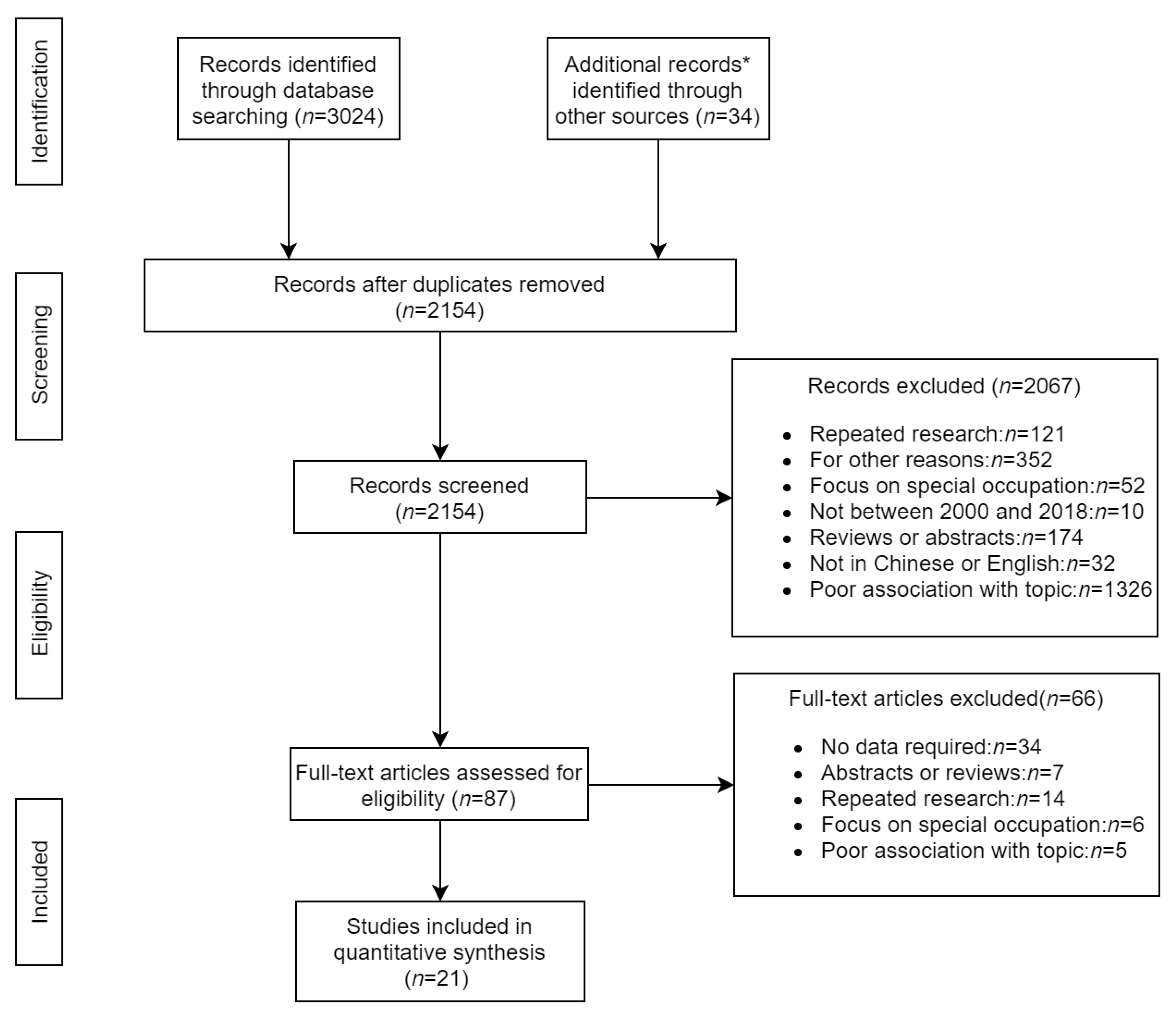
This paper aimed to pool OA prevalence data from current publications and to provide accurate estimates of the prevalence of OA in knee, lumbar, cervical, hand, and hip joints. “The middle-aged and elderly” refers to individuals who are aged 40 years old and over. It may be the first systematic review to provide overall estimates for the prevalence of osteoarthritis in the middle-aged and elderly in China, hoping to fill the vacancy and provide evidence for policy makers.
4. Discussion
This is the first systematic review and meta-analysis to provide the overall prevalence of OA in the middle-aged and elderly in China. It presented pooled population-based prevalence of OA in knee, lumbar, cervical, and hand joints. For hip OA, there were not enough articles available to conduct a meta-analysis; therefore, the prevalence of hip OA was just displayed. In addition, the distribution of prevalence of OA between age, sex, region, and diagnostic criteria was obtained by subgroup analysis. Before this review, the overall prevalence of OA in the middle-aged and elderly in China stayed unknown. There is a lack of larger-scale and multicenter epidemiological research for the prevalence of OA in China, which can also be concluded by systematic researching. Twenty-one articles were included in this paper, 20 of which were conducted in the scale of one province or city, and only one article conducted research in six cities of China. In addition, the prevalence of OA reported in different research studies had a huge difference to each other, making it unclear how to outline the overall prevalence according to an individual research study. Lastly, there were more research studies focused on the prevalence of knee OA, while sparse studies were conducted for lumbar OA, cervical OA, and hand OA. By systematic review, 21 articles reported the prevalence of knee OA, with 6–7 articles reporting the prevalence of lumbar OA, cervical OA, and hand OA and one article reporting the prevalence of hip OA. This review provided data on the overall prevalence of OA by pooling existing articles, filling the vacancies in the field of epidemic research for OA in China.
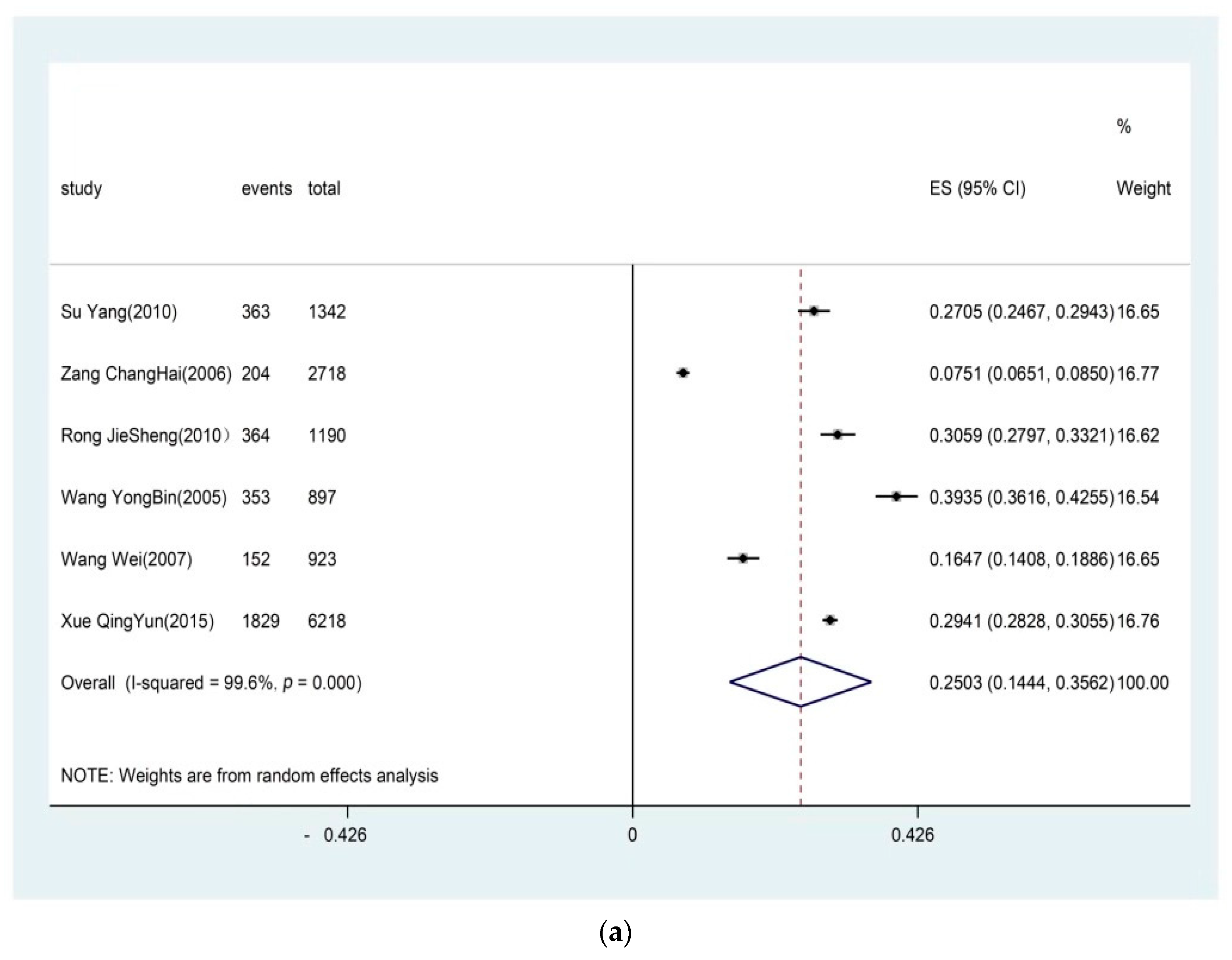
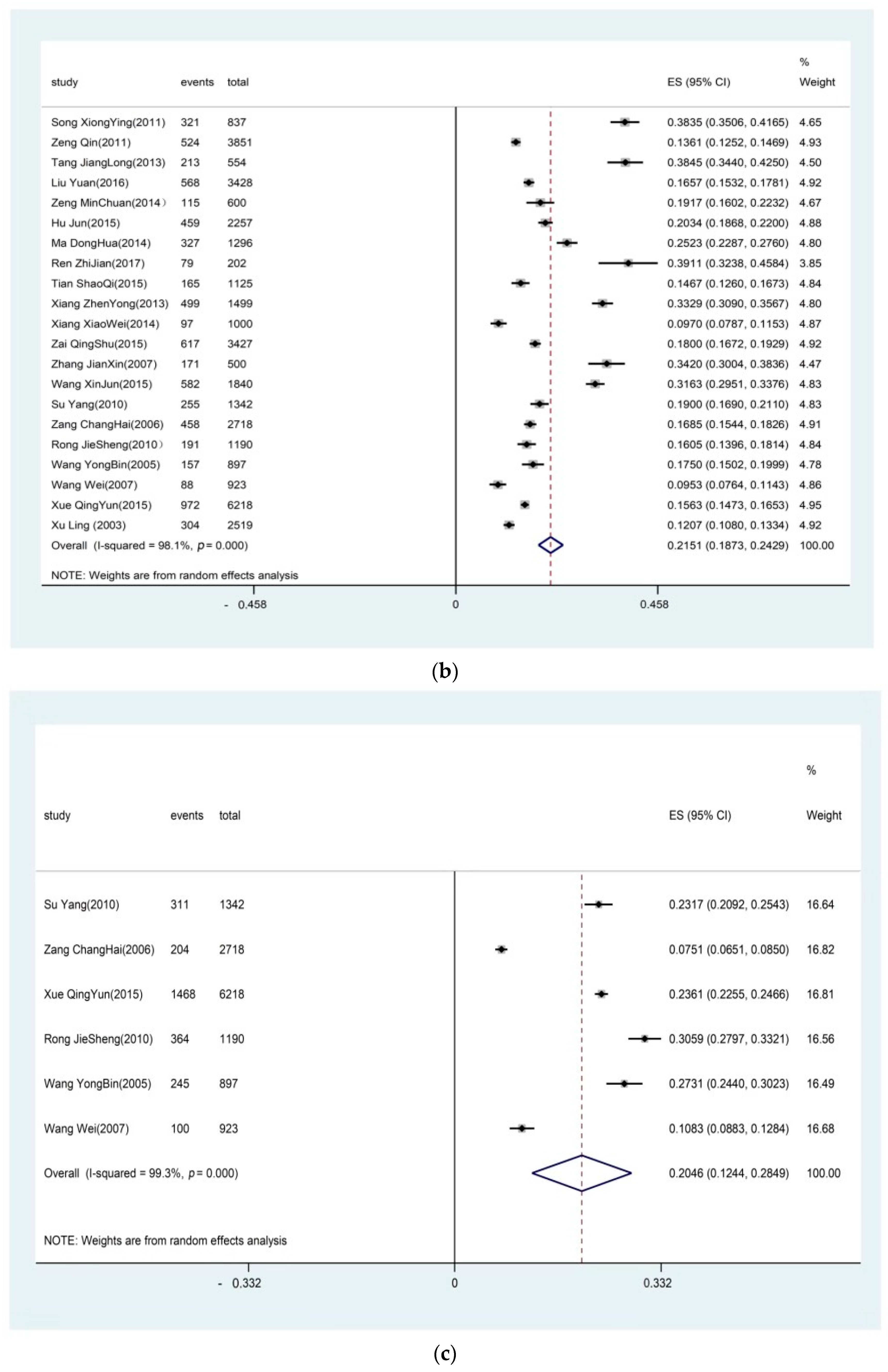
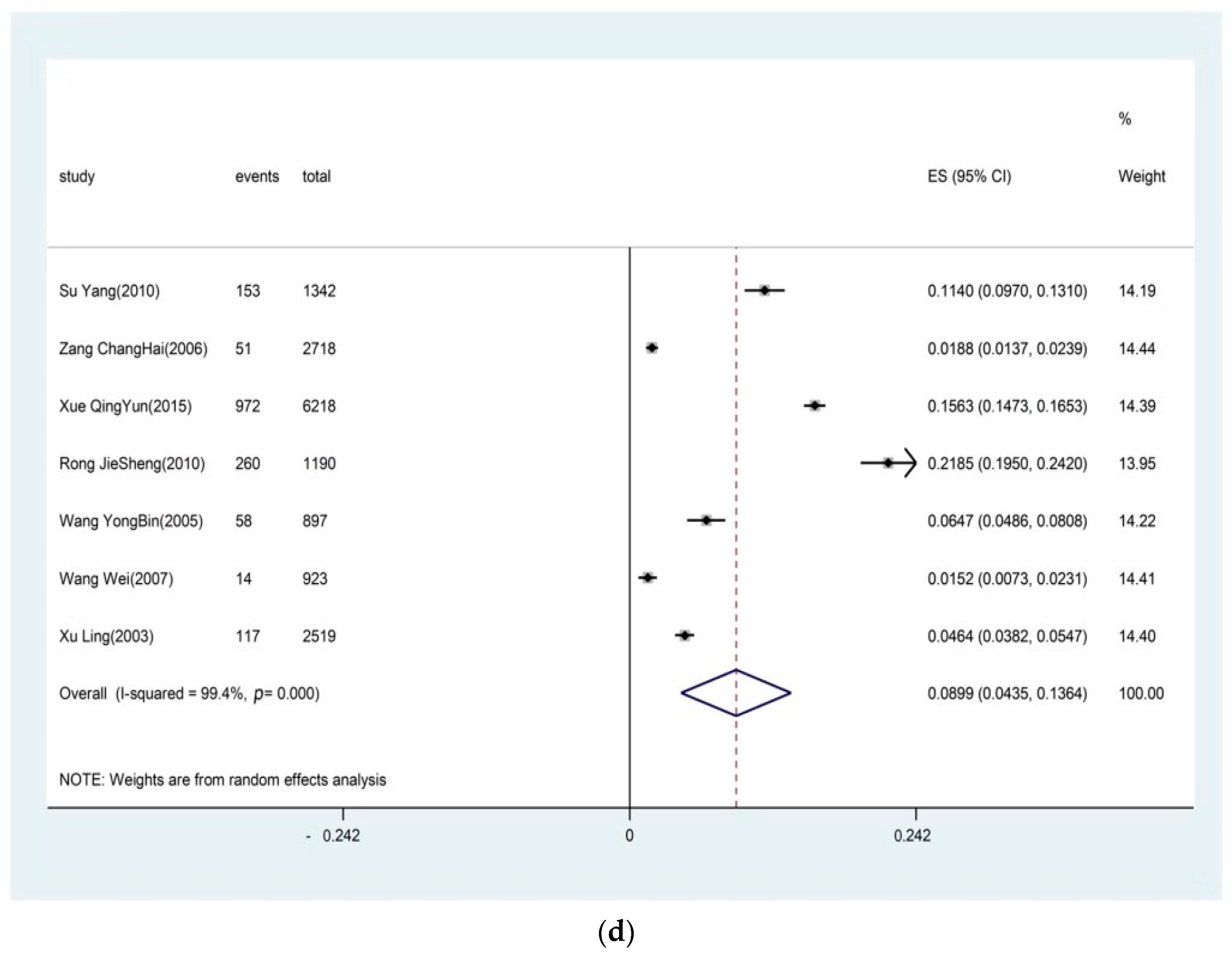
It can be concluded from the results that lumbar OA was the most prevalent, followed by the prevalence of knee OA, cervical OA, and hand OA. Hip OA was rare in China [
37]. It was supposed that the knee should be the most prevalently affected joint, given the heavy burden that knee joints bear; however, according to the results, lumbar OA was the most prevalent among the five joints. The result that lumbar OA was the most prevalent was consistent with Wang and Xue’s findings [
35]. Maybe because of the high level of mobility and load forces, the facet joints can be a potentially important source of symptoms, especially in the lumbar area [
38]. According to Xue’s research, the common risk factors of lumbar OA in the six cities are age and the Chinese life style of squatting defecation, which may explain the relatively higher prevalence of lumbar OA [
39]. The high prevalence of lumbar OA should be paid great attention because the osteoarthritic (facet joint changes) and degenerative alternation (disk area changes) in lumbar joints can be potential sources of low back pain (LBP), which is widespread and is the second most common concern expressed by patients in primary care [
40].
Through the subgroup analysis of the prevalence of OA in sex, age, regions, and diagnosis criteria, the distributions of OA can be found. A trend can be seen that the prevalence of OA in females, southern regions, and the elderly was higher, which was consistent with the findings of Felson et al. [
41]. They conducted the Framingham Osteoarthritis Study and found that the prevalence increased with age. They supposed that aging cartilage (shorter proteome chains, decreased water content) may be susceptible to fatigue fractures, producing OA; the increased subchondral stiffness to trabecular microfractures may account for increased OA (this increased bony stiffness remains to be identified); and that neuromuscular changes with age may predispose the joint to damages, resulting in OA [
41]. The gender-related prevalence finding was consistent with most of the survey [
41,
42]. The gender-related prevalence may be attributed to estrogen levels and different health-seeking behavior [
32,
42]. Estrogen levels in postmenopausal women are significantly lower than normal [
29]. Because of the difference of health-seeking behavior between females and males, women are more sensitive to the changes of their joints [
39]. The result that the prevalence was higher in southern regions was not consistent with Tie’s findings [
12]. It was supposed that the difference between southern regions and northern regions was mostly temperature and humidity, and a higher prevalence of OA can occur where it is cold and damp [
12]. With the improvement in economic conditions, the heating system in the northern regions has greatly improved and less people work outside than before. The cold weather may not affect people’s joints in the northern regions; however, there are more rains in the southern regions than northern regions, and the southern region is more humid, which may be contributable to the higher prevalence of OA.
Three suggestions based on the findings of this review can be provided for policy makers. First, more epidemiological data on OA should be collected through multiple ways. Through the systematic review, there was no national population-based survey to report the overall prevalence in China, while the survey for lumbar OA, cervical OA, hand OA, and hip OA was especially sparse. In order to have a thorough knowledge of the prevalence of OA in China, providing more evidence for policy makers, more population-based surveys are urgently needed. Meanwhile, one more item about OA could be considered to be added by the Chinese National Health Service Survey, which is conducted every five years. The question can be on the self-reported condition of OA, to obtain the epidemiological character for OA in the whole countryside from the view of self-reported prevalence. Furthermore, to solve the lack of data of lumbar OA, cervical OA, hand OA, and hip OA, more joints can be considered for inclusion in the surveys conducted in the future to provide more evidence for other joints. Based on the results, the prevalence of OA in several joints was relatively high and increased with age. With the aging process, the prevalence of OA will continue to increase, and the number of OA patients will increase year by year. To add, the WHO estimated that the OA would be the main crippling disease, causing great disease burden for society. According to the Fifth Chinese National Health Service Survey [
43], the prevalence of hypertension and diabetes was lower than the prevalence of OA in this review. Both hypertension and diabetes have been included in Key Chronic Disease Management in China; however, the management of OA has not been heightened. There are clear targets and end points to treating hypertension and diabetes, the goal of treating OA being pain/symptom relief. Compared with using healthcare in hospitals, more management and treatment of OA can be undertaken by primary healthcare institutions and communities. It can draw experience from the management of hypertension and diabetes, making full use of community medical care and primary medical care to carry out community-based health management for OA [
44,
45]. Meanwhile, more advertising about the prevention, diagnosis, and treatment of OA can be carried out in the communities to improve the initiative of self-management among the middle-aged and elderly population. Last, but not the least, due to the lack of a population-based survey, the method evidence-based medicine shows great advantages in obtaining the overall prevalence of OA.
To our knowledge, this is the first systematic review to explore the overall prevalence of OA in lumbar, knee, cervical, hand, and hip joints in China. However, there are still some limitations in this study. First, the heterogeneity between different studies was statistically significant; therefore, the results should be adopted with caution. To solve this, a random effects model was adopted when the heterogeneity was significant. Second, due to different diagnosis criteria adopted in the included articles, the prevalence extracted from the papers was not calculated by the same criteria, which may affect the polled results. To solve this, subgroup analysis was conducted for the articles with different diagnosis criteria. Third, compared with knee OA, the small number of articles included for lumbar OA, cervical OA, and hand OA may have caused the pooled estimates to be unstable. With more research conducted in the future, these results may be affected.

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}



